
Abstract
The findings of this scoping review suggest that occupational therapists should consider recommending weighted blankets as a sleep intervention option for people of all ages.
Sleep is a basic human need and as such is considered an important occupational domain by occupational therapists (American Occupational Therapy Association [AOTA], 2020). Sleep disorders “involve problems with the quality, timing, and amount of sleep” (American Psychiatric Association [APA], n.d., para. 1), with insomnia (problems getting to sleep and staying asleep) the most frequently experienced disorder (APA, n.d.). Sleep problems are associated with many health conditions over the life course and increase a person’s risk of developing or exacerbating chronic conditions, including heart disease, stroke, and mental health issues (Australian Institute of Health and Welfare, 2021). Even short-term sleep disturbances can affect a healthy person’s quality of life (Medic et al., 2017), with the effects often extending to caregivers (Gehrman et al., 2018). Given the importance of sleep for maximizing people’s health, well-being, and participation in daily activities, occupational therapists have a responsibility to address sleep problems with their clients and offer discipline-specific sleep interventions (Tester & Foss, 2018). Research, however, indicates that although occupational therapists identify sleep problems among their clients, they infrequently address sleep issues (Enam et al., 2023).
Clinical practice guidelines for the pharmacological treatment of chronic insomnia among adults report that the evidence is weak for commonly used drugs to treat insomnia (Sateia et al., 2017). In addition, there are risks associated with prescribing medications for individuals with a range of conditions, including people with dementia (National Health and Medical Research Council, 2016) and attention deficit hyperactivity disorder (ADHD; Scantlebury et al., 2018). Conversely, nonpharmacological sleep interventions are often multicomponent (Wilfling et al., 2021), with complexity a barrier to successful uptake. Thus, it is important to identify effective and straightforward nonpharmacological sleep interventions.
Weighted blankets, which promote relaxation through deep pressure stimulation (Mullen et al., 2008), are emerging as a nonpharmacological sleep intervention. Weighted blankets are heavier than a usual blanket and may be weighted with glass beads (ball blanket), fiber (fiber blanket), or metal chains sewn into the fabric (chain blanket). Weighted blankets are an assistive-technology device that occupational therapists may prescribe within their scope of practice. Occupational therapists use weighted blankets in different settings with people of all ages. Recent studies examining overnight use of weighted blankets for people experiencing sleep disturbances have included nursing home residents (Hjort Telhede, Arvidsson, & Karlsson, 2022), adults with insomnia (Ekholm et al., 2020) and psychiatric diagnoses (Steingrímsson et al., 2022), and children and adolescents with ADHD (Larsson et al., 2021). These studies indicated that weighted blankets may improve sleep (Hjort Telhede, Arvidsson, & Karlsson, 2022) and positively affect people’s daytime levels of activity (Ekholm et al., 2020).
In clinical practice, clear guidelines for use are required to support decision-making processes for patient care (Woolf et al., 2012). Although clinical guidelines and care protocols should be based on the best available evidence, the development of guidelines can be challenging in areas where the evidence is emerging or of poor quality. Currently, there are no definitive guidelines regarding use of weighted blankets (Eron et al., 2020). Although weighted blankets are used to support sleep for a range of populations, there is a lack of consensus about practice guidelines recommending frequency, duration, and method of use and outcomes. This review aimed to summarize the literature about the outcomes and application of weighted blankets as a sleep intervention to inform clinical decision-making. Therefore, our research questions were (1) What is the evidence regarding use of weighted blankets as a sleep intervention? (2) What implementation strategies are recommended to facilitate use of weighted blankets as a sleep intervention?
Method
We conducted a scoping review to identify the quantity and quality of research evidence available on the overnight use of weighted blankets, summarize the key findings, and identify gaps in the research (Grant & Booth, 2009). This scoping review methodology is informed by the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) review guidelines, which provide a framework that is transparent, objective, and rigorous (Page et al., 2021).
We drew on implementation frameworks to answer the second research question on identification of recommended implementation strategies. Specifically, we used the theoretical domains framework (TDF), which describes the range of factors affecting behavior change (e.g., knowledge, skills, social influences) and types of intervention strategies (e.g., education; Cane et al., 2012), and the Capability, Opportunity, and Motivation–Behavior (COM–B) model, which describes how capability, opportunity, and motivation lead to a behavior (Michie et al., 2011). These two frameworks promote an understanding of the barriers to and facilitators of implementation in health care settings and inform implementation interventions (Wright et al., 2023).
Inclusion Criteria
We included peer-reviewed published literature in English (including conference abstracts) from 1995 onward in which weighted blankets were used overnight as a sleep intervention for any human population. Studies that did not include results or a discussion of the use of weighted blankets overnight were excluded.
Search Strategy and Data Extraction
Databases searched included MEDLINE, Cochrane Library, CINAHL, PsycINFO, Scopus, Embase, and the first 100 results of a Google advanced search. (Search terms are presented in Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot.) We used Covidence (an online literature review tool) to manage the screening process. Titles and abstracts were screened for eligibility, followed by full text review against inclusion and exclusion criteria. Two researchers conducted the reviews (Jenny Cleland and Suzanne Dawson, Lorraine Ng, or Kimberly Charlton), and a third researcher (Stacie Attrill) clarified ambiguity when a consensus was not reached. Cleland reviewed reference lists from eligible sources to identify further sources.
We extracted key data into an Excel spreadsheet. Information extracted included authors, date, country, study design and aim, setting, participants, intervention description, guidelines for blanket use, and results–findings.
Data Synthesis
To address the first research question, we synthesized and critically appraised data to provide information about weighted blanket outcomes. We separated the reporting for children–adolescents and adults to reflect the differences in findings across age groups.
To address the second research question, we used the TDF and COM–B frameworks to identify and synthesize recommendations for implementation. First, we mapped data pertaining to implementation of weighted blankets against the domains of the TDF framework to understand the key factors affecting behavior change. Second, we mapped the TDF domains against the COM–B model domains of capability, opportunity, and motivation to describe how these key factors led to a change in behavior (Cane et al., 2012). The narrative presented a synthesis of the key factors affecting behavior change from the included studies.
Quality Appraisal
To provide contextual information for the first research question, we used three critical appraisal tools to assess the quality of reporting for the included studies. We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist (von Elm et al., 2008) for the observational and randomized controlled trials. The four areas assessed included (1) design and setting, (2) participants and eligibility, (3) outcomes, and (4) analysis. Studies were scored 1 for each domain that was clearly reported. We used the Joanna Briggs Institute (JBI) Checklist for Qualitative Research (Aromataris & Munn, 2020) for qualitative studies and the Mixed Methods Appraisal Tool (Hong et al., 2018) for the one mixed-methods study.
After data extraction and critical appraisal, we further assessed methodological rigor using the Levels of Evidence for Therapeutic Studies from the University of Oxford Centre for Evidence-Based Medicine (Burns et al., 2011). This enabled the development of practice recommendations against the main study outcomes. Recommendations were made by mapping the levels of evidence against the Grade Practice Recommendations table (Burns et al., 2011) to inform evidence-based clinical practice guidelines.
Results
Search Results
Figure 1 shows the search strategy and selection of studies. Eighteen sources met the inclusion criteria (see Table A.2 in the Supplemental Material), with several papers reporting on the same study (Hjort Telhede, Arvidsson, & Karlsson, 2022; Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022) and data set (Odéus et al., 2023; Steingrímsson et al., 2022). Thirteen studies were published since 2020. Studies adopted a range of methodologies, including quantitative (n = 15), qualitative (n = 2), and mixed methods (n = 1). Three articles reported on randomized controlled trials (RCTs; Baumgartner et al., 2022; Ekholm et al., 2020; Gringras et al., 2014), with most studies using lower quality methods, including case series or case study methodologies, pre–post design, or small participant samples. One study was reported as a conference abstract (Danoff-Burg et al., 2020). Studies were conducted in Sweden (n = 8), the United States (n = 5), Australia (n = 1), the United Kingdom (n = 1), Denmark (n = 2), and Japan (n = 1). Participant sample sizes ranged between one (Nakamura & Yamauchi, 2021) and 4,092 participants (Odéus et al., 2023). Weighted blankets were most frequently trialed with participants in their own home, with one study conducted in an inpatient psychiatric unit (Dawson et al., 2022) and three studies conducted in residential senior care facilities (Hjort Telhede, Arvidsson, & Karlsson, 2022; Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022; Nakamura & Yamauchi, 2021).
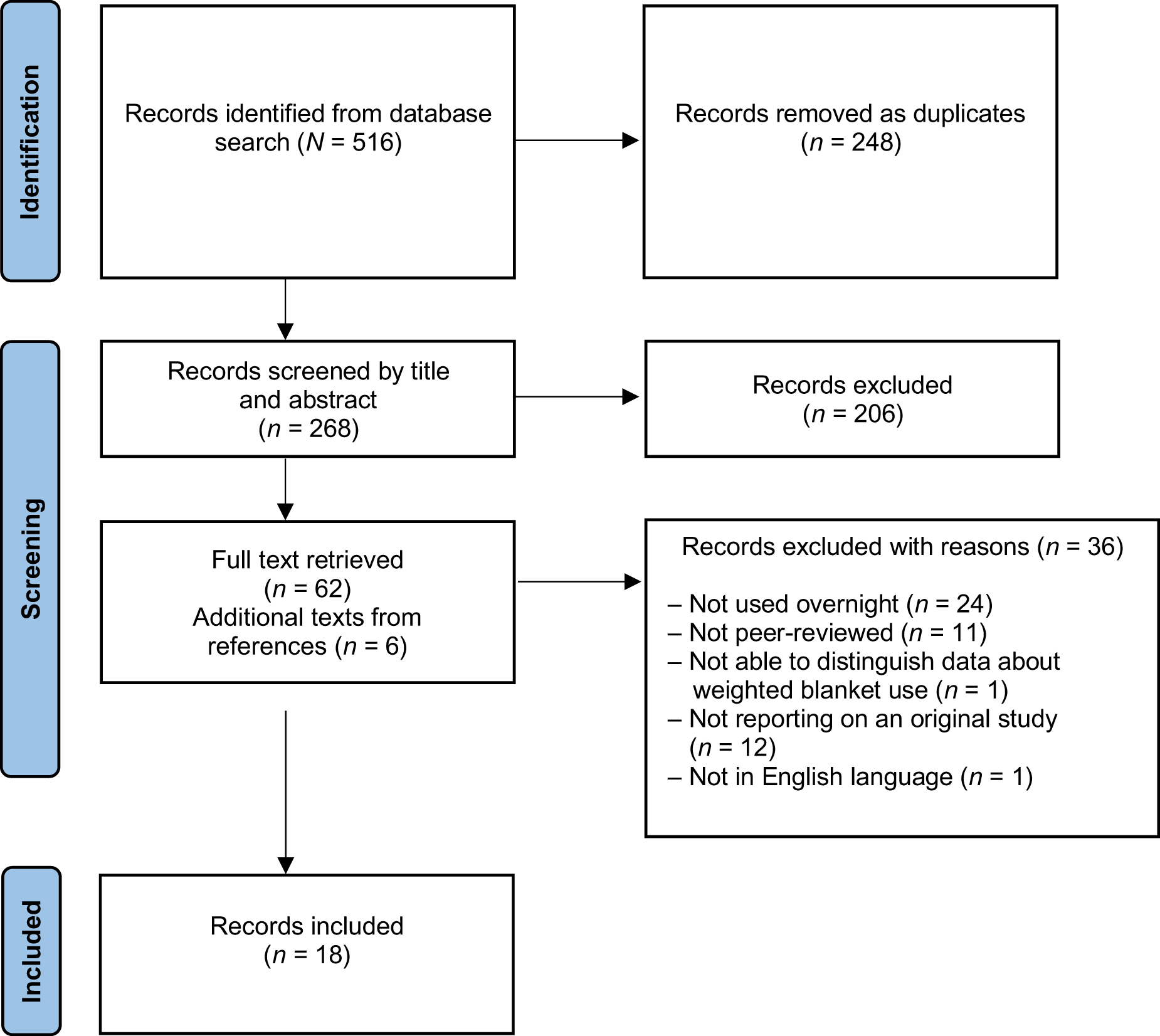
Flow of studies through the scoping review.
Quality Appraisal
We appraised all 18 studies. Of the 15 observational trials or RCTs that were included, 12 assessed 4 out of 4, and 3 assessed 2 out of 4 against four STROBE appraisal criteria: design and setting, participants and eligibility, outcomes, and analysis (see Table A.3 in the Supplemental Material). The two qualitative studies included in the review assessed 8 out of 10 based on the 10 JBI quality appraisal criteria (see Table A.4). The one mixed-methods study assessed 12 out of 16 according to the criteria outlined in the Mixed Methods Appraisal Tool (see Table A.5). All studies were included in this scoping review, with the limitations of studies with quality scores of 2 out of 4 considered when we present the results.
Population
Eleven studies included adults as participants. Most of these studies focused on individuals with sleep disturbances (n = 5; Ackerley et al., 2015; Bolic Baric et al., 2021; Danoff-Burg et al., 2020; Hjort Telhede, Arvidsson, & Karlsson, 2022; Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022) and mental health diagnoses, including schizophrenia, anxiety, depression, bipolar disorder, schizoaffective disorder, ADHD, and autism spectrum disorder (ASD; n = 5; Bolic Baric et al., 2021; Dawson et al., 2022; Ekholm et al., 2020; Odéus et al., 2023; Steingrímsson et al., 2022). Other conditions included chronic pain (Baumgartner et al., 2022) and dementia (Nakamura & Yamauchi, 2021). Two studies included reports on staff perceptions of the use of weighted blankets (Dawson et al., 2022; Hjort Telhede, Arvidsson, & Karlsson, 2022). Eight studies included children or adolescents as participants with sleep disturbances associated with autism and ADHD (Bolic Baric et al., 2021; Gee et al., 2016, 2017, 2021; Gringras et al., 2014; Hvolby, 2020; Hvolby & Bilenberg, 2011; Larsson et al., 2021).
Intervention
Intervention Summary for Overnight Use of Weighted Blankets
Denotes most frequently reported.
Purpose of Weighted Blankets
All studies explored overnight use of weighted blankets, with most focusing specifically on use as a sleep intervention. Other foci included examining the impact on pro re nata (PRN) medication use for mental health clients (Dawson et al., 2022) and the impact on chronic musculoskeletal pain (Baumgartner et al., 2022).
Blanket Weight and Type
Thirteen studies reported the blanket weights. The studies with children reported weights ranging from 2.3 kg to 10 kg. For adults, although weights were often reported to be 10% body–blanket weight ratio, individuals were reported to prefer heavier weights when provided with an option (Ackerley et al., 2015; Baumgartner et al., 2022; Ekholm et al., 2020). In two studies, participants had a body–blanket weight ratio of more than 12% (Ackerley et al., 2015); this included a female participant with severe dementia (Nakamura & Yamauchi, 2021). The heaviest reported blanket weight was 14 kg (Odéus et al., 2023; Steingrímsson et al., 2022). Different blanket types were used in the studies. Participants in one study reported preferring the chain blanket (64%), ball blanket (20%), and fiber blanket (16%; Odéus et al., 2023).
Prescription Process (Who Prescribes?)
Seven studies reported on prescription processes. Weighted blankets were predominantly recommended by occupational therapists. A study of an inpatient psychiatric rehabilitation unit required medical staff to assess for overnight use and encouraged nurses to offer low-weight blankets (Dawson et al., 2022). In a study conducted in Sweden, both physical and occupational therapists prescribed weighted blankets for individuals with mental health conditions who had a history of sleep problems and were referred to a clinic for assessment (Odéus et al., 2023; Steingrímsson et al., 2022). Bolic Baric et al. (2021) described a clinic where children with ADHD or autism and sleep problems were prescribed weighted blankets.
Safety Considerations
Five studies reported recommendations for safe use of weighted blankets. In studies involving children, caregivers were educated to ensure the child could remove the blanket, avoid covering the head, and check regularly and not use the blanket if the child was hot or the blanket was worn (Gee et al., 2016, 2021). In institutional settings (an adult inpatient psychiatric rehabilitation and nursing home), instructions included ensuring the person could independently remove the blanket (Dawson et al., 2022; Hjort Telhede, Arvidsson, & Karlsson, 2022), avoiding placing the blanket twice over the chest or tightly around the person, assessing suitability through observation, and removing the blanket if the person showed discomfort (Hjort Telhede, Arvidsson, & Karlsson, 2022).
Outcomes
Recommended Reasons and Levels of Evidence for Overnight Use of Weighted Blankets for Adults and Children
Note. Level A = strong recommendation; Level B = recommended but considering patient preferences and new data; Level C or D = optional with patient preference having a strong influence.
Although there were no Level A recommendations, overnight weighted blanket use for adults was recommended (alongside consideration of patient preferences) for improving sleep and mood and reducing medication use and pain. All these were rated Level B. Weighted blanket use overnight was recommended for children to improve their daily functioning (Level B rating).
The following sections present a detailed synthesis of the main outcomes reported across the studies. There were no adverse outcomes reported in any studies.
Sleep
Sleep was a key outcome of overnight use of weighted blankets in most studies (n = 16). For adults, this included outcomes from a range of populations.
Improved sleep outcomes were observed among older adults, including a single case study of a person with severe dementia (Nakamura & Yamauchi, 2021). A study investigating use of weighted blankets with nursing home residents using standardized measures pre- and postintervention (Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022) and qualitative interviews with nursing home staff (Hjort Telhede, Arvidsson, & Karlsson, 2022) identified improvements in sleep. Residents fell asleep more quickly, were less disturbed throughout the night, slept longer, and were less tired during the day. An RCT study evaluating the effect of weighted blankets on insomnia and sleep-related daytime symptoms for individuals with psychiatric disorders resulted in significantly better sleep during the night and reduced fatigue during the day (Ekholm et al., 2020). These findings were supported by participant reports of improved sleep in a psychiatric inpatient setting (Dawson et al., 2022). Other studies reported improvements in sleep for adults with ADHD or autism (Bolic Baric et al., 2021), sleep onset and sleep maintenance issues (Danoff-Burg et al., 2020), and insomnia (Ackerley et al., 2015). A study with adults experiencing chronic pain found no significant improvements in sleep quality (Baumgartner et al., 2022).
All studies on children reported the impact that weighted blankets had on sleep. A qualitative study exploring parents’ experience of using weighted blankets for children with ADHD and sleep problems reported improvements in the children’s sleep onset latency, sleep continuity, and sleep routines (Larsson et al., 2021). This finding was supported by two case control studies that reported reduced sleep onset latency and decreased nighttime wakening using ball blankets with children with ADHD (Hvolby, 2020; Hvolby & Bilenberg, 2011). However, other studies identified minimal improvements in sleep for children using weighted blankets. Specifically, studies investigating the efficacy of using weighted blankets with autistic children with sleep disturbance reported minimal improvements or changes in sleep duration and time to fall asleep (Gee et al., 2016, 2017, 2021). An RCT conducted with autistic children (n = 73) found weighted blankets did not significantly affect sleep duration, time taken to fall asleep, or frequency of waking, although weighted blankets were positively regarded by parents and children (Gringras et al., 2014).
Medication
Three studies reported weighted blanket use led to reduced medication use (Dawson et al., 2022; Hjort Telhede, Arvidsson, & Karlsson, 2022; Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022; Steingrímsson et al., 2022). The use of weighted blankets resulted in a significant reduction in use of PRN medication in the second 3-mo period following implementation in an inpatient psychiatric setting (Dawson et al., 2022). In a senior care setting, weighted blankets were found to positively affect residents’ emotional and psychological expressions, resulting in reduced daytime medication use (Hjort Telhede, Arvidsson, & Karlsson, 2022; Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022). A study measuring sleep medication prescriptions before and after receiving a weighted blanket among adults with psychiatric diagnoses reported a reduction in the use of sleep medications (except for melatonin) following weighted blanket use (Steingrímsson et al., 2022). From this same data set, an observational study investigating the cost of weighted blankets showed that the prescription process for weighted blankets was longer and more costly than prescribing sleep medication (Odéus et al., 2023).
Mood and Behavior
Eight studies with adults reported on participants’ moods or behaviors. Staff reported that older adults in nursing homes experienced reduced anxiety and improved ability to communicate feelings (Hjort Telhede, Arvidsson, & Karlsson, 2022). In addition, care staff reported an older person with severe dementia experienced slightly reduced severity of elation–euphoria following use (Nakamura & Yamauchi, 2021). Individuals in a psychiatric inpatient rehabilitation setting reported increased concentration and confidence (Dawson et al., 2022), and participants attending an affective disorder clinic reported reduced daytime symptoms of depression and anxiety (Ekholm et al., 2020). A study with adults with sleep onset and maintenance issues identified reduced feelings of stress and enhanced relaxation when trying to fall asleep (Danoff-Burg et al., 2020). Conversely, overnight weighted blanket use had no significant impact on anxiety for adults living with chronic pain (Baumgartner et al., 2022).
All studies examining the use of weighted blankets with children reported on their moods or behaviors. Studies examining the impact of weighed blankets on morning mood of autistic children found no consistent improvement for two of the four participants (Gee et al., 2016, 2017). A study of two participants found caregivers’ ratings of children’s morning mood improved with the intervention (Gee et al., 2021). Two case control studies reported improved attention and reduced impulsivity, hyperactivity, and behavioral symptoms (Hvolby, 2020; Hvolby & Bilenberg, 2011). A qualitative study examining parents’ experiences of weighted blanket use with children with ADHD and sleep problems (Larsson et al., 2021) and a retrospective follow-up study on the impact of weighted blankets on children with ADHD or autism (Bolic Baric et al., 2021) support these findings, reporting that children were more relaxed and less anxious, angry, and irritable, with improved sleep contributing to a more stable mood.
Pain
One RCT conducted in the home setting demonstrated that overnight weighted blanket use significantly reduced perceptions of chronic pain (Baumgartner et al., 2022). Participants experienced musculoskeletal (61%), neuropathic (19%), secondary visceral (7%), cancer-related (2%), and posttraumatic pain (1%), with 40% meeting criteria for more than one category.
Daily Function
Seven articles reported on the impact of weighted blankets on daily function. In a study with older adults in nursing homes, nursing staff reported increased wakefulness was related to increased independence during daily activities and activity during mealtimes (Hjort Telhede, Arvidsson, & Karlsson, 2022). However, in the same study, quantitative measures (using the Katz Index of Independence in Activities of Daily Living assessment) reported improved food intake but not increased independence (Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022). Positive engagement in leisure activities and nighttime routine was described by staff in a single-case design involving a female participant with Alzheimer’s, alongside a reported decrease in care level (Nakamura & Yamauchi, 2021).
Positive associations between weighted blanket use and daily functioning were also observed in studies of children with ADHD (Bolic Baric et al., 2021; Hvolby, 2020; Hvolby & Bilenberg, 2011; Larsson et al., 2021). Parents reported increased participation in their child’s school activities and homework, increased participation in tasks at home, and enhanced engagement in leisure activities and socializing (Larsson et al., 2021). Weighted blanket use was reported to improve children’s activity levels and attention span as rated by teachers (10%) and parents (6%; Hvolby & Bilenberg, 2011), improved attention and reduced impulsivity as rated by teachers and parents (Hvolby, 2020), and improved school performance as reported by participants in interviews (Bolic Baric et al., 2021).
Implementation Strategies
Implementation Strategies for Using Weighted Blankets
Note. COM–B = Capability, Opportunity, and Motivation–Behavior model; TDF = theoretical domains framework.
Capability
Staff knowledge and skills were important factors in supporting weighted blanket use and included procedural knowledge (how to apply the intervention) and understanding the rationale for weighted blanket use. Procedural knowledge was obtained via training (Dawson et al., 2022) and protocols that referred to blanket weights and, specifically, offering heavier weights prior to lighter weights (Ackerley et al., 2015; Ekholm et al., 2020), ensuring independence in removing blankets (Dawson et al., 2022; Gee et al., 2016, 2021; Hjort Telhede, Arvidsson, & Karlsson, 2022; Odéus et al., 2023), assessing blanket hygiene and wear (Dawson et al., 2022; Hjort Telhede, Arvidsson, & Karlsson, 2022; Hjort Telhede, Arvidsson, Karlsson, & Ivarsson, 2022), and obtaining medical clearance for people with conditions that may complicate use (e.g., impaired respiratory functioning; Dawson et al., 2022; Nakamura & Yamauchi, 2021). Protocols for children incorporated parental sleep routines (Larsson et al., 2021) and recommended checking on the child during use (Gee et al., 2017, 2021).
Procedural knowledge included prescription processes related to the setting. Odéus et al. (2023) recommended using a screening tool to identify who may benefit from weighted blanket use in community settings, whereas Dawson et al. (2022) suggested offering low-weight blankets to all individuals in an inpatient psychiatric rehabilitation setting on admission.
Opportunity
Social influences, the environmental context, and the availability of resources were emphasized in a study that examined the implementation of weighted blankets in a psychiatric rehabilitation unit (Dawson et al., 2022). Recommendations included building relations between staff (e.g., reporting successes, using current service processes to promote use, having an interdisciplinary steering committee to support use), between clients and staff (e.g., involving clients in developing educational resources), and between clients (e.g., providing opportunities for sharing experiences).
The environmental context and resources can encourage or discourage staff behavior. Resources included ensuring weighted blankets are available, accessible, and well maintained; encouraging a mix of targeted and opportunistic approaches to promote use; and ensuring protocols for use are available (Dawson et al., 2022).
Motivation
Recommendations to promote staff motivation to prescribe weighted blankets referred to professional roles, identities, and beliefs about capabilities and consequences. Although occupational therapists are usually responsible for prescribing weighted blankets, identifying staff leads from other disciplines (e.g., nursing, medical) was suggested to promote uptake (Dawson et al., 2022). Strategies to address staff beliefs about capabilities and consequences included aligning the intervention with service models of care, staff values, and professional role–identity and challenging low staff expectations regarding clients’ ability to engage in or benefit from weighted blankets (Dawson et al., 2022).
Discussion
Findings from this scoping review provide valuable insights into the current use of weighted blankets as a sleep intervention for individuals across ages with a range of health conditions and provide a useful framework for translation into practice. Most studies investigating weighted blanket use for sleep have occurred since 2020, demonstrating an increasing level of interest in weighted blankets as a sleep intervention. Although Mullen et al. (2008) demonstrated the safety and therapeutic effects (specifically, reduced anxiety) of weighted blankets almost two decades ago, broad uptake into clinical practice has been slow. Safety concerns raised in protocols for weighted blanket use (Royal College of Occupational Therapists, 2023; Te Pou, 2021) may be affecting use, although there has been increased popularity in use in recent years outside the therapeutic sphere. Outcomes from the studies in this review show that the effectiveness of weighted blankets as a sleep intervention is variable, with stronger positive results for adults (including older adults) than children and adolescents. Studies also reported other positive changes as a result of overnight weighted blanket use, including reduction in medication use, mood, and pain levels (for adults) and improved occupational functioning (for children). Importantly, no adverse outcomes were reported in any studies.
Although there were some high-quality RCTs (Baumgartner et al., 2022; Ekholm et al., 2020; Gringras et al., 2014), many studies in this review had low participant numbers and lacked control groups and long-term outcome measures. The methodological quality of the studies affected the strength of recommendations that can be made regarding the use of weighted blankets as a sleep intervention when considering effectiveness. Understandings, however, of evidence-based health care have expanded over the past two decades (Jordan et al., 2018; Pearson et al., 2005). The updated JBI model of evidence-based health care identified the following factors as core features for consideration: feasibility, appropriateness, meaningfulness, and effectiveness (Jordan et al., 2018). Effectiveness, although important, is one component of evidence-based practice. Patient preference (meaningfulness) and successful implementation of an intervention (feasibility and appropriateness) are also essential components. Two studies with diverse participant groups—people living with dementia and their family caregivers (Harris & Titler, 2022) and infants with neonatal abstinence syndrome (Summe et al., 2020)—have demonstrated the feasibility and appropriateness of daytime weighted blanket use. Potential measures of fidelity (e.g., days of blanket use, lack of adverse events) and acceptability (satisfaction, perceived benefits) can inform our understanding of these factors. Although the studies in this review did not specifically examine these implementation outcomes, a level of feasibility or acceptability can be inferred through participants completing the research (involving the weighted blanket intervention) and positive reports from patient, family, or staff. Most evidence outcomes for adults in this review were rated at Level B evidence. As such, occupational therapists can recommend weighted blankets for sleep, with consideration of patient preferences. For children, although occupational functioning was reported to improve (Level B) because of overnight weighted blanket use, minimal changes in sleep were reported. A Level C rating does not preclude occupational therapists from exploring weighted blankets as a sleep intervention option. However, evidence should be used to inform transparent discussions with parents and children.
Commonly experienced barriers to implementing evidence-based health care exist at the individual (clinician and client) and systems (service) levels (Raphael et al., 2021; Williams et al., 2015). Adapting the environment, including the use of assistive devices or equipment (such as weighted blankets), is a recommended occupation-based sleep intervention (Ho & Siu, 2018). This review identified occupational therapists as the key profession prescribing weighted blankets. Thus, clinician-level barriers to addressing sleep issues, including lack of knowledge in sleep assessment and sleep (Enam et al., 2023), will have an impact on uptake of weighted blanket use. The various strategies that promoted implementation and use (described in Table 3) and details of the weighted blanket intervention (summarized in Table 1) can be applied by occupational therapists in clinical practice. Current guidelines typically recommend limited weight–body ratios (usually up to 10%) and discourage prolonged or overnight use and independent or unsupervised use (Royal College of Occupational Therapists, 2023; Te Pou, 2021). This evidence summary found that the body–blanket weight ratio was often over 10%, with heavier weights preferred (Ackerley et al., 2015; Baumgartner et al., 2022; Ekholm et al., 2020). Blanket weight was guided by user preferences or manufacturer recommendation of 10% body–blanket ratio (Gringras et al., 2014; Larsson et al., 2021; Odéus et al., 2023; Steingrímsson et al., 2022). Most studies reported on weighted blanket use in the home setting, suggesting that overnight use was unsupervised. Conversely, overnight use of blankets involved increased supervision and support with young children and older adults with cognitive impairment (Gee et al., 2021; Hjort Telhede, Arvidsson, & Karlsson, 2022).
Service-level barriers to implementing evidence-based practice in health care settings include workload, unsupportive staff or management, lack of resources, lack of authority for practice change, and resistive workplace culture (Williams et al., 2015). Implementation frameworks and theories seek to address these barriers by understanding the broad range of contextual factors affecting uptake of any targeted interventions (Nilsen, 2015). As contextual factors are likely to affect intervention effectiveness (Raphael et al., 2021), understanding and addressing potential barriers and emphasizing facilitators of implementation will support development of strategies for successful uptake of weighted blankets (Wright et al., 2023). In addition to drawing on implementation strategies presented in this article, clinicians can apply implementation theories to inform quality improvement projects in clinical practice. For example, the TDF checklist or interview could be used as a guide to assess readiness for implementation and then map the key issues against the Behavior Change Wheel (COM–B) to devise tailored implementation strategies (Atkins et al., 2017). As such, implementation theories can be used to design the implementation strategies for an intervention and address staff capability (e.g., through education or mentoring), opportunity (e.g., by ensuring availability of resources), and motivation (e.g., through modeling; Michie et al., 2014).
Nonpharmacological sleep intervention options are increasingly recommended for a range of patient groups, including people experiencing chronic pain (Becker et al., 2018) and children with neurodisabilities with sleep disturbance (Scantlebury et al., 2018). Dementia care protocols and guidelines recommend nonpharmacological approaches as the first treatment option (National Health and Medical Research Council, 2016), and there are calls for reduction or elimination in use of restrictive practices (including chemical restraint) in a range of contexts (Baker et al., 2021; Royal Commission Into Aged Care Quality and Safety, 2021). Given the weak evidence for sleep medications (Sateia et al., 2017) and potential harms for some patient groups (National Health and Medical Research Council, 2016; Scantlebury et al., 2018), weighted blankets are an alternative option. Occupational therapists should advocate for nonpharmacological sleep interventions for clients across a range of health care settings (Enam et al., 2023).
Limitations of the Review
Although the detailed implementation strategies were predominantly derived from one study (Dawson et al., 2022), these strategies aligned with findings from two other relevant studies that examined ways to promote staff optimism and intention to use weighted blankets, including using personalized safety plans (Wright et al., 2020) and using education to address staff concerns about risks (Wright et al., 2023). Because these studies were all situated within adult mental health service contexts in Australia, the interpretation and translation of these strategies into settings and populations beyond these settings should be done with caution. Future studies should consider using hybrid designs to examine both clinical effectiveness and implementation (Curran et al., 2012).
Implications for Occupational Therapy Practice
The findings of this scoping review have the following implications for occupational therapy practice: Overnight use of weighted blankets can be recommended for adults to improve sleep and mood and to reduce pain and medication use. Overnight use of weighted blankets may be trialed with children based on child and caregiver preferences under supervision. Successful implementation requires protocols that define the intervention (purpose, blanket weight or type, clinician role, safety considerations) and development of tailored strategies for uptake or use.
Conclusion
Findings from this scoping review can be used to inform occupational therapists’ clinical decision-making and the future development of practice guidelines for overnight use of weighted blankets. The findings show that weighted blankets are being used as a sleep intervention option for individuals presenting with a range of health problems. Current evidence regarding effectiveness indicates more evidence for weighted blanket use for adults than for children and adolescents. Recommendations regarding implementation or use of weighted blankets focused on staff knowledge. Other facilitators of use included professional role and identity, social influences, and the environmental context and resources. Further explorations of weighted blankets as a sleep intervention should occur in daily clinical practice as well as through more rigorous research, including hybrid trials that examine effectiveness and implementation.
Supplemental Material
Supplementary material for Weighted Blankets as a Sleep Intervention: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050676.pdf for Weighted Blankets as a Sleep Intervention: A Scoping Review by Suzanne Dawson, Kimberly Charlton, Lorraine Ng, Jenny Cleland, Lemma Bulto, Michael Page and Stacie Attrill in The American Journal of Occupational Therapy
Footnotes
*Indicates articles included in the scoping review.
Acknowledgments
We acknowledge Josephine McGill from Flinders University Library Services for support with developing and running the search.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.