
Abstract
This study provides important insights into early interventions by occupational therapists and the impact on children with developmental delay and parent-child interactions.
Developmental delays (DD) are characterized by a significant delay of 25% or more from the expected rate in one or more areas of development, such as sensory, cognitive, gross, and fine motor skills; communication and personal–social skills; and daily life activities (Bellman et al., 2013; Shevell et al., 2005). Among children younger than age 5 yr, 12% to 16% have a delay in at least one developmental area (Tonelli et al., 2016). In early childhood, language development problems occur among approximately 5% to 12% of children (median = 6%; Law et al., 2000; Wallace et al., 2015), learning difficulties are present among about 8% (Rittey, 2003), and cognitive dysfunction is observed in about 14.3% of 2-yr-old children (Rosenberg et al., 2008). Additionally, children at risk for DD are also at risk for behavioral problems (e.g., social–emotional, interactions; Rydz et al., 2006). DD may be temporary or permanent (Tonelli et al., 2016), and children with permanent DD are at risk for learning disabilities, behavioral problems, and functional disorders later in life (Keogh et al., 2004). The design and delivery of early intervention programs to improve the developmental outcomes of infants with DD and a neurodevelopmental disorder have gained importance (Inguaggiato et al., 2017; Kohli-Lynch et al., 2019). Early intervention includes services provided to children ages birth to 3 yr to improve health and well-being, develop emerging skills, minimize DD, address existing or emerging disabilities, prevent functional impairments, and promote parental adjustment (Blauw-Hospers & Hadders-Algra, 2005).
In the literature, it is often observed that early intervention programs are primarily directed toward premature infants and those diagnosed with cerebral palsy (CP; Harbourne et al., 2021; Morgan et al., 2014; Wu et al., 2019). The most frequently used early intervention approaches are neurodevelopmental therapy (NDT; Klimont, 2001; Law et al., 1997); Goal–Activity–Motor Enrichment (GAME; Morgan et al., 2014, 2016; Wu et al., 2019); the Supporting Play, Exploration, and Early Development Intervention (SPEEDI; Dusing et al., 2020; Finlayson et al., 2020); and the Infant Behavioral Assessment and Intervention Program (IBAIP©; Meijssen et al., 2010; Verkerk et al., 2012). Early intervention approaches have mostly focused on motor training (Morgan et al., 2021), parent education (Finlayson et al., 2020; Morgan et al., 2014), environmental enrichment (Dusing et al., 2020), participation support (Colyvas et al., 2010; Mobbs et al., 2022), and home visits (Brorson, 2005; Salisbury & Cushing, 2013). In addition, therapists have frequently used home-based (Bann et al., 2016) and routine-based (Hwang et al., 2013) approaches with children with DD, or they have used sensory-enriched environmental programs, such as Interdisciplinary Sensory-Enriched Early Intervention (ISEEI; Blanche et al., 2016).
In addition to providing early intervention strategies tailored to specific themes for children with CP or at high risk of prematurity, the literature emphasizes the importance of adopting a holistic perspective when assessing development, recognizing the interconnected nature of sensory, cognitive, and motor outcomes (Başar, 2012; de Paula Machado et al., 2019). Despite this, early intervention studies have often focused predominantly on motor skills, neglecting the integral roles of sensory and cognitive abilities. To address this gap in research and practice, we implemented a comprehensive early intervention program for children with DD that incorporates the GAME approach’s principles of intensive motor training, parent education, and environmental enrichment, as well as a range of activities that promote sensory and cognitive development. GAME is an early intervention program for children at high risk for CP developed by Morgan et al. (2014). Previous studies have focused on GAME’s effects on motor and cognitive skills (Morgan et al., 2014, 2016). In our study, this approach was used for the first time with children with DD, in addition to focusing on sensory processing and parent–child interactions.
Notably, children with DD face an elevated likelihood of behavior problems, including challenges in social–emotional and interactive domains (Reynolds et al., 2007; Steenis et al., 2015). Despite this heightened risk, a research gap exists concerning the natural reinforcement contingencies experienced by children with DD in diverse environments. Although parent and child behavior is recognized to vary according to context (Holden & Miller, 1999), surprisingly little research has explored spontaneously occurring parent–child interactions across different situations (Humphrey, 2001; Lundqvist‐Persson et al., 2012). The lack of a sufficient number of studies on this topic is quite remarkable because these children have limited independent interaction with their environment and are largely dependent on their parents or caregivers to provide meaningful experiences (Agazzi et al., 2023; Blauw-Hospers & Hadders-Algra, 2005). Consequently, this study also investigated how the early intervention program influenced parent–child interactions.
There is a need in Türkiye for occupational therapists who focus on addressing parent-supported approaches (T.C. Aile ve Sosyal Hizmetler Bakanlığı, 2021). The outcomes of this study highlight the contribution to the comprehensive development of children with DD of a holistic occupational therapy program based on the principles of the GAME approach. In this study, we examined the effect of an early intervention program based on GAME principles led by an occupational therapist and a home program implemented by the parent on (1) developmental parameters (motor, cognitive, sensory, language, personal–social, and social–emotional skills) and (2) parent–child interaction among children with DD.
Method
Participants
This study was conducted in the Pediatric Rehabilitation Unit of Hacettepe University’s Faculty of Health Sciences, Department of Occupational Therapy, in collaboration with Hacettepe University’s Faculty of Medicine, Department of Pediatrics, Unit of Social Pediatrics. It targeted children ages 24 to 36 mo with DD. The inclusion criteria were as follows: DD as assessed with the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley III); ages 24 to 36 mo; having received no neurological, psychiatric, or orthopedic diagnoses; commitment to regular attendance in the intervention program; and engagement in assessments. Exclusion criteria were having been placed in institutional care and having received any neurological, psychiatric, or orthopedic diagnoses. The study received ethical approval from the Clinical Research Ethics Committee (Decision 2015-KAEK-71-22-0.1). Primary parents were informed, and their verbal and written consent was obtained before the initial assessment. The trial was registered with ClinicalTrials.gov (Identifier NCT06052410).
Sample
On the basis of a Cohen’s effect size of 0.20, meaning that there would be a 0.20 difference between the two repeated measurement scores, the required sample size for this study was determined to be 52 with 80% power, using G*Power (Version 3.1.9.4; Faul et al., 2007). A total of 89 children diagnosed with DD on the basis of results from the Bayley III, administered by a developmental pediatrician, were referred to Hacettepe University, Faculty of Health Sciences, Department of Occupational Therapy. The parents of 3 children did not want to participate in the study, and 4 were not included because they were older than 36 mo. Using a simple random assignment method, numbers from 1 to 82 were randomly assigned, and with the help of the online randomization application at https://www.randomizer.org/, the 82 remaining hildren were divided into an intervention group (n = 41) and a control group (n = 41). Subsequently, 11 children in the intervention group withdrew from the study in the middle of the 12th wk for various reasons. One child in the control group was excluded from the study because the final evaluations could not be completed. A total of 70 children completed the study (intervention group, n = 30; control group, n = 40). The CONSORT guidelines for randomized controlled trials (Schulz et al., 2010) were followed in designing the study (Figure 1).
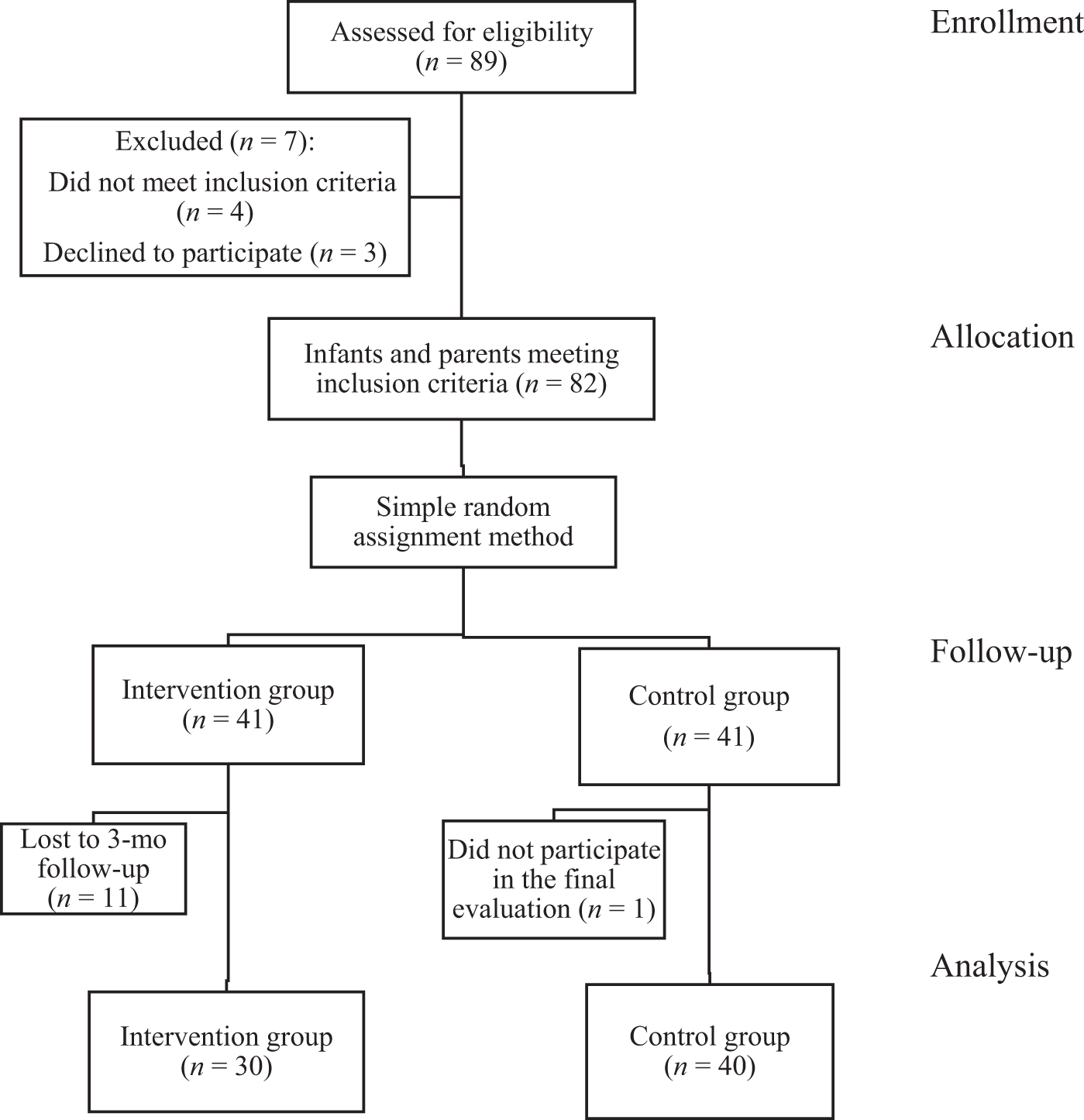
Consolidated Standards of Reporting Trials (CONSORT) flow diagram illustrating the flow of participants through the study.
Measures
The Bayley III and Ages and Stages Questionnaires (ASQ) were used to assess developmental domains, the Infant/Toddler Sensory Profile 2 (ITSP–2) to assess sensory development, the ASQ:Social–Emotional (ASQ:SE) to assess social–emotional development, and the Parenting Interactions with Children: Checklist of Observations Linked to Outcomes (PICCOLO™) to assess parent–child interactions. These evaluations were performed face-to-face in the pediatric occupational therapy clinic before and after the intervention.
Sociodemographic Information Form
The parents participating in the study provided information about their children, including whether the birth was premature, the child’s age, corrected age for premature infants, gender, and birth order. Information about the parents was also recorded, including the mother’s and father’s ages, maternal and paternal education levels, and parent income level.
ITSP–2
The Infant/Toddler Sensory Profile 2 (ITSP–2; Dunn, 2014) is an assessment tool developed to evaluate sensory processing skills in children ages 7 to 35 mo. It consists of a total of 54 items that specifically provide a profile of children’s fundamental sensory and behavioral reactions, particularly for those who have just started walking. It provides results in terms of four quadrants (Seeking, Sensitivity, Registration, and Avoiding) and six sensory sections (General, Auditory, Visual, Tactile, Vestibular, Oral, and Behavioral Responses). The sensory sections assess how the child responds to stimuli in each sensory system. The questionnaire is completed by the parent. The researcher administered this test to parents twice, before and after the intervention, using a 5-point scale for scoring (5 = almost always, 4 = often, 3 = sometimes, 2 = rarely, 1 = almost never, 0 = not applicable). The Turkish validity and reliability of this test demonstrate high test–retest reliability (intraclass correlation = .95) and excellent internal consistency (Cronbach’s α = .95) for all sensory systems (Uzer, 2018).
Bayley III
The Bayley III is an assessment tool designed to evaluate the developmental functions of infants and young children ages 1 to 42 mo (Bayley, 2006). The primary purpose of the test is to identify children with DD and provide practitioners with information for intervention planning (Albers & Grieve, 2007). The Bayley III is primarily used to assess cognitive, motor, and language domains. Test items are scored as 0 (unable to perform the skill) or 1 (able to perform the skill). A starting point score is determined on the basis of the child’s age, and the test continues until five consecutive scores of 0 are obtained. The raw score is then converted to a scaled score and a composite score on the basis of the child’s age. A composite score higher than 89 indicates normal development, 80 to 89 suggests below-average development, 70 to 79 indicates borderline development, and 69 or lower signifies very poor and high-risk development (Albers & Grieve, 2007; Bayley, 2006; Kaya-Kara et al., 2019; Smith et al., 2024).
ASQ
The ASQ (Squires & Bricker, 2009) is an assessment tool developed to evaluate the development of children ages 3 to 72 mo. It can be completed by caregivers or teachers who know the child. The ASQ assesses various areas of development, including communication, fine and gross motor skills, problem-solving, and personal–social development. The person completing the form is asked to mark the “yes” box if the skill is performed, the “sometimes” box if it is performed occasionally, and the “not yet” box if it has not yet been achieved. “Yes” is assigned 10 points, “sometimes” is assigned 5 points, and “not yet” is assigned 0 points (Squires & Bricker, 2009). Each developmental area has a cutoff score based on the child’s age. If the child scores below the cutoff value, their development is considered problematic; if they score at or above the cutoff value, their development is considered normal (Squires & Bricker, 2009). The Turkish validity and reliability of the ASQ were validated by Kapci et al. (2010). Cronbach’s α values ranged from .38 (4 mo) to .95 (36 mo) for Communication, .61 (6 mo) to .93 (18 and 22 mo) for Gross Motor, .63 (16 mo) to .93 (60 mo) for Fine Motor, .44 (20 mo) to .93 (60 mo) for Problem-Solving, and .50 (16 mo) to .90 (60 mo) for Personal–Social (Kapci et al., 2010).
ASQ:SE
The ASQ:SE was developed by Squires et al. (2002) as an addition to the ASQ (Baker & Feinfield, 2003). The ASQ:SE assesses social–emotional behaviors in the areas of self-regulation, communication, adaptive behavior, independence, emotions, and interaction. This form is also completed by caregivers, and items are marked as often, sometimes, or rarely/never. Each item is accompanied by a symbol—0 (0 points), V (5 points), or X (10 points)—that indicates the scoring direction for the item. Similar to the ASQ, the child’s development is classified as problematic or normal on the basis of the cutoff score (Kapçı et al., 2007; Squires et al., 2002). The validity and reliability of the Turkish version of the ASQ:SE were validated by Kucuker et al. (2011). Cronbach’s α values ranged from .67 to .91.
PICCOLO
To evaluate parent–child interaction, approximately 10-min video recordings taken by parents while they played with their children were sent to us and evaluated by a certified occupational therapy researcher (Ezginur Gündoğmuş) using the Turkish version of the PICCOLO. The PICCOLO was developed by Roggman et al. (2013) and validated in Turkish by Bayoğlu et al. (2013). It includes a checklist of 29 observable behaviors. The aim was to analyze parents’ interactions with children in four domains: Affection, Responsiveness, Encouragement, and Teaching. Each of the four PICCOLO domains consists of seven to eight items; each item includes a short label for and a more detailed description of an observable parenting behavior. Each item is scored as follows: 0 (none, no observable behavior), 1 (barely, brief, minor, or newly emerging behavior), or 2 (clear, definite, strong, or frequent behavior). The optimal PICCOLO total score is 42 or above, and the optimal score for the Affection, Responsiveness, and Encouragement domains is 11 or above. For the Teaching domain, a score of 9 or higher is considered optimal (Bayoğlu et al., 2013).
Compliance Checklist
Compliance with the home program was monitored in both groups through a weekly checklist completed by parents to ensure that the intervention group received 36 hr of the home program and the control group received 60 hr. On the checklist, parents marked an X on the days they performed the activities.
Interventions
Intervention Group
Children in the intervention group received an early intervention program based on the principles of the GAME approach. In addition to GAME protocols, the intervention included client-centered sensory and cognitive activities based on the child’s initial assessment results. The program was delivered by the first author (Gündoğmuş), an expert occupational therapist, in a pediatric clinic 1 hr/day, 2×/wk, for 12 wk, for a total of 24 hr.
In addition to this program, the intervention group also received an individualized home program based on the results of the developmental assessments. The home program was implemented by the children’s parents in their own homes 1 hr/day, 3×/wk, for 12 wk, for a total of 36 hours. Parents contacted the occupational therapist via WhatsApp or phone calls (Novak et al., 2009; Temiz et al., 2023). Parents’ adherence to the home program was monitored via phone calls, WhatsApp, and the weekly compliance checklist forwarded to the occupational therapist. The home program was prepared by considering the criteria suggested for the success of home programs. These criteria include checking whether the parent has received a home program before, not overloading the parents, making sure that the parents are willing to participate in the home program, cooperating with the parents on activities and goals, making the activities more suitable for daily life, reducing the number of activities to six, providing the parents with the necessary time to implement the program, and calling the parents by phone. Final evaluations were conducted after 12 wk. The intervention group’s home program was similar that of the control group. During phone calls with the occupational therapist, the families exchanged ideas about their difficulties, and the therapist provided coaching to the parents. The total intervention dose was 60 hr.
GAME approach.
The GAME approach is an early intervention strategy developed by Morgan et al. (2014). The basic principles of the GAME approach can be divided into three parts (Morgan et al., 2014, 2015): goal-focused intensive motor training, parent education, and environmental enrichment.
Goal-focused intensive motor training.
The first parameter of the GAME approach is goal-focused intensive motor training. Parents and therapists collaborate to determine goals for motor skill development. In our study, the goals created in collaboration with parents included activities consisting of motor, sensory, or cognitive development areas—for instance, playing with tactile sensitivity–reducing materials such as shaving foam, jumping in place on a trampoline, and placing geometric objects, such as triangles and rectangles, in their appropriate locations. During this part of the GAME approach, the therapist assisted parents in setting realistic goals that were appropriate for the child’s developmental level; as the child achieved these goals, new ones were determined in collaboration with parents. As the child’s performance of activities improved, the difficulty was increased by adjusting the activity or the environment. Parents were involved in therapy sessions, and they were provided with information on how to work on the skills they wanted the children to acquire (Morgan et al., 2014; Tetreault et al., 2003).
Parent education.
Family education is the second parameter of the GAME approach. Parents are educated on how to encourage the emergence of intentional movements in their children and how to promote progress. It is essential to discover the time periods in which children are most suitable for and receptive to therapy. In our study, the education provided to parents included giving children opportunities for trial and error, creating and sustaining effective play with minimal materials in the home environment, and encouraging the skill development and providing different activities to achieve the targeted skills and goals. This education was provided to the family at the beginning of the program.
Environmental enrichment.
The third parameter of the GAME approach is environmental enrichment. Within the scope of the GAME approach, assessing the home environment includes helping to create motor-enriched play environments to support the child’s self-produced movements, discovery, and task success in the natural learning environment. In our intervention, parents were provided with examples of materials and were supported in working with different materials at home. The environmental richness of the home environment was assessed remotely using the necessary visuals and videos sent by the parents, and feedback was provided by the occupational therapist via WhatsApp and phone calls. Ayres Sensory Integration® (ASI) approach principles were used as a basis for planning the activities. These environmental arrangement recommendations were given at the beginning of the program.
Sensory-based activities.
Sensory-based activities were crafted in accordance with the ASI theory, with the aim of delivering personalized and regulated sensory experiences. The goal was to assist in moderating individual responses to environmental stimuli (Ayres & Robbins, 2005; Baranek, 2002). These interventions specifically addressed hyper- or hyposensitivities. The fundamental rationale behind the use of sensory-based treatments is to enhance sensory processing, promote self-regulation, increase adaptive functioning, and facilitate the child’s active participation in daily activities (Ayres & Robbins, 2005). In this study, sensory-based activities were used to construct an environment featuring sensory stimuli that were centered around the child, planned at an appropriate level, controlled, and customized to the child’s specific needs. The objective was to offer sensory stimulation and encourage active participation by creating an environment carefully designed to present an optimal level of challenge for the child.
Cognitive-based activities.
In this study, cognitive skills related to the child’s learning of activities were addressed within the activities. These skills included attention, memory, orientation, problem-solving, motor planning (praxis), visual perception, visual attention, visual memory, object relations, perceptual–motor skills, learning, and executive functions. For this purpose, activities and materials, such as memory cards, boxes for matching geometric shapes, visual matching, and plug-ins, were added to the activities.
The session plan for the intervention group was as follows: ▪ Week 1 Session 1: The therapist performed basic sensory interventions, taking into account the child’s sensory profile. Session 2: The therapist continued basic sensory interventions, determined activities that need to be practiced at home, and provided parents with education on skill areas. ▪ Weeks 2 to 4 Sessions 3 to 8: The therapist continued basic sensory interventions and gradually increases the difficulty level of the activity. The therapist provided feedback on environmental enrichment as seen in the photos and videos sent by the parent remotely and through communication tools (phone calls, WhatsApp). ▪ Weeks 5 to 12 Sessions 13 to 28: The therapist performed sensory, motor, and cognitive skill–based interventions, prioritizing the child’s active participation, implementing activities in accordance with each child’s developmental performance level, and continuing to monitor environmental enrichment through communication tools.
Final evaluations were performed after 12 wk.
Control Group
The control group completed the same assessments as the intervention group. According to the evaluation results, an individualized home program was prepared by an occupational therapist (Gündoğmuş). The control group received the home program only, which was delivered by their parents for 1 hr/day, 5×/wk, for 12 wk. The total intervention dose was 60 hr.
The occupational therapist was in touch with the parents via WhatsApp, phone calls, and the compliance checklist. Parents exchanged ideas with the occupational therapist via phone calls about any difficulties they had, and the therapist provided coaching on these issues. The parents indicated their engagement in activities by marking an X on the compliance checklist, which was then forwarded to the occupational therapist after the interventions.
The home programs were similar to those of the intervention group; they included activities specific to each skill area (sensory, motor, cognitive, communication) and were individually prepared by the occupational therapist, taking into account the criteria recommended for the success of home programs. These criteria include checking to see whether the parent has received a home program before, not placing an excessive burden on the parents, making sure that parents are willing to participate in the home program, collaborating with parents to decide on activities and goals, making the activities more suitable for daily life, making the number of activities fewer than six, providing parents with the necessary time to implement the program, and making phone calls to parents. This approach aimed to provide a structured and supportive environment for both groups, address the developmental needs of at-risk children, and enable parents to actively participate in the intervention process (Squires et al., 2002). Sensory and cognitive activities consisted of examples of activities that the family could implement at home—for example, playing with shaving foam for a child with tactile sensitivity. The home program was implemented by the parents for 12 wk, and final evaluations were performed after 12 wk.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics (Version 23.0). Continuous variables were summarized using means and standard deviations, and categorical variables were summarized as frequencies and percentages. The data distribution was examined using histogram, kurtosis, skewness, and the Kolmogorov–Smirnov test. On the basis of the distribution characteristics, median and interquartile ranges (IQR) or means and standard deviations are presented. Group differences were also analyzed.
The absolute change was calculated in the follow-up period for task scores as follows:
Differences between groups in absolute values were examined using generalized linear models, adjusting for mother–child pair characteristics (maternal age and education, household income, number of children [one or more than one], child’s age, child’s gender, presence of prematurity). Means and Wald 95% confidence intervals (CIs) were calculated. Within-groups changes over time and between-groups differences in test scores (Time × Group interaction) were evaluated through repeated measures using the generalized linear model while accounting for mother–child pair characteristics. Means and 95% CIs were calculated.
The difference in the frequencies of typical ITSP–2 subscores, based on the implementation of occupational therapy home intervention, was calculated using logistic regression, controlling for the same mother–child pair characteristics. Odds ratios and 95% CIs were calculated.
For all analyses, p < .05 was considered statistically significant.
Results
Eighty-nine participants were evaluated for eligibility, and 70 completed the study. The participants were randomly assigned to the intervention group (n = 30) or the control group (n = 40). At baseline, the average age of the children in the intervention group was 30.70 mo (SD = 2.61 mo); 46.7% were premature, and 73.3% were male (n = 22). The average age of children in the control group was 30.60 mo (SD = 3.11); 40.0% were premature, and 65.0% were male (n = 26). The sociodemographic information of the children and parents participating in the study is provided in Table 1.
Demographic Characteristics of the Participants
Developmental Domains and Parent–Child Interactions
The preintervention means and standard deviations, median and interquartile range, and scores indicating pathology of the two groups are given in Table A.1 in the Supplemental Material, which is available online with this article at https://research.aota.org/ajot. The two groups’ scores at admission and postintervention are given in Table 2. There was a statistically significant postintervention difference between the two groups on the Bayley III in all areas of development evaluated (p < .001). The absolute change in Bayley III scores varied from 0.3 to 7.4 in the control group, whereas it varied from 2.8 to 20.4 in the intervention group. On the ASQ and ASQ:SE, absolute change varied from 5.2 to 19.8 in the control group, whereas it varied from 17.7 to 68.3 in the intervention group. In terms of ASQ and ASQ:SE scores, there was a statistically significant difference between the two groups in Gross Motor, Fine Motor, Problem-Solving, and Social–Emotional scores (p < .05). For the PICCOLO, although the absolute change varied from 20.9 to 48.5 in the control group, it varied from 39.2 to 100.5 in the intervention group, and a significant between-groups difference was found on all parameters evaluated (p < .001).
Bayley III, ASQ and ASQ:SE, and PICCOLO Scores on Admission, After Intervention, and Absolute Change at Follow-Up
Note. Unless otherwise indicated, values are means and Wald 95% CIs. Values labeled with different lettered subscripts indicate significant differences (p < .05) in pairwise comparisons; those with the same lettered subscript indicate no significant differences. p values for on admission and after intervention were determined through repeated-measures GLM after adjusting for mother–infant pairs; p values for absolute change were determined through GLM controlling for mother–infant pairs. ASQ = Ages and Stages Questionnaires; ASQ:SE = Ages and Stages Questionnaires:Social–Emotional; Bayley III = Bayley Scales of Infant and Toddler Development Third Edition; CI = confidence interval; GLM = generalized linear modeling; PICCOLO = Parenting Interactions with Children: Checklist of Observations Linked to Outcomes.
aValues are M [95% CI].
ITSP–2 Scores
The preintervention means and standard deviations, medians and interquartile ranges, absolute differences, probable differences, and typical performance percentages on the ITSP–2 of the two groups are given in Table A.2 of the Supplemental Material. The typicality rates of ITSP–2 test scores between the two groups postintervention are given in Table 3. The intervention group showed 6.2 times more typification (normal sensory processing) in Sensory Seeking, 9.9 times more in Avoidance, 12.4 times more in Low Registration, and 20.3 times more in General Processing compared with the control group.
Differences in the Frequencies of Typical ITSP–2 Subscale Scores by Group
Note. Each subscale was compared with multiple logistic regression after controlling for confounding factors. Significant correlations are shown in bold. ITSP–2 = Infant/Toddler Sensory Profile 2.
*p < .05.
Compliance
Both groups were 100% compliant with the home programs.
Discussion
This randomized controlled study demonstrated the effectiveness of the GAME-based intervention in fine motor and cognitive development. It also showed significant differences between the intervention group and the control group in sensory skills, receptive language, gross motor skills, personal–social development, social–emotional development, and parent–child interaction.
Clinic-Based Intervention and Home Program Versus Home Program Only
In this study, the intervention group showed significant improvements in most outcome variables compared with control group. In a study conducted by Wu et al. (2014) with a sample similar to that of our study, infants at risk of DD were divided into three groups: a clinic-based intervention program, a home-based intervention program, and an intervention program involving standard practices. Similar to our study’s results, Wu et al. (2014) found that the clinic-based early intervention program was more effective in the development of cognitive skills, and infants showed a lower rate of motor delay. In another study (Altunalan et al., 2023), home program practices, including family education with a clinic-based early intervention approach, were compared with the NDT approach alone. The authors reported that clinic-based early intervention combined with a home program resulted in improvements in children’s cognitive functions and expressive language skills. In our study, we found significant improvements in parent–child interaction in the intervention group, who received a home program in addition to clinic-based interventions. Our research fills a gap in knowledge regarding service delivery for children with DD by demonstrating positive changes in development and parent–child interactions resulting from consistent provision of therapeutic activities in the home setting combined with strong parent education in a clinic-based intervention.
GAME Approach
A single-blind, randomized controlled study using the GAME early intervention program examined its effect on developmental outcomes among premature infants with DD and found significant improvements in the areas of motor and cognitive development in the GAME group (Morgan et al., 2016). Although there is increasing evidence that children with DD experience sensory processing difficulties (Blanche et al., 2016; Wickremasinghe et al., 2013), early intervention approaches, such as GAME, SPEEDI, and IBAIP, developed in the field of early intervention in recent years, appear to ignore sensory processing problems and do not address sensory strategies. Our study attempted to fill this gap by addressing sensory processing issues in the intervention group with a GAME-based clinical intervention. NDT combined with parent-centered physiotherapy may not be enough to improve motor and cognitive performance in preterm infants (Elbasan et al., 2017).
Another study compared the Family Collaborative Approach (FCA) and NDT-based family training (Adiguzel et al., 2023). These authors found that FCA at home in the early period was more effective than the NDT in the short and long terms. A study conducted by Harbourne et al. (2021) showed that the Sitting Together and Reaching to Play early intervention program, which they developed on the basis of observations of infants with motor delays, resulted in significant improvements in cognitive and fine motor skills among infants with severe motor delays compared with the control group. The group with mild motor delay had positive improvements in receptive language development. Van Hus et al. (2016) examined the effectiveness of the IBAIP program on cognitive and motor skills among patients born prematurely at less than 32 wk gestation and found significant improvements in motor skills but no change in cognitive skills. In their pilot study, Finlayson et al. (2020) applied the SPEEDI approach with infants born preterm. In this approach, which prioritizes parental education and environmental enrichment, the child’s developmental results are evaluated with the Bayley III. Infants in the SPEEDI group made more significant progress in gross motor, receptive language, and expressive language skills than the control group. Besios et al. (2018) examined the effect of the NDT approach on neurodevelopmental outcomes. However, in this study, the control group received no intervention. In another randomized controlled study (Elbasan et al., 2017) that used the NDT approach with at-risk infants, the age-matched control group received no intervention. In that study, no significant between-groups differences were observed in terms of motor and cognitive development.
In our study, similar to the outcomes of programs developed in recent years, we observed a significant improvement in the intervention group in all developmental areas as assessed with the Bayley III. On the parent-completed ASQ, improvements were noted for the intervention group in all developmental areas except Communication. We believe that this difference between the two tests may be attributed to parents’ high expectations regarding their infants’ communication skills. Furthermore, we believe that the difference in developmental areas between the groups indicates that activities performed solely by parents in a home program may not be sufficient, consistent with the literature. Unlike the environmental enrichment (Wu et al., 2019) and target-focused (Harbourne et al., 2021) literature, we posit that the impact on development stems from the use of activities targeting sensory, cognitive, and motor skills. We believe this is due to the provision of more intense sensory stimulation.
Sensory Activities
The findings of our study demonstrate that a GAME-based clinical intervention and home program, in addition to emphasizing interaction and shared participation with the infant, is effective in the development of sensory skills. The results we obtained in sensory skills development show that activities involving sensory-based interventions are effective in enhancing the child’s regulation process. Additionally, these activities have a positive impact on behavioral responses related to sensory processes, influencing the development of social–emotional skills, including parameters such as crying, calming, self-harm, expressing desires, and making eye contact. Similarly, Blanche et al.’s (2016) ISEEI program, which they implemented with children at risk for DD, dealt with sensory strategies that provide environmental enrichment; however, the study provided information only about their effects on developmental skills. Pekçetin et al. (2016) examined the effectiveness of a sensory integration intervention with premature infants. They found that the 8-wk intervention resulted in improvements in sensory processing problems in touch, deep pressure, vestibular and visual systems, and adaptive motor functions. Lecuona et al. (2017) examined the effect of the Ayres Sensory Integration® approach with premature infants in the first 12 mo. This study, which evaluated sensory development with the ITSP, found a significant increase in the number of children in the intervention group with typical performance in the areas of low registration, sensory sensitivity, sensory avoidance, and low neurological threshold behaviors.
According to our research, our study is the first to include sensory strategies in a GAME-based clinical intervention to improve sensory processing skills among children with DD. We found, similar to studies dealing with sensory integration, that children in the intervention group approach more typical performance—that is, normal sensory processing skills—in the Seeking, Avoiding, and Low Registration quadrants of the ITSP–2’s sensory quadrants and in general sensory processing. In our sessions, which began with analyzing the child’s sensory profile, different materials were used to stimulate the tactile, vestibular, and proprioceptive systems. Initially, children were regulated with sensory integration activities. Then activities for motor and cognitive skills were added to support other developmental areas. In addition, we observed that the intervention group program increased general sensory processing skills, demonstrating that our intervention results in significant improvements in both behavioral and sensory responses related to the sensory process. Unlike other studies, in our study, meaningful sensory activities, including cognitive and motor skills, were presented to the children according to the children’s sensory profiles. Thus, we believe that, among infants with DD, sensory processing difficulties, activity avoidance, inconsistency in response to stimuli, and intense stimulus-seeking behaviors decrease, and there is progress toward typical development.
Cognitive Activities
In our study, unlike in traditional early intervention programs, basic cognitive skills, such as attention, memory, visual perception, problem-solving, and executive functions, were supported in activities (e.g., placing geometric shapes in the appropriate space, matching memory cards, playing plug-and-play puzzle games, symbolic play activities) in accordance with level of development of the infant’s cognitive skills. Our results indicated that the infants in the intervention group had better cognitive skills development.
Bann et al. (2016) examined the effectiveness of a home-based early developmental intervention on cognitive development among infants at risk for DD. In addition to this intervention, which was based on parent education and home visits, parents in the intervention group also received health education, whereas the control group received only health education. Compared with the control group, children in the intervention group showed significant increases in cognitive skills development. In a randomized controlled trial, Hwang et al. (2013) examined the effect of a routine-based early intervention program versus traditional home visits among 5- to 30-mo-old infants at risk for DD. Both approaches resulted in significant increases in cognitive skills. Verkerk et al. (2012) examined the effectiveness of IBAIP on cognitive and motor skills among infants born prematurely at less than 32 wk. Although significant improvements were observed in motor skills, there was no improvement in cognitive skills. In their randomized controlled study, Wu et al. (2014) divided 24-mo-old infants at risk of DD into three groups: clinic-based intervention program, home-based intervention program, and intervention program with standard practices. The clinic-based early intervention program was more effective in the development of cognitive skills than the other programs, and the infants showed a lower rate of motor delay.
Although there are studies in the literature that have examined the effect of early intervention approaches on cognitive skills, we found no study that integrated cognitive skills into the early intervention program, as our study did. In this respect, we think our study is important.
Parent –Child Interaction
Little is known about parent–child interaction and its impact on children with significant delays in cognitive and motor development (Nakken & Vlaskamp, 2007; Van Keer & Maes, 2018). In this study, the PICCOLO was used to assess parent–child interaction during unstructured play via 10-min videos. At baseline, both the intervention and the control groups showed difficulties with affection, responsiveness, encouragement, and teaching. After the intervention, parent–child interaction increased more in the intervention group compared with the control group. Initially, the intervention group had higher PICCOLO scores, which we attribute to the lower age and higher education level of the mothers.
Van Keer and Maes (2018), using a assessment method similar to that of our study, used 10-min videos taken during unstructured play to evaluate parent–child interaction among typically developing children. Parents were found to be sensitive to their children, with children visually attending for less than half of the time, occasionally displaying gestures and active play behaviors, and these behaviors varied on the basis of the children’s developmental level (Van Keer et al., 2019). Passey and Feldman (2004) also noted the presence of behavioral problems among children with DD, indicating that parents’ attention to and engagement with their children, particularly in play, could influence the rate of such problems. In our study, we found significant improvements in parent–child interactions for both groups, but the intervention group showed more change than the control group. We think this is because parent education was more intensive in the intervention group because of the GAME approach. In the GAME protocol, parents are educated on how to encourage the emergence of intentional movements in their children and how to promote progress within the scope of parent education. This education provided parents with more information about their children. Similarly, Hackworth et al. (2018) found that provision of individualized parent support was important to all forms of engagement. In a study conducted by Bagner et al. (2009) with a single case using Parent–Child Interaction Therapy, parents aimed to increase their children’s positive social behaviors, decrease their negative behaviors, and teach skills to establish a secure relationship with them. Despite a reduction in children’s behavior problems in this study, Bagner et al. (2009) noted no changes in parent–child interaction.
In this context, our study comprehensively assessed and demonstrated changes in parent–child interaction. In addition, our study reveals the effect on parent–child interaction of occupational therapists’ involvement in parent-supported approaches within the scope of early intervention.
Limitations and Strengths
The limitation of this study might be the heterogeneity of PICCOLO values at admission. The strength of this study is that it is, to the best of our knowledge, the first randomized controlled early intervention study to address parent–child interaction among infants with DD. The results of this study will shed light on pediatric rehabilitation, literature, and clinical practices.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ In addition to motor-based activities, sensory- and cognitive-based activities should be added to early intervention programs. ▪ Parent–child interaction should be considered in early intervention studies. ▪ Providing education to parents increases parent–child interaction with at-risk infants. ▪ Providing clinic-based therapies along with a home program to children with DD can result in significant improvements in developmental parameters and parent–child interaction.
Conclusion
This study examined the effects of GAME-based clinical interventions on developmental domains and parent–child interaction among children with DD ages 24 to 36 mo. The results show that an early intervention program that includes activities that target sensory, cognitive, and motor skills, as well as parent education and environmental enrichment—the parameters included in the GAME approach—and a home program can be effective in improving all developmental domains and increasing parent–child interaction.
Supplemental Material
Supplementary material for Effect of Early Intervention on Developmental Domains and Parent–Child Interaction Among Children With Developmental Delay: A Randomized Controlled Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050706.pdf for Effect of Early Intervention on Developmental Domains and Parent–Child Interaction Among Children With Developmental Delay: A Randomized Controlled Study by Ezginur Gündoğmuş, Gonca Bumin and Sıddika Songül Yalçın in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This article is based on Ezginur Gündoğmuş’s master’s dissertation. We thank the children and their families who participated in this study.