
Abstract
This rapid review of the current literature provides practitioners with evidence on supports for school children with sensory processing challenges.
Sensory processing challenges affect the way the world is experienced in all areas of life, including schooling (Jones et al., 2020), and may result in functional difficulties. For example, a student who has difficulty filtering background noise may choose to withdraw from classroom activities—and in doing so may inadvertently reduce their access to learning opportunities and peer support. Within the general population, it is estimated that 5% to 14% of 4- to 6-yr-old children have a sensory processing challenge (Ahn et al., 2004), although rates within clinical samples are much higher. Studies suggest up to 90% of autistic people (Leekam et al., 2007) and 69% of people with attention-deficit hyperactivity disorder (ADHD; Parush et al., 2007) experience sensory processing challenges. Furthermore, 78% of autistic young people (ages 5–20 yr) reported experiencing difficulty in school, with almost half (46%) stating they required more support (Australian Bureau of Statistics, 2018). Studies have found that autistic children typically underachieve academically and experience high rates of school exclusion (Brede et al., 2017; Keen et al., 2016), with sensory processing challenges identified as a primary factor affecting poor educational outcomes (e.g., Ashburner et al., 2008; Jones et al., 2020). The identification of effective school-based interventions (henceforth, supports 1 ) for students with sensory processing challenges, therefore, is a discipline priority.
School-based supports for children with sensory processing challenges are often delivered by occupational therapists with the goal of enabling school access, participation, and achievement. These supports vary greatly, with some altering the physical environment (e.g., multisensory environments [MSEs]; Unwin et al., 2021a, 2021b) and others focusing specifically on the child (e.g., use of noise-canceling headphones; Ikuta et al., 2016). Sensory supports may also target an individual sensory modality, such as proprioception, audition, or vision, whereas others take a multisensory approach (e.g., sensory diets; Benson et al., 2020). For example, it is claimed that weighted vests focus on supporting a singular sensory modality (e.g., proprioception), which is hypothesized to provide organizing input to students’ adaptive systems (Deris et al., 2006), thereby creating a calming effect and improving classroom attention (VandenBerg, 2001). MSEs, conversely, seek to support students’ mood, self-regulation, and stimulation by modifying the physical environment across multiple sensory modalities, such as vision, touch, and audition. Although studies have been conducted to evaluate these approaches, the quality of these studies is often poor (Barton et al., 2015), and there are cases of conflicting research evidence for a given support (e.g., Fedewa et al., 2015 vs. Krombach & Miltenberger, 2020). The lack of quality data limits understanding of whether the support has a measurable impact on school outcomes for children (e.g., Barton et al., 2015). To enable practitioners to make evidence-informed judgments about the appropriateness of a given support, comprehensive evidence synthesis is required.
Several evidence reviews on the topic of sensory supports have been completed over the last decade (e.g., Barton et al., 2015; Bodison & Parham, 2018; Dargue et al., 2021). Although they offer valuable information to practitioners, current reviews are limited in utility because they assess only one type of outcome or support or lack specificity in defining the support setting (i.e., clinic vs. school). For example, some reviews have focused on the outcome of school participation (e.g., Grajo et al., 2020; Ouellet et al., 2021), but other important outcomes such as school access and academic achievement have not been considered. Other reviews have only focused on one kind of support, such as MSEs or weighted vests (e.g., Breslin et al., 2020; Taylor et al., 2017). Although these reviews are valuable in providing in-depth insights about one approach, they are of less value in providing practitioners with the broad overview needed to select the most appropriate support from the vast array available. The lack of specificity in past reviews in defining study settings similarly limits the utility of research findings for school-based practitioners (e.g., clinic; Bodison & Parham, 2018). Because the utility of support may vary across settings, recommendations for school-based practice should be drawn from literature considering school-based contexts. Therefore, we conducted a new, comprehensive evidence synthesis to address multiple relevant outcomes, the full range of supports, and school settings. Our research questions was, What school-based supports (including assessments) are effective in improving school access, participation, and achievement for students with sensory processing challenges?
Method
We used a Rapid Evidence Assessment (REA; discussed in Grant & Booth, 2009) approach following the Center for Evidence-Based Management guidelines (Barends et al., 2017). We used a “PICOC” mnemonic (i.e., Population, Intervention, Comparison, Outcome, Context) to ensure all aspects of the research question were captured in the search strategy. An example of the search terms can be found in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot). Searches were run by an independent librarian in multiple databases, including CINAHL Complete, Education Research Complete, ERIC, MEDLINE, PsycINFO, and Scopus. Inclusion and exclusion criteria are listed in Table 1.
Inclusion and Exclusion Criteria for the Rapid Evidence Assessment
We conducted the REA across three phases: (1) three separate literature searches, (2) data extraction and level of evidence assessment (see Table A.2 in the Supplemental Material), and (3) interpretation and synthesis (Table A.3 and Table A.4). All identified articles were imported into Covidence (2022) and screened for inclusion. One reviewer (Tennille Johnson) screened the title and abstract to assess the article’s eligibility for inclusion, and another researcher (Katy Unwin) screened the full texts of potentially eligible articles. To ensure reliability, each reviewer assessed 10% of the other’s decisions. Across all screening and full text examinations, both reviewers were highly consistent in their assessments (mean intraclass correlation coefficient = .92, p < .05).
The wide range in terminology used meant multiple iterative literature searches were run. The results of the initial search are displayed in Figure 1.
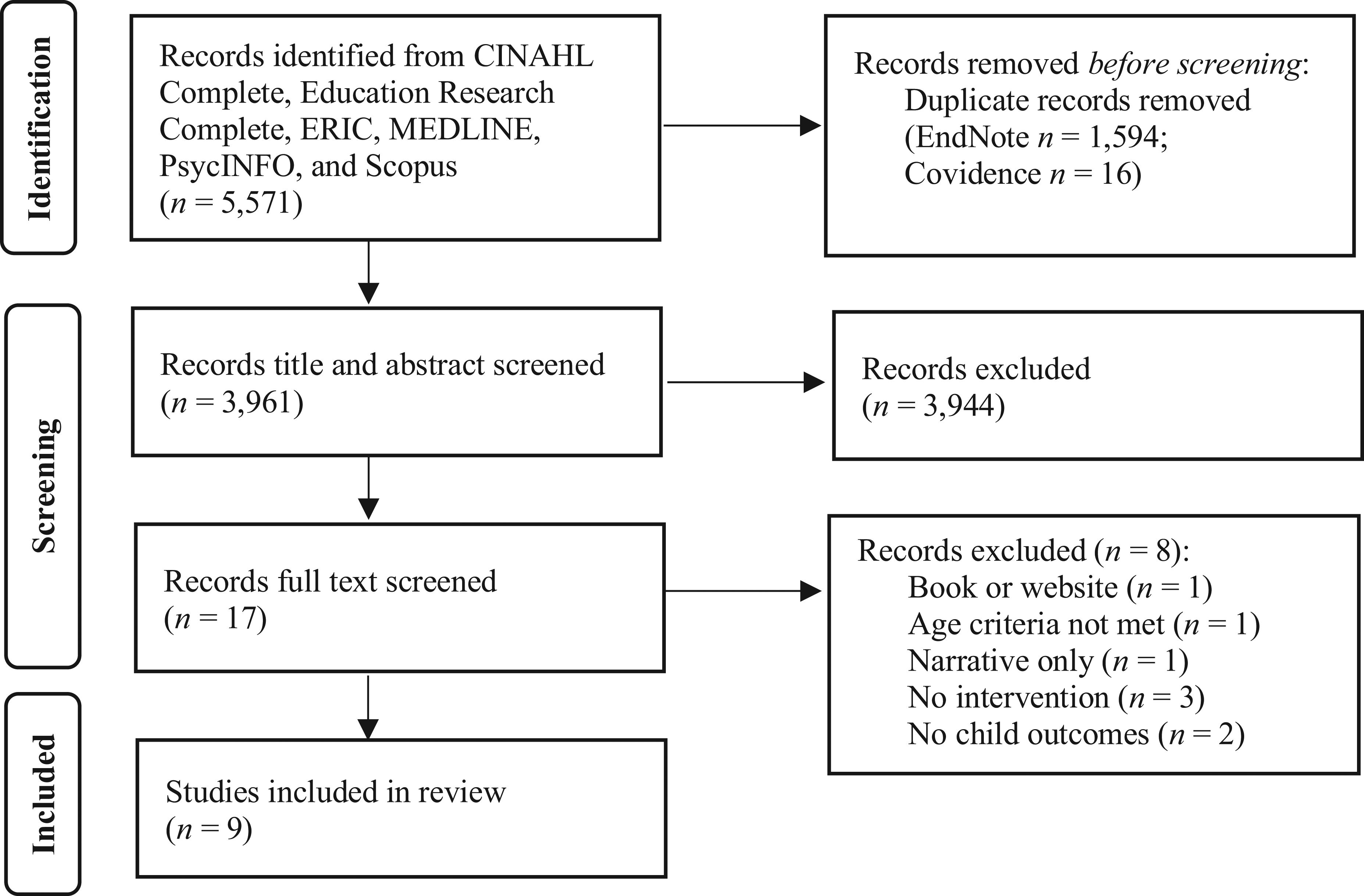
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow of study selection process from initial search before deduplication across the different searches.
We reviewed the identified articles and found that relevant articles were missing. Amendments to the search terms did not elicit any further articles. The original 2010 review (Department of Education and Training, Queensland, 2011) contained relevant articles (pre-2010) widely cited since; therefore, we conducted a second search by extracting all articles that cited articles contained in the 2010 review. We used Harzing’s Publish or Perish (Harzing, 2007) software to identify and store articles from Google Scholar citing the source articles from the 2010 review. Each article included in the 2010 review was then entered individually into Harzing’s Publish or Perish prior to extraction of the articles citing the original (source) articles. The resultant citations were extracted and uploaded to Covidence for screening (Figure 2). We again reviewed the resultant articles, identifying there was a missing literature on “multisensory environments.” This was most likely due to varied terminology used in this literature; therefore, a specific search was run with additional search terms (Figure 3). Articles from all three searches were combined (n = 66), and duplicates were removed (Figure 4). An updated search was run (April 2023) to capture articles published since the initial review, with 676 articles identified and screened; none, however, were eligible for inclusion.
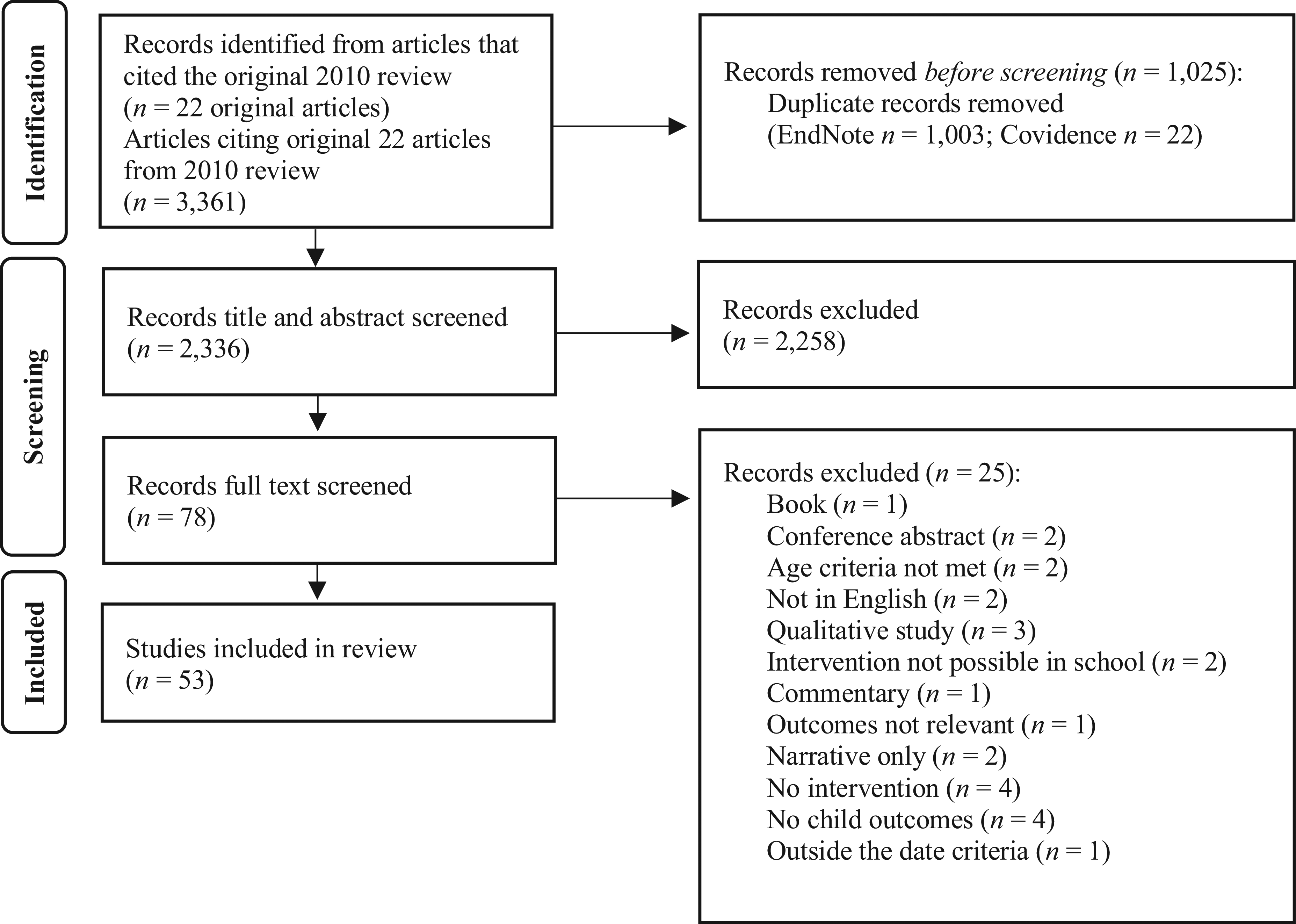
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow of study selection process of all extracted articles that cited the articles contained in the 2010 review.
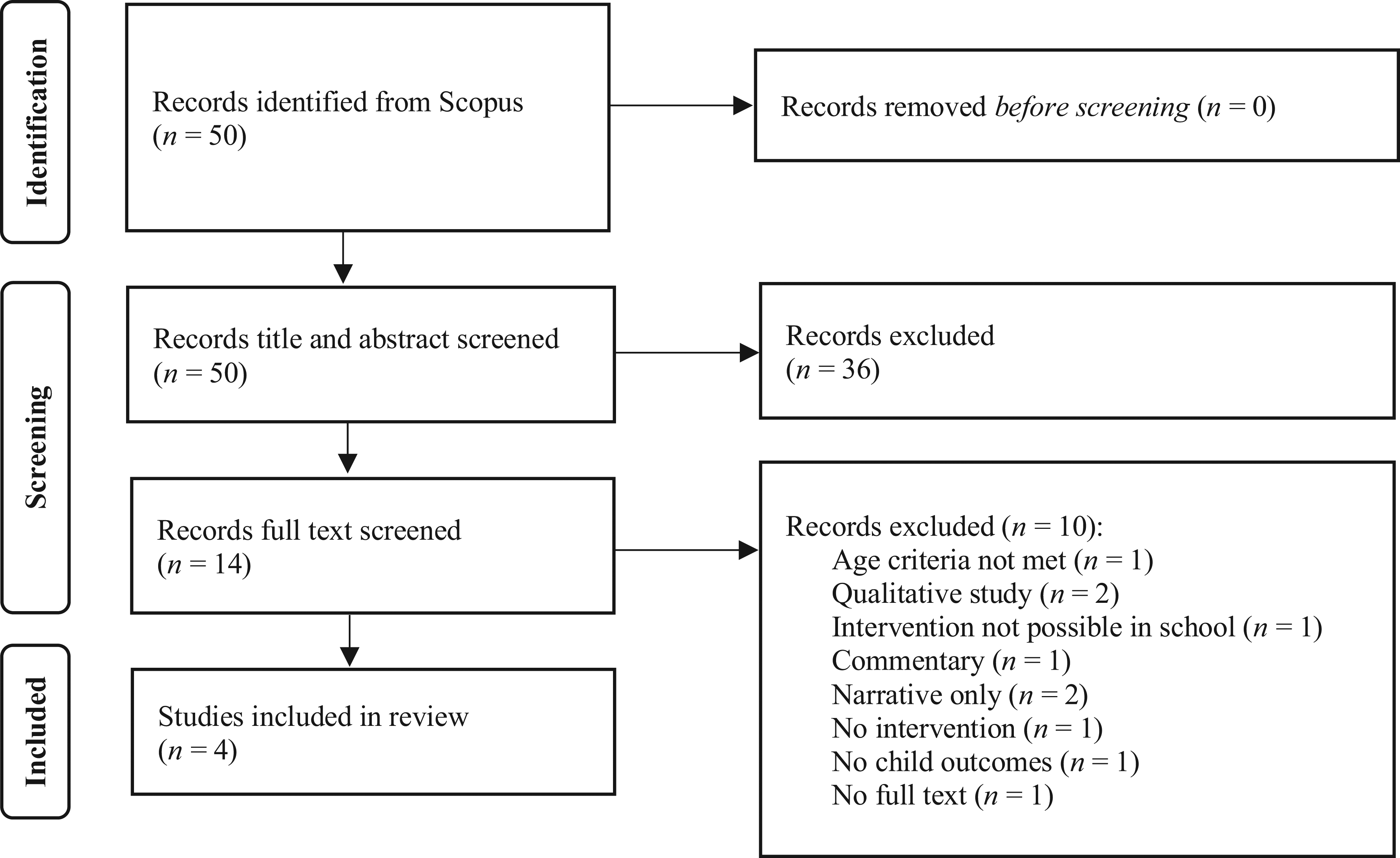
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow of study selection process from multisensory environment search (March 2022) before deduplication across the different searches.
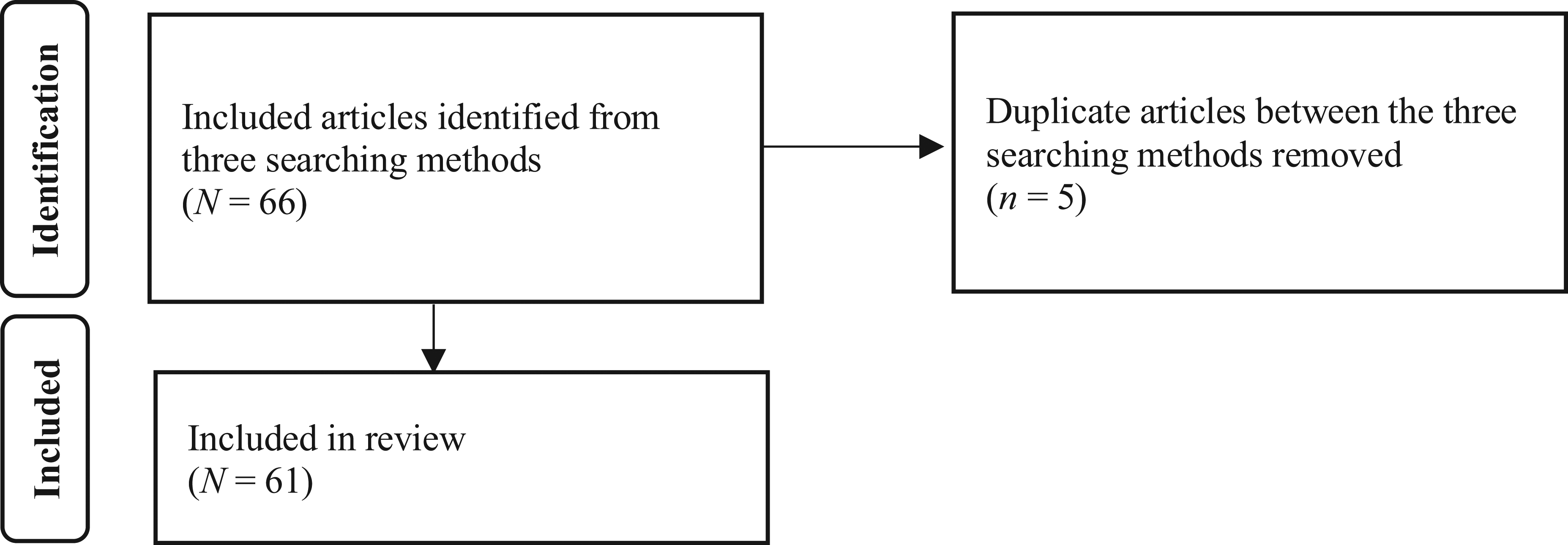
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow of study selection process for the deduplication of articles from the three search strategies.
We extracted all eligible articles and assessed each for level of evidence using an adapted version of the Oxford Levels of Evidence (Oxford Center for Evidence-Based Medicine, 2009) and those provided in MacDermid and Law (2007; see Table A.2). The articles were then summarized into a database for synthesis and interpretation.
A team of three research and practice-focused occupational therapists (Tennille Johnson, Alison Lane, and Katy Unwin), with 39 yr of combined experience supporting children in schools, reviewed the evidence for all supports. Where there was sufficient evidence, they conducted further analysis of the supports to make a recommendation for practice, categorizing supports as “not recommended,” “recommended in specific conditions,” or “recommended in all conditions.”
Results
Fifty-one empirical studies (Table A.3) and 10 reviews (Table A.4) were included in the evidence synthesis. Studies included children with multiple conditions, including autism (n = 35 studies), ADHD or attentional issues (n = 6 studies), sensory processing challenges (n = 4 studies), emotional–behavioral concerns (n = 3 studies), intellectual and developmental disability (n = 5 studies), and no diagnosis or typically developing (n = 9 studies). Of the studies assessed in this review, only 15% were rated as providing good evidence (9 randomized controlled trials [RCTs]), 38% provided adequate evidence (23 studies; 10 two-group and 13 one-group nonrandomized studies), and 31% provided poorer evidence (19 single-case studies; Table A.3). The remaining 16% were reviews focusing on nonhomogeneous RCTs and pre–post studies (70%), nonrandomized and case studies (20%), and single-case study research (10%; Table A.4).
Support Approaches
The studies included in the synthesis examined a wide variety of supports for students with sensory processing challenges (e.g., stability balls, sound amplification systems, MSEs). To aid coherence in comparison, we subdivided the included studies into three categories based on approach: (1) individual sensory practices, consisting of approaches focused on an individual sensory modality (e.g., weighted vests; n = 35, 69%); (2) multisensory practices, consisting of approaches combining multiple sensory modalities (e.g., MSEs; n = 14, 27%); and (3) cognitive strategies, consisting of any practice that supported the students to use cognitive strategies to manage sensory processing challenges (e.g., group cognitive–behavioral therapy; n = 2, 4%).
Individual Sensory Modality Practices
The category of “individual sensory modality practices” was further divided by modality; proprioceptive, auditory, and visual. Twenty of the included studies investigated proprioceptive approaches that use elements of body awareness, positioning, or movement to address sensory processing challenges (e.g., weighted vests, movement breaks, flexible seating, Ayres Sensory Integration®, snug vests, yoga, deep pressure). Thirteen studies examined practices that sought to address difficulties in processing auditory stimuli. These practices could be further subcategorized as (1) auditory training, whereby listening and sound processing skills were directly addressed; and (2) auditory modifications, in which modifications were made to the sound environment to improve access to sound stimuli. Examples of these practices include auditory integration training, listening therapy, noise cancelation headphones, and sound amplification systems. One study examined practices designed to address difficulties in processing visual stimuli. All practices focused on modifications to the physical environment and included adjustments to lighting types and intensities and reduction of visual displays.
Multisensory Practices
Fifteen studies focused on multisensory practices, with 9 exploring sensory diets and six exploring multisensory environments. For the purposes of this review, sensory diet practices were defined as any practice that provided a prescribed set of sensory or sensorimotor activities to support learning that was classified as a sensory diet. Practices included providing students with a schedule of planned and purposeful sensory activities, augmenting learning activities with sensory elements, or providing sensory-based play. Multisensory environments, conversely, are spaces curated to provide a sensory-rich environment for students to retreat to or focused-learning purposes.
Cognitive Practices
In this review, 2 studies evaluated cognitive practices, defined as any practice that supported students to use cognitive strategies to manage sensory processing challenges (e.g., reframing, planning, goal setting). Specifically, studies examined cognitive–behavioral therapy and the Alert Program®.
Outcomes of Support Approaches
We further analyzed the outcomes of supports where there were sufficient available data in the form of multiple studies. Four supports met this criterion: sound amplification systems, alternate seating, MSEs, and weighted vests.
Sound Amplification Systems
Four studies (Rance et al., 2014, 2017; Schafer et al., 2013; Wilson et al., 2021) and 1 systematic review (van der Kruk et al., 2017) investigated the use of classroom sound amplification systems for older school-age students with signs of auditory processing challenges. All studies focused on autistic students, with one study including students with ADHD and no disability. All studies reported positive effects on student listening as a result of sound amplification, with some studies also reporting effects on communication, social interaction, phonological processing, and reduced stress in social situations. The quality of the studies ranged from low to moderate, hence some results were considered inconclusive.
Alternate Seating
Fifteen studies (Benson et al., 2019; Brennan & Crosland, 2021; Erwin et al., 2016; Fedewa et al., 2015; Fedewa & Erwin, 2011; Gaston et al., 2016; Krombach & Miltenberger, 2020; Macphee et al., 2019; Mead & Scibora, 2016; Olson et al., 2019; Piragasam et al., 2018; Sadr et al., 2015, 2017; Umeda & Deitz, 2011; van der Wurff et al., 2021) and 4 systematic reviews (Barton et al., 2015; Dargue et al., 2021; Grajo et al., 2020; Ouellet et al., 2021) examined the effectiveness of dynamic seating, including stability balls, floor seating, seat cushions, and T-bar stools for sensory processing challenges among school-age children. Studies were conducted with students with autism, ADHD, intellectual disability, and no disability. The studies reported mixed findings. The weakest evidence was found for seat cushions, with ineffective and inconclusive results reported for in-seat and on-task behavior of autistic students. Furthermore, no effect for alternate seating on classroom behavior (including hyperactivity, oppositional defiance), attention, and in-seat behavior was reported in four studies. A positive effect of stability balls was reported on physical activity, attention span, and anxiety in two studies. The remaining studies reported inconclusive results for in-seat and on-task behaviors.
MSEs
Six studies (Garzotto et al., 2020; Hill et al., 2012; Kim & Park, 2022; Seckman et al., 2017; Unwin et al., 2021b; West et al., 2017) and 1 scoping review (Breslin et al., 2020) examined the use of MSEs to enhance learning and minimize distress for students with sensory processing challenges. Students included in the studies ranged in age from 3 yr to 18 yr and consisted of students with autism, intellectual disability, emotional–behavioral disorders, or no disability. One study was a small RCT (Unwin et al., 2021b), with the other studies using nonrandomized or single-case study designs. When children were given control of sensory changes within the MSE, Unwin et al. (2021b) found a reduction in repetitive motor behaviors, sensory behaviors, and stereotyped vocalizations and an increase in attention. Three other studies reported that MSEs were effective in reducing anxiety, distress, and challenging behavior and in improving student well-being. Two studies examined the effect of an MSE on the use of restraint and seclusion and reported limited effects (inconclusive and ineffective, respectively). The findings of the remaining studies were inconclusive for effects on behaviors including stereotypy.
Weighted Vests
Three studies (Collins & Dworkin, 2011; Hodgetts et al., 2011; Macphee et al., 2019) and 6 systematic reviews (Barton et al., 2015; Bodison & Parham, 2018; Grajo et al., 2020; Ouellet et al., 2021; Taylor et al., 2017; Weitlauf et al., 2017) examined weighted vests as a practice to address sensory processing challenges among school-age children. Studies were conducted with students with ADHD, autism, sensory processing difficulties, and no disability. Evidence from all studies indicated that weighted vests were ineffective for addressing in-seat and on-task behavior, classroom behavior, sitting time, and attention in the classroom. No study reported a positive effect from the use of weighted vests on these behaviors for any student group.
Discussion
Available evidence suggests that sound amplification systems, alternate seating, and MSEs may be effective in improving school access, participation, or achievement for some students with sensory processing challenges in certain circumstances. However, we found no support in the literature for the use of weighted vests. The applied nature of research in this area means efficacy was challenged by small sample sizes, inconsistent dosing regimens and practice protocols, and poorly defined populations. As such, we could not determine the effectiveness of each support identified in the review. This highlights the importance of evidence-informed practitioners incorporating these findings with their clinical judgment when assessing the appropriateness of a support for a child.
Compared with other supports in this review, there was more consistent and higher quality evidence confirming the efficacy of sound amplification systems for improved speech recognition or listening behaviors (Rance et al., 2014, 2017; Schafer et al., 2013; Wilson et al., 2021), along with improved educational outcomes (Rance et al., 2014) and increased on-task behavior (Schafer et al., 2013). Sound modification systems were investigated with larger samples than are typical for the field (N = 20–30). However, most of the studies tested this support only on autistic children ages 8 and older, and so the efficacy of this support for those with other diagnoses, and of other ages, is yet to be established. Although use of these supports appears promising, sound modification systems are expensive and do not effectively support all children (e.g., Wilson et al., 2021). Clinical judgment is required to determine whether the benefits outweigh the costs for the child requiring support.
We concluded that alternate seating, particularly stability balls, may be an effective strategy for some attentional concerns associated with sensory processing challenges (Fedewa & Erwin, 2011; Gaston et al., 2016). There was also some evidence that use of stability balls could increase on-task and in-seat behavior, but these studies were methodologically poor, typically using small samples (e.g., Brennan & Crosland, 2021, n = 3; Krombach & Miltenberger, 2020, n = 4). There was significant evidence that the practice was accepted or even viewed positively by teachers (Brennan & Crosland, 2021; Fedewa & Erwin, 2011; Gaston et al., 2016; Olson et al., 2019; Piragasam et al., 2018; Sadr et al., 2015; Umeda & Deitz, 2011). The value of this perception should not be underestimated, because teachers are integral partners in supporting students’ sensory challenges, and multidisciplinary practices remain the gold standard of support provision. However, evidence for the effectiveness of alternate seating is far from compelling. There are multiple alternate seating options available (e.g., stability balls, seat cushions) and a paucity of research, thus far, to understand their impact. Indeed, it has been suggested that it is the sense of agency or control a child feels when aligning seating type with their practical needs that is bringing benefit rather than seating type per se (e.g., Cole et al., 2021). Further research interrogating the perceived benefits would support more accurate practitioner recommendation. Considering this, and despite the relatively low cost of implementation and low clinician input compared with other supports (e.g., deep pressure brushing), the implementation of alternate seating should occur only after a thorough understanding of a child’s needs and a review of other evidence-informed strategies is established. Ongoing monitoring of the effect of alternate seating on educational goals is strongly recommended.
MSEs may be effective in reducing distress, anxiety, and challenging behaviors and in improving attention and well-being among school-age students with and without disability, particularly when the child is given control over the sensory changes in the MSE. However, the quality of research within this field is generally poor, and it is not clear why these highly sensory spaces may be beneficial. Unwin et al. (2021b) found changes in behavior when the autistic participants were provided with control over the sensory changes within the MSE. Benefit from having control aligns with broader literature findings that increasing predictability (e.g., Pellicano & Burr, 2012) and agency (e.g., Pfeiffer et al., 2017) may be beneficial for autistic people. This finding alludes to a candidate for the mechanism of effect or “active ingredient” within MSEs.
Individual differences pose a challenge in the evaluation of effectiveness of supports, contributing to observed inconsistencies in research findings. Hofmann and Hayes (2019) advocated for a departure from assessing named supports to embracing process-based therapy (PBT). PBT is founded on the concept that the mechanism of effect, or the active ingredient, is empirically tested instead of the support itself. Crucially, PBT does not focus on testing the active ingredient of a support on individuals with a specific condition (e.g., autism) but instead focuses on those with the same underlying difficulty (e.g., multisensory integration). This allows practitioners to pinpoint the student’s core challenge and prescribe a support with a specific active ingredient that research has shown will effectively address that specific difficulty—essentially, empirically aligning active ingredients of a support with underlying difficulties across diagnostic groups.
In the current literature, an active-ingredient approach is not commonly applied in study designs. Instead, standardized supports are frequently tested on groups with the same condition. To progress, we need to first establish the active ingredients or mechanisms of effect of our supports through rigorous studies. These can then be tested on those with the concomitant underlying difficulty, and, in this way, we will be able to know what works best for whom. It is noteworthy that the best evidence within this review was for sound amplification systems, in which the mechanism of effect was clearer than for other supports. For example, many autistic people have difficulty listening in the context of background noise (e.g., Alcántara et al., 2004), and one mechanism of effect of sound amplification systems is the improving signal-to-noise ratio (i.e., amplifying the teacher’s voice relative to background noise). When sound amplification systems are used with students who have difficulty hearing amid background noise, they will likely be successful because the mechanism of effect of the support aligns with the need of the student. It follows that this is just one type of support, and the mechanisms of effect must be understood for a range of supports so practitioners can align these with a child’s needs.
Frameworks are available to support researchers or clinicians in investigating mechanisms of effect when conducting RCTs (e.g., Kraemer et al., 2002), but it remains problematic that RCTs in this field are rare, with our review finding only one full RCT (1.6%) and five lower quality RCTs (8%). We contend that, until further RCTs are conducted, discipline progress toward a truly individualized approach will remain constrained.
Limitations
To address a perceived gap in previous reviews and support practitioners in the selection of potentially useful supports, we prioritized breadth over depth by including 61 studies in the final review. In practice, this meant that we could not discuss each study individually; therefore, we recommend practitioners use this review to overview the range of possible supports, then interrogate the specific relevant studies to inform decision-making.
Within the breadth of our review, we had hoped to identify and include assessments tools or instruments relevant to this context, although none were found. We note that adequate assessment of sensory challenges is the cornerstone of selecting and implementing appropriate support. Although we did not identify any in this review, practitioners should prioritize this stage, and more research and reviews are needed to support practitioners in selecting appropriate assessments. However, due consideration must be given to methodology because assessments of this nature do exist. The vast variation in terminology within the field and the lack of a shared (common) researcher and clinician language constitute a problem of practice yet to be fully addressed (Schaaf & Lane, 2015). Our review methodology further highlights this issue, requiring multiple iterative searches to locate all known or seminal literature. Variation in terminology is likely related to the discipline-wide limited conceptual understanding of sensory processing as a construct constraining measurement and efficacy of interventions designed to ameliorate sensory challenges (see Unwin et al., 2022). We consider a discipline-wide commitment to establishing agreed conceptualization of the sensory construct via a precise and practical common lexicon a high priority.
Limiting the scope of a review is necessary to maintain its quality and relevance, and for this reason we acknowledge that not all articles were captured within our review. We did not find sufficient evidence for the use of weighted vests, but an uncaptured study found that weighted vests could improve attention outcomes among children with ADHD (n = 110; Lin et al., 2014). This study was not included in our review because it was not related to the school setting. Although this single study did not constitute sufficient evidence for the use of weighted vests, it demonstrated the potential for higher quality research in this area that could benefit practitioners. However, the main issue remains that more of these high-quality studies are needed to fully understand how specific sensory supports, such as weighted vests, can be useful. When more of these studies are conducted, a new review will be necessary. Therefore, we recommend that this article be used to support practitioners in identifying relevant supports for their clients while also engaging with the broader literature, where necessary.
Implications for Occupational Therapy Practice
An intriguing finding that potentially challenges much current practice is that no supports could be wholly recommended without conditions or caveats. Indeed, and exemplifying this finding, the use of weighted vests is not recommended as a practice to improve classroom behavior or attention whatsoever. However, the following supports can be recommended, with the specific qualifications listed: ▪ Sound amplification systems. Autistic students 8 yr and older with identified auditory processing difficulties may benefit from classroom sound amplification systems to address listening-related stress in social and learning contexts and to improve phonological processing. ▪ Alternate seating. Alternate seating may be an effective strategy in some school settings for some attentional concerns associated with sensory processing challenges but is not recommended for managing behavioral concerns such as hyperactivity and oppositional defiance. Implementation of alternate seating should occur only after a thorough understanding of need and review of other evidence-informed strategies. We strongly recommend ongoing monitoring of the effect of alternate seating on educational goals. ▪ MSEs. MSEs may be effective in reducing distress and anxiety, challenging behaviors, and improving attention and well-being among school-age students with and without disability, particularly when the child is given control over the sensory changes in the MSE. The evidence for the effectiveness of MSEs to reduce the use of restraint and seclusion was mixed and, therefore, only recommended as appropriate in specific conditions.
Conclusion
Our review suggests that sound amplification systems, alternate seating (especially stability balls), and MSEs may improve school outcomes for students with sensory processing challenges under specific circumstances, but the use of weighted vests is not recommended. However, the efficacy of research included in this review was challenged by small sample sizes, inconsistent dosing regimens, and practice protocols. Challenges in assessing support effectiveness underscore the need for a shift toward process-based therapy, in which empirical testing of active ingredients or mechanisms of effect of supports on those with similar underlying difficulties—as opposed to those with the same diagnosis—is advocated. To achieve this ambitious goal, more RCTs are needed to assess the impact of active ingredients on those with specific underlying difficulties. Overall, this review highlights the importance of evidence-informed practitioners incorporating consideration of these findings in their clinical judgment when assessing the appropriateness of a support for a child within their educational context.
Supplemental Material
Supplementary material for Evidence Synthesis and Clinical Recommendations for Supporting School Students With Sensory Processing Challenges: A Rapid Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2024.050766.pdf for Evidence Synthesis and Clinical Recommendations for Supporting School Students With Sensory Processing Challenges: A Rapid Review by Katy Unwin, Kylie Wales, Tennille Johnson, Carl Leonard, Gaenor Dixon, Libby English and Alison Lane in The American Journal of Occupational Therapy
Footnotes
*Indicates articles included in the rapid review.
1In line with current best practice, we aim to avoid ableist language (Bottema-Beutel et al., 2021) and therefore use the term supports in place of interventions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.