
Abstract
This is the first study to establish a connection between attachment insecurity in adults and lower levels of engagement in meaningful activities during adulthood.
A core tenet of occupational therapy theory is that engaging in meaningful activities is of therapeutic value. Evidence suggests that occupational engagement stimulates resilience, promotes a sense of belonging, enhances self-efficacy, and is beneficial to health and life satisfaction (Thomson & Jaque, 2017). Preliminary findings suggest a link between meaningful activity engagement and adverse childhood experiences (ACEs; Kerley et al., 2022). Childhood adversity (CA) is also associated with attachment insecurity (Alexander, 1992; Erozkan, 2016; Felitti et al., 1998; Fonagy, 2010; Heenan et al., 2020; Prather & Golden, 2009; Thomson & Jaque, 2017; Toof et al., 2020; Yumbul et al., 2010), and both have been related to lower levels of physical, psychological, and socioeconomic well-being and overall quality of life (Darban et al., 2020; Downing et al., 2021). Attachment insecurity has been shown to mediate the association between CA and health-related variables in adulthood (Howard et al., 2023). Given the effects that CA can have on lifelong outcomes, attachment may represent a key mechanism in the association between CA and adult engagement in meaningful activity (EMA). Literature provides extensive evidence to support an association between CA and adulthood attachment insecurity; however, theory regarding the relationships between attachment insecurity and EMA lacks a strong empirical base. This study aims to extend previous findings regarding associations between attachment patterns and CA and contribute novel discoveries regarding the associations between attachment insecurity and EMA to inform clinical approaches and guide future research.
Adverse Childhood Experiences
ACEs are traumatic events that occur before a person is age 18 yr, including abuse, neglect, parental mental illness or divorce, and witnessing violence. The original ACE study (Felitti et al., 1998)—which investigated seven categories of ACEs, including sexual abuse and parental mental illness—and subsequent research (e.g., Hughes et al., 2017) have shown that exposure to CA is a risk factor for a range of negative physical and mental health outcomes in adulthood. CA can have enduring and negative effects on health, well-being, and life opportunities and is associated with poorer academic and vocational outcomes and with higher risks of cancer, suicide, and heart disease (Hughes et al., 2017). Evidence indicates that occupational therapy intervention has the potential to protect a person against the effects of CA as well as their likelihood of poorer outcomes in adulthood (Whitney, 2020).
Attachment Theory
According to Bowlby (1969), attachment theory is a fundamental theoretical model of emotional and social development based on the bond formed between child and caregiver. Unmet attachment needs during childhood are typically associated with attachment insecurity in adulthood, reflecting attachment anxiety and attachment avoidance, whereas children who had responsive and predictable caregivers are more likely to form a secure attachment pattern. Erozkan (2016) reported that different types of unmet needs during childhood resulted in various insecure attachment patterns in adulthood; for example, children who receive unresponsive caregiving tend to form avoidant–dismissive attachment patterns, whereas children whose needs are inconsistently met by caregivers are susceptible to forming anxious–preoccupied attachment patterns. Attachment experiences in childhood shape internalized perceptions of self and others (Thomson & Jaque, 2017). These internalized working models have lifelong implications and determine attachment-based behavioral, cognitive, and emotional tendencies throughout the lifespan (Thomson & Jaque, 2017).
Associations Between Childhood Adversity and Attachment
Alexander (1992) was one of the first researchers to consider the associations between childhood trauma and adult attachment. She proposed that adults with a history of childhood sexual abuse are more likely to develop attachment insecurity and that, by understanding attachment theory, the functionality of future relationships associated with different dimensions of attachment insecurity in trauma survivors can be predicted. Literature has continued to accumulate in support of these original propositions, and consistently, CA has been linked with attachment insecurity in childhood and adulthood across various populations (Prather & Golden, 2009; Toof et al., 2020; Yumbul et al., 2010), with Fonagy (2010) stressing that trauma is the most destructive factor in attachment formation.
Levinson and Fonagy (2004) reported associations between childhood trauma and attachment insecurity in adults with a psychiatric disorder in a prison population. Results revealed that CA and attachment insecurity were both positively correlated with the presence of psychiatric disorders, violence, and imprisonment, lending credence to associations among CA, attachment insecurity, and poor psychological and functional outcomes.
Erozkan (2016) and Thomson and Jaque (2017) both conducted studies using different measures of CA and attachment and found links between attachment and CA in samples drawn from a university population and a community population, respectively. More recently, Heenan et al. (2020) found a link between childhood trauma and attachment anxiety in adult patients undergoing cardiac rehabilitation and indicated that these two variables were related to poorer physical and mental quality of life.
Links With Engagement in Meaningful Activity
Meaningful activity engagement serves an important role in fostering meaning in life and life satisfaction (Eakman, 2012; Goldberg et al., 2002). Occupational therapists are becoming increasingly aware of the negative influence of CA on EMA, with links demonstrated between CA and lower levels of engagement among children (Fraser et al., 2019). More recently, Kerley et al. (2022) were the first to establish a negative correlation between CA and EMAs in adulthood. Arikan et al. (2016) found that attachment insecurity negatively influences the likelihood of posttraumatic growth in people who have experienced CA, which has implications for EMA in adulthood (Kaye-Tzadok & Icekson, 2022); However, the relationship between attachment patterns and engagement has not yet been investigated, and interrelations among CA, attachment insecurity, and EMAs have not been investigated within the literature.
Present Study
With CA and attachment insecurity well established as determinants of physical, psychological, and socioeconomic health, it is surprising that so few studies have been conducted to investigate the associations of these variables with EMAs. The limited studies exploring associations between CA and EMA have revealed preliminary data to support bivariate relationships; however, no attention has been paid to associations between attachment insecurity and EMA or to the role of attachment insecurity in the relationship between CA and EMA. To elaborate on existing evidence, and to address these gaps in the literature, the interrelationships among CA, adult attachment, and adult EMA need to be investigated.
On the basis of existing research, we pose two hypotheses. Hypothesis 1 is that higher levels of attachment insecurity will be related to lower levels of EMA in adulthood. Hypothesis 2 is that both attachment anxiety and attachment avoidance will mediate the relationship between CA and EMA.
Method
Research Design
This study is a secondary analysis of a preexisting dataset, with one paper having been published previously (Kerley et al., 2022). Using convenience snowball sampling, we conducted a cross-sectional online survey. We obtained ethical approval for both the initial (Project No. 2018002377) and the secondary (Project No. S221695) data analyses from The University of Queensland and the University of the Sunshine Coast, respectively.
Setting and Participants
A total of 366 participants provided informed consent to participate. Of these, 312 completed all questionnaires and were included in all analyses; an additional 17 participants completed two questionnaires and were included in relevant analyses.
Inclusion criteria were as follows: Participants had to ▪ be at least 18 yr old, ▪ reside in the community (i.e., not in a hospital or inpatient service), ▪ report that they were not currently experiencing distress (determined on the basis of self-report), ▪ understand standard English to complete the questionnaires, and ▪ volunteer to participate in the study with the knowledge that there were no incentives for participating or penalties for withdrawing.
Data Gathering
Participants were recruited by means of convenience and snowball sampling, using notices on notice boards at The University of Queensland and through social media posts. The questionnaires were conducted using SurveyMonkey. Interested participants were able to access the questionnaires through a web link, a notice, or a social media post. Participation in the survey was voluntary, and participants provided consent before completion of the survey.
Measures
We measured CA with the Risky Families Questionnaire (RFQ; Taylor et al., 2004), which contains 12 retrospective questions regarding CA in a respondent’s family environment between the ages of 5 and 15 yr. For each question, participants rate how frequently they experienced adverse events on a 5-point Likert scale ranging from 1 (not at all) to 5 (very often). Sample items include, “How often did a parent or other adult in the household swear at you, insult you, put you down, or act in a way that made you feel threatened?” and “How often would you say that a parent or other adult in the household behaved violently toward a family member or visitor in your home?” Positively worded questions were reverse scored. The RFQ has been widely used in CA research, and strong or acceptable psychometric properties have been reported (Taylor et al., 2006).
Attachment orientation was measured by the Experiences in Close Relationship Scale–Short Form (ECR–S; Wei et al., 2007), which consists of 12 statements relating to how a person feels in romantic relationships. The measure consists of two subscales measuring attachment anxiety and attachment avoidance, with six statements on each subscale. For each statement, participants rate their level of agreement on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Sample items include “I need a lot of reassurance that I am loved by my partner” (anxiety subscale), and “I try to avoid getting too close to my partner” (avoidance subscale). Of the 12 items, four are reverse scored. The ECR–S has been reported to have adequate psychometric properties in multiple languages, demographics, and settings (Constantinescu et al., 2022; Feddern Donbaek & Elklit, 2014; Wei et al., 2007).
Meaningful activity engagement was measured with the Engagement in Meaningful Activities Survey (EMAS; Goldberg et al., 2002), which was “developed to measure the extent of engagement in meaningful activities” that make participants “feel good about themselves” (Goldberg et al., 2002, p. 24). This study used a version of the EMAS modified by Eakman (2012); both the original and modified versions possess good psychometric properties across demographics and settings. The interview schedule comprises 12 statements that describe the meaningfulness of one’s daily activities. Participants rate the extent to which they feel each statement is true on a 4-point Likert scale ranging from 1 (rarely) to 4 (always). Sample items include “The activities I do contribute to my feeling competent” and “The activities I do give me a feeling of control.” Participants’ subjective levels of engagement in meaningful activity are classified as low (EMAS scores less than 29), moderate (EMAS scores of 29–41), or high (EMAS scores greater than 41; Eakman, 2015).
Statistical Analyses
We conducted statistical analyses using IBM SPSS Statistics (Version 26). Normal distributions for anxious attachment and EMA were revealed by the Shapiro-Wilks test of normality (Cohen et al., 2003); therefore, these variables were suitable for parametric testing. Avoidant attachment was not normally distributed; therefore, nonparametric testing was used where relevant. For each continuous study variable (CA, EMA, avoidant attachment, anxious attachment), we calculated descriptive statistics (mean, standard deviation, and range), and Cronbach’s α was calculated for scales and subscales (Table 1). Univariate analyses involved summarizing the categorical demographic characteristics of participants who provided responses for two or more of the following variables: CA, attachment insecurity (anxious and avoidant attachment subscales), and EMA. We used a one-way analysis of variance to determine the associations among gender and study variables, because gender differences have been found in the associations between CA and negative outcomes in adulthood (Haahr-Pedersen et al., 2020). Because gender was initially gathered as a categorical variable with three categories, it was recoded as a dichotomous variable to enable correlation and other analyses. We conducted bivariate correlation analyses to determine relationships among CA, attachment insecurity, and EMAs (Mukaka, 2012).
Descriptive Statistics and Correlations Among Study Variables (N = 329)
a n = 312. b n = 322.
*p ≤ .01. **p ≤ .001.
We performed a series of mediation regression analyses to investigate the interrelations among CA, attachment variables, and EMA. A variance inflation factor (Miles, 2014) was calculated to assess collinearity between independent variables that yielded appropriate values. We used Model 4 in PROCESS (Hayes, 2013) to test the roles of anxious attachment and avoidant attachment as mediators on the association between CA and EMA in adulthood. In the present research, we also used 5,000 bootstrap samples and a 95% confidence interval (Hayes, 2013).
Results
Participants
Demographic characteristics for the study are presented in Table 2. Participants were primarily women, ages 25 to 34 yr, White, Australian residents who had a university education.
Descriptive Details for Demographic Variables of Study Sample (N = 329)
Descriptive Statistics
Cronbach’s αs, means, standard deviations, ranges, and correlations among study variables are presented in Table 1. As displayed in Table 1, attachment insecurity in adulthood was significantly positively associated with CA, a finding previously reported by Kerley et al. (2022). Both avoidant attachment insecurity and anxious attachment insecurity were significantly negatively correlated with EMAs in adulthood. Gender was significantly positively correlated with avoidant attachment and significantly negatively correlated with EMA. The correlations were of small to medium size, with the strongest correlations found between CA and attachment anxiety.
Attachment Dimensions as Mediators in the Association Between Childhood Adversity and Meaningful Activity Engagement
The mediating effect is illustrated by simple mediation models (Figure 1). The total indirect effect for the mediators in the model was significant. The specific indirect effects for attachment anxiety and attachment avoidance were significant: For attachment anxiety, β = −0.129, p < .001; 95% confidence interval (CI) = [−0.043, −0.001]; F(2, 309) = 7.608, and for attachment avoidance, β = −0.229, p < .001; 95% CI = [−0.064, −0.016]; F(2, 309) = 13.207. Bootstrap CIs for the indirect effects of attachment anxiety (ab = −0.019) and attachment avoidance (ab = −0.038) on the basis of 5,000 bootstrap resamples were entirely below zero; thus, it can be inferred that mediation has occurred. CA has a direct effect on EMA and also has an indirect effect on EMA through attachment insecurity. The link between CA and EMA remained significant on the inclusion of attachment anxiety and avoidance in the regression analyses, which indicates partial mediation (Figure 1). As such, this suggests that attachment anxiety and avoidance partially mediated the relationship between CA and EMA among adults. R2 measures demonstrate that this mediation model explains that 4.7% and 7.9% of the variation in EMA is accounted for by attachment anxiety and attachment avoidance, respectively.
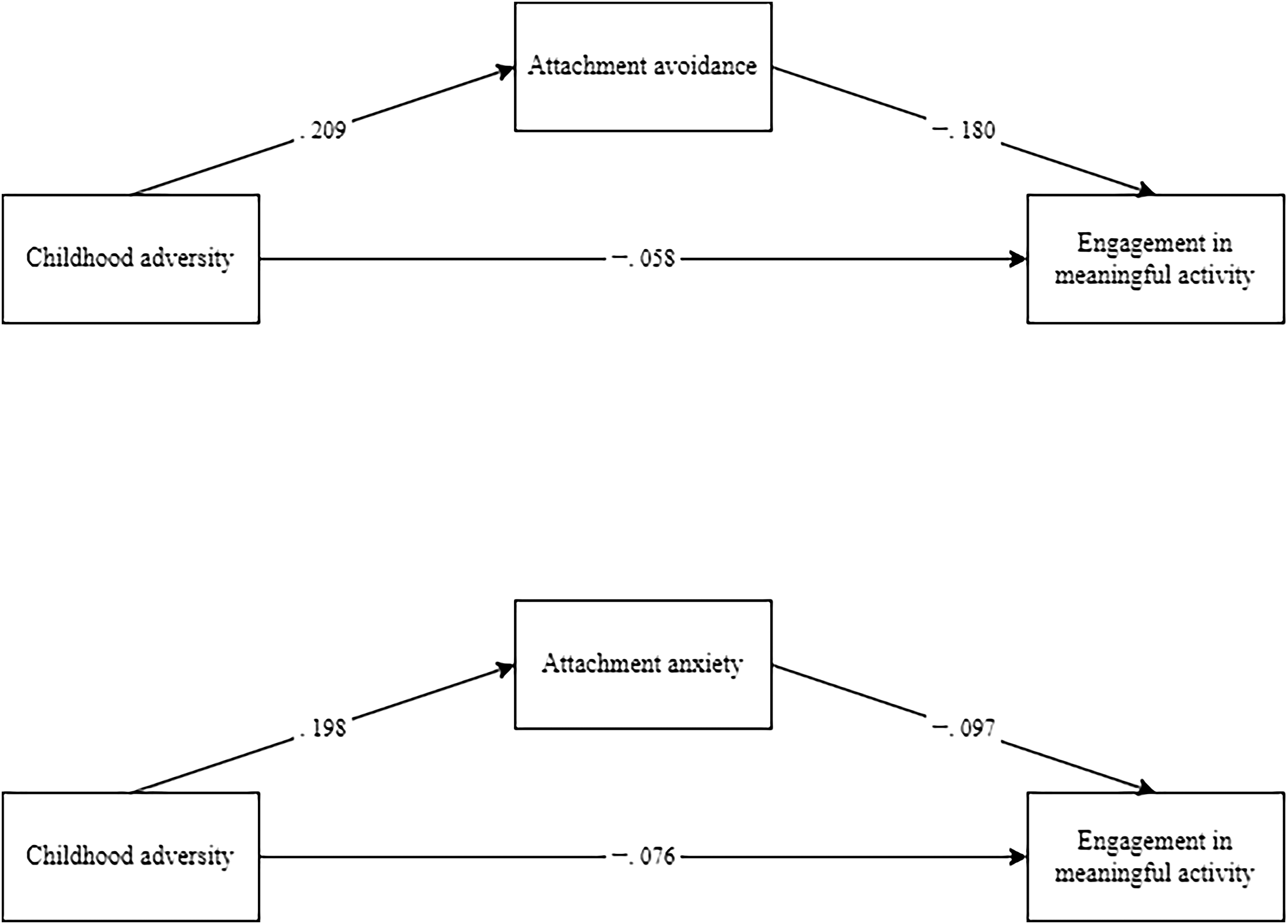
Mediation models for engagement in meaningful activity (n = 312).
Discussion
This study offers valuable insights into the associations among CA, attachment insecurity, and EMAs in adulthood. To our knowledge, it is the first investigation of these variables to identify a link between attachment insecurity and EMAs and also to determine the role of attachment insecurity in mediating the relationship between CA and EMA.
Our primary hypothesis, that attachment insecurity would be negatively associated with meaningful activity engagement, was supported. This is congruent with the vast body of literature that supports associations between attachment insecurity and a range of negative outcomes in adulthood (Thomson & Jaque, 2017). Our findings suggest that higher levels of attachment insecurity influence levels of EMA in adults, although this theory cannot be confirmed by the extent of our research.
Our second hypothesis, that attachment insecurity would mediate the relationship between CA and EMA, was also supported. The significant mediating effect of attachment insecurity provides preliminary evidence to suggest that exposure to CA has a greater influence on EMA in people who are more insecurely attached than those who are more securely attached. On the basis of this result, we may infer that insecure attachment patterns can predict EMA for people who have experienced CA.
Consistent with previous findings, attachment insecurity was significantly positively correlated with CA. These findings lend confidence that CA manifests in adulthood through attachment insecurity (Prather & Golden, 2009; Toof et al., 2020; Yumbul et al., 2010).
Limitations
The present study has several limitations that should be acknowledged; therefore, the results should be interpreted cautiously. First, neither the presence of clinical diagnoses nor information about any specific diagnosis was included as a variable in the current study. Because both CA and attachment insecurity are correlated with various psychopathologies (Hughes et al., 2017; Pearse et al., 2020), it may be advantageous to consider relevant diagnoses in future studies. Second, we did not consider different categories of CA experienced by participants as variables in this study. This is important to examine, because particular kinds and severities of adversity have various effects on outcomes (Felitti et al., 1998). Third, although findings were highly significant, the relatively small effect sizes suggest that we should be cautious about the practical application of results.
Future Research Directions
Given the limitations of our study, future research should explore the associations among different types of CA, and attachment insecurity and EMA. Future studies should also investigate the relationships between other types of attachment (secure and fearful), CA, and EMA. These investigations would enhance clarity regarding the associations between variable subscales.
To increase confidence in generalizability of results, establish more conclusive evidence, and strengthen the body of literature in both basic and applied studies, future research should replicate the present study with samples that better represent the general population. This replication should include participants from a wider range of socioeconomic status, a higher representation of males, and across varying levels of education (Schäfer & Schwarz, 2019).
To confirm the clinical specificity of results, it would also be beneficial to replicate the present study with participants with mental health diagnoses, because CA and attachment insecurity are associated with a range of mental illnesses, including depression, generalized anxiety disorder, obsessive–compulsive disorder, and posttraumatic stress disorder (O’Connor & Elklit, 2008; Santos et al., 2023; Tibi et al., 2020; Williams et al., 2019).
Additionally, longitudinal studies are required to determine causality and directionality of associations among variables. Future studies should also explore the possibility that providing intervention to address one dependent variable may improve outcomes in another variable; for example, future research could investigate the effect of attachment-based intervention on client’s EMA in adulthood, or vice versa.
Furthermore, future studies should explore the relationship between attachment insecurity and therapeutic alliance. Given that our profession utilizes EMAs as a crucial aspect of recovery, and acknowledging that adults affected by CA demonstrate lower rates of engagement in such activities, there exists a heightened possibility that insecure attachment patterns could restrict the effectiveness of therapeutic relationships in facilitating optimal outcomes from meaningful occupational engagement.
Implications for Occupational Therapy Practice
Although the results of this study are provisional, they extend previous findings regarding the relationship between CA and attachment. This study has, for the first time to our knowledge, revealed an association between attachment insecurity and EMA, and determined that attachment insecurity mediates the relationship between CA and EMA. These associations have the following implications for occupational therapy practice: ▪ A history of CA and current attachment pattern should not be underestimated as influencing a client’s present EMA. ▪ It is important to use trauma-informed practices during routine clinical assessment and service provision for adults with lower levels of EMA. ▪ Understanding trauma enhances the capacity to facilitate posttraumatic growth and, consequently, improve occupational engagement. ▪ Clinical reasoning should be informed by the client’s experience of CA and current attachment pattern and should be applied through a trauma-informed lens. ▪ It is important not only to consider a client’s experience of CA and attachment pattern but to also reflect on the practitioner–client therapeutic alliance.
Conclusion
The findings of this study offer support for interrelations among CA, attachment insecurity, and EMA. This is the first study to demonstrate an association between attachment insecurity and EMA in adulthood and to highlight the mediating role of attachment insecurity on the relationship between CA and EMA. Consistent with previous findings, attachment insecurity in adulthood was positively associated with CA. The findings further suggest that attachment insecurity in adulthood mediates levels of EMA in people who have experienced CA. Additional research is needed to strengthen and extend these findings.
Footnotes
Acknowledgments
This research was completed as part of Samantha Aquilina’s occupational therapy honors degree and Lou Kerley’s doctoral degree. We express our appreciation to the people who completed the survey for their engagement in this study. We are also grateful for the statistical advice of Daniel Meloncelli.