
Abstract
The Bimanual Arm Trainer (BAT) is a novel device that can be used in occupational therapy to improve arm function after a stroke.
Upper extremity (UE) deficits are common among persons with stroke, with approximately 80% having consequent UE impairment (Hayward et al., 2019). Reduced, or complete loss of, UE motor function often results in the need for increased physical assistance from caregivers for completion of activities of daily living (ADLs), participation in one’s roles and responsibilities, and use of assistive devices for mobility. Research has indicated that UE deficits can continue for at least 6 mo after a stroke, and only a small percentage of persons with stroke achieve complete recovery of UE function (Chen et al., 2019; Sethy et al., 2018). According to the American Heart Association guidelines for adult stroke rehabilitation, 60% of persons with stroke develop joint contractures on the more affected side within the first year (Winstein et al., 2016). This lack of active and/or passive range of motion can negatively affect participation in ADLs, including bathing, dressing, and other areas of self-care.
Recent studies have shown that completing bilateral simultaneous movements during UE interventions may result in coactivation and interhemispheric activation of both the ipsilesional and contralesional brain areas, with one limb entraining the other and enabling the limbs to function as a unit (Sethy et al., 2018). According to one systematic review and meta-analysis, bilateral training yielded superior improvements in motor impairment as measured by the Upper Extremity Fugl-Meyer Assessment of Motor Recovery after Stroke (FMA–UE; Fugl-Meyer et al., 1975) when compared with unilateral training (Chen et al., 2019). However, the two yielded similar improvements in motor impairment as measured by the Wolf Motor Function Test, Action Research Arm Test (ARAT; Lyle, 1981), and Box and Block Test (Chen et al., 2019).
Virtual reality and mirror therapy activities have been investigated as potential treatment interventions for persons with stroke. Virtual reality generally refers to the interaction of a person with a virtual device, such as a computer or mobile device simulation, that appears and feels similar to real-world objects and events (Karamians et al., 2020). During mirror therapy, persons with stroke watch a reflection of their less affected arm move, providing the illusion that motor function in their more affected arm is restored (Zeng et al., 2018). Research has demonstrated that virtual reality interventions can improve UE function after stroke because they are motivating and challenging; offer external feedback that may facilitate motor learning; and allow for the high-intensity, repetitious practice necessary to drive recovery (Warland et al., 2018). Mirror therapy also has been shown to improve sensory and attentional deficits and to support motor recovery in the distal hemiplegic limb (Fong et al., 2019).
Coupling bilateral simultaneous UE movement and virtual reality activities is the purpose of the Bimanual Arm Trainer (BAT), a nonpowered mechanical device by which the nonparetic UE moves the paretic arm (Raghavan et al., 2017). Figure 1 provides an image of the device. The BAT allows persons with various levels of weakness to move their arms via the device through bimanual arm training with a virtual reality component. The virtual reality component requires participants to interact with the device to pace a rowboat, pick apples from a tree, or fill a cup of water, depending on the program chosen. The device can be adjusted to a person’s height, arm length, and shoulder width to ensure appropriate setup. The BAT offers four programs: (1) shoulder internal/external rotation; (2) elbow flexion/extension; (3) forearm pronation/supination; and (4) grip release, in which only shoulder and elbow movements use the bimanual function of the device. This means that in the other two programs one side does not cause the other side to complete the desired movement. For this particular study, only the bimanual shoulder internal/external rotation program was used.

Bimanual Arm Trainer.
The BAT was developed on the basis of therapeutic principles: (1) Mirror therapy facilitates recovery, (2) bimanual therapy engages both sides of the body and brain in regaining movement, (3) video gaming increases motivation for exercise, (4) real-time feedback facilitates error correction, [and] (5) repetition of normal movements in the absence of abnormal compensatory movements is critical. (Mirrored Motion Works, 2020, paras. 4–10)
Only a limited amount of research has examined the BAT, other than determining that it is safe and feasible to use. Because of its novelty, the developers suggested future studies to determine its effectiveness over a long-term period (Raghavan et al., 2017).
The purpose of this study was to determine the effectiveness of the BAT compared with traditional occupational therapy treatment sessions in promoting UE functional return after stroke, as measured by scores on the ARAT and FMA–UE. We hypothesized that participants who received BAT interventions in addition to traditional occupational therapy services will demonstrate statistically significant improvements in UE function as evidenced by their scores on the ARAT. These conclusions will potentially help clinicians better serve persons with stroke in the early phases of their recovery by offering a treatment intervention that may improve UE motor return for increased independence in daily self-care routines.
Method
Study Setting
This clinical trial was conducted at a 33-bed inpatient rehabilitation facility (IRF) and was prospectively registered. Approximately 40% of all admissions at this IRF are persons with stroke, and the facility is a Joint Commission–designated comprehensive stroke center. It also is accredited by the Commission on Accreditation of Rehabilitation Facilities with a Stroke Specialty Program subaccreditation. The unit houses an interdisciplinary team that includes physical medicine and rehabilitation staff, nursing staff, case managers or social workers, physical therapists, occupational therapists, speech-language pathologists, and recreational therapists. The goal of this setting is to maximize the patient’s functional independence and safety, facilitating a return to the community setting or other appropriate environment. Patients receive at least 3 hr of daily rehabilitation therapies, 5–7 days/wk, with an average length of stay between 10 and 14 days. Initial evaluations by each discipline are performed to obtain a patient’s baseline level of function, develop goals, and initiate appropriate discharge planning.
Outcome Measures
The ARAT is a validated outcome measure that evaluates UE functional limitations as a result of injury resulting in hemiplegia (Lyle, 1981). A total score of 57 is a composite of 19 action-based items that are grouped into the following four subtests: (1) Grasp, (2) Grip, (3) Pinch, and (4) Gross Movement. Patients attempt each item and receive a score of 0 (cannot perform any part of the test item), 1 (performs the test item partially), 2 (completes the test item but takes an abnormally long time), or 3 (performs the test item normally; Yozbatiran et al., 2008).
The ARAT has strong measurement properties and facilitates goal-setting on the basis of performance (Grattan et al., 2019). It has been shown to have high interrater reliability and test–retest reliability (Wei et al., 2011). Research has shown a good correlation between the ARAT and FMA–UE at pre- and posttreatment assessments, which is indicative of concurrent validity. The ARAT displays floor effects, with difficulty detecting change in persons with stroke who have dense hemiplegia (Sivan et al., 2011).
The FMA–UE is a stroke-specific outcome measure that assesses sensory, proprioceptive, and motor impairments. A total of 33 items are assessed for the Motor subscale, which has a maximum score of 66 points. The Sensation subscale (light touch and proprioception), with a maximum score of 12 points; Passive Joint Motion subscale, with a maximum score of 24 points, and Joint Pain subscale, with a maximum score of 24 points, are also scored. The total maximum score for all UE subsections combined is 126. Items are scored on a 3-point Likert scale, with greater total values indicating less severity of deficit. A clinically important improvement of upper limb function as demonstrated by this scale has been determined to be ≥6 points (Page et al., 2012).
Excellent interrater reliability, intrarater reliability, and construct validity have been demonstrated on the FMA–UE, with the measure able to accurately capture change in UE impairment after stroke (Bushnell et al., 2015; Hsieh et al., 2009). The FMA–UE has excellent test–retest reliability and responsiveness, with the responsiveness of the FMA–UE being significantly larger than that of the ARAT (Hsueh et al., 2008).
Participants
The population for this study included adults age ≥18 yr with a diagnosis of acute ischemic stroke. Patients were admitted from acute care facilities, subacute rehabilitation facilities, chronic medical/ventilator units, or home. To meet IRF admission criteria, a patient must be considered medically stable, with functional limitations that affect their capability to be safely discharged to the community.
Study inclusion criteria required that the patient have a diagnosis of ischemic stroke with an ARAT score ≤17, because patients with a score of >17 follow different standard-of-care treatment at this facility. Patients who receive a score <17 on the ARAT were excluded because this indicates impaired cognition that affects the ability to understand and participate in a virtual reality system, pain resulting in poor tolerance of range of motion, impaired sitting balance, and/or poor tolerance of sitting in upright posture in a chair without armrests. Although a formal cognitive assessment was not used to include or exclude participants, speech-language pathologists were consulted as needed for feedback on the cognitive abilities of potential participants. Two enrolled participants were removed from the study, one because of cognitive concerns and one because of an onset of pain in the affected shoulder during treatment.
Intervention
We reviewed patients’ electronic medical records from November 2019 to November 2020 to identify 27 consecutive persons with stroke who received standard-of-care occupational therapy services and who met relevant inclusion criteria. In this clinical setting, standard-of-care occupational therapy services after stroke include ADL and instrumental activity of daily living (IADL) interventions, functional mobility and transfers, and addressing UE deficits. All stroke patients participate in the ARAT assessment within 3 days of admission as part of standard care. Those who receive a score of ≤17 on the ARAT typically participate in a variety of UE interventions, which may include range of motion activities, mirror therapy, electrical stimulation, and repetitive functional task training. From the aforementioned medical records, relevant data were then extracted for demographics, and ARAT scores at evaluation and discharge were retrieved. The data were assigned to the retrospective control group because the BAT was not available for use during their hospitalization.
The BAT was obtained on April 23, 2020, and was introduced as standard-of-care practice in November 2020. Since its introduction as part of standard of care, it has been used for patients on the unit as determined appropriate by treating clinicians.
This clinical trial was reviewed and approved by the Johns Hopkins School of Medicine Institutional Review Board. From November 2020 through June 2023, 27 patients who met the criteria outlined earlier were enrolled in the study through written informed consent. Consent to this study was voluntary, and declining participation did not alter any treatment interventions provided to the patients. All patients admitted with a stroke diagnosis had the ARAT completed within 72 hr of admission to the unit. In addition to ARAT scores (taken as standard of care), clinicians recorded FMA–UE scores for participants who had provided consent. All study participants completed the FMA–UE within 24 hr of enrollment. Both measures were completed before any BAT training sessions were administered.
Consenting patients participated in at least (but not limited to) three BAT training sessions, lasting ≥10 min each and averaging 10 repetitions/min. Participants were also administered all other standard therapy sessions throughout their rehabilitation stay. Before being discharged, and after they had completed the required number of training sessions, each participant was reassessed with both the ARAT and the FMA–UE.
Statistical Analysis
We conducted a 2 × 2 (Group × Time) repeated-measures analysis of variance with time (evaluation, discharge) as the within-subject factor and group (BAT, control) as the between-subjects factor, with the covariates days poststroke at admission and length of stay, with ARAT score as the primary outcome. A paired t test was used to compare FMA–UE scores at evaluation and discharge in the BAT group; FMA–UE scores were not available for the control group. All analyses were set with α ≤ .05.
Results
Sample Characteristics
There were no statistically significant between-group differences in age, days poststroke at admission, length of stay, or admission ARAT scores. Demographic characteristics are presented in Table 1.
Participant Characteristics
Note. There were no statistically significant differences on any participant characteristics between the groups. Dashes indicate data that are not applicable. ARAT = Action Research Arm Test; BAT = Bimanual Arm Trainer; FMA–UE = Fugl-Meyer Assessment of Motor Recovery after Stroke.
aSex: 11 male, 16 female; race: 12 White, 15 Black/African American.
bSex: 18 male, 9 female; race: 16 White, 11 Black/African American.
cRange = 0–57. Higher scores indicate better function.
dRange = 0–126. Higher scores indicate less severity of deficit.
ARAT
There was a significant main effect of time (p = .02), indicating that both groups showed significant improvement on the ARAT from evaluation to discharge (Figure 2). There was no significant main effect of group (p = .88): The BAT and control groups had similar ARAT scores at both evaluation and discharge. There were no significant effects of days poststroke at admission (p = .61) or length of stay (p = .22) and no significant interactions (Time × Group, p = .63; Time × Days Poststroke at Admission, p = .38; Time × Length of Stay, p = .28).
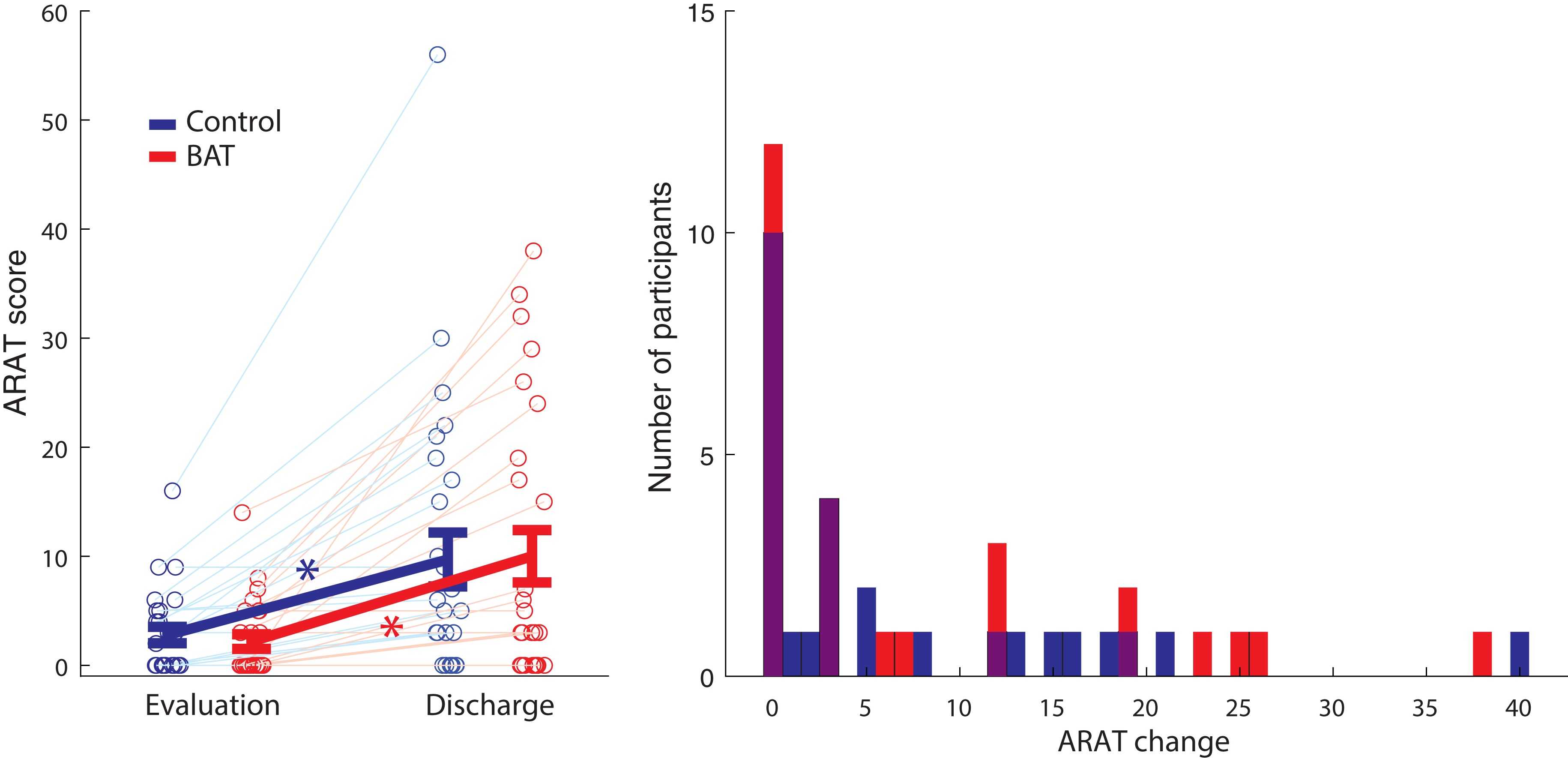
Score changes on the ARAT from evaluation to discharge and total number of participants for each ARAT score in the control group and the BAT group.
FMA–UE
Participants in the BAT group showed significant improvement in both the combined (sensory and motor) and Motor-Only FMA–UE scores from evaluation to discharge (both ps < .001; Figure 3).
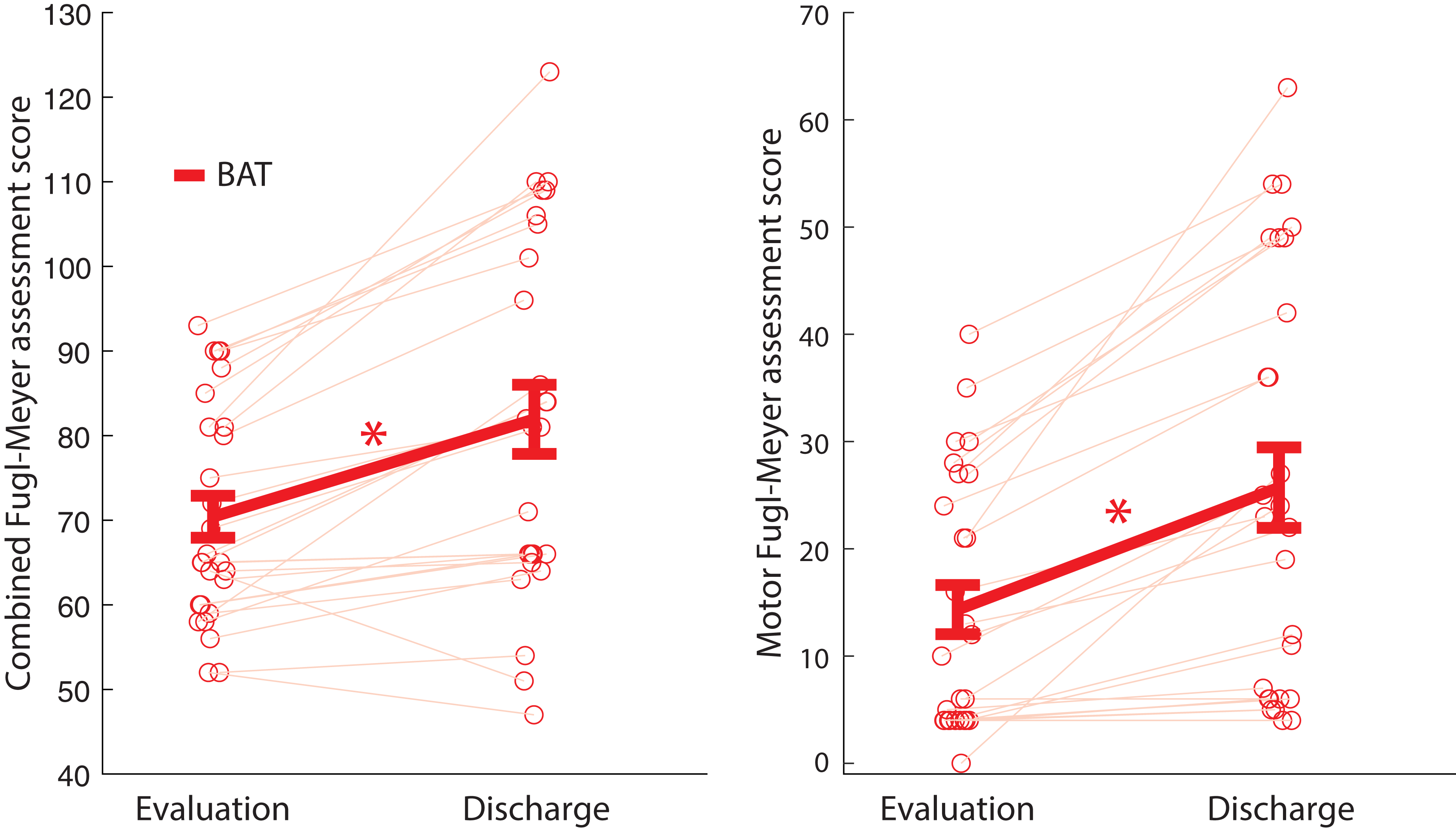
Combined and Motor-Only FMA–UE scores from evaluation to discharge in the BAT group.
Discussion
The existing literature contains very limited research on the BAT, especially in an IRF setting, because it is a novel device and not widely available. We hypothesized that patients with stroke in the BAT group would demonstrate statistically significant improvements in UE function compared with those in the control group. The results showed that both traditional occupational therapy services and occupational therapy services with the addition of the BAT resulted in significant improvements in UE function in patients with stroke. However, although the ARAT scores of each group improved, the BAT group did not demonstrate significant differences in ARAT scores compared with the control group. In addition, the BAT group demonstrated improvements in both the combined (sensory and motor) and Motor-Only FMA–UE scores.
Although FMA–UE scores were not available for the control group, past research has demonstrated statistically significant improvements in FMA–UE scores with standard occupational therapy treatments (Aydilek et al., 2022; Doğan, 2023). In a study that compared conventional occupational therapy services with specialty arm therapy services, a mean increase of 8 points was shown on the FMA–UE after conventional occupational therapy, demonstrating results similar to a mean of increase of 10 points shown in the experimental group (Dickey, 2021). In the existing literature, it does not appear that the BAT has a significant impact on change in FMA–UE scores compared with traditional occupational therapy services.
Several sample characteristics, including the amount of time poststroke, length of stay in the rehabilitation hospital, and age, were considered for the control and the BAT groups. All participants were in the acute phase after an ischemic stroke. According to Maulden et al. (2005), fewer days between stroke-onset symptoms and admission to an IRF were correlated with better functional outcomes at discharge. The participants in the control group had an average of 8.1 days poststroke, and those in the BAT group had an average of 7.3 days poststroke, which is in line with the literature that supports early intervention. The average length of stay for the control group was 18.9 days; for the BAT group it was 21.0 days. According to Camicia et al. (2016), stroke patients with severe impairment had an average length of stay of 22.2 days in IRFs, which correlates well with our participants. Finally, the average age of the control group participants was 69.7 yr, and the average age of the BAT group was 65.4 yr. According to Kissela et al. (2012), the average age for stroke has been lowering, with the average age in 2005 being 69.2 yr. This is comparable to the average ages of participants in this study. Howard et al. (2018) found that women age 45–75 yr are at a lower risk for stroke; however, men and women age ≥75 and older are at similar risk. Age differences among stroke recovery and outcomes measures may be worth investigating in future research.
One of the goals of the BAT is to increase the number of repetitions and practice volumes of the more affected UE poststroke. Although the role of practice volumes and schedules in neuroplasticity and motor learning has long been suggested, its role in stroke rehabilitation is less clear (Kleim & Jones, 2008). Literature reviews have found that poststroke UE training volumes may not moderate outcomes in traditional occupational therapy but may have a dose–response relationship in robotic training (French et al., 2010; Hayward et al., 2021; Kwakkel et al., 2008). Recent studies of lower poststroke extremity training volumes have shown a strong dose–response relationship, although at much higher volumes than have been described in UE rehabilitation (Hornby et al., 2015, 2020; Newton et al., 2023). Whether the inconsistent support for higher repetition UE training compared with lower extremity training is due to differences in affected vascular distributions or the training volumes that have been examined so far remains unclear.
Because of the nature of the IRF setting, our participants were involved in occupational therapy services on our unit only as long as they met criteria to remain in the IRF. The ultimate goal of our setting is to discharge patients to their home environment as safety allows. The discharge date is driven by patient’s functional outcomes, and each length of stay (which can be as short as 3–5 days) is patient specific. Therefore, our study required only three sessions of ≥10 min on the BAT program to maintain feasibility among patients’ varying lengths of admission. Patients would participate in these BAT sessions alongside sessions that emphasized ADL performance, IADL performance, and functional transfers. According to Wilfred (2020), community-dwelling participants with chronic stroke engaged in 12 1-hr sessions on the BAT over a 6-wk period and showed considerable improvements in FMA–UE scores. However, these patients also participated in standard occupational therapy services, and whether their outcomes were better than those of individuals in the community who did not use the BAT as part of their treatment plan is unclear. The effectiveness of the BAT in different treatment settings (i.e., outpatient) compared with patients who receive only traditional occupational therapy services is worth investigating.
Limitations
Several limitations should be considered when interpreting the results of this study. The sample size was small (n = 27) for both the control and intervention groups, and the long-term effects could not be evaluated because of participants being discharged from the IRF. In addition, this study had a quasi-experimental design, so there was no randomization of participants. Another limitation is that there were no FMA–UE scores available for the control group, so no comparisons could be made between the FMA–UE data and the BAT group’s data. Moreover, only the bimanual shoulder internal/external rotation program of the BAT was used; we did not consider for this study the other three available programs.
Another limitation is that no treatment interventions were withheld from participants; therefore, patients in both the control and the intervention groups may have received mirror therapy, neuromuscular electrical stimulation, strengthening, and other therapeutic interventions. These interventions were patient specific and were not the same from participant to participant. We could not control for these variables during this study because doing so would have potentially negatively affected patients’ outcomes. Because all participants received all other standard-of-care occupational therapy interventions, we could not determine which interventions best facilitated improvements in ARAT and FMA–UE scores given that both groups demonstrated improvements.
Implications for Occupational Therapy Practice
In this clinical trial, we investigated the use of an innovative virtual reality device in a population of persons with stroke. It has the following implications for occupational therapy practice: ▪ The BAT has considerable potential to be used as an intervention technique because it is practical and efficient for both patients and clinicians. ▪ Routine occupational therapy interventions alone may potentially be effective in improving UE outcomes among persons with stroke in an IRF setting. ▪ The BAT may have more potential for other levels of care outside of an IRF setting that may allow patients to use the programs more routinely and for longer durations.
Conclusion
Persons with stroke showed significant improvements in ARAT and FMA–UE scores from evaluation to discharge after the BAT intervention; however, improvements in ARAT scores after the BAT intervention were not significantly larger than those resulting from traditional occupational therapy sessions alone. Additional research is needed to understand how to optimize BAT interventions to maximize patient outcomes.
Footnotes
Acknowledgments
We acknowledge the occupational therapists who assisted with providing BAT treatment sessions to participants at the Johns Hopkins Bayview Specialty Hospital, as well as the persons with stroke who agreed to help further our knowledge in this important area of research. The registry number for the clinical trial is 05106595. This research was presented at the Johns Hopkins PM&R Research and Clinical Expo in 2022 and 2023.