
Abstract
These Practice Guidelines support interventions that promote access, inclusion, engagement, and optimal participation in occupations that are meaningful to autistic people across the lifespan.
Autism is often characterized by social communication differences and patterns of behavior, interests, or activities that may facilitate or hinder coping and adaptation. The current prevalence rate of autism among children in the United States is 1 in 36 children (Maenner et al., 2023), and hence there is an urgent need to develop supports and services that accommodate the autistic community’s differences and abilities while valuing them holistically (Botha et al., 2022; Kornblau & Robertson, 2021). Chang and Coster’s (2014) conceptual framework describes participation in life situations as active involvement in activities that are intrinsically social and occur in a societally defined context. Autistic people can face challenges that are due to societal attitudes and barriers that can greatly affect their participation in these contexts (Dwyer, 2022). The clinical and research communities have historically viewed autistic differences as deficits, an idea that has driven the research, for example, in the area of interests. These differences have historically been pathologized, and research evidence has been geared toward successful reductions (Patten, 2022) in these “restricted and repetitive” interests (Murthi et al., 2023).
As we shift our thinking in line with the advocacy community as to the importance and relevance of autistic interests, the research will, we hope, follow. In the occupational therapy profession, as well as special education and other related services, viewing people’s differences as deficits results in a focus on intervention and support or remediation instead of task or environmental modifications (Patten, 2022). The focus of such research has led members of the autistic community to camouflage or mask their symptoms, leading to exhaustion, burnout, anxiety, depression, and other negative mental health challenges. The concept of neurodiversity, in contrast, is reimagined and adapted from the term biodiversity (Singer, 2017). From the original description of neurodiversity, and through the inclusion of principles from the social model of disability, there is a growing acceptance that interventions need to be reimagined for the autistic community to accommodate both individual needs while emphasizing societal restrictions and challenges (Dwyer, 2022). As autistic people increasingly engage in self-advocacy, research and practice are moving beyond a deficit-based approach and are beginning to view the nuanced differences between nonautistic and autistic performance as rooted in a lack of understanding between the nonautistic and autistic communities (Chen et al., 2021; Davis & Crompton, 2021).
As research and practice communities expand their understanding of autistic people’s experiences, racial and ethnic inequities in diagnosis and service access persist. Studies have consistently shown disparities in the timely diagnosis of autism: White autistic children are diagnosed earlier than peers from historically marginalized groups (e.g., Durkin et al., 2017), and the latter access fewer intervention services (McManus et al., 2020). Later autism diagnoses and decreased intervention services matter because an early diagnosis positively influences developmental trajectories (Gabbay-Dizdar et al., 2022), and research shows that the intensity of intervention services, in particular early in life, result in increased functional outcomes for autistic people (McManus et al., 2019). Within autism research, recent investigations have pointed to the underrepresentation of historically marginalized racial and ethnic groups (e.g., Cascio et al., 2021; Steinbrenner et al., 2022; West et al., 2016), including underrepresentation in occupational therapy research (Little et al., 2024).
The inclusion of historically marginalized racial and ethnic groups in research is critical for many reasons, including, but not limited to, understanding how social systems work in unison to support autistic people, whether intervention efficacy may be generalizable across all people with autism, and how community members from marginalized communities perceive interventions. Moreover, research in occupational therapy with minoritized autistic people may be approached using frameworks such as minority stress models (Botha et al., 2022; Patten, 2022), which have explained the detrimental impacts that arise from a combination of proximal stressors (from internalized ableism) and distal stressors from a society not inherently designed and built to accommodate their needs. In addition, the concept of intersectionality may be used to study the ways in which socially constructed frameworks about specific identities intersect to perpetuate and reinforce exclusion and marginalization (Crenshaw, 1991).
Although systemic barriers stem from racial and ethnic identities among autistic individuals, ableist ideologies hinder access to services along the lifespan of this population (Jones et al., 2020). As Bottema-Beutel et al. (2021) explained, autism research is filled with ableist language that has the potential to harm autistic people. Ableism consists of “beliefs and practices that devalue and discriminate against people with physical, intellectual, or psychiatric disabilities and often rests on the assumption that disabled people need to be ‘fixed’ in one form or the other” (Smith, n.d.). Language choices are important and can inform attitudes toward and a general understanding of autism and how autistic people are perceived. Researchers should center and value autistic perspectives in their research and writing (Botha, 2021; Bottema-Beutel et al., 2021). Clinicians and researchers can use neutral and non-value–laden terminologies as descriptors to characterize autistic people’s cognitive functioning, challenge areas, and sensory or support needs. When professionals use neutral language, the accuracy, validity, and utility of non–value-laden descriptors increase, and an understanding of this population in nonautistic communities expands (Murthi et al., 2023; Natri et al., 2023; Pukki et al., 2022). Researchers and clinicians are increasingly taking autistic perspectives into account in their writing and participatory action research, and they are partnering with autistic researchers who research autism to incorporate into their work their expertise to inform education, practice, and research.
In these Practice Guidelines, we avoid ableist language, which includes the medicalization of autism (e.g., “special” needs or interests, “normal” or “typical” vs. autistic, “high” vs. “low” functioning), which often does not represent the experience of the autistic person. As occupational therapy practitioners, we can instead discuss people’s level of support needs, the barriers that autistic people face daily, and differences between the autistic and nonautistic experiences (Patten, 2022). We understand that autistic people’s interests are heterogeneous, diverse, and wide ranging. Some positive outcomes of using interests in autism research have been reduced anxiety and a calming effect (Patten Koenig & Hough-Williams, 2017), improved self-efficacy and self-determination, improved social communication, and development of knowledge and expertise in the participants’ area of interests (Murthi et al., 2023). Hence, the goal of these Practice Guidelines is to acknowledge and respect autistic people’s interests and to explore the existing evidence base to include interest-driven interventions (Gordon et al., 2015; Martin et al., 2020). Although we avoid ableist language throughout these Practice Guidelines, readers may note that the clinical recommendation tables include research that uses ableist language. This discrepancy is due to the nature of research published between 2013 and 2021, much of which may have been completed when remediation was emphasized and therefore used behavior modification and deficit-focused practices. The language in the tables reflects that used in the original articles and seeks to provide additional clinical rationales and strategies as part of these Practice Guidelines to support the adoption of neurodiversity-affirming and strengths-based practices for this population (Murthi et al., 2023).
These Practice Guidelines are based on four questions presented in several systematic review briefs (Baker et al., 2023; Benevides et al., 2023a, 2023b; Jirikowic et al., 2023a, 2023b; Little et al., 2023a, 2023b, 2023c, 2023d; Tomchek, Baker, et al., 2023; Tomchek, Dean, et al., 2023; Watling et al., 2023) and include autistic researchers as authors of three of the four review articles. Although acknowledging the hurdles associated with systematic reviews, in particular the time lag between dissemination and implementation of results, we opted to use Systematic Review Briefs in developing these Practice Guidelines because we were drawn to their inherent comprehensiveness. The systematic review questions were developed through continued collaborations and listening sessions with autistic community members, many of whom participated as authors (Appendix Figure A.1). The current Practice Guidelines updates the 2016 Occupational Therapy Practice Guidelines for Individuals With Autism Spectrum Disorder (Tomchek & Patten Koenig, 2016). The previous guidelines, which were based on a systematic review of research within the scope of occupational therapy, had minimal autistic community member input and focused on interventions for (1) social skills, social communication, restricted and repeated behaviors, play performance, and leisure participation; (2) sensory integration and sensory-based practice; (3) performance in work, activities of daily living (ADLs), instrumental activities of daily living (IADLs), and education; and (4) parent self-efficacy, family coping, and resiliency and family participation in daily life routines. At the time the prior Practice Guidelines were published, autistic priorities for research had not been well elucidated in the literature. This has since changed considerably given that research priorities have been identified by autistic people as well as their families (Clark & Adams, 2020; Davis & Crompton, 2021 ; Poulsen et al., 2022; Roche et al., 2021).
By integrating community member engagement and feedback into the current Practice Guidelines, we elucidated a different set of priorities addressed in the current review; specifically, these Practice Guidelines focus on positive mental health development; self- determination and self-advocacy; ADLs and IADLs, rest and sleep, work, education, play, and leisure occupations for children, adolescents, and adults; social participation and health management; person-, student-, and family-centered planning for adolescents and adults; and interventions to support participation in basic ADLs and IADLs among autistic children and adolescents (birth–18 yr).
Systematic Review Questions
These Practice Guidelines are based on the following four questions: What are the interventions in the scope of occupational therapy to support (or improve) self-determination and positive mental health for people on the autism spectrum (Patten et al., 2023a, 2023b)? What are the interventions within the scope of occupational therapy to address participation in ADLs, IADLs, rest and sleep, work, education, play, leisure, social participation, and health management among autistic children and adolescents (birth–18 yr; Baker et al., 2023; Little et al., 2023a, 2023b, 2023c, 2023d; Tomchek, Baker, et al., 2023; Tomchek, Dean, et al., 2023)? What are the person-, student-, or family-centered planning approaches within the scope of occupational therapy that foster the achievement of participation goals for autistic people and their families (Benevides et al., 2023a, 2023b; Watling et al., 2023)? Within the scope of occupational therapy, what interventions are effective for autistic people >18 yr that address participation in ADLs, IADLs, rest and sleep, work, education, play, leisure, social participation, and health management (Jirikowic et al., 2023a, 2023b)?
Goals of These Practice Guidelines
Through these Practice Guidelines, the American Occupational Therapy Association (AOTA) aims to help occupational therapy practitioners, as well as the people who manage, reimburse, or set policy regarding occupational therapy services, understand occupational therapy’s contribution in providing services to people on the autism spectrum and their care partners. These guidelines can also serve as a reference for health care professionals, health care facility managers, education professionals, education and health care regulators, third-party payers, managed care organizations, and those who conduct research to advance care of autistic persons.
These Practice Guidelines were commissioned, edited, and endorsed by AOTA without external funding being sought or obtained. They were financially supported entirely by AOTA and were developed without any involvement of industry. All authors of the reviews completed conflict-of-interest disclosure forms, with no conflicts noted. AOTA reviews Practice Guidelines, and updates them as needed, every 5 yr to keep recommendations on each topic current according to criteria established by ECRI (2020). Guideline topics are evaluated by a multidisciplinary advisory group consisting of AOTA members, nonmember content experts, and external community members. These Practice Guidelines were reviewed and revised on the basis of feedback from a group of content experts on autism that included practitioners, advocates, researchers, educators, practitioners, and policy experts. Reviewers who agreed to be identified are listed in the Acknowledgments.
These Practice Guidelines report the findings from systematic reviews of published scientific research focused on topic-specific questions. The systematic reviews were conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting systematic reviews (Moher et al., 2009). The protocol and questions were developed with input from a multidisciplinary advisory group that also included consumers and information end users. A medical research librarian conducted searches of the literature, and review teams evaluated the search results and synthesized the findings (see the Appendix for an overview of the systematic review methods and findings). Interventions that were described in sources other than the published literature and that did not meet the inclusion criteria were excluded from the reviews.
Occupational therapy practitioners should not consider these Practice Guidelines to be a source of comprehensive information about autism or about application of the occupational therapy process. The occupational therapy practitioner makes the ultimate clinical judgment regarding the appropriateness of a given intervention considering a specific client’s or group’s circumstances, needs, and response to intervention, as well as the evidence available to support the intervention. Examples of how evidence can inform practice with autistic people are included in the “Case Illustrations and Evigraphs” section.
AOTA supported the systematic reviews on the effectiveness of interventions within the scope of occupational therapy for autistic people as part of its Evidence-Based Practice (EBP) Program. AOTA’s EBP Program is based on the principle that the EBP of occupational therapy relies on the integration of information from three sources: (1) clinical experience and reasoning, (2) preferences of clients and their families, and (3) findings from the best available research. The systematic reviews and these Practice Guidelines report the findings from the best available research.
Clinical Recommendations for Occupational Therapy Interventions for Autistic People
Clinical recommendations are the final phase of the synthesis of systematic review findings. The findings for each systematic review question are graded in terms of how confident a practitioner can feel that using the interventions presented will improve the outcomes of interest to their clients. The grade is based on the specificity of the intervention, number of studies supporting the intervention, levels of evidence of the studies, quality of the studies, and significance of the study findings. Interventions included in the clinical recommendations are specific to a population, and the articles that describe them provide sufficient detail for practitioners to understand the intervention and the outcomes of interest.
Describing the strength of clinical recommendations is an important part of communicating an intervention’s efficacy to practitioners and other users. The recommendations for these Practice Guidelines were evaluated and finalized by AOTA staff, the AOTA research methodologist, and systematic review and Practice Guidelines authors. AOTA uses the grading methodology provided by the U.S. Preventive Services Task Force (2018) for clinical recommendations. The clinical recommendations pertaining to each review, along with the studies’ level of evidence and supporting details, are presented in Tables 1 through 4.
Clinical Recommendations for Improving Self-Determination and Positive Mental Health
Note. ADLs = activities of daily living; ASD = autism spectrum disorder; BIACA = Behavioral Interventions for Anxiety in Children with Autism; CBT = cognitive–behavioral therapy; IADLs = instrumental activities of daily living; MBSR = mindfulness-based stress reduction; MBT–AS = mindfulness-based therapy for autism spectrum disorders; NR = not reported; PEERS = Program for the Education and Enrichment of Relational Skills; PEGASUS = Psychoeducation Group for Autism Spectrum Understanding and Support; TAASD = Treatment of Anxiety in Autism Spectrum Disorder.
Clinical Recommendations for Clients Age ≤18 yr: ADLs, IADLs, Rest and Sleep, Work, Education, Play, Leisure, Social Participation, and Health Management
Note. ABA = applied behavior analysis; ADHD = attention deficit hyperactivity disorder; ADLs = activities of daily living; ASD = autism spectrum disorder; CBT = cognitive–behavioral therapy; GoriLLA = Growing, Learning, and Living with Autism; IADLs = instrumental activities of daily living; ICPS = I Can Problem Solve; ImPACT = Immediate Post-concussion Assessment and Cognitive Testing; JASPER = Joint Attention Symbolic Play Engagement and Regulation; NR = Not reported; PEBM = parent education and behavioral management; PEERS = Program for the Education and Enrichment of Relational Skills; PRISM = Practical, Robust Implementation and Sustainability Model; PT/ST = Play Time/Social Time; PRT = Pivotal Response Treatment; SCERTS = Social Communication, Emotional Regulation, and Transactional Support; SST = social skills training; SST–PTI = social skills training with parent–teacher involvement; START = Social Tools And Rules for Teens.
Clinical Recommendations: Person-Centered, Student-Centered, or Family-Centered Planning Approaches
Note. ACCESS = Acquiring Career, Coping, Executive-Control, and Social Skills; ADHD = attention deficit hyperactivity disorder; APCP = Assessment of Preschool Children’s Participation; ASD = autism spectrum disorder; CI–ASD = Contextual Intervention adapted for Autism Spectrum Disorder; COPM = Canadian Occupational Performance Measure; COPM–2 = COPM, 2nd Edition; GAS = goal attainment scaling; GPA = grade point average; ID = intellectual disability; IFit = Into Fitness Together; NR = not reported; PCP = person-centered planning.
Clinical Recommendations for Clients Age >18 Yr: Participation in ADLs, IADLs, Rest and Sleep, Work, Education, Play, Leisure, Social Participation, and Health Management
Note. ACCESS = Acquiring Career, Coping, Executive-Control, and Social Skills; ADLs = activities of daily living; ASD = autism spectrum disorder; CBT = cognitive–behavioral therapy; NR = not reported; IADLs = instrumental activities of daily living; PEERS = Program for the Education and Enrichment of Relational Skills.
For the purpose of these Practice Guidelines, we report recommendations graded A, B, and D, the grades that best support clinical decision-making: A: There is strong evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. Strong evidence was found that the intervention improves important outcomes and that benefits substantially outweigh harms. B: There is moderate evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. There is high certainty that the net benefit is moderate, or there is moderate certainty that the net benefit is moderate to substantial. D: It is recommended that occupational therapy practitioners not provide the intervention to eligible clients. At least fair evidence was found that the intervention is ineffective or that harms outweigh benefits. In these reviews, we did not find Grade D evidence.
These grades are reported in Tables 1 through 4 and designated with green, indicating should consider if appropriate (A), or yellow, indicating could consider if appropriate (B). None of the studies included in these reviews reported adverse events or harms related to the interventions evaluated (D).
The complete findings from the systematic reviews can be found in the Systematic Review Briefs on this topic published in the American Journal of Occupational Therapy (Baker et al., 2023; Benevides et al., 2023a, 2023b; Jirikowic et al., 2023a, 2023b; Little et al., 2023a, 2023b, 2023c, 2023d; Tomchek, Baker, et al., 2023; Tomchek, Dean, et al., 2023; Watling et al., 2023). As always, practitioners’ clinical decisions should be informed by the evidence presented in these Practice Guidelines in combination with their clinical experience and the client’s particular goals.
Translating Clinical Recommendations Into Practice
Clinical Reasoning Considerations
Very rarely will practitioners find an evidence-based intervention that perfectly fits their clinical setting and the client’s specific needs. Occupational therapy practitioners need to consider several questions as they evaluate the research and consider whether they can use an intervention, or adapt it in a well-reasoned way, to exact meet the client’s needs (Highfield et al., 2015): Exactly what intervention do I need to provide? What types of client outcomes am I looking for? Do the studies located provide enough detail on the intervention so that I know what to do and how to do it? How well do the conditions in which I will provide the intervention match those in the studies? What are the demographic characteristics (e.g., age, gender, diagnosis, comorbidities) of the participants in the research studies? In which setting (e.g., inpatient, home, community, school) did the studies take place? Do any contextual factors (e.g., resources, policies) that are different from those in the studies influence my ability to provide the intervention? How flexible is the intervention, and how much can I modify or adapt it? If my setting or client population differs from those of the studies, can I modify or adapt the intervention without changing its integrity? If I modify or adapt the intervention, what client characteristics (e.g., comorbidities) do I need to consider? Can I be proactive and plan how to modify or adapt the intervention before I start implementing it? Can I make minimal changes to the intervention, such as reordering the content of the sessions, or does the need for substantial changes indicate I should select another intervention?
To modify or adapt evidence-based interventions in practice, practitioners must plan and proactively think through the changes they need to make to fit the intervention to the client and practice setting. In addition, they must document how and why they altered the researched intervention so others in their setting know how to implement the intervention and why the changes were made. If an intervention must be adapted extensively, it may not be the right fit for the situation. If extensive adaptations to the intervention are necessary, the intervention is probably not right for the client or setting. If the practitioner finds that the intervention does not suit the client, they should not use that intervention.
Case Illustrations and Evigraphs
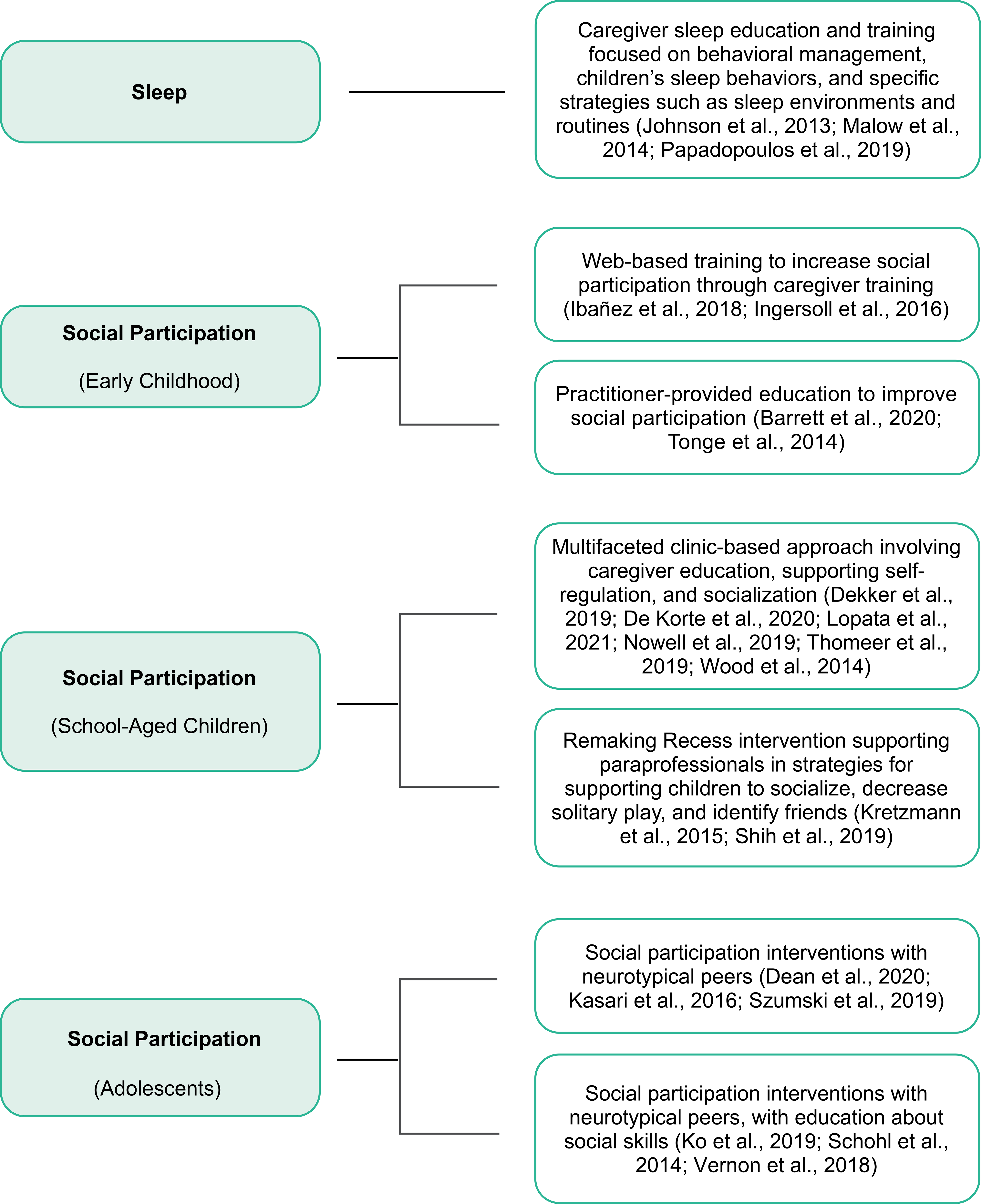
The case studies in this section illustrate how occupational therapy practitioners can translate evidence from the systematic reviews to professional practice when collaborating with autistic individuals. Each case study highlights interventions that are supported by evidence and expert opinion. Evigraphs developed by AOTA staff based on the clinical recommendations are also included (Figures 1–3); each evigraph can be used to guide decisions and actions for practitioners to take. Practitioners must consider each potential intervention in relation to the client’s individual goals, interests, habits, routines, and environment and choose interventions that strongly align with or are supportive of these factors in the context of the client’s occupational profile.
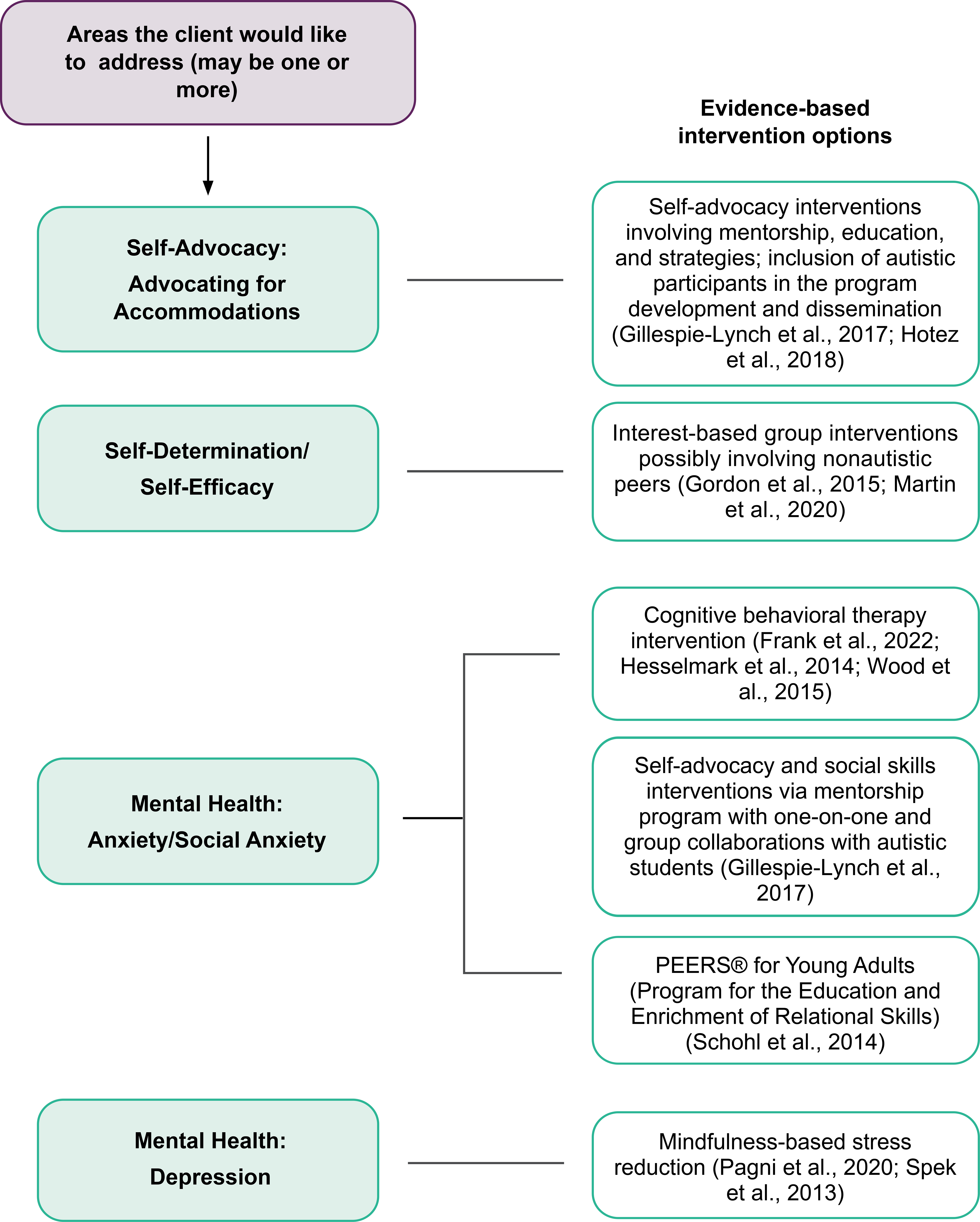
Interventions to improve self-advocacy, self-determination and self-efficacy, and mental health.
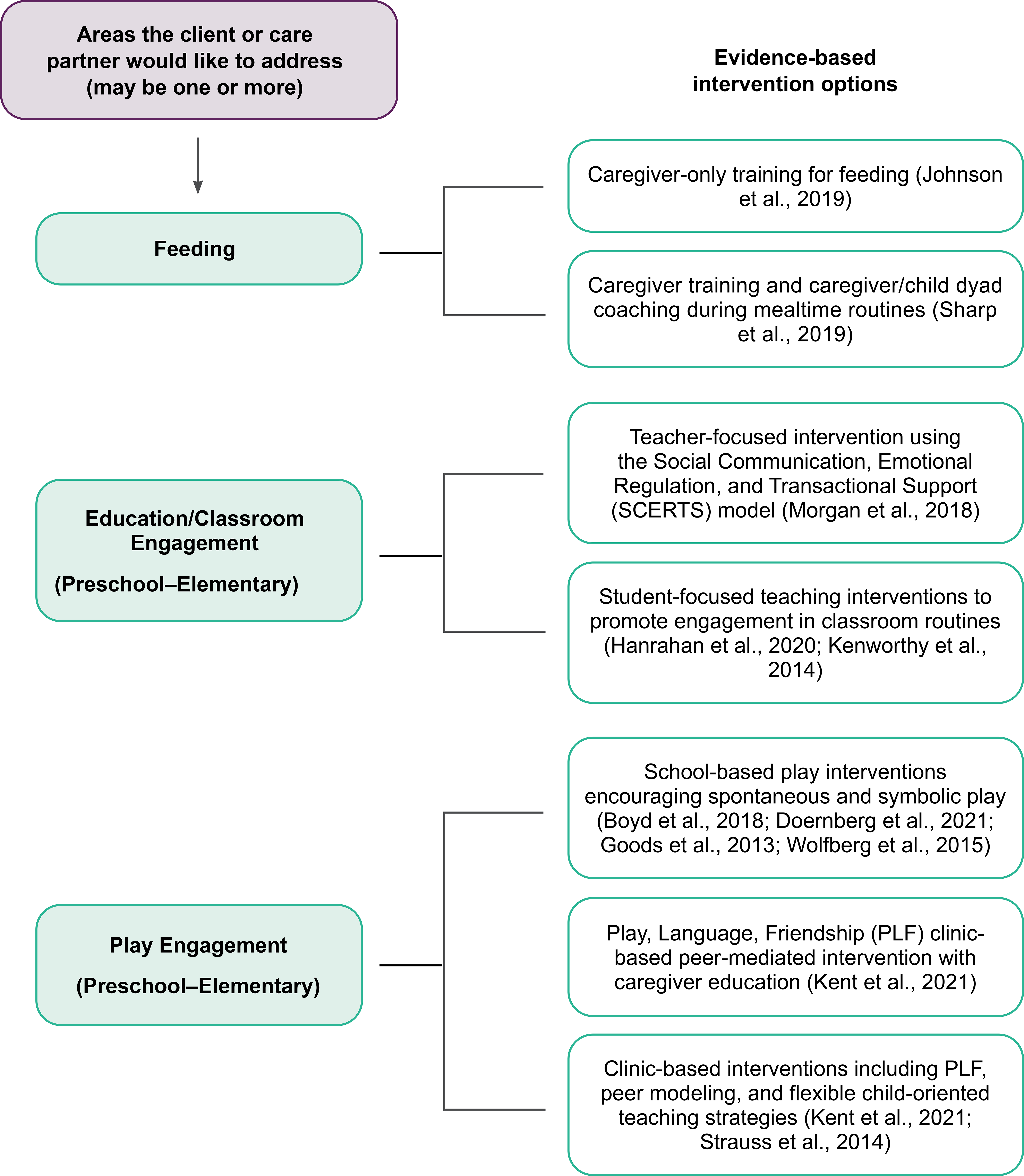
Interventions to improve activities of daily living, instrumental activities of daily living, rest and sleep, work, education, play, leisure, social participation, and health management for children and youth.
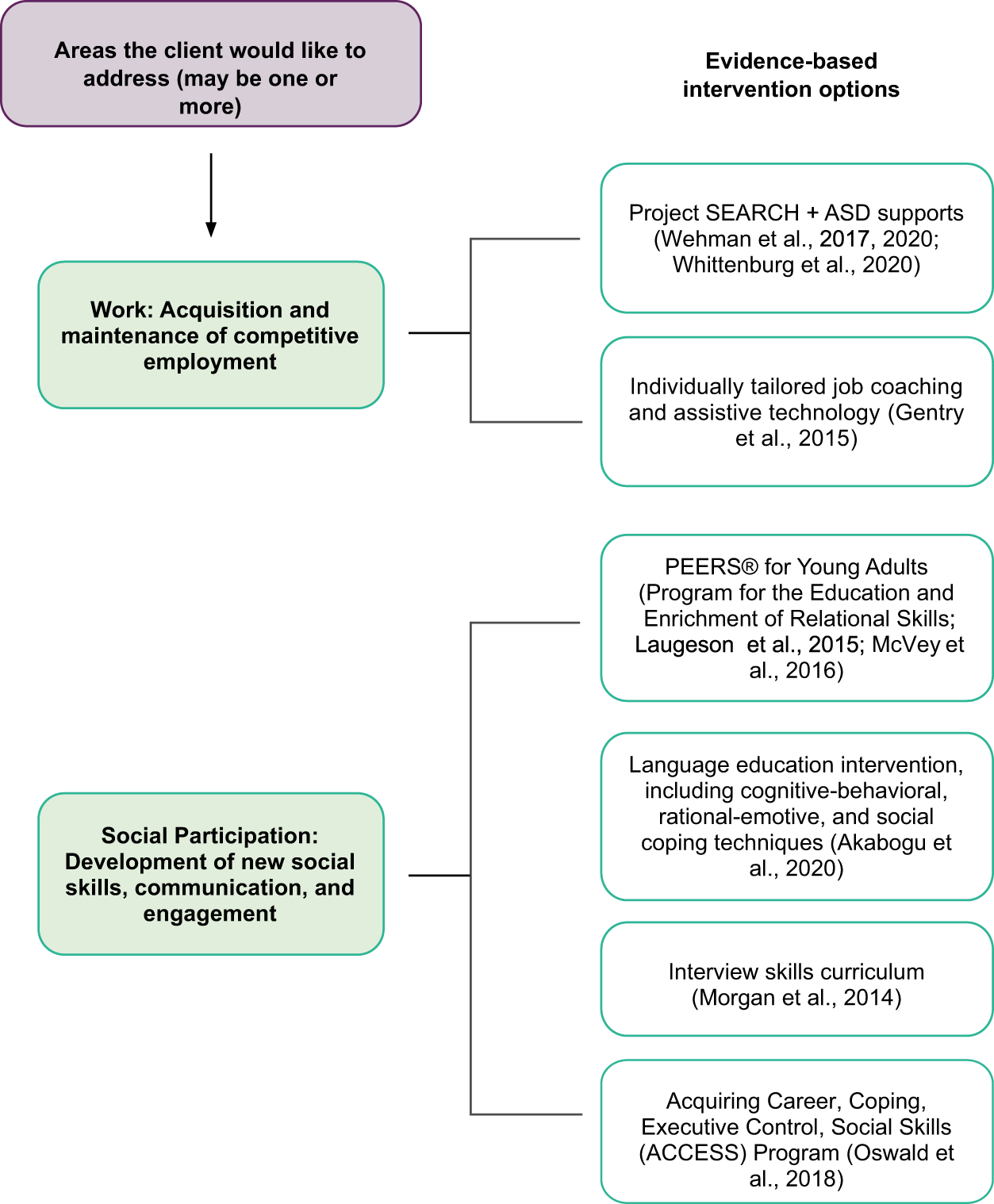
Interventions to improve activities of daily living, instrumental activities of daily living, rest and sleep, work, education, play, leisure, social participation, and health management for adults.
Case Study 1: Jade
Occupational Profile
Jade’s occupational therapist initiated the evaluation using AOTA’s (2021) Occupational Profile Template as a guide to collect relevant information. Jade is a 6-yr-old soon-to-be-kindergartener. She lives in an apartment with her mother, Betsy, and 3-yr-old brother, Derek, on the west side of Chicago. Betsy has lived in this neighborhood for much of her life. Her mother lives close by, as does her sister’s family. Betsy and her children are active in their church and connect with family on the weekends. Betsy works in the office at the public school Jade will attend next fall.
Jade has a strong bond with Betsy and spends most of her time with her. Betsy describes Jade as spirited, energetic, smart, strong, and independent. She notes that Jade is “a wiz with her cell phone and anything with a screen.” She loves how Jade immediately dances when she hears music and relayed that the Sunday school teacher says Jade has “never heard a song she didn’t like.” Jade loves Junie B. Jones and always picks a Junie B. Jones book to read with Betsy. She is protective of Derek, and if he is hurt she tries to comfort him with hugs.
Jade was diagnosed with autism spectrum disorder at age 5 yr. Her speech has been delayed since early in life. In addition, Betsy has had long-standing concerns about how Jade responds in specific situations. As long as she can remember, it has been challenging to take Jade to stores because she will become upset and will run off if she is not in a cart. Jade also has difficulty while at the park playing with her cousins and other children; Betsy says Jade does not respond when peers try to engage her, and she prefers to walk around the perimeter of the park. Betsy indicates that Jade is selective about when she engages in play with her cousins at family gatherings and most often does so if all are moving (e.g., dance party, chase). She also likes spinning on the swings at the park. Jade has always had inconsistent sleep patterns and limits her diet to a few foods. She has maintained a stable growth pattern, although Betsy is concerned about her health and nutrition because of her limited variety of foods and inconsistent sleep.
Betsy and Jade received early intervention services from an occupational therapist and speech pathologist to support social–communication development and additional play and adaptive concerns. Betsy reports that she often adjusts activities and routines to support Jade’s participation. She explains that most often she has to break things down or get rid of outside distractions to support Jade’s attention to a particular activity. At the time of transition to preschool services, Betsy and the pediatrician discussed Jade’s continued speech delays and daily challenges. At that time, the pediatrician mentioned that Jade may have a diagnosis of autism spectrum disorder. Preschool services were initiated on the basis of her developmental delay. Consultative speech and occupational therapy services were added to Jade’s Individualized Education Program (IEP). An interdisciplinary evaluation conducted more than 1 yr later at a university-affiliated tertiary diagnostic center confirmed the autism diagnosis.
Jade is transitioning from preschool to elementary school. Betsy is both excited and apprehensive that Jade will be in the building in which she works during the school day. Given the challenges Jade has experienced in preschool, Betsy is thankful she will be there to support her when needed but is concerned about the impact of Jade’s school performance on her own interactions with the school staff. Jade’s IEP continues to include both occupational therapy and speech pathology consultations. Betsy is familiar with the school-based occupational therapist and knows that occupational therapy in schools is focused on academic performance. Occupational therapy consultations in the school, according to the IEP’s specially designed instruction and statement of related services, will focus on classroom engagement and social participation at recess. Betsy wants direct support with Jade’s sleep and eating difficulties as well as outpatient services to address Jade’s occupational performance at home and in the community. Betsy attends a local outpatient clinic with Jade to supplement the school-based occupational therapy services. She wants to set Jade up for success when she starts kindergarten in the fall, and she feels getting Jade’s sleep and mealtime routines to a better place would lay the foundation for successful participation in school. With a lens for supported decision-making, Jade was asked about her priorities to guide the initial evaluation and goal planning. She was asked open-ended questions, and brainstorming supported the interaction. She quickly indicated she wanted to have more friends to chase or dance with on playdates.
Occupational Therapy Initial Evaluation and Findings
To ensure consistency of services across school and the clinic, the occupational therapist reviewed Jade’s school records, evaluation findings, and planned interventions. She also set up a phone call with the school-based occupational therapist to brainstorm about how to build on Jade’s strengths and interests across therapy settings. During a classroom-based observation in the preschool setting, the occupational therapist reported that Jade most often explored the classroom on her own and demonstrated minimal social initiation with peers. When peers attempted to engage with Jade by sharing a toy or pulling her into an activity, she joined in only when situations involved dancing or movement. While in centers, Jade was content to engage in an activity on her own in the corner of the area. Classroom observations and teacher reports noted that her most frequently selected centers were the sand and water, computer, and music and movement ones. At recess and during free play, she tended to stay to herself on the periphery of the area. She needed redirection and support from an instructional assistant to manage her school materials (e.g., organize her desk) and complete school tasks. The school report stated that the School Function Assessment (Coster et al., 1998) will be administered at the start of the school year to validate classroom observations highlighting cognitive–behavior task assistance and adaptations that would support Jade’s activity participation in the classroom during playground and recess and in snack and mealtime settings. Relevant occupational therapy–supported goals on the IEP included the following: Jade will engage in a collaborative activity she chooses with a peer for a 10-min period in a preferred center (i.e., sand and water, computer, or music and movement) given graded adult support from teacher or instructional assistant. Jade’s attention will be congruent with the circle time activity (e.g., weather, story) during a 10-min period with environmental and sensory supports. Jade will engage in turn-taking activity or cooperative play activity with peers at recess 50% of the period when on the playground daily after receiving peer education and with graded adult support.
Jade was initially cautious when entering the open clinic, staying close to Betsy’s side and holding her hand. She acknowledged the occupational therapist, who responded by giving her a fist bump. Jade quickly warmed to the setting when she saw a reading corner and plopped herself down in a soft beanbag. As Betsy and the occupational therapist chatted, Jade checked in visually for reassurance as she slowly started exploring the sand table.
On the basis of Betsy’s requested focus of intervention on feeding and mealtime routines and sleep, coupled with Jade’s goals of developing a circle of friends, the analysis of occupational performance (AOTA, 2020) relied on the Short Sensory Profile 2 (SSP–2; Dunn, 2014), the Adaptive Behavior Assessment System: Third Edition (ABAS–3; Harrison & Oakland, 2015), and the Brief Autism Mealtime Behaviors Inventory (BAMBI; Lukens & Linscheid, 2008), to supplement clinical observation and inform collaborative goal planning. The assessment findings are summarized in Table 5.
Jade’s Initial Evaluation Results
M = 100, SD = 10.
The results of the ABAS–3 highlighted Betsy’s social (leisure and social participation) and practical (home living, health and safety, self-care) concerns for Jade. Betsy’s report on the SSP–2 indicated that Jade’s primary sensory patterns relate to sensory seeking and sensitivity. Jade was reported to struggle to complete tasks and to maintain focused attention, especially during nonpreferred tasks. She is distracted when there is background noise and was noted to be observant of her surroundings and to look away from tasks to notice actions in a room. These habits, like her sensory seeking, affect Jade’s ability to successfully engage in activities. Jade was noted to pursue movement and will frequently bounce her foot or rock in her chair when in an activity. She also often jumps from one activity to another, and she shows strong preferences for particular tastes and will refuse unfamiliar tastes or food textures. The sensory and behavioral sections of the ABAS–3 highlighted considerations for intervention planning.
Clinical observations during the evaluation validated Betsy’s report. Jade was easily engaged in play-based routines that evaluated self-regulation, executive functioning, and motor control when choices for activities were provided. Jade’s activity choices were used to create a schedule of activities. These activities were conducted in a private, enclosed room because she required additional prompts for task completion when activities were initially attempted in the open clinic gym. Periodic breaks in the open clinic gym during desirable activities (e.g., swing, scooter board) and snacks were embedded into the schedule. Activity progression and self-monitoring strategies supported Jade’s transition back to the private room. Taking into consideration sensory-seeking and sensitivity pattern influences on Jade’s observable behavior will be important to highlight when collaborating with Betsy and Jade during interventions. Specific to reported sleep difficulties, Jade often has difficulty “calming down” to fall asleep. Betsy reports Jade will rock in her bed and sing for extended periods before she falls asleep. Once asleep, Jade has difficulty maintaining her sleep. When she wakes up, it is difficult to get her to lie back down; she instead tries to engage with her toys in her bedroom. Betsy reports that she must be extremely quiet and limit her movement and activity in the apartment for fear that she will wake Jade up.
Additional information was gathered about ongoing mealtime routines by report and clinical observation during simulated snack breaks. Betsy noted that Jade has always been “finicky” and “selective” in the foods she will eat. A list of foods in Jade’s current diet was obtained. When the BAMBI was used to gather structured information, Betsy reported that Jade often, or almost always, is inflexible about mealtimes, does not accept a variety of foods, prefers the same foods with each meal, and dislikes certain foods and will not eat them. Jade prefers crunchy foods at home. She selected only crunchy snacks (i.e., chips, pretzels, BelVita bars) during the evaluation. When asked about her preferred foods, Jade said she likes to “chew food and really feel the food in [her] mouth.” She also noted she does not like to “have to use a spoon.” She typically walks around during mealtimes rather than sitting for a meal at the table. Jade also prefers to have food prepared and served in a particular way. In general, Jade was reported to have food selectivity, food refusal, and mealtime rigidity.
On the basis of Jade’s assessment results, the occupational therapist, Betsy, and Jade talked about priority goal areas and potential goals. They clarified what success will look like. Betsy and Jade collaborated with the occupational therapist to establish the following goals for treatment: Jade will add at least five new foods to the established list of foods she will eat that are typically served at school in the lunchroom or are easy to bring to school from home before the start of school in fall. Jade will be in bed by 9:00 p.m. for her bedtime routine of reading and rocking with Betsy. By 10:00 p.m., lights will be out and Jade quiet. Jade will respond to her cousin’s attempts to engage her in play at family gatherings for cooperative play. Jade will have a monthly playdate with a friend from school on the school playground.
Occupational Therapy Interventions at School
Attention to Classroom Activities
On the basis of the evidence, the occupational therapist collaborated with Jade’s classroom teacher to improve Jade’s attention to tasks using principles from the Social Communication, Emotional Regulation and Transactional Support (SCERTS) model (Morgan et al., 2018), which integrates the child’s goals into classroom activities and targets antecedent-based positive behavior supports. For example, Jade’s goal of attending for 10 min during circle time was integrated into all group-based classroom activities. Jade’s teacher would use a timer so Jade could see the passage of time and understand how much time was left. The teacher and the occupational therapist collaborated on ways to grade the activity; they planned that Jade would attend group-based activities for 3 min at the beginning of the school year with the goal of slowly increasing the amount of time. In addition, the occupational therapist developed social narratives to prepare Jade for classroom tasks and engagement (e.g., Hanrahan et al., 2020). When Jade had a social narrative about what was going to happen in circle time (e.g., “First you sit on your circle spot, then the teacher reads a story”), she knew what to expect and was better able to attend.
Socialization With Peers
The occupational therapist worked with Jade’s classroom teacher to provide an integrated playgroup in the classroom with peers to promote Jade’s social communication and social reciprocity (Wolfberg et al., 2015). Because the teacher had concerns about the social communication of many students in her class, she was receptive when the occupational therapist offered to hold a small group in the classroom every Wednesday afternoon. During this small group, the occupational therapist paired Jade with one peer who shared her interest in music and dance, and they engaged with two other dyads. The small group focused on social reciprocity (e.g., responding to gestures or words, recognizing nonverbal cues, turn-taking) and symbolic play. Given Jade’s interest in water play and sand (driven by her sensory-seeking nature), the occupational therapist paired Jade with a student who also enjoyed messy activities, so they could engage in activities that fulfilled both of their sensory needs.
In addition, the occupational therapist worked with the classroom teacher and school paraprofessionals to implement the Remaking Recess intervention (Kretzmann et al., 2015), in which the occupational therapist shared information with the paraprofessionals and spent 1 day/wk coaching on the playground to help them support unengaged children on the playground. Although this was an investment of time at the beginning of the school year, the occupational therapist saw that the paraprofessionals were increasingly engaged with children on the playground and had the knowledge and strategies to support Jade and other unengaged children throughout the school year.
Occupational Therapy Interventions at Home and in the Community
Mealtimes
The occupational therapist used parent coaching on behavioral strategies to promote structure and consistency during mealtimes (see Johnson et al., 2019; Sharp et al., 2019); specifically, the occupational therapist visited Jade and Betsy during a meal to observe the authentic routine and problem-solve together strategies to more effectively structure mealtimes. The occupational therapist suggested that Betsy offer Jade a nonpreferred food followed by a preferred food and limit screen time during meals. Because Jade prefers crunchy foods, the occupational therapist and Betsy brainstormed about healthy foods that could be introduced during mealtimes that meet Jade’s sensory preferences.
Sleep
On the basis of the assessment data, the occupational therapist noted that Jade shows sensory-seeking and sensory sensitivity. Her sensory seeking means that she is always “on the move,” so it takes her a little longer to calm her body and get ready for sleep. In addition, her sensory sensitivity means that noises wake her easily. The combination of these sensory patterns makes it difficult for Jade to fall asleep and stay asleep. The occupational therapist used parent coaching and education about children’s sleep behaviors, including prevention techniques for bedtime routines, and reinforcement to address Jade’s sleep (see Johnson et al., 2013; Malow et al., 2014; Papadopoulos et al., 2019). The occupational therapist coached Betsy on ways to promote relaxation, routine, and sleep hygiene at bedtime as well as how to not positively reinforce Jade’s nighttime waking (e.g., no television or playing during the night).
Play
The outpatient occupational therapist chose to support Jade’s play by meeting Betsy, Jade, and Jade’s cousin at the playground. The occupational therapist knew that incorporating a peer would support Jade’s play and social interaction development (Dean et al., 2020; Kasari et al., 2016; Szumski et al., 2019), so the occupational therapist and Betsy instructed Jade’s cousin on how to initiate interactions with Jade. When Jade’s cousin initiated a game, the occupational therapist coached Betsy on how to support Jade’s response. Betsy joined in the game, modeled a response, and then offered Jade a reward (e.g., a sticker) when Jade would follow her cousin’s lead for a game of tag or a race around the playground.
Outcomes
Goal attainment was the primary consideration for discharge. By the end of the school year, Jade had reached all her IEP goals (Table 6). She attended during circle time with visual and sensory supports and was engaging in cooperative play at the sand and water centers in the classroom. Betsy reported that Jade would fall asleep more quickly but continued to sometimes have night wakings. With regard to eating and mealtimes, Betsy no longer offered screen time during mealtimes, and Jade had incorporated new crunchy foods into her diet, including snap peas, veggie straws, and granola bars. Jade also was responsive to her cousin’s bids for social interaction and followed along in active games.
Jade’s Discharge Evaluation Results
M = 100, SD = 10.
Case Study 2: KJ
Occupational Profile
KJ (they/them/their) is a 13-yr-old autistic student entering eighth grade at an inclusive community public school. KJ migrated to the United States from Central America with their family when they were age 4 yr. Although 9 yr have passed since then, KJ and their family still experience stress related to cultural differences and leaving their close extended family. KJ has an IEP and receives support from a reading specialist; team consultations with English-language–learning staff; and direct and indirect school-based services, including counseling, speech-language therapy, and occupational therapy. KJ has been immersed in a transitional bilingual education program since they were age 4 and has acquired language proficiency over 9 years. Although KJ’s parents have acquired some English language skills over time, effective communication between home and school personnel requires the assistance of an interpreter. The current occupational therapy evaluation is in preparation for KJ’s upcoming IEP meeting, which will be their last IEP meeting before beginning to plan for the transition to eighth grade.
Occupational Therapy Initial Evaluation and Findings
Using AOTA’s (2021) Occupational Profile Template as a guide, KJ’s occupational therapist conducted the evaluation, which revealed the following:
KJ has a strong bond with their math teacher and basketball coach. These two have become important social connections and provide guidance, support, and encouragement, contributing to KJ’s academic and personal growth and development.
KJ’s homeroom teacher describes them as a compassionate, diligent student who is motivated to learn and succeed.
KJ displays a keen interest in math and basketball, deriving joy from engaging in both activities and participating in Mathematical Olympiads for Elementary and Middle School (https://moems.org/) and the school’s basketball team.
KJ experiences social anxiety, which results in heightened self-consciousness, a tendency to withdraw from new situations, a reluctance to engage with others, and an aversion to attending school. At times, they have difficulty using spoken language in these situations, but they have adapted to using a text-to-speech app on their phone.
KJ expresses fondness for basketball, finding joy in playing it and engaging in mental math games. Although they occasionally prefer solitude, they express openness to being in the company of others with similar interests, such as their math teacher and basketball coach.
KJ’s team would like to focus on promoting KJ’s self-advocacy and participation in school-related occupations. Their school uses strengths-based approaches (Koenig & Kinnealey, 2010; Kotler & Koenig, 2012; Lanou et al., 2012) in which all students are provided with the opportunity to create an aspirational goal, which facilitates their growth and development in skills they find fulfilling and in which they feel competent. KJ was evaluated with goal attainment scaling (GAS; Mailloux et al., 2007), an individualized assessment that focuses on goal selection and scaling that takes a standardized approach. GAS promotes client involvement in the assessment and intervention process and promotes multidisciplinary team collaboration (Cardillo & Choate, 1994). Additional findings from the evaluation are provided in Table 7, an explanation of GAS is provided in Table 8, and resultant goals and benchmarks are listed in Table 9.
Assessments and Findings: KJ
Note. AIR = American Institutes for Research; NA = not applicable.
Goal Attainment Scaling: Levels of Expected Outcome
KJ’s Goal Attainment Scaling Scores
After coordinating with the reading specialist, English-language–learning staff, counselors, a speech-language therapist, and KJ’s parents, the occupational therapist and KJ developed the following goals. KJ provided their input using the text-to-speech software on their phone.
KJ will improve their ability to set three goals for themself. KJ will improve their ability to cope with anxiety using the Behavioral Interventions for Anxiety in Children with Autism (BIACA) program (Frank et al., 2022; Wood et al., 2015). KJ will use the KICK (Knowing I’m Nervous, Icky Thoughts, Calm Thoughts, and Keep Practicing) plan, which is part of the BIACA program (Wood et al., 2008, 2009), independently over the course of 3 wk to report the use of positive coping skills to deal with anxiety-inducing situations and will use coping skills when exposed to situations that increase their anxiety. When needed, KJ will develop confidence in understanding the importance of self-advocacy and effectively advocating for their needs, rights, and accommodations when seeking help.
They also set an aspirational goal: KJ will show and teach a math problem-solving game that they designed to a chosen peer during lunchtime. An example of how KJ’s goals were determined using GAS is presented in Table 8.
Occupational Therapy Interventions
At the IEP meeting, the decision was made that KJ would receive weekly group-based occupational therapy sessions in school with up to four other students over the next academic year, as well as indirect consultation with the occupational therapy practitioner about KJ’s leisure and productivity, use of effective coping strategies and assistance with problem-solving, and use of coping skills as needed. The sections that follow describe evidence-based interventions that could be implemented with KJ by an occupational therapist or occupational therapy assistant.
KJ’s occupational therapist and occupational therapy assistant comprehensively reviewed existing interventions and found that social skills training by Dekker et al. (2019) had strong levels of evidence (2b and 1b). However, KJ’s therapy team consciously decided to avoid these interventions because they focused on normalizing KJ’s social skills by using reinforcers to promote nonautistic patterns of social communication. Instead, KJ’s occupational therapist and the other team members agreed that the reinforcement would be intrinsic when their strengths and interests are authentically incorporated into an interest-based club. Moreover, evidence from a recent scoping review by Murthi et al. (2023) highlighted that incorporating strengths and interests into interventions alleviated negative mental health symptoms, increased skill acquisition around interests, and facilitated the development of a sense of belonging and community. Hence, KJ’s therapy team decided they would enjoy participating in a meaningful activity (Ryan & Deci, 2000), so they created a strengths- and interest-based club to promote KJ’s competence and mastery.
Competence and Mastery
Half of the group-based intervention sessions focused on competence- and mastery-related interventions using KJ’s strengths in an after-school program. Interventions recognized the importance of autonomy, relatedness, and competence, which are core components of self-determination theory (Ryan & Deci, 2000). Students in the program worked on gaining competence in areas of interest, which in KJ’s case is math. KJ’s occupational therapists adapted an inclusive, informal after-school engineering club model that was based on Martin et al.’s (2020) study to help develop self-determination skills. In the program, students could choose math problems from a 14-wk curriculum that focused on a new topic every week. They could solve problems, choose a theorem, and dissect it during the 45-min weekly session. They could work together or independently to find solutions. The students were encouraged to invite teachers, peers, and parents to a final showcase event. This program was intended to enhance students’ mastery of mathematics by providing multiple opportunities to solve challenging problems in a safe club environment. At the end of the school year, KJ and their friends participated in a mock Olympiad organized by the club teachers and presented their experiences in a showcase. KJ demonstrated notably greater ease and engagement when allowed to make choices and have a say in their experiences. This prepared KJ to lead a show and teach a math game they had designed during lunchtime that their peers enjoyed. KJ’s math teacher was impressed and wanted KJ to take over one math class/wk next year.
Mental Health
The remaining half of the sessions over the school year focused on promoting positive coping strategies in school situations using the BIACA program, a cognitive–behavioral therapy (CBT) intervention. Through this program, KJ and their peers learned about coping skills and developed individual KICK plans. Throughout the sessions, the occupational therapy practitioner and the occupational therapy assistant emphasized that Icky Thoughts are not necessarily bad but simply are thoughts that may be causing discomfort or affecting their participation in a desired activity. In Knowing I’m Nervous, KJ indicated that they “felt nervous about eating in the cafeteria because there are a lot of people.” They identified an Icky Thought: “Everyone will have somewhere to sit, and I won’t.” They also identified a Calm Thought: “The cafeteria is busy, but I can walk with a friend, and we can sit together.” By the end of the school year, KJ would often come to the group with a list of situations they had encountered over the past week when they had felt nervous, including their initial thoughts and their thoughts after reflection. KJ also recognized that many of their peers had the same concerns and that some strategies that they used to cope might be helpful to their peers, too, such as choosing a seat that would allow for an easy exit if distressed, setting a goal for how long to participate in a new activity, or choosing to go to a new activity with a group.
Outcomes
By the end of the school year, KJ had achieved all the IEP goals (Table 10). Through repeated practice at school and home, they learned how to cope with social anxiety and use the KICK plan independently by identifying the stressor, writing down nervous (Icky) thoughts, and thinking calming thoughts. They also would reach out to their support network at school, which included two peers, their basketball coach, and their math teacher, when they needed to brainstorm a solution. KJ understood the value of advocating for themself and would do so through writing or using text-to-speech software. By participating in the math club, they mastered three crucial topics in the math Olympiad: sequences, divisibility, and logic. Moreover, they undertook the role of “math club expert” four times during the school year to help a peer, and they enjoyed designing math problems and teaching them to their fellow students.
KJ’s Discharge Results
Strengths and Limitations of the Current Body of Evidence
There are strengths and limitations related to the current body of evidence in the systematic reviews that inform these Practice Guidelines. Systematic reviews address specific clinical questions guided by an a priori protocol for the question development and review process. No systematic review can address all aspects of a topic; authors make many decisions before conducting the review. In addition, no review is perfect, and even the most careful searches sometimes miss articles. The way to reduce these potential sources of bias is to conduct the review using best-practice methodology.
Strengths
The review authors followed best-practice methodology to the best of their ability at every step of the process—for example, by getting input at all stages from practitioners, researchers, consumers, and experts in the areas included in the reviews. The questions for the systematic reviews were developed with an intentional focus on occupation-based outcomes. The goal of occupational therapy is improvement in these outcomes, so the systematic reviews targeted studies that reported occupation-based interventions and outcomes.
Limitations: Gaps in the Evidence
Gaps in knowledge exist when there is insufficient, imprecise, inconsistent, or biased information in the literature about an intervention (Robinson et al., 2011). Gaps also exist when the literature is insufficient to answer a clinical question.
A lack of research supporting particular interventions does not mean practitioners should not use those interventions. In working with clients, practitioners considering specific interventions when there is not enough evidence to support EBP should use expert knowledge and their own training and experience to guide practice. In this section, we pinpoint important gaps in evidence for interventions and approaches practitioners may consider using as appropriate.
Occupational therapy practitioners need to consider the elements of EBP as they evaluate these guidelines in light of gaps in the literature related to their clinical practice. Practitioners should consider the following questions when identifying these gaps (Gutenbrunner & Nugraha, 2020): What evidence exists? What are the best practices associated with providing services to this client population? What interventions are contraindicated for this population? What outcomes am I hoping to achieve with this client? Does evidence exist in another field or discipline related to interventions and desired outcomes that are within the scope of occupational therapy practice? What are my client’s preferences and values? Does my client prefer one intervention over another? Are available resources, cost, or time influencing my client’s preference? How might the intervention I am considering affect my client’s performance patterns and roles? Does my client find the intervention I am considering meaningful? What experience and expertise do I have that can help guide my decisions? What types of interventions have I used previously that were effective with similar clients or populations? What types of interventions have I used previously that were ineffective with similar clients or populations? What potential risks does the intervention I’m considering pose to my client or this client population? Will the health care system or organization be supportive of this intervention? How will I document this intervention? How will I document the outcomes associated with this intervention? Is it likely that this intervention will be reimbursed?
These Practice Guidelines report the literature available at the time of publication of each of the systematic reviews. Although Practice Guidelines authors are required to use the literature available when forming recommendations and case studies, occupational therapy researchers should integrate community- engaged research to prioritize the intervention needs of autistic people and their caregivers. Indeed, many of the reviewed interventions do not support the priorities identified by autistic persons (Benevides et al., 2020; Sterman et al., 2023). There are gaps in the occupational therapy research with autistic people across the lifespan, including the promotion of ADLs and IADLs, a focus on self-efficacy of caregivers of young autistic children, assistive technology, experiences of autistic adults, trauma-informed care, and sexuality and sexual identity among autistic people; all of these need to be researched.
Additional Implications for Occupational Therapy
The following list presents additional information and common occupational therapy interventions for autistic persons that are not addressed in these Practice Guidelines because of a lack of relevant evidence. These list items are based on existing or emerging evidence, expert opinion, or both. These Practice Guidelines were developed using only studies written in English. We encourage researchers to consider research conducted in other countries and presented in languages other than English. Although we understand that accessing and interpreting research studies presented in other languages is a challenge, this is an important area to focus on and build new research. It is important to emphasize that these Practice Guidelines were prepared using existing Level 1 through 3b evidence published between 2013 and 2021. Although this enabled us to use the highest levels of evidence to develop these guidelines, we understand that we might not have been able to incorporate more recent evidence from inclusive interventions that might have a potential to promote well-being in the autistic community. There is a need to include and increase autistic people’s involvement in all aspects of assessment, planning, and intervention, along with the involvement of care partners and caregivers as appropriate. There is a need to include autistic people’s perspectives and partner with them in collaborative endeavors that represent their lived experiences in research and educational initiatives. Systemic barriers to accessing and participating in occupational therapy services persist for historically marginalized population groups. Reporting on race and ethnicity reveals the socially constructed pathways to health disparities, aids in addressing inequalities, and guides targeted interventions for marginalized communities. Reporting on race and ethnicity illuminates the role of societal and systemic factors that cause health disparities. It is a vital step toward health equity, ensuring equal access to quality health care for all racial and ethnic groups through evidence-based strategies. For young autistic children, occupational therapy practitioners must integrate interventions into families’ everyday lives and authentic contexts to ensure the sustainability of routines. For autistic children and youths, occupational therapy practitioners must facilitate social participation with nonautistic peers to foster a broader understanding and acceptability of autistic people. Occupational therapy practitioners must recognize and integrate their training, expertise, and skills into improving mental health outcomes using strengths-based approaches (Murthi et al., 2023) and community-informed interventions. The autistic community has pointed out that strengths-based mental health interventions are urgently needed. These Practice Guidelines do not include a comprehensive overview of the use of assistive technology. Occupational therapy practitioners and researchers may consider how assistive technology can be used and studied in the context of occupational therapy practice. Despite evidence surrounding the use of assistive technology with autistic people, especially children (e.g., social robots and other communication technology; Kouroupa et al., 2022), in these Practice Guidelines we refrained from incorporating studies that used assistive technologies to normalize or remediate the behaviors and social skills of autistic people. Assistive technologies developed for such practices have been criticized for being ableist and reductionist given that they emphasize pathology in autistic people that require services that focus on the normalization of social and communication skills (Williams, 2021). Moreover, assistive technologies, such as organizers, planners, and mobile-based applications to develop executive functions, are gaining traction with promising applications to circumvent executive function challenges through environment-based adaptations (Desideri et al., 2020). We support the recommendations of two self-advocates, Zisk and Dalton (2019), who emphasized that practitioners and researchers should support the use of a variety of communication technologies instead of focusing only on verbal and spoken communication strategies. They also underscored the importance of broadening communication strategies as a whole, using a varied collection of strategies, including low-cost resources, rather than focusing on oral speech and fluency of communication. Moreover, they recommended evaluating the effectiveness of communication devices rather than focusing only on autistic people’s skill levels. Practitioners also need to respect the individual choices and autonomy of autistic people as they choose augmentative and alternative communication methods and devices (e.g., some autistic people prefer to type and then use spoken language to read what they have typed; Zisk & Dalton, 2019). Despite opportunities to collaborate with other professionals, such as applied behavior analysts, cognitive–behavioral therapists, speech-language pathologists, and physical therapists, among others, we advocate for occupational therapy practitioners to engage in critical analysis and reflexive judgment to acknowledge, recognize, listen to, and respect autistic voices that highlight the negative impacts and trauma inflicted by certain interventions (e.g., trauma inflicted by interventions that deny an individual’s personal agency and preferences for their own actions and behaviors). There is evidence supporting the use of CBT throughout these guidelines, which is distinct from applied behavior analysis (ABA; Patten et al., 2023a); however, it is crucial to include the perspectives of autistic people in both the use and evaluation of CBT intervention approaches. Leaf et al. (2022) recommended carefully listening to autistic community members and their lived experiences and perspectives to explore the possible negative impact of behavioral interventions. Moreover, the successful petition by the student section of the American Medical Association House of Delegates (2023) to broaden the inclusion of other evidence-based services apart from ABA can be considered a successful step toward developing authentic and inclusive neurodiversity-affirming care. Mathur et al. (2024) underscored the importance of recognizing autistic people’s strengths, bringing their perspectives to the forefront, and augmenting the implementation of functional assessments by ABA specialists to embrace a future neurodiversity- affirming approach in their services. Occupational therapy practitioners need to recognize and integrate their training and skills, including using models such as coaching, the Cognitive Orientation to daily Occupational Performance (Polatajko & Mandich, 2004), and the Engineering Design Process (Murthi & Patten, 2023) to support autistic people in developing independent cognitive strategies (e.g., problem-solving, self-advocacy skills, productive failing, fail-forward) along with functional skills that enhance occupational performance. Occupational therapy practitioners must understand the importance of using interest-driven and strengths-based activities to teach functional skills, because such activities have the potential to become meaningful occupations.
Conclusion
These Practice Guidelines highlight the current evidence that supports occupational therapy’s unique contribution to autistic people and their caregivers or partners. Clinical recommendations based on the current evidence are provided, and application to practice has been exemplified through case studies and decision-making algorithms. We have highlighted gaps in the evidence for interventions for this population by incorporating feedback from the autistic community. Priorities included the need to shift from deficit-based approaches that may negatively affect health and well-being to adopting neurodiversity-affirming approaches that holistically value autistic people and their strengths with support for their limitations. Occupational therapy practitioners should consider these gaps when supporting autistic persons and their caregivers or partners, and researchers should further investigate these gaps to advance the authentic involvement of autistic people in research that is meaningful to the community and affects their mental health, well-being, inclusion, engagement, access, and participation in occupations.
Practitioners can use these Practice Guidelines to integrate their own professional experience and reasoning, their clients’ individual and family preferences, and the best available research evidence to provide the highest quality of care for autistic people and their caregivers or partners. They can also use these guidelines to challenge their understanding of racial and ethnic inequities and ableism that persist in everyday practice. As the profession and the care of autistic people continue to evolve, occupational therapy can lead in providing neurodiversity-affirming practices based on the profession’s long-standing commitment to holistic health care and a deep understanding of what is meaningful to those we serve. As a profession, we know the tools and insight; we just need commitment. We must ask ourselves: What would happen if we were the members of the care team to promote what is most meaningful to this autistic person? What if we promote this individual’s strengths? We must remain steadfast in our core values as occupational therapy practitioners: We provide distinct values; we are the team members to promote function and participation; and we provide best-practice services grounded in evidence, theory, and occupation. To prepare future practitioners to best advance participatory research methods and create co-constructed research questions that matter the most to autistic people and their caregivers or partners, we must maintain innovative in-service delivery models and increase educational opportunities in which those with lived experiences are centered. It is then that we will succeed.
Footnotes
*Indicates studies included in the systematic review.
Acknowledgments
We acknowledge and thank the following individuals for their participation in the content review and development of this publication:
Practice Guidelines Series Editor
Susan Cahill, PhD, OTR/L, FAOTA, Director of Evidence-Based Practice, American Occupational Therapy Association, North Bethesda, MD
Practice Guidelines Editor and Research Methodologist
Elizabeth G. Hunter, PhD, OTR/L, Assistant Professor, Graduate Center for Gerontology, College of Public Health, University of Kentucky, Lexington
Evigraph Development and Knowledge Translation
Hillary Richardson, MOT, OTR/L, AOTA Practice Manager, Knowledge Translation, Evidence-Based Practice and Practice Improvement
Practice Guidelines Program Support
Shannon White, COTA/L, MA, AOTA Program Manager, Practice Improvement and Advanced Certification
Systematic Review Authors
Alissa Baker, MS, OTR/L; Roxanna Bendixen, PhD, OTR/L, FAOTA; Teal Benevides, PhD, MS, OTR/L, FAOTA; Yu-Lun Chen, PhD, OT/L; Samantha R. Cohen, BA, OTS, OTD Student; Evan Dean, PhD, OTR/L; Roger Ideishi, JD, OTR/L, FAOTA; Kavitha Murthi, MSc(OT), FHEA(UK), OTR, PhD Candidate; Dora Onwumere, MS, OTR/L, PhD Candidate; Kristie Patten, PhD, OTR/L, FAOTA; Beth Pfeiffer, PhD, OTR/L, BCP, FAOTA; Scott Michael Robertson, PhD; Stephen Shore, EdD; Robert Smythe, MFA; Scott Tomchek, PhD, OTR/L, FAOTA; Anna Wallisch, PhD, OTR/L; Renee Watling, PhD, OTR/L, FAOTA
Practice Guidelines Reviewers
Jessie L. Bricker, OTD, OTR/L; Bryden Carlson- Giving, OTD, OTR/L; Julie Diaz, DHA, MEd, COTA/L; Kevin Durney, MS, OTR/L; Mequeil L. Howard, OTR/L, OTD; Roger Ideishi, JD, OT/L, FAOTA; Tracy Jirikowic, PhD, OTR/L, FAOTA; Lauren E. Milton, OTD, OTR/L; Scott Michael Robertson, PhD; Brittany St. John, PhD, MPH, OTR/L; Anna Wallisch, PhD, OTR/L; Renee Watling, PhD, OTR/L, FAOTA; Chuck Willmarth, CAE, Vice President, State Affairs and Health Policy at AOTA
Appendix: Overview of the Systematic Review Methods and Findings
The systematic reviews completed for these Practice Guidelines were conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and are reported in a manner consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).