
Abstract
These Practice Guidelines will assist occupational therapy practitioners, educators, and researchers in applying evidence and expert opinion to practice across the cancer continuum of care, including identifying gaps in care.
Cancer is a group of diseases characterized by uncontrolled growth that can start in almost any organ or tissue of the body (American Cancer Society [ACS], 2023; World Health Organization, 2023). Although there are more than 100 types of cancer, the most common ones include breast, prostate, colorectal, and lung cancer (ACS, 2023). Cancer affects 1 in 3 people, and in 2022 the United States had nearly 18 million cancer survivors, with that number projected to grow to 22.5 million by 2032 (ACS, 2023; National Cancer Institute, 2022). A person is considered a cancer survivor from the time the diagnosis is made throughout their life (National Coalition for Cancer Survivorship, 2014). Although the incidence of a cancer diagnosis increases with age, and approximately 45% of people diagnosed in the United States are between the ages of 20 and 64, there has been a rise in early-onset cancers diagnosed in people younger than age 50 yr (Howlader et al., 2021; Koh et al., 2023). With this increase in the number of survivors, it is no surprise that cancer-related impairments, occupational performance, and participation restrictions may lead to the need for occupational therapy services.
Occupational therapy practitioners can intervene at many points across the cancer care continuum, including at the time of diagnosis, throughout survivorship, and in end-of-life care. Services may be delivered in settings including, but not limited to prehabilitation, acute and medically complex settings, rehabilitation, long-term care, outpatient, home, community, palliative care, and hospice care (Braveman & Newman, 2020). Occupational therapy practitioners are essential members of the interdisciplinary cancer rehabilitation team. According to Silver et al. (2015), Cancer rehabilitation is medical care that should be integrated throughout the oncology care continuum and delivered by trained rehabilitation professionals who have it within their scope of practice to diagnose and treat patients’ physical, psychological, and cognitive impairments to maintain or restore function, reduce symptom burden, maximize independence, and improve quality of life in this medically complex population. (p. 3636)
Because of the late and lasting side effects of cancer and cancer treatment that affect occupational performance, survivorship is now considered a chronic condition (Baxter et al., 2017). Therefore, there is a growing need for occupational therapy practitioners to meet the needs of these clients by using both compensatory and remedial approaches to treat conditions such as cancer-related fatigue (CRF); cancer-related cognitive impairment (CRCI); chemotherapy-induced peripheral neuropathy (CIPN); and psychosocial issues, including depression and anxiety. Occupational therapy practitioners can use health management interventions to teach and support those living with and beyond cancer to manage their own care. Health management includes self-care activities that support the development, management, and maintenance of health and wellness routines (American Occupational Therapy Association [AOTA], 2020). For people living with and beyond cancer, these self-care activities include symptom management, medication management, and social–emotional health.
The side effects of cancer and its treatments can significantly affect one’s occupational performance, participation in everyday life, and quality of life. Some commonly overlooked occupations are sleep and rest, sexual activity, caring for others, driving, community mobility, work, and social participation. As part of an interdisciplinary cancer care team, occupational therapy practitioners are well positioned to address all areas of occupation to improve performance and participation for people living with and beyond cancer.
Systematic Review Question
These Practice Guidelines are based on the following question: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve performance and participation for adults living with and beyond cancer?
Goals of These Practice Guidelines
Through these Practice Guidelines, AOTA aims to help occupational therapy practitioners, as well as the people who manage, reimburse, or set policy regarding occupational therapy services, understand occupational therapy’s contribution in providing services to people living with and beyond cancer and their care partners. These guidelines can also serve as a reference for health care professionals, health care facility managers, education professionals, education and health care regulators, third-party payers, managed care organizations, and those who conduct research to advance care of people living with and beyond cancer.
These Practice Guidelines were commissioned, edited, and endorsed by AOTA without external funding being sought or obtained. They were financially supported entirely by AOTA and were developed without any involvement of industry. All authors of these Practice Guidelines completed conflict-of-interest disclosure forms, with no conflicts noted. AOTA reviews Practice Guidelines, and updates them as needed, every 5 yr to keep recommendations on each topic current according to criteria established by ECRI (2020). Guideline topics are evaluated by a multidisciplinary advisory group consisting of AOTA members, nonmember content experts, and external stakeholders. These Practice Guidelines were reviewed and revised on the basis of feedback from a group of content experts on people living with and beyond cancer that included practitioners, researchers, educators, and policy experts. Reviewers who agreed to be identified are listed in the Acknowledgments.
These Practice Guidelines were developed using the umbrella review method, an overview of existing systematic reviews. With the proliferation of systematic reviews, it is now methodologically important to move a step back and begin to synthesize systematic reviews (Aromataris et al., 2014). This allows for an overall examination of a body of information on a given topic. In addition, we followed the guidance provided by Rosenfeld et al. (2013) in the process we used to develop these Practice Guidelines. A medical research librarian conducted searches of the literature, and review teams evaluated the search results and synthesized the findings (see the Appendix for an overview of the review methods and findings). Interventions that were described in sources other than the published literature and that did not meet the inclusion criteria were excluded from the review.
The current Practice Guidelines update the previous Practice Guidelines, Occupational Therapy Practice Guidelines for Cancer Rehabilitation With Adults (Braveman & Hunter, 2017). Those guidelines, which were based on a systematic review of interventions within the scope of occupational therapy for adults with cancer (Hunter et al., 2017a, 2017b), discussed nine categories of interventions or outcomes: (1) multidisciplinary rehabilitation, (2) symptom management, (3) psychosocial needs, (4) physical activity, (5) lymphedema, (6) complementary health approaches and integrative health, (7) physical agent modalities (PAMs), (8) sexuality, and (9) return to work. Many of the recommendations in these new Practice Guidelines add to and support the previous recommendations. Both Practice Guidelines documents highlight the importance of physical activity to manage many symptoms, such as fatigue, and the use of psychosocial interventions to address symptoms of emotional distress. The current Practice Guidelines have expanded the breadth of recommendations with topics such as a specific focus on sleep, the use of technology and telehealth, and addressing posttraumatic growth and spiritual well-being. Braveman and Hunter’s (2017) Practice Guidelines provided recommendations that did not emerge in the updated Practice Guidelines, in large part because of methodology. Important previous recommendations that are helpful to include here include three areas that did not emerge in the current Practice Guidelines. 1. Interventions for the management of lymphedema: ○ Strong evidence supports using compression bandages, worn daily, to control lymphedema volume. However, manual lymph drainage did not improve results when performed in addition to the wearing of a compression sleeve. ○ Strong evidence supports exercise to improve range of motion, quality of life, mood, and weight loss without increasing lymphedema symptoms. ○ Moderate evidence supports using low-frequency, low-intensity electrotherapy to treat lymphedema in the arms, to reduce pain, heaviness, and tightness. 2. Recommendations related to the use of PAMs: ○ Strong evidence supports adding neuromuscular electrical stimulation to traditional swallowing training for clients with dysphagia after treatment of head and neck cancers. ○ Moderate evidence supports using low-frequency, low-intensity electrotherapy to reduce pain, heaviness, and tightness when treating lymphedema in the upper extremities.
3. Recommendations related to sexuality and work: ○ Strong evidence supports physical training (strength, interval, and home-based activities) in place of usual care to promote interest in sex and sexual activity among male prostate cancer survivors. ○ For clients who wish to maintain or restore (recover) work-related abilities after treatment, moderate evidence supports using high-intensity physical training, such as strength, interval, and home-based activities. ○ Moderate evidence supports the use of multidisciplinary interventions (in particular those with physical, psychological, and vocational components) to improve work outcomes for cancer survivors.
These previous recommendations are still valuable to current practitioners; the current guidelines present updated and expanded recommendations and evidence.
Occupational therapy practitioners should not consider these Practice Guidelines to be a source of comprehensive information about cancer or about application of the occupational therapy process. The occupational therapist makes the ultimate clinical judgment regarding the appropriateness of a given intervention in light of a specific client’s or group’s circumstances, needs, and response to intervention, as well as the evidence available to support the intervention. Examples of how evidence can inform practice with people living with and beyond cancer are included in the “Case Illustrations and Evigraph” section.
AOTA supported this review of the effectiveness of interventions within the scope of occupational therapy for adults living with and beyond cancer as part of its Evidence-Based Practice (EBP) program. AOTA’s EBP program is based on the principle that the EBP of occupational therapy relies on the integration of information from three sources: (1) clinical experience and reasoning, (2) preferences of clients and their families, and (3) findings from the best available research. The Systematic Review Briefs (Amanat, Morikawa, & Newman, 2023; Amanat, Newman, & Morikawa, 2023; Campbell et al., 2023; Fleischer et al., 2023; Morikawa, Amanat, & Newman, 2023; Morikawa, Newman, & Amanat, 2023; Newman, Amanat, & Morikawa, 2023; Polo, Fleischer, & Campbell, 2023; Polo, Hunter, & Morikawa, 2023) and these Practice Guidelines report the findings from the best available research.
Clinical Recommendations for Occupational Therapy Interventions for Adults Living With and Beyond Cancer
Clinical recommendations are the final phase of the synthesis of systematic review findings. The findings for each systematic review question are graded in terms of how confident a practitioner can feel that using the interventions presented in the evidence will improve the outcomes of interest to their clients. The grade is based on the specificity of the intervention, number of studies supporting the intervention, levels of evidence of the studies, quality of the studies, and significance of the study findings. Interventions included in the clinical recommendations are specific to a population, and the articles that describe them provide sufficient detail for practitioners to understand the intervention and the outcomes of interest.
Describing the strength of clinical recommendations is an important part of communicating an intervention’s efficacy to practitioners and other users. The recommendations for these Practice Guidelines were evaluated and finalized by AOTA staff, the AOTA research methodologist, and systematic review and practice guideline authors. AOTA uses the grading methodology provided by the U.S. Preventive Services Task Force (2018) for clinical recommendations. The clinical recommendations pertaining to each review, along with the studies’ level of evidence and supporting details, are presented in Table 1.
Clinical Recommendations for Interventions Within the Scope of Occupational Therapy Practice to Improve Performance and Participation for Adults Living With and Beyond Cancer
Note. ACT = acceptance and commitment therapy; CBSM = cognitive–behavioral stress management; CBT = cognitive–behavioral therapy; CBT-I = cognitive–behavioral therapy for insomnia; CG = control group; chemo = chemotherapy; CI = confidence interval; CRCI = cancer-related cognitive impairment; GI = guided imagery; HBW = home-based walking; HR = heart rate; IG = intervention group; MBCR = mindfulness-based cognitive rehabilitation; MBCT = mindfulness-based cognitive therapy; MBI = mindfulness-based intervention; MBSR = mindfulness-based stress reduction; NR = not reported; PA = physical activity; PET = psychoeducational treatment; PMR = progressive muscle relaxation; PTG = posttraumatic growth; QOL = quality of life; RCT = randomized controlled trial.
Articles had to have a sample of at least 70% patients with advanced cancer (Stage 3 or 4).
Systematic review and meta-analysis.
Sixteen of 45 RCTs addressed cognitive interventions.
16 out of the 20 systematic review articles evaluated computerized-cognitive stimulation, 10 were RCTs, and 6 were feasibility or pilot studies.
Sixteen out of 45 RCTs evaluated the effect of physical activity on cognition.
Four out of 20 studies (mixed designs) evaluated the effect of physical activity on cognition.
Thirty-two articles reporting on 31 interventions; RCTs (n = 16), quasi-experimental (n = 3), and pretest–posttest (n = 12).
Forty studies had a randomized or quasi-randomized design with control groups.
Twenty-five studies were included in the systematic review; study designs were mixed.
For the purposes of these Practice Guidelines, we report recommendations graded A, B, and D, the grades that best support clinical decision-making: A: There is strong evidence supporting the intervention for eligible clients. Strong evidence was found that the intervention improves important outcomes and that benefits substantially outweigh harms. B: There is moderate evidence supporting the intervention for eligible clients. There is high certainty that the net benefit is moderate, or there is moderate certainty that the net benefit is moderate to substantial. D: It is recommended that occupational therapy practitioners not provide the intervention to eligible clients.
These grades are reported in Table 1 and designated with green, indicating should consider if appropriate (A), or yellow, indicating could consider if appropriate (B). None of the studies included in this review reported adverse events or harms related to the interventions evaluated (D).
The complete findings from the review can be found in the Systematic Review Briefs on this topic published in the American Journal of Occupational Therapy (Amanat, Morikawa, & Newman, 2023; Amanat, Newman, & Morikawa, 2023; Campbell et al., 2023; Fleischer, Campbell, & Polo, 2023; Morikawa, Amanat, & Newman, 2023; Morikawa, Newman, & Amanat, 2023; Newman et al., 2023; Polo, Fleischer, & Campbell, 2023; Polo, Hunter, & Morikawa, 2023). As always, practitioners’ clinical decisions should be informed by the evidence presented in these Practice Guidelines, in combination with their clinical experience and the client’s particular goals.
Expert Opinion Clinical Recommendations for Occupational Therapy Interventions for Adults Living With and Beyond Cancer
Expert opinion clinical recommendations are developed for important/common clinical interventions that did not reach the level of an evidence-based clinical recommendation because of a lack of research. The Practice Guidelines team analyzed the evidence and generated intervention topics that could be presented as an expert clinical recommendation. The team drafted the recommendations and provided information supporting the use of the interventions. This was then presented to an expert consensus panel (three people) of subject matter experts from both academic and clinical settings to review the usefulness of the recommendations, appropriate wording, quality of the support provided, and their overall level of agreement that the recommendations should be included in the Practice Guidelines. Feedback from the expert panel was used to revise the recommendations, and the revisions were sent back to the experts until a consensus was reached. Expert opinion recommendations are always considered to be at higher risk of bias because there is a lack of research evidence to support them; they will always have a low strength of evidence. In the absence of high-quality published research, expert opinion is the best knowledge available to guide practice.
Recommendation: Expert Recommendations for the Use of Compensatory Strategies for CRCI
Occupational therapy practitioners may consider using compensatory strategies to address clients’ perceived changes in cognitive function after a cancer diagnosis and treatment, with the aim of maximizing function and optimal performance in daily roles and routines. Cognitive rehabilitation interventions for adults with cancer can be implemented in all practice settings (acute care, outpatient/community practice, home and inpatient rehabilitation) across the continuum of care in multiple treatment formats (individual therapy, group therapy, educational sessions).
As many as 75% of adults living with and beyond cancer report some form of CRCI after a cancer diagnosis and cancer treatment (Mackenzie & Marshall, 2022). Self-management and compensatory strategies, which have been useful in helping improve occupational performance limitations for people with cognitive dysfunction resulting from other chronic illnesses, can be used to address CRCI (Newman, Lyons, et al., 2019). The training and application of compensatory strategies can be completed in individual therapy sessions to allow the practitioner and the client an opportunity to problem-solve together to effectively identify appropriate strategies (shared decision-making), and group-based training can potentially motivate participants to practice compensatory strategies while learning from each other (Syed Alwi et al., 2021). Group sessions are useful for providing education in a group format and problem-solving with peer feedback. Adults living with and beyond cancer can master compensatory strategies for various domains of cognitive impairment, including executive function, attention, memory, and the ability to process new information (Syed Alwi et al., 2021).
Examples of cognitive compensatory strategies to address CRCI and optimize occupational performance include the following: pausing and reflecting to allow time for processing thoughts, using a daily checklist for intentions and goals, activity prioritization, activity pacing throughout the day or week to manage energy levels, using a timer to start and stop tasks, and using phone alarms or alerts for activity or appointment reminders (Radomski et al., 2021).
Occupational therapy practitioners should use a client-centered collaborative approach to identify how CRCI influences valued and meaningful occupations for each client and incorporate compensatory strategies that include both external supports (e.g., a daily checklist, a calendar, alarms) and internal cognitive processes (e.g., pausing and reflecting, internal cues).
Recommendation: Expert Recommendations for the Use of Energy Conservation Interventions for Adults Living With and Beyond Cancer
Occupational therapy practitioners may consider using energy conservation management (ECM) interventions, with occupational analysis and shared decision-making with the client, to reduce fatigue for adults living with and beyond cancer across various practice settings and the cancer care continuum. To ensure successful implementation, occupational therapy practitioners should consider the individual client’s occupations; contexts, including environmental and personal factors; performance patterns; and performance skills.
Effective ECM interventions need to be delivered by means of methods that support behavior change at the just-right time, when clients are most receptive to change, and in ways that increase confidence in their ability to change (Matuska et al., 2007). In addition, practitioners should use a shared decision-making process that includes assessing the client’s understanding of options and preferences for energy conservation options and integrating these preferences into the care plan process (Cahill & Richardson, 2022).
Energy conservation has been described as the intentional management of a person’s energy to maximize participation in desired activities and tasks (Barsevick et al., 2004). This includes examining daily routines to explore strategies to minimize the effort needed to complete tasks, prioritizing tasks, and implementing rest breaks to maintain levels of activity to engage in one’s daily routine, as well as minimizing physical inactivity (Mitchell et al., 2014). Some common energy conservation strategies include analyzing and modifying activities to reduce energy expenditure, balancing work and rest, delegating activities, examining and modifying standards and daily priorities, using the body efficiently during task performance, organizing workspaces, and using assistive technologies to conserve energy (Matuska et al., 2007).
Several studies have demonstrated the use and benefit of ECM techniques in addressing CRF with adults living with and beyond cancer. One Australia-based study found energy conservation to be one of the most common interventions provided in cancer care by occupational therapy practitioners (Buckland & MacKenzie, 2017). A study by Sadeghi et al. (2016) demonstrated that an intervention of ECM strategies consisting of five weekly small-group discussion sessions with education was effective in reducing CRF after medical intervention compared with patients receiving standard care. Another study, conducted by Van Heest et al. (2017), demonstrated considerable reductions in fatigue, increases in self-efficacy, and improvements in quality of life after participation in an individual fatigue management course in an outpatient setting.
Translating Clinical Recommendations Into Practice
Clinical Reasoning Considerations
Very rarely will practitioners find an evidence-based intervention that perfectly fits their clinical setting and the client’s specific needs. Occupational therapy practitioners need to consider several questions as they evaluate the research and consider whether they can use an intervention, or adapt it in a well-reasoned way, to exactly meet the client’s needs (Highfield et al., 2015):
1. Exactly what intervention do I need to provide? ○ What types of client outcomes am I looking for? ○ Do the studies I have located provide enough detail on the intervention so that I know what to do and how to do it?
2. How well do the conditions in which I will provide the intervention match those in the studies? ○ What are the demographic characteristics (e.g., age, gender, diagnosis, comorbidities) of the participants in the research studies? ○ In which setting (e.g., inpatient, home, community, school) did the studies take place? ○ Do any contextual factors (e.g., resources, policies) that are different from those in the studies influence my ability to provide the intervention?
3. How flexible is the intervention, and how much can I modify or adapt it? ○ If my setting or client population differs from those of the studies, can I modify or adapt the intervention without changing its integrity? ○ If I modify or adapt the intervention, what client characteristics (e.g., comorbidities) do I need to consider? ○ Can I be proactive and plan how to modify or adapt the intervention before I start implementing it? ○ Can I make minimal changes to the intervention, such as reordering the content of the sessions, or does the need for substantial changes indicate I should select another intervention?
To modify or adapt evidence-based interventions in practice, practitioners must plan and proactively think through the changes they need to make to fit the intervention to the client and practice setting. In addition, they must document how and why they altered the researched intervention so others in their setting know how to implement the intervention and why the changes were made. If an intervention must be adapted extensively, it may not be the right fit for the situation. When practitioners adapt an intervention, it is no longer evidence based but rather evidence informed. If extensive adaptations to the intervention are necessary, the intervention is probably not right for the client or setting. If the practitioner finds that the intervention does not suit the client, they should not use that intervention. Clinical interventions should be as similar as possible to the interventions used in the research.
Case Illustrations and Evigraph
The case illustrations in this section show how occupational therapy practitioners can translate evidence from the systematic review to professional practice when collaborating with people living with and beyond cancer. Each case study highlights interventions that are supported by evidence and expert opinion.
The evigraph (Figure 1) is based on clinical recommendations and was developed by the authors and AOTA staff to assist practitioners with clinical decision-making. Practitioners must consider each potential intervention in relation to the client’s individual goals, interests, habits, routines, and environment and choose interventions that strongly align with or are supportive of these factors in the context of the client’s Occupational Profile. It is important to note that the evigraph in these Practice Guidelines presents simplified examples of the decision-making processes occupational therapy practitioners might use to address their specific clients’ goals.
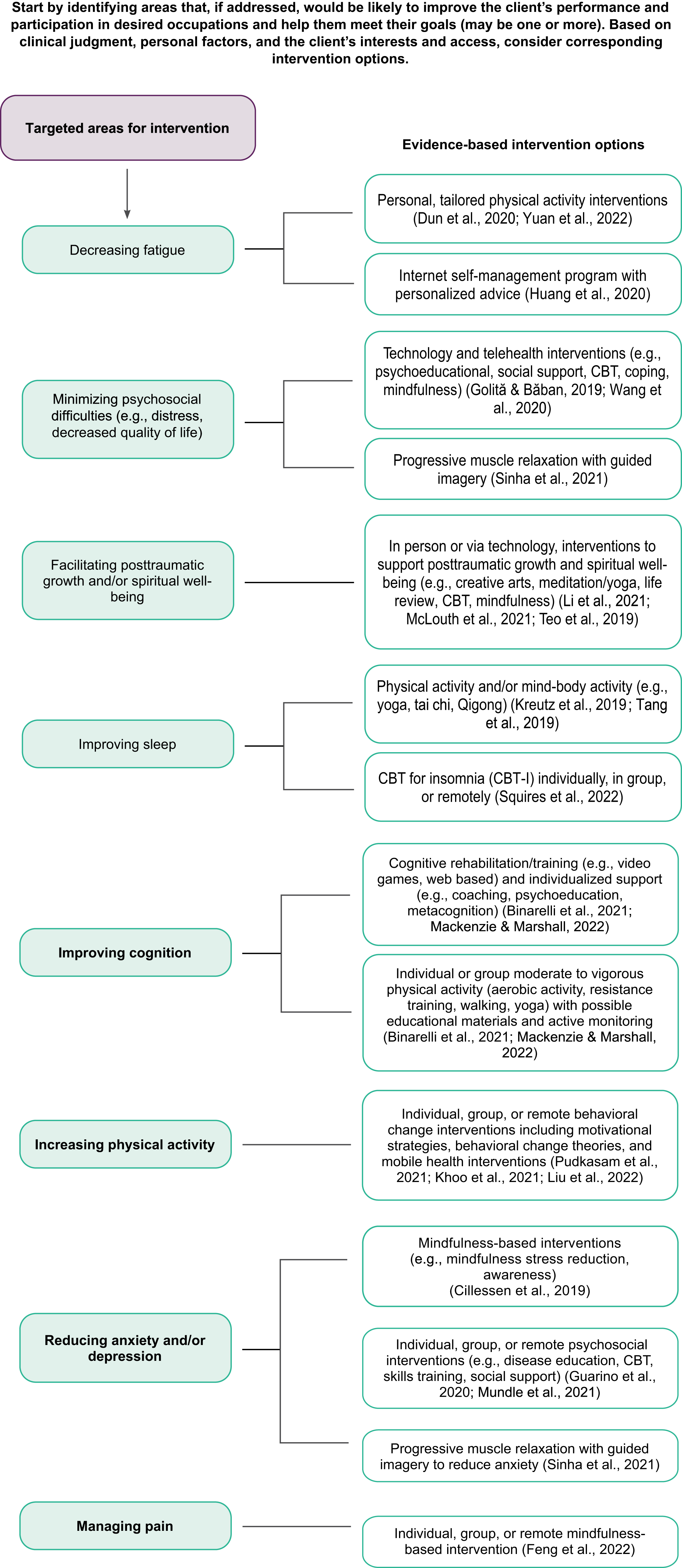
Evidence-based interventions to target fatigue, sleep, cognition, physical activity, pain, anxiety and depression, posttraumatic growth and spiritual well-being, and psychosocial difficulties.
Case Study 1: Mark
Occupational Profile
Mark is a 45-yr-old man who has been diagnosed with Stage 3 colorectal cancer. He had a partial colectomy surgical procedure and is undergoing chemotherapy that comprises a combined regimen including neurotoxic agents, such as oxaliplatin. Mark was on medical leave from his job as a tool and die maker for 2 wk after his surgery, but he has been trying to work full time during his chemotherapy treatments, requiring 1 day off for each treatment cycle. He was referred to occupational therapy services during this active phase of cancer treatment. Mark is married and has two children, ages 10 yr and 14 yr. Mark lives in a rural town; his residence is a 2-story home with a long driveway to the street.
Mark reports fatigue with his daily routine, weakness in his arms and legs, and changes in his cognitive function since starting chemotherapy. Mark works in a fast-paced environment. His job requires that he read and interpret engineering drawings to determine the requirements for the parts needed to create an automobile and then program a computer to create the parts according to the specifications. Mark has noticed he has more difficulty maintaining the focused attention to details and accuracy that are required for his job. He has also noticed fatigue throughout his work day and difficulty standing for the majority of his shift. Mark reports that his job tasks of standing for long periods of time on concrete, walking and transporting items, and having sufficient continuous energy for bending and lifting during tool production are becoming more difficult because of fatigue. He also reports that his fatigue level is affecting his ability to mow and care for his lawn, which his neighbor is now doing for him. Mark describes difficulty falling and staying asleep at night, which leaves him feeling exhausted even at the beginning of his day. In addition, he finds that he does not have the energy or desire to socialize with friends and family.
As a result of his cancer-related fatigue and changes in his cognition, Mark is referred for outpatient occupational therapy services halfway through his chemotherapy regimen. Mark’s strengths include strong family support from his wife and children and a prior history of exercising regularly, consisting of walking 2 miles/day approximately 3–4 days/wk. He used to regularly bowl with friends once a week. Mark is motivated to participate in occupational therapy to improve his endurance and activity tolerance and learn strategies to manage his cognitive changes so he can better manage his job responsibilities.
Occupational Therapy Initial Evaluation and Findings
On the basis of Mark’s primary concerns about his work performance, which is being limited by fatigue and cognitive impairments, and a desire to resume previous social activities, the occupational therapist administered the Brief Fatigue Inventory (BFI; Mendoza et al., 1999), the Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983), and the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005). The Canadian Occupational Performance Measure (COPM; Law et al., 2019) was used to develop an Occupational Profile (AOTA, 2021), guide collaborative goal development and intervention planning, and assess changes in perceived activity participation and occupational performance. Mark’s scores on these measures (Table 2) supported his reports of disrupted work performance, fatigue, impaired cognition, and changes in his social participation activities.
Mark’s Initial Assessment Results
Note. BFI = Brief Fatigue Inventory; COPM = Canadian Occupational Performance Measure; HADS = Hospital Anxiety and Depression Scale; MoCA = Montreal Cognitive Assessment; PSQI = Pittsburgh Sleep Quality Index.
On the basis of the initial assessment results, the occupational therapist and Mark developed the following goals for treatment: Mark will increase participation in walking forms of physical activity health management to 3 days/wk, for a minimum of 30 min, to improve his functional endurance with his work routines. Mark will participate in cognitive training activities 3 days/wk, for a minimum of 15 min, to improve his ability to concentrate, focus, and summarize key details when skimming (previewing) new engineering drawings. Mark will practice using cognitive compensatory strategies for 20-min intervals 5 days/wk to support his memory and attention to details in his work environment. Mark will use strategies to initiate and participate in one social activity each week with either friends or family.
Occupational Therapy Interventions
Mark was seen for a combination of on-site therapy sessions and telehealth sessions at an outpatient occupational therapy clinic. He attended a total of eight occupational therapy follow-up sessions, 1×/wk. After the in-person initial evaluation, Mark attended his first follow-up session on site, and then his therapy sessions alternated between telehealth and on-site visits, for a total of four on-site sessions and four telehealth sessions.
Multicomponent Interventions for Fatigue and Sleep Disturbance
During the on-site sessions, the occupational therapy practitioner used tailored and supervised moderate-intensity walking interventions to target cancer-related fatigue (Dun et al., 2020) and sleep disturbances (Kreutz et al., 2019 ; Tang et al., 2019). They recommended that Mark carry over this moderate physical activity at home for 30 min, 3×/wk for 8 wk. In addition, Mark and the occupational therapy practitioner identified energy conservation techniques to manage fatigue, including examining his work and daily routines to identify strategies to minimize the effort needed to complete tasks and the use of rest breaks to maintain levels of activity, especially at work. The occupational therapy practitioner also reviewed with Mark ways to use his body more efficiently during work performance as well as ideas on organizing his workspace to conserve energy. During his telehealth sessions, the occupational therapy practitioner worked with Mark on self-management interventions to improve adherence to his moderate-intensity walking routine, including using motivational interviewing and his activity tracker’s step counter (Pudkasam et al., 2021). Mark worked toward adherence to and accountability for walking with a friend 3×/wk for fulfillment of a moderate-intensity exercise program for fatigue.
Individually Tailored Cognitive Rehabilitation Interventions
The occupational therapy practitioner used the following tailored cognitive rehabilitation interventions to address Mark’s cognitive changes to maintain his function with work and daily life skills: cognitive training (Mackenzie & Marshall, 2022), compensatory strategies, coaching, and metacognition strategies (Binarelli et al., 2021). The cognitive training interventions consisted of reading and summarizing instructions for assembling car parts, listening to a story (audiobook) followed by answering comprehension questions, and completing web-based cognitive activities (e.g., word searches, word categorization, word generation). The occupational therapy practitioner recommended that these be completed for 20 min/day for at least 3 days/wk as a part of Mark’s home program (Mackenzie & Marshall, 2022). During his telehealth visits, Mark identified a need to learn compensatory strategies to enable him to work more effectively and complete his desired daily activities with less forgetfulness. The occupational therapy practitioner provided education on how to identify the level of energy and focus (duration of time, environment) needed for his work and household management tasks, improve his ability to focus on one task at a time by minimizing distractions and setting a timer, and remember to complete critical tasks by writing a daily agenda in the notes section of his phone (with priority level and estimated amount of time required for each task). In addition, Mark learned how to identify three achievable daily goals (goal-setting) and develop a plan to achieve these goals, including the use of scheduling strategies to keep him more accountable (Syed Alwi et al., 2021, Binarelli et al., 2021).
Multicomponent Intervention for Social Participation
Mark wanted to go out in the community for social events with his friends but was concerned about developing an infection and uncertain about eating at restaurants. He felt too tired to entertain in his home or resume participation in bowling with friends. Because he was working full time and had limited sick days, telehealth sessions were scheduled during his lunch hour 1×/wk. These tailored sessions focused on developing weekly goals to increase his social participation. During these sessions, Mark identified current supports and barriers to participating in desired social activities. Mark and his occupational therapy practitioner identified various behavior change strategies that he could use during the following week to meet his weekly social participation goal (Wang et al., 2020). In addition, the occupational therapy practitioner taught Mark how to incorporate cognitive–behavioral mindfulness techniques into his daily routine to support the behavior change strategies he was using to increase physical activity and social participation with friends and family (Goliţă & Băban, 2019).
Outcomes
Mark improved on all outcome measures and met each of his occupational therapy treatment goals. He reports an improved ability to maintain focused attention for longer periods of time at work and having more energy throughout his shift. Mark has been consistently walking a minimum of 3 days/wk for 30 min after his work shift and uses his phone to track his walking and weekly participation in cognitive activities (e.g., web-based word categorization and word generation, listening to an audiobook). Mark said he feels more prepared for his work day and can identify when he needs a rest break. Mark initially struggled to achieve his weekly social participation goals. However, after Week 2, he identified strategies to meet his subsequent weekly social participation goals. He reported improvements in participation and occupational performance in work and social activities, which enhanced his overall quality of life. Mark is an alternate for his bowling team and plans to rejoin as a roster player in the next season. Mark achieved clinically meaningful scores on the COPM, MoCA, and BFI (Table 3).
Mark’s Discharge Results
Note. BFI = Brief Fatigue Inventory; COPM = Canadian Occupational Performance Measure; HADS = Hospital Anxiety and Depression Scale; MoCA = Montreal Cognitive Assessment; PSQI = Pittsburgh Sleep Quality Index.
Case Study 2: Patricia
Occupational Profile
Patricia is a 62-yr-old woman who was diagnosed with and underwent treatment for Stage 3B right breast invasive lobular carcinoma 2 years ago. Her treatment course consisted of eight cycles of chemotherapy, right mastectomy with tissue expander placement, right axillary dissection with positive lymph nodes detected, and radiation therapy after surgical intervention. The occupational therapy practitioner completed an Occupational Profile (AOTA, 2021). Patricia lives alone in a second-floor apartment located in an urban setting with no elevator access. She fatigues easily when accessing her apartment, frequently taking breaks on the stair landing, especially when carrying groceries. Patricia is independent to modified independent (i.e., she requires extra time to complete tasks) in all activities of daily living (ADLs); however, she says she experiences significant difficulty with completing instrumental activities of daily living (IADLs). She reports lapses in memory, forgetfulness, and difficulty multitasking when engaging in cooking, managing her medication, and paying bills. She often forgets that items are on the stove, and she calls her daughter regularly with questions about managing her finances or refilling her medication. Patricia also expresses difficulty coping with this last change because she previously worked as an accountant before retirement and has always prided herself on being savvy with money. Since retiring because of the cancer treatment, Patricia has explored new occupations, such as photography; however, she is finding that she cannot participate in this activity to the extent she would like to because of fatigue she experiences when standing for long periods of time in addition to pain when holding up the camera for long periods. Patricia expresses feelings of distress and anxiety because of these changes, stating that she does not feel like herself and is worried that she will not be able to return to her baseline level of functioning. She reports poor sleep because of these feelings keeping her awake at night. Patricia also identifies her cancer diagnosis and treatment as trauma she has experienced, expressing difficulty coping with how to progress given her fear of not returning to a functional baseline and of the recurrence of cancer. Patricia is not able to identify any strategies to cope with this trauma or find meaning from it. Her strengths include a strong support system, including neighbors who visit her frequently, and access to transportation.
Occupational Therapy Initial Evaluation and Findings
Because Patricia’s primary concerns include cognitive difficulties that are affecting her independence with IADLs, decreased engagement in occupations due to fatigue and pain, poor sleep, and overall feelings of distress and anxiety, the occupational therapy practitioner administered the Functional Assessment of Cancer Therapy–Cognitive Function (FACT–Cog; Van Dyk et al., 2020; Wagner et al., 2009), Pittsburgh Sleep Quality Index (Beck et al., 2004), a visual analog pain scale (Scott & Huskisson, 1979), and the Distress Thermometer (National Comprehensive Cancer Network, 2023). In addition, occupational therapy practitioner arranged for initial circumferential measurements of her bilateral upper extremities to be taken for prospective surveillance of lymphedema. The COPM was used to further explore Patricia’s self-performance and satisfaction with performance in everyday activities, support collaborative goal-setting and intervention planning, and observe change in self-perceived behaviors in participation over time. Patricia’s scores on these measures, which are listed in Table 4, indicated notable disengagement and decreased independence with IADLs and desired occupations as listed in Table 5.
Patricia’s Initial Assessment Results
Note. COPM = Canadian Occupational Performance Measure; CRCI = cancer-related cognitive impairment; FACT–Cog = Functional Assessment of Cancer Therapy–Cognitive Function; PCI = Perceived Cognitive Impairment; PSQI = Pittsburgh Sleep Quality Index; VAS = visual analog scale.
Patricia’s Initial Circumference Measurements (Centimeters)
Note. LUE = left upper extremity; MCP = metacarpophalangeal; RUE = right upper extremity.
On the basis of Patricia’s assessment results, the occupational therapist and Patricia developed the following goals for treatment: Patricia will improve sleep participation by incorporating at least 2 physical activity and sleep hygiene principles into her daily routine. Patricia will increase leisure participation 1×/wk with a self-reported pain level ∼2 on a scale ranging from 0 to 10 by incorporating mindfulness-based strategies. Patricia will improve IADL management by incorporating at least 2 physical activity and adaptive cognitive compensatory strategies into her daily routine. Patricia will improve her health management by incorporating at least two adaptive cognitive compensatory strategies weekly into her routine.
Occupational Therapy Interventions
Patricia attended 12 occupational therapy sessions on a weekly basis at an outpatient occupational therapy clinic.
Physical Activity and Mind–Body Exercise Interventions for Sleep and Cognitive Performance
To further improve Patricia’s sleep quality and perceived cognitive performance in everyday functioning, the occupational therapy practitioner used physical activity and mind–body exercise interventions to address these areas of concern (Kreutz et al., 2019; Mackenzie & Marshall, 2022, Tang et al., 2019). The occupational therapy practitioner worked with Patricia to establish a home physical activity program tailored to her individualized needs. Because Patricia had initially experienced fatigue, the occupational therapy practitioner worked in collaboration with her to progress her participation in aerobic exercise, gradually increasing the number of minutes and number of times per week based on her activity tolerance demonstrated during sessions, monitoring of symptoms, and response to activity. Patricia’s activity and response to moderate exercise were actively monitored during the first six occupational therapy treatment sessions. As her tolerance to activity increased, a home program was created to continue her participation in physical activity. Her home program included printed educational materials to help decrease her forgetting and maximize her adherence. Patricia also explored yoga to integrate mind–body exercise into her physical activity. As she progressed weekly, her home program increased to include aerobic exercise that included moderate-intensity walking for 30 min 3×/wk and yoga 30 min, 3×/wk. To support her goal of completing her home program, Patricia asked her neighbor to walk with her. Patricia’s participation in physical activity and yoga resulted in higher sleep quality, including decreased sleep disturbances and perceived cognitive improvement, including better attention and verbal memory.
Mindfulness-Based Interventions for Anxiety/Depression, Pain, and Posttraumatic Growth
The occupational therapy practitioner used mindfulness-based interventions to address the symptoms that were affecting Patricia’s participation in photography, her desire for spiritual enhancement, and her overall well-being (Cillessen et al., 2019; Feng et al., 2022; Li et al., 2020). The occupational therapy practitioner provided training on mindfulness-based stress reduction, including breathing exercises, body scan meditation practices, and guided imagery. Patricia and the occupational therapy practitioner discussed attainable incorporation of these practices into Patricia’s daily routine and established a goal of completing them twice daily: once in the morning and once in the evening before sleep. Patricia was also introduced to various web-based applications, including Headspace (https://www.headspace.com) and Calm (https://www.calm.com), and encouraged to explore meditation practices. The occupational therapy practitioner provided education on navigating the applications, as well as setting up notifications and reminders on them.
Cognitive Training Interventions and Cognitive Compensatory Strategies to Improve Occupational Performance
To improve Patricia’s cognitive performance and independence with IADLs and health management, the occupational therapy practitioner used cognitive retraining and coaching (Binarelli et al., 2021; Mackenzie & Marshall, 2022). For meal preparation, the occupational therapy practitioner introduced strategies, including the use of a timer, visual cues, and environmental adaptations, to support Patricia in addressing deficits in multitasking, short-term memory, and attention. To help her during meal preparation, Patricia learned to set individual timers for items on the stove; use visual aids, such as written step-by-step directions; and minimize distractions in her environment. With regard to managing medication, the occupational therapy practitioner introduced compensatory techniques, training in use of adaptive equipment, environmental modifications, and activity modifications. Strategies consisted of using a weekly pill organizer and color-coded medication bottles, electronic reminders/alarms to fill the pill organizer and take her medication, setting up text messages to remind her to get refills, and step-by-step instructions for procuring her prescriptions. To assist Patricia in managing her finances, the occupational therapy practitioner used similar strategies that included setting up weekly and monthly reminders; introducing electronic features, such as auto-pay; and using an app to track her weekly budget. Training and education were provided on all strategies, with Patricia demonstrating increased adherence to and integration of strategies in her daily routine each week. In addition, a home-based cognitive stimulation program was introduced with specific focus on attention and memory (Binarelli et al., 2021). Patricia was instructed to participate in this program 3×/wk for 30 min each time. These interventions contributed to improved perceived cognitive performance, specifically with memory, attention, and processing, which resulted in Patricia’s independence in the areas of cooking, medication management, and bill management.
Cognitive–Behavioral Therapy Intervention for Insomnia
The occupational therapy practitioner and Patricia identified that she had difficulty falling asleep, remaining asleep, and an overall poor sleep quality. To address these issues, the occupational therapy practitioner used cognitive–behavioral therapy for insomnia (CBT-I; Squires et al., 2022). The occupational therapy practitioner explored Patricia’s sleep patterns, identifying her current routine, habits, and thoughts and feelings around sleep. They worked together to establish a sleep hygiene routine for use at home that comprised setting sleep limits, identifying relaxation techniques before sleep, modifying her sleep environment, and restructuring her thoughts. With education and increased awareness, Patricia became more aware of the factors inhibiting her sleep and learned strategies to mitigate these barriers. She was able to establish and integrate an individualized routine at home that consisted of principles of CBT-I, including associating her bed with sleep and using it only for sleep; limiting her naps; and incorporating activities of relaxation, such as journaling, meditation, and breathing techniques, into the hour before sleep. After using these strategies, Patricia reported improved sleep participation, including increased ease of falling asleep, longer periods of sleep before waking, and improved sleep quality.
Outcomes
Patricia improved on all outcome measures (Tables 6 and 7) and met all her occupational therapy treatment goals. She reported improvements in participation and occupational performance in IADLs and sleep, which enhanced her overall quality of life and well-being. At the end of 12 wk, Patricia was independent with IADLs and health management, including managing her basic monthly bills, getting her prescriptions filled and remembering to take them daily, and completing meal preparation daily. She engaged in photography weekly while experiencing only minimal pain. She was able to participate in increased physical activity, going on daily walks with her neighbor. Her engagement in mindfulness-based practices several times a week and her daily physical activity resulted in significantly decreased distress and improved sleep. Patricia reported feelings of hope and a sense of newfound meaning in this next phase of her recovery. Measurements were again taken of her bilateral upper extremities, with no change from intake noted. Patricia was also provided with guidance and resources for contacting a certified lymphedema therapist should further intervention or lymphedema needs arise.
Patricia’s Discharge Assessment Results
Note. COPM = Canadian Occupational Performance Measure; CRCI = cancer-related cognitive impairment; FACT–Cog = Functional Assessment of Cancer Therapy–Cognitive Function; PCI = Perceived Cognitive Impairment; PSQI = Pittsburgh Sleep Quality Index; VAS = visual analog scale.
Patricia’s Discharge Circumference Measurements (Centimeters)
Note. LUE = left upper extremity; MCP = metacarpophalangeal; RUE = right upper extremity.
Strengths and Limitations of the Current Body of Evidence
There are strengths and limitations related to the current body of evidence in the review that informed these Practice Guidelines. The systematic review addressed a specific clinical question guided by an a priori protocol for the question development and review process. No systematic review can address all aspects of a topic; authors make many decisions before conducting the review. In addition, no review is perfect, and even the most careful searches sometimes miss articles. The way to reduce these potential sources of bias is to conduct the review using best practice methodology.
Strengths
The review authors followed best practice methodology to the best of their ability at every step of the process. The clinical recommendations in these Practice Guidelines come from recent, existing high-quality systematic reviews. The guidelines team provided expertise from practitioners, researchers, consumers, and experts on the topic. This methodology is a strength because it allowed for extensive time to be taken to conduct the assessment and synthesis of systematic reviews rather than conducting reviews that already exist. In addition, we include in these Practice Guidelines two expert opinion clinical recommendations for important topics that did not emerge in our evidence-based clinical recommendations.
Limitations
Gaps in knowledge exist when there is insufficient, imprecise, inconsistent, or biased information in the literature about an intervention (Robinson et al., 2011). Gaps also exist when the literature is not sufficient to answer a clinical question.
A lack of research supporting particular interventions does not mean practitioners should not use those interventions. In working with clients, practitioners who are considering specific interventions when there is not enough evidence to support EBP should use expert knowledge and their own training and experience to guide their practice. In this section, we pinpoint important gaps in the evidence for interventions and approaches practitioners may consider as appropriate to use.
Occupational therapy practitioners need to think about the elements of EBP as they evaluate these guidelines, taking into consideration gaps in the literature related to their clinical practice. They should consider the following questions when they identify these gaps (Gutenbrunner & Nugraha, 2020):
1. What evidence exists? ○ What are the best practices associated with providing services to this client population? ○ What interventions are contraindicated for this population? ○ What outcomes am I hoping to achieve with this client? ○ Does evidence exist in another field or discipline related to interventions and desired outcomes that are within the scope of occupational therapy practice?
2. What are my client’s preferences and values? ○ Does my client prefer one intervention over another? ○ Are available resources, cost, or time influencing my client’s preference? ○ How might the intervention I am considering affect my client’s performance patterns and roles? ○ Does my client find the intervention I am considering meaningful?
3. What experience and expertise do I have that can help guide my decisions? ○ What types of interventions have I used previously that were effective with similar clients or populations? ○ What types of interventions have I used previously that were ineffective with similar clients or populations? ○ What potential risks does the intervention I am considering pose to my client or this client population?
4. Will the health care system or organization be supportive of this intervention? ○ How will I document this intervention? ○ How will I document the outcomes associated with this intervention? ○ Is it likely that this intervention will be reimbursed?
In the following sections, we present additional information and common occupational therapy interventions for adults living with and beyond cancer that are not addressed in these Practice Guidelines because of a lack of relevant evidence. These sections are based on existing or emerging evidence, expert opinion, or both.
During the systematic review process, we found that included articles did not focus on younger (age 18–39 yr) and older adults (65+), certain social determinants of health (e.g., race, ethnicity, socioeconomic status), type of cancer (other than breast cancer), or stage of cancer (advanced), nor did they report sexual orientation or gender identities. The clinical recommendations included in these Practice Guidelines are based on gender assigned at birth.
Occupation- and Participation-Based Measures
In this review, we uncovered gaps in the literature related to the use of occupational therapy assessments and interventions that support occupational performance and participation. The findings of the review highlight the use of management strategies to alleviate the effects of symptoms such as fatigue, anxiety, depression, and cognitive function. The importance, however, of measuring occupational performance and participation among adults living with and beyond cancer is globally recognized (L’Hotta et al., 2020). Notable gaps in occupational participation outcomes include areas of occupations that are affected by cancer and cancer treatment, including sexuality and intimacy, work, driving, and social and leisure participation. Occupational therapy researchers are encouraged to include performance-based measures as primary outcomes in cancer research. At present, occupation- and performance-based measures, such as the COPM to evaluate satisfaction with and performance of daily activities, and the Occupational Performance Inventory of Sexuality and Intimacy (Walker et al., 2020) for the screening, assessing, and measurement of sexuality and intimacy, are available to cancer care practitioners to use in research and practice. Occupational therapy practitioners in cancer care should consider incorporating the use of occupational performance and participation measures into routine practice to support the highest integration of the use of occupation as ends and means.
Underrepresented Symptoms in the Literature
Much of the evidence included in the systematic reviews focused on symptoms arising from breast cancer diagnosis and treatment. There is a lack of research pertaining to symptom management for cancer diagnoses outside of breast cancer. The physical and psychological symptom management of problem areas, including body image, sexuality, and CIPN, also were identified as gaps.
Individuals with head and neck cancer undergoing medical treatment and those with cancer requiring stoma surgery have been found to have body image difficulties that have implications for functional status, interpersonal relationships, and overall quality of life (Ahmed et al., 2019; Alias & Henry, 2018; Jayarajah & Samarasekera, 2017; Williams, 2021). In addition, those with other cancers and undergoing treatment, including surgery, can experience symptoms that affect body image and ADLs, such as sexual activity, potentially contributing to feelings of increased distress and worry (Pergolotti et al., 2020). Although most of the literature on interventions includes people with breast cancer, evidence supports CBT interventions and those that take a psychoeducational approach. Occupational therapy practitioners could consider using these interventions to address body image difficulties (Fingeret et al., 2014; Lewis-Smith et al., 2018). In addition, there is limited evidence on interventions related to sexuality; however, moderate evidence indicates that physical exercise to address sexuality can be helpful (Hunter et al., 2017b). Further research across various practice settings and the cancer care continuum should include the exploration and testing of interventions to address body image difficulties that are affecting sexuality.
CIPN can contribute to sensorimotor impairment by influencing areas of occupational performance, including ADLs, fall risk, sleep, and work performance (Baxter et al., 2017; Streckmann et al., 2022). The American Society of Clinical Oncology includes exercise as a recommendation to manage neuropathy, as supported by the results of a standardized, individualized, moderate-intensity, 6-wk home-based, progressive walking and resistance exercise program that found that exercise significantly reduced CIPN symptoms of heat/coldness in the hands and feet (Loprinzi et al., 2020). In addition, for clients with CIPN, the recommendation based on the current literature is sensorimotor training, at least 2×/wk (Streckmann et al., 2022). Occupational therapy intervention can support people managing these important physical and psychological symptoms by helping them maximize their psychosocial and functional well-being. Intervention methods may include remediation and adaptation, lifestyle management, and therapeutic exercise; however, further research should include the testing of interventions to support these areas across various practice settings and the cancer care continuum.
Advanced Cancer
There is limited evidence demonstrating the use of occupational therapy interventions that focus on occupational performance and participation in daily life to support adults living with advanced cancer. This is an important gap to mention because adults with advanced cancer have chronic and complex conditions that affect their functional, emotional, and occupational engagement; some of these adults have a potential life expectancy of >6 mo. Evidence shows that the prolonged side effects of cancer treatment and the evolving physical and emotional changes of advanced cancer can create issues with ADLs and IADLs, leading to further disability and role disruption (Neo et al., 2017).
Occupational therapy practitioners should use comprehensive, client-centered, functional assessments and interventions to maximize their clients’ occupational performance across the cancer continuum. Adults with advanced cancer may require guidance on how to maintain independence with meaningful daily occupations and may benefit from strategies to navigate mild cognitive impairment, fatigue, pain, and weakness in their everyday routines. Earlier access to occupational therapy interventions for adults with advanced cancer is imperative if those interventions are to support the person’s ability to participate in meaningful occupations at the highest capacity and facilitate continued engagement and performance through activity modifications and productive goal-setting (Dolgoy et al., 2021). Occupational therapy practitioners can address the care needs of clients with advanced cancer by adopting an approach tailored to each client and their support networks that includes shared decision-making and collaborative problem-solving regarding the illness’s impact on occupational performance, symptom management, and equipment needs (Dolgoy et al., 2021).
To validate the importance of occupation-based interventions, we encourage occupational therapy practitioners to focus on such interventions and document the ones that lead to successful ADL and IADL outcomes. Multidisciplinary collaboration and education are crucial to highlight the impact of occupational therapy interventions for adults with advanced cancer and improve the medical model’s understanding of activity analysis, ADL modifications, and the translation of medical concerns into functional outcomes (Dolgoy et al., 2021). Further studies are needed to establish which interventions are most appropriate to improve occupational performance and participation while addressing common side effects experienced across the cancer continuum.
Additional Implications for Occupational Therapy
To complement the intervention recommendations provided in these Practice Guidelines tables, in the sections that follow we describe general implications for occupational therapy for adults living with and beyond cancer.
Further studies are needed to establish which interventions and service delivery methods (e.g., individual sessions, group sessions) are most appropriate to improve occupational performance and participation while addressing common side effects experienced across the cancer continuum, from prehabilitation through acute care, and settings that include medically complex milieux as well as rehabilitation, long-term care, outpatient, home, community, palliative care, and hospice care (Braveman & Newman, 2020)
▪ Although these systematic reviews highlight the symptom management of common side effects of cancer, the symptoms of cancer and cancer treatment do not occur in isolation: Survivors often present with multiple impairments (e.g., fatigue, cognitive changes, psychosocial dysfunction), and the presentation is frequently multifactorial. Although symptom management is important to the health and wellness of adults living with and beyond cancer, occupational therapy practitioners need to consider using a top-down approach, including the use of occupation-based assessments and interventions to address all aspects of client health management and other critical occupations that are affected by multiple side effects. Practitioners should not rely solely on impairment-based assessments and interventions because these methods do not generalize to changes in occupational performance and participation (Brick et al., 2021; Newman, Alfano, et al., 2019). ▪ Occupational therapy practitioners and researchers who are using patient-reported outcome short forms (e.g., the Patient-Reported Outcomes Measurement Information System [https://www.healthmeasures.net/explore-measurement-systems/promis#], FACT–Cog) should know that such instruments may lack sensitivity to identify impairments in participation and occupational performance (Brick et al., 2021; L’Hotta et al., 2020). Therefore, during intervention and research planning practitioners and researchers in cancer care should also use complementary screenings for the need for occupational therapy services and assessment tools to ensure that clients living with and beyond cancer are receiving holistic, client-centered services (Polo, Romero, et al., 2023). ▪ On the basis of these Practice Guidelines, there is strong evidence to support telehealth service delivery to improve psychosocial outcomes for and the spiritual well-being of adults living with and beyond cancer. In addition, telehealth-based cancer rehabilitation interventions appear to be a promising approach to improving disability for this population (Brick et al., 2022). Occupational therapy practitioners should consider using this service delivery option to improve access and reduce barriers to care for clients living with and beyond cancer.
Conclusion
The incidence and prevalence of people being diagnosed with cancer are significantly increasing across the globe. Occupational therapy practitioners will encounter survivors across the cancer continuum, from diagnosis through survivorship and end of life. Practitioners should use these Practice Guidelines to integrate evidence into their practice with clients living with and beyond cancer. They also should use this impairment-focused information and apply it using a holistic, client-centered lens to address these clients’ occupational performance and participation needs.
Footnotes
*
Indicates articles included in the systematic reviews.
Acknowledgments
We acknowledge and thank the following individuals for their participation in the content review and development of this publication:
Susan Cahill, PhD, OTR/L, FAOTA, Director of Evidence-Based Practice, American Occupational Therapy Association, North Bethesda, MD
Elizabeth G. Hunter, PhD, OTR/L, Associate Professor, College of Health and Human Services, Bowling Green State University, Bowling Green, KY
Hillary Richardson, MOT, OTR/L, Practice Manager, Knowledge Translation, Evidence-Based Practice and Practice Improvement, American Occupational Therapy Association, North Bethesda, MD
Shannon White, COTA/L, MA, Program Manager, Practice Improvement and Advanced Certification, American Occupational Therapy Association, North Bethesda, MD
Tiffany Bystra, MS, OTR, CHSE; Claire M. Dolislager, DrOT, OTR/L, CLT-LANA; Sherry Hite, MOT, OTR/L; Asfia Mohammed, EdD, OTR, MOT; Lynne F. Murphy, EdD, OTR/L; Colton Sayers, OTD, OTR/L, CNS; L. Hunter Stafford, MS, CES; Amanda Wheeler, PhD, OTR/L, CLT
Appendix: Overview of the Umbrella Review Methods and Findings
These Practice Guidelines were developed on the basis of the methodology of an umbrella review, which provides an overview of existing systematic reviews. With the proliferation of systematic reviews, it is now methodologically important to move a step back and begin to synthesize the systematic reviews (Aromataris et al., 2014). This allows for an overall examination of a body of information on a given topic. In addition, we followed the guidance from Rosenfeld et al. (2013) in the process used to develop a clinical practice guideline.