
Abstract
Supporting clients and their families to live ordinary lives lies at the heart of occupational therapy. But an ordinary life—no matter who is living it—is full of risks, and risks often make us a little anxious. What if I, as a practitioner, encourage a client to take a risk and something undesirable does happen? Will I have shirked my duty of care? Not all experiences we label risky lead to undesirable outcomes. Some simply involve challenges: pushing people beyond their comfort zone so they can achieve more than ever before. Self-esteem is born out of meeting challenges; so is respect. In supporting clients and families to meet the challenges of an ordinary life, we balance duty of care with dignity of risk.
In this Eleanor Clarke Slagle Lecture, Dr. Anita Bundy discusses how supporting clients and their families to live ordinary lives lies at the heart of occupational therapy.
I have been fortunate to lecture about play around the globe: assessing it, promoting it, and studying it. Play as occupation. Play as medium. In those talks, I often speak about play as a paradox (i.e., having seemingly contradictory qualities; Merriam-Webster, 2024). Here is what I mean: ▪ Play is the primary occupation of children—and, indeed, it is a lifelong occupation. ▪ Play is the primary means by which children learn and the means by which all people challenge themselves to be the best they can be. ▪ Here is the paradox: Play is a waste of time.
No wonder play causes problems for occupational therapy practitioners. But play is not the only paradox. In preparing for this lecture, I realized just how many paradoxes there are in occupational therapy and occupational science.
In his seminal book The Reflective Practitioner: How Professionals Think in Action, Donald Schön (1983) wrote, “In the varied topography of professional practice, there is a high, hard ground where practitioners can make effective use of research-based theory and technique” (p. 42). It would be so simple if all practice occurred on this high ground.
Schön (1983) went on. There is also “a swampy lowland where situations are confusing ‘messes’ incapable of technical solution” (p. 42). Occupational therapy is about everyday life. Is there anything less muddy than everyday life? Particularly when it involves people experiencing conditions or contexts that challenge their everyday lives?
Let’s go to the swamp—where we will find more paradoxes—and wallow in the mud of difficult decisions. First, let me acknowledge some of my current “swamp-dwelling colleagues,” a team supported by the Norwegian Research Council, led by Ellen Beate Sandseter and comprising Mariana Brussoni, Rasmus Kleppe, Ole Sando, Håvard Lorås, and Lise Storli. Our team is examining the extent to which children who experience risky play are better able than other children to manage risk in real life (Sandseter et al., 2023).
David Ball, Professor of Risk Management and Co-Director of the Centre for Decision Analysis and Risk Management at Middlesex University, is an external member of our team. In 2002, the United Kingdom’s Health and Safety Executive commissioned David to research playground safety. He found that the risk of serious injury on playgrounds was actually very small. He concluded that because of the misguided fears of adults and public agencies, children and young people were being deprived of important physical, social, emotional, and cognitive benefits that can be derived from play. By the way, all that is still true today, more than 20 years later, in the United States as well as elsewhere around the world (Ball, 2002).
Ball’s (2002) study led him and his UK-based colleagues to develop a risk–benefit assessment (Ball et al., 2012; Figure 1) instead of taking the more traditional approach, in which risk preventionists determine the seriousness of particular activities or objects by plotting the severity of potential harm against the likelihood of its occurrence (Figure 2). A risk–benefit viewpoint promotes an as-safe-as-necessary approach to prevent serious, disabling injury, not an as-safe-as- possible approach (Brussoni & Olsen, 2013; Margolis, 1996; Sandseter & Kennair, 2011). But Ball went further. Borrowing from American social scientist Howard Margolis (1996), Ball and Ball-King (2011) wrote that those who seek to control risk should adopt the Hippocratic oath (i.e., “First, do no harm”).


Traditional approach to risk assessment.
Welcome to the swamp.
Although professionals often focus on ensuring safety from even minor injury, Ball and Ball-King (2011) argued that measures adopted to keep people free of all injury often decrease enjoyment. To enjoyment, I add self-esteem and self-efficacy. When we consider freedom from any possible physical injury to be more important than self-efficacy, self-esteem, and enjoyment, we run the risk of inflicting psychological harm.
“Do no harm” is known formally as nonmaleficence. Nonmaleficence and beneficence are flip sides of a coin. Whereas nonmaleficence requires avoiding actions that cause harm, beneficence requires taking action to incur benefit (Beauchamp & Childress, 2019). Nonmaleficence and beneficence are two of six principles in the American Occupational Therapy Association’s (AOTA’s; 2020) Code of Ethics. Not coincidentally, autonomy—the right to make choices on the basis of one’s values and beliefs—is the third principle (Beauchamp & Childress, 2019).
The Preamble to AOTA’s Code of Ethics states that we are “committed to promoting inclusion, participation, safety, and well-being for all recipients of service in various stages of life, health, and illness and to empowering all beneficiaries of service to meet their occupational needs” (p. 1). But ensuring safety, participation, inclusion, and well-being, all at the same time, can be problematic—and can even present ethical dilemmas (Ball & Ball-King, 2011; Margolis, 1996).
AOTA’s Code of Ethics acknowledges those potential dilemmas, saying that to make ethical decisions, we must consider conflicts between competing principles. Principles may need to be carefully balanced and weighed while considering professional values, individual and cultural beliefs, and organizational policies.
Now we really are in the swamp—trying to find a clear path through the mud. Take safety and autonomy, for example, remembering that ensuring safety from physical injury may cause serious psychological harm (Ball & Ball-King, 2011). Paradox, anyone?
In a draft of an unpublished study, University of Sydney PhD candidate Jo Ragen (2022) asked adults and adolescents with a significant disability and parents of children with a significant disability about advice professionals had given them and how that advice affected their everyday lives. Each of those participants indicated that although professional advice did not always support it, a life worth living is one of joy and happiness.
But the difficult decisions that support a happy life are often muddy.
Both Ragen (2022) and Anita Niehues et al. (2015) reported on the same mother of a 5-year-old with osteogenesis imperfecta (brittle-bone disease). That mother recounted a time when her family had been looking forward to a special outing. “As they were getting ready to go, the child broke a bone, something that happened to him all the time. He just looked up at his mother and said, “I broke. Oh, well; just get a plaster, put it on, and let’s GO!” (Niehues et al., 2015, p. 817). Missing out on something he wanted to do was, for this child, far worse than breaking a bone. His parents knew that their son’s need to experience life fully was more important than protecting him from every broken bone or adhering to every expert’s cautious recommendation (Niehues et al., 2015; Ragen, 2022). His parents made a conscious decision that [their son] would not thank them for living a life ruled by the fear of breaking a bone, but he would thank them for a good life. “He’ll be remembering the times he rode the motorcycle with his dad or swam with dolphins” (Niehues et al., 2015, p. 817).
The same parent, participating in Ragen’s (2022) study, concurred,
[It’s] been what guided the way. . . . We can fix a broken arm. What we can’t fix is a life that is dull, and not got anything in it. It’s not a life if you’re just sitting in four walls and not out there living it.
It goes without saying that we want to keep recipients of our services, and our children, and our parents, safe; that is, we all have a duty of care. The American health care system seems relatively silent on duty of care, but the Australian Mental Health Recovery Institute has offered cogent advice. Although this advice specifically refers to adults with mental health challenges, I believe it works for all people. They began with a definition of “duty of care”: “legal responsibility of an organization (or its staff) not to harm the people they support” (Workplace Mental Health Institute, 2015).
Duty of care is often incorrectly assumed to mean that people must be free of all risk. But duty of care is not the same as overprotection. Duty of care also is not about keeping people safe from their own choices or promoting only activities that a caregiver feels are safe.
The problem is that anything can cause harm: There is no action or object that is not hazardous under certain circumstances. We cannot treat all potential hazards with the same degree of seriousness. We must consider the consequences of a particular action to a particular person in a particular situation. Children with or without a disability continually gain skills. Adults of any age, with or without a disability, benefit from support and other ways of mitigating risk, so we must also consider the particular time of concern. Moreover, a degree of risk is often beneficial, if not essential—even if it is in the context of something that is more than a little scary and when other people disapprove.
Consider Australian Jessica Watson who, in 2009, when she was age 16, embarked on a journey to sail nonstop around the world—solo. (Incidentally, Jessica’s mother, Julie, is an occupational therapist.) You can imagine the criticism heaped on her parents, especially when she collided with a 63,000-ton Chinese cargo ship less than 1 day after she sailed out of her home port. In a Sydney Morning Herald column titled “I’m Glad Jessica Watson Isn’t My Daughter,” columnist Cosima Marriner (2009) wrote the following:
Jessica Watson is preparing to sail solo around the world, but where do parents draw the line in allowing their children to pursue their dreams? … I will encourage my daughter to follow her dreams, tell her she can achieve anything she puts her mind to, and counsel her not to listen to ignorant critics. [But] when my daughter reaches 16, I can’t say I or my husband would sanguinely quit our jobs to support a risky solo sail around the world, nor would we blithely wave her off from the dock. … We all want our kids to have the confidence to take risks and establish their own independence. Yet as a parent, where do you draw the line between encouraging children to follow their dreams and saying no for their own good? (para. 1–5)
Marriner went on to accuse the Watsons of being desensitized to the real potential for something disastrous to occur, and she referred to Jessica’s voyage as an obsession of both Jessica and her parents. Nevertheless, Jessica (and her family) persisted, and Jessica succeeded, surviving seven knockdowns and 210 days alone at sea.
At the close of her journey, then–Australian Prime Minister Kevin Rudd declared Jessica an Australian hero. Jessica responded that she was not a hero: She was just an “ordinary person, who had a dream, worked hard, and proved that anything is possible.” Jessica’s sail was unassisted; that is, she was alone in the boat. But—and this is critical—she was not without help. Her family and her support team were in touch constantly by radio, consulting weather reports and providing advice and encouragement. There are countless ordinary people with big dreams who made those dreams happen, through hard work and with a lot of support.
With regard to children, Vygotsky (1978) called that support “scaffolding”: providing assistance while the child masters concepts and skills that are a little beyond their ability. With adults, the concept is similar: providing support to enable another to go a little beyond what they feel comfortable doing. With older adults, the concept often applies to maintaining skills and involves assessing the benefits and discussing and mitigating the risks.
In this lecture, I introduce you to a few more people who had big dreams and took big risks. They were not people with extraordinary ability. In fact, because they were older or had impairments, many probably considered them less capable and at greater risk than cognitively or physically able adults or young people. I am sure these people must have been scared to death, exhausted, and ready to give up countless times. Certainly, all of them encountered repeated failures in their journeys. But they got up, dusted themselves off, and kept going.
Failure is a common and important component of challenge.
Importantly, all these individuals had people who believed in them and supported them, but I’m sure those support people also were scared to death at times.
Meet Chris Nikic, who has a developmental delay and was born with a heart defect. In November 2020, when he was 21, Chris became the first athlete with Down syndrome to complete an Ironman triathlon. Chris’s father, Nik, recognized the benefits of taking on tasks with uncertain outcomes. When he sought a trainer to help Chris prepare, he ensured that the trainer was prepared to let his son fail (ESPN, 2021).
Consider Diana Nyad. At age 64, and on her fifth attempt, she met a goal she had set more than 30 years earlier: to be the first person to swim the 103 miles between Cuba and Florida, alone and without a shark cage. She failed four times before she succeeded. Her life was at stake. The people closest to her said she could not do it. But she persevered. And although she swam alone, she was not without support. A team traveled beside her, ready to step in (Chin & Vasarhelyi, 2023).
I expect you know many such people. They may not sail around the world, complete an Ironman, or swim from Cuba to Florida; for them, the dream may be living independently, or driving, or even climbing a tall tree.
Isn’t catching dreams part of our remit as occupational therapy practitioners? Do things go wrong sometimes? Of course they do. Finding the just-right challenge means we sometimes go a little beyond our abilities. “I thought I could, but I didn’t this time. I will next time.”
One of the adult participants with a significant disability in Jo Ragen’s (2022) study commented on the lowered expectations professionals have of people with a disability, the perception that people with a disability are just not capable, and that trying difficult tasks is too risky. Too risky for whom? And whose life is it, anyway?
In 1972, Robert Perske coined the phrase “dignity of risk.” In 2020, Roy Richard Grinker, author, Psychology Today columnist, and father of a child with a disability, wrote about the dignity to fail as a part of dignity of risk:
There is dignity in risk, in having the opportunity to succeed, to fail, to not fit in, to create one’s own spaces for a meaningful life. In fact, most of the positive stories I’ve heard about someone’s struggles with disability and stigma involve some failures. Nearly every negative story about disability and stigma is about someone who has been sheltered, protected, and denied the opportunity to fail. (Grinker, 2020)
In reference to people with mental illness, the Australian Mental Health Recovery Institute described a continuum, with duty of care on one end and dignity of risk on the other. I prefer to think about maintaining a balance between providing adequate help (duty of care) and promoting dignity of risk and to think about this balance for all people (Figure 3).
Dignity of risk is the right of every person to make choices and decisions, to make mistakes and learn from them. In a nutshell, it is autonomy (Principle 3 of AOTA’s Code of Ethics). If you or the average everyday person has the right to do something, even if it is potentially harmful (e.g., smoking, overeating, climbing a tree), then the people in our care also have that right.
Whereas duty of care foregrounds risks, dignity of risk foregrounds benefits. The Australian Mental Health Recovery Institute suggests that we start with dignity of risk (i.e., the benefits). Only when the threat of death or permanent serious disability occurs, or the person has been deemed by a legal entity to lack the capacity to make decisions, or an involuntary treatment order is in place, do we move to duty of care. In short, the modern interpretation of “First, do no harm” is that we consider whether potential benefits outweigh potential risks (Shmerling, 2020).
Let’s shift the risk discourse. What if, rather than equating risk with danger and harm, we redefine risk as challenge, with a degree of uncertainty and the potential for benefits?
I did not start out to study risk. I wanted to study play. I gathered a multidisciplinary team of researchers (a psychologist, a human geographer, and a pediatric exercise scientist). All of us were interested in play for various reasons. We deliberated until we created work that would add to the professional knowledge of all our disciplines, and we convinced the Australian government to fund us.
We named our first grant “Popping the Bubblewrap” (Bundy et al., 2011). The research ultimately became known as the Sydney Playground Project. We completed a pilot study and two cluster trials: one in mainstream elementary schools, where our primary outcomes were physical activity, play, and social skills, and the second in schools with substantially separate programs for autistic children, many of whom also had intellectual disabilities. The primary outcomes in that study were play and coping skills. Play was the medium in both rounds.
The Sydney Playground Project consisted of two interventions. The first was changing the physical environment of the playground by adding loose parts (i.e., recycled materials) that children could use in whatever way they chose (Figure 4).
Sydney Playground Project: Child using recycled materials on the playground.
We named the second intervention “risk reframing.” Risk reframing comprised a series of small- and large-group activities conducted, as much as possible, with parents and teachers together. We deemed risk reframing to be necessary. Although the likelihood of even minor injury was small, we worried that a few fearful adults could create enough discomfort to threaten the playground experiences and the project. We included parents and teachers together so that each group could see that the other group held the same hopes for the children and the same fears of being thought to be a bad parent or a bad teacher (Niehues et al., 2013).
A card sort in which small groups of participants agreed on three characteristics they wanted for their children as they grew up was an important risk- reframing activity in both trials. Interestingly, participants in all schools selected resilience as a top trait. This occurred so often that we began to ask participants what they were doing to promote resilience, pointing out that resilience comes about only in the face of significant difficulty or failure. That realization marked an “aha moment” for many participants.
We also asked participants to tell stories about activities they had done as children that they could not wait to get to. Most of the stories involved risky play involving water, climbing trees, and riding go-carts fast downhill. There were never any adults in the stories and, unsurprisingly, most of the stories ended with “But we would never let children do these things today. We have a duty of care.”
In response, we began asking participants whether their parents had been negligent or whether they had learned something valuable that they would not have learned if adults had been present. After thinking, and talking more, participants often responded that they had learned to take responsibility for their safety, and often for that of a younger sibling: “If a parent had been there, they would have decided whether an activity was safe. We would not have thought about it.” That marked another aha moment.
In the second round of the Sydney Playground Project (Bundy et al., 2015), in which we intervened with autistic children, many of whom also had an intellectual disability, we videotaped and analyzed potentially risky occurrences: times when adults got involved or when we assumed an adult would have gotten involved had they seen the event. Not surprisingly, teachers often stepped in to prevent potential harm before it occurred. They seemed more concerned about what might happen, or what children might do, than what they did do.
Here’s an example:
Two children were engaged in imaginative play. One child was handing out “awards” as prizes. That child pick[ed] up a stick . . . to hand to the other child. A teacher [came] over and reprimand[ed] them for picking up a stick. [It was against school rules.] (Spencer et al., 2016, p. 311)
Why did teachers stop the play? Teachers often justified their decisions by blaming children’s perceived deficits arising from autism (“They just don’t have good judgment,” “They don’t see danger”) or school rules (“No sticks,” “Don’t climb too high”). Spencer et al. (2016) wrote that teachers explained that shutting down opportunities for children to engage in risk is logical. But we as researchers secretly believed that stopping the play emanated from fears about risks to themselves (i.e., being thought to be a bad teacher).
We also interviewed school personnel after the end of the project. They held widely differing beliefs about the children and, hence, about the project. Not surprisingly, children whose teachers/administrators believed in them fared the best. In fact, many of those whose teachers felt the children required bubble-wrapping did not change on some measures (coping) and got worse on others (sophistication of play; Grady-Dominguez et al., 2021).
One teacher in a school that expected a lot from the autistic children said this:
I don’t think I think of them any differently. They play the same games that other kids play, and they do the same things that other kids do, so . . . I let them do their own thing. Why not? And if they look like they’re going to . . . get injured or hurt someone, of course I’ll step in. (Grady-Dominguez et al., 2021, p. 13)
Contrast the beliefs inherent in that quote with this one from a teacher in a school that saw autism first and felt their primary role was to keep children safe:
Some of them don’t get the rules, and they don’t understand the danger. A lot of the kids don’t have any understanding of the danger. I feel some do, but I think a lot of them are just trying to get through the day. (Grady-Dominguez et al., 2021 p. 9)
The parents and teachers we studied were ordinary people who just wanted the best for their children. And it’s not just children with a disability whose parents and teachers fear for their safety. In her doctoral work, Anita Niehues asked parents of typically developing children when they thought their children would be ready to cross the street or walk to school alone. Several responded, “probably when they are 12 or so, by the time they go to secondary [high] school” (Niehues et al., 2013, p. 13).
Social psychologist Jonathan Haidt (ExcelinEd, 2023), author of numerous books, including a new one entitled The Anxious Generation: How the Great Rewiring of Childhood Is Causing an Epidemic of Mental Illness (Haidt, 2024), suggested that children born prior to 1981 (i.e., Gen X, Boomers) went out to play unsupervised when they were 6 or 8. But children born after 1995 (Gen Z) need two digits in their age before they are allowed to play unsupervised. Childhood has changed completely—and not because the world has gotten less safe. In fact, despite what the media portray, the world is safer now than it ever has been. Life expectancy continues to rise (Dattani et al., 2023), and child mortality is falling (see https://childmortality.org/data). Serious injuries often happen at home or in the car (Centers for Disease Control and Prevention, 2020).
Bubble-wrapping children and keeping them always under the watchful eye of adults has consequences. Haidt (ExcelinEd, 2023) described a cycle of incompetence (Figure 5) in which adults assume children are socially and physically incompetent. Hence, they ban risky play and mitigate all conflict. As a result, children become socially and physically incompetent.
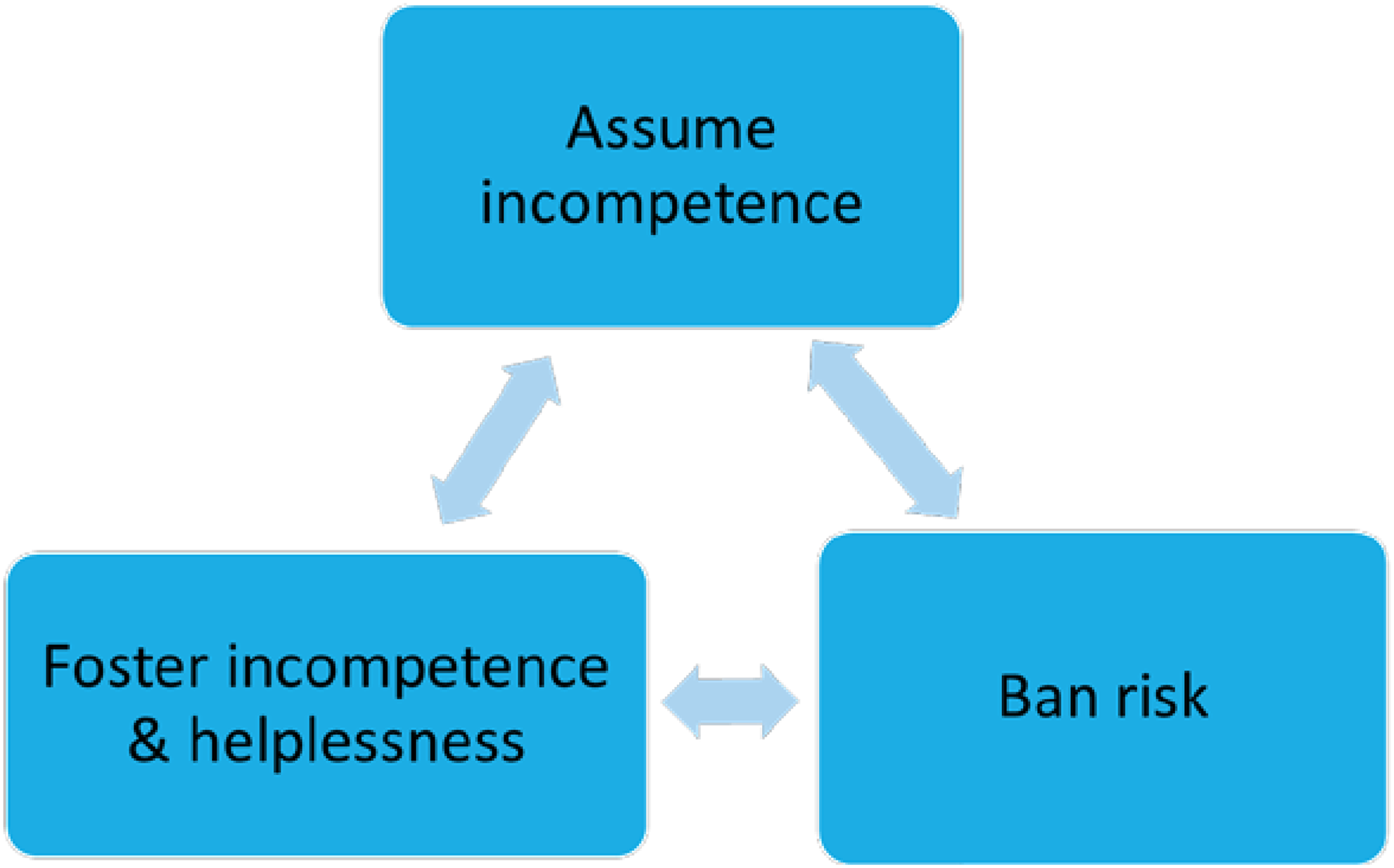
Cycle of incompetence.
Children are not the only ones at risk for overprotection. Thompson and Sobolew-Shubin (1993) pointed out that caregivers often underestimate older adults, especially those with chronic illness. Consequently, caregivers do things for adults that those adults would be fully capable of doing themselves. Thompson and Sobolew-Shubin (1993) defined “overprotection” as a “perception on the part of . . . [adults that they are] overhelped, induced to be dependent, shielded from stress, and generally not treated as adult[s]” (p. 87).
Falls are a common concern for older adults. In a recent study, Steckhan et al. (2023) argued that people who have fallen, or who are afraid of falling, engender feelings of overprotection in their caregivers. However, drawing on a substantial body of research, they pointed out the following:
The restriction of activities due to a fear of falling can indeed reduce falls (Rivasi et al., 2019). However, avoiding activities results in deterioration in physical functioning, which in turn increases the risk of falls (Liu et al., 2020; Whipple et al., 2018). This process can lead to a downward spiral of immobility (Clemson et al., 2012) and may result in a loss of independence in the long term. (p. 437)
In fact, Hajek and König (2020) found just that in a sample of older adults: Fear of falling predicted lower perceived autonomy 3 years later.
Of course, falls are only one concern for older adults. Haidt’s (ExcelinEd, 2023) cycle of incompetence seems to apply equally well to older adults and to all people with a disability in a range of circumstances. Overprotection of people of all ages and abilities leads to feelings of helplessness and incompetence.
In reference to the children they studied, Niehues et al. (2013) asked a key question: “How do children learn the limits of their abilities if there is never any risk of failing?” (p. 224). To learn how much we are capable of doing will involve failing.
Failing is not all bad. Failing lays the foundation for living with one’s own, and others’, fallibility in an unpredictable world. Finally, resilience is derived from failing (Kvalnes, 2017). (You may remember that Sydney Playground Project parents and teachers agreed that resilience was a trait they all wanted for their children.)
Niehues et al. (2013) went on: “If they are never allowed to experience discomfort, how do children develop physical skills, learn to regulate their emotions, extend themselves in social relationships or persevere in the face of cognitive challenges?” (p. 224).
The questions Niehues et al. (2013) asked about learning one’s limits and persevering in the face of challenges pertain equally well to adults:
How do [adults] maintain their abilities if they are offered only activities where there is no risk of failing? Furthermore, if they are never allowed to experience discomfort, how do [those adults] maintain skills, regulate their emotions, extend themselves in social relationships or persevere in the face of cognitive challenges? (p. 224)
What if there is no risk? When people are prevented from taking risks, they do not have the opportunity to overcome their fears, even when they actually have the ability to handle the situation (Kvalnes & Hansen Sandseter, 2023).
What allowed some of the participants in Niehues et al.’s (2013) study to permit their children to take risks even knowing and sometimes fearing potential consequences; that is, what allowed them to see that the benefits outweighed the risks? For one group, Niehues et al. (2015) explained:
Parents who had experienced threats in life themselves, for example, growing up in a war-torn country, caring for a baby hospitalized with life-threatening asthma, or parenting a child with a serious, lifelong disability, chose to acknowledge life’s uncertainties. They took on some risks themselves to make sure their children did not miss out on the benefits of age-appropriate risk taking because of their own fears. (p. 817)
It boils down to respect: trusting that most people are good judges of what they can and cannot do (Sennett, 2003). When we perpetually do things for others that they are fully capable of doing for themselves, or continually say, “You can’t,” we give the message “You are not capable.” Sooner or later those people believe us. Is that the message you want to give?
If you watched the 2024 Super Bowl, or 2024 women’s March Madness basketball, you may have seen the Dove Body confidence-in-sports commercial (Dove US, 2024). The gist of that commercial applies beyond sport. Knocks don’t stop people—not believing in themselves does. When important others don’t believe in us, we stop believing in ourselves. No matter our age or ability, we all need, and enjoy, a challenge.
Taleb (2012) called the increased capability to thrive as a result of stressors “antifragility”:
Just as spending a month in bed . . . leads to muscle atrophy, complex systems are weakened, even killed, when deprived of stressors. . . . This is the tragedy of modernity: As with neurotically overprotective parents, those trying to help are often hurting the most. (p. 5)
Taleb’s concept of antifragility, and Haidt’s (ExcelinEd, 2023) cycle of incompetence, cause us to ask whether removing all risk is possible, practical, or desirable.
What is safety, anyway? Ball and Ball-King (2011) offered this suggestion: If there are words to avoid, safe and safety could be them.
On the one hand, those words mean such different things to [different] people, including professionals, that they are best circumvented; although if this proves impossible, and it may do because they are so frequently used [e.g., in AOTA’s Code of Ethics], be careful to state what you mean. (p. 19)
Be careful for which person, at which time, and under what circumstances?
Ball and Ball-King (2011) went on: “If you should be so rash as to say that some activity or thing is ‘safe,’ then you may be interpreted as having guaranteed zero risk, which, being a virtual impossibility, would render you a hostage to fortune” (p. 19).
Although safety is difficult to define, and zero risk is virtually impossible to achieve, safety is not irrelevant. Sometimes risks do outweigh benefits. In his book The Anxious Generation, Jonathan Haidt (2024) argued compellingly that children today are not safe. But this is not because of crime, or perverts, or drunk drivers, all of which have decreased. Haidt argued that the end of play-based childhood (circa 2010) and the birth of a phone-based childhood (circa 2012) has led to increased anxiety, social deprivation, sleep deprivation, attention fragmentation, and a rise in serious behavioral addictions. He called for sharp decreases in smartphones (not before age 14 yr) and social media (not before age 16 yr) as antidotes.
Returning from a phone-based childhood to a play-based childhood will not be easy for anyone. But consider that it may be even more difficult for children from low socioeconomic backgrounds and some children of color. Going outside to play is more difficult for many of those children than it is for White or middle- or upper-class children. Parents living where needles are on the playground, or drug deals or prostitutes frequent the neighborhood, understandably want their children at home. And there are families under increased surveillance (e.g., families of color, undocumented families) who rightly fear what will happen to them if others see their child engaging in risky play. Newscasts are full of stories of Black youth, innocent of any crime, detained by police; some have lost their lives. Those children are safer at home than on the streets (Gerlach et al., 2019; Pinckney & Outley, 2023).
But all children (not just children of privilege) need and deserve the benefits that come from play and risky play. Sometimes, it will be up to schools and other entities to make sure there are spaces for risky play. Jonathan Haidt (ExcelinEd, 2023) and his colleague Lenore Skenazy (labeled “the world’s worst mom” because, in 2008, she allowed her 9-year-old son to ride the subway alone) offered some ideas: longer recess periods with less adult interference, school playgrounds that open half an hour before school starts, a play club where children can sign up to remain on the school playground for a set time after school one day each week. They also mentioned placing “loose parts” (e.g., cardboard boxes, car tires) on the playground.
It is not just children who are sometimes unsafe; not all adults are safe, either. But adults and people of all ages with a disability deserve a risk–benefit analysis.
Here is a formula for a risk–benefit analysis you as a professional working with your clients or as a parent or a caregiver can complete: ▪ First, explicitly list the potential benefits. What will be lost without doing the activity? ▪ Next, explicitly weigh the benefits against the potential of serious risk. ▪ Then, list mitigating factors (e.g., available supports). ▪ The bottom line is this: Answer the question “Is the potential risk acceptable given the expected benefits and available supports” (Figure 6)? Risk–benefit analysis.
When I put “Bubble Wrap” in the title of this talk, I had no idea how many ways that would be fitting. Two engineers, Alfred Fielding and Marc Chavannes, developed bubble wrap in 1957. They sealed two shower curtains together, capturing bubbles of air between them. They planned to market it as wallpaper. That never took off. Then, they sought to market it as greenhouse insultation. That also failed. Several years later, bubble wrap became popular for wrapping packages. It was never meant to be for people—except perhaps for stress reduction. The best part is that, more than 40 yr after its initial failure, Fielding and Chavannes were inducted into the New Jersey Inventors Hall of Fame (“Bubble Wrap (Brand),” 2024).
Here is one final story. Aimee Mullins is a model, an actress, and a public speaker. In 1996, she was a Paralympian. Aimee was born with fibular hemimelia. As an infant, both her legs were amputated below the knee. Aimee has told the following story: As a 5-year-old, she bargained, unsuccessfully, to get out of physical therapy. One day, her doctor came into physical therapy and remarked, “Wow! Aimee, you are such a strong and powerful little girl, I think you’re going to break one of those bands. When you do break it, I’m going to give you a hundred bucks” (Pangambam, 2019, p. 17). As an adult, Mullins advised,
The question isn’t whether you’re going to meet adversity, but how you’re going to meet it. . . . Our responsibility is not simply shielding those we care for from adversity but preparing them to meet it well. And we do a disservice . . . when we make [any person] feel they’re not equipped to adapt. . . . All you really need is one person to show you the epiphany of your power, and you’re off. (Pangambam, 2019, pp. 30, 31, 63)
I challenge you to be that person—that parent, that caregiver, that professional.