
Abstract
This study presents important insights into the impact of occupational performance coaching on patients with heart failure.
Heart failure (HF) is a complex clinical syndrome resulting from a functional or structural abnormality of the heart. The prevalence of HF has been reported to be 8.1% among Iranian people. Symptoms such as fatigue, breathlessness, reduced exercise capacity, and ankle swelling accompany HF (Ahmadi et al., 2014), leading to restricted activity engagement (Nordgren & Söderlund, 2016) and participation (Olano-Lizarraga et al., 2023). For instance, fatigue, muscle weakness, and limited mobility can affect the ability to perform household activities or engage in leisure. Additionally, concerns about safety during physical activities may lead to avoidance of these activities. Studies have suggested that managing these symptoms can improve the activity participation and quality of life (QOL) of individuals with HF (Nordgren & Söderlund, 2016; Olano-Lizarraga et al., 2023).
Optimal health self-care behavior (HSCB) can enhance the activity participation of patients with HF (Bhuyan, 2004). HSCB is defined as a decision-making process that influences actions to enhance knowledge and understanding of symptoms, maintain physiological stability, and direct symptom management (Riegel et al., 2016). HSCB of patients with HF are essential to maintain independence (Harkness et al., 2015), optimize health outcomes and disease management (Graven & Grant, 2014; Jaarsma et al., 2021), and reduce morbidity and mortality, leading to improved QOL. Conversely, inadequate HSCB can exacerbate symptoms of the disease, leading to hospitalization (Calero-Molina et al., 2022) and hindering participation in activities and occupations (American Occupational Therapy Association, 2020).
Despite efforts to support HSCB, it remains poor among people with HF (Liljeroos et al., 2020). Only 4.4% of HF patients in the Iranian population had desirable HSCB (Mansouri et al., 2018). The lack of HSCB may be due to education that focuses on increasing knowledge without effectively supporting behavioral change (Dickson & Riegel, 2009). Promoting HSCB is a process that requires support for behavioral changes (Flores et al., 2020). Therefore, interventions that emphasize behavioral changes are crucial to improve HSCB among patients with HF.
Occupational therapy that incorporates a holistic, client-centered lifestyle approach can promote HSCB among patients with HF by supporting engagement and activity participation (Norris, 2020). Occupational performance coaching (OPC) is an occupational therapy intervention aimed at changing behavior and enhancing activity participation (Graham et al., 2020). OPC can help individuals develop habits and routines to achieve overall participation goals (Graham et al., 2020). OPC promotes autonomy and competence in achieving participation goals through a nondirective, client-centered approach (Chien et al., 2020). Collaborative performance analysis (CPA), a structured process of goal setting to overcome barriers and find solutions, and evaluation of planned actions to attain goals are used, with the therapist providing guidance and emotional support and facilitating knowledge exchange (Angelin et al., 2021; Kessler et al., 2021). Previous studies have found that OPC enhances performance of and satisfaction with participation goals among stroke patients (Kessler et al., 2017) and mothers of children with cerebral palsy (Ahmadi Kahjoogh et al., 2019), and it improves fatigue and self-efficacy among individuals with multiple sclerosis (Askari et al., 2022).
The impact of OPC intervention on the participation and HSCB of HF patients remains unexplored. In this study, we investigated the potential impact of OPC on improving HF patients’ HSCB and other outcomes as they worked toward achieving participation goals. Therefore, we planned a randomized controlled trial (RCT) to examine the effectiveness of the OPC intervention in improving activity participation and HSCB among patients with HF.
Method
Study Design
This study was a parallel-groups, single-blind (assessor-blind) RCT with a superiority design. Outcome assessments were administered at baseline, and follow-up assessments were done 8 and 12 wk after the intervention was completed. Both groups received one session of health self-care education, and the intervention group also received eight weekly sessions of OPC.
The evaluation and interventions were performed in the cardiac rehabilitation department of the Rajaie Cardiovascular, Medical, and Research Center. This study was approved by the Iran University of Medical Sciences institutional review board and has been registered with the Iranian Registry of Clinical Trials (Ethical Code IR.IUMS.REC.1399.1414 and IRCT20120910010806N10).
Recruitment
The participants were consecutively recruited from an outpatient HF clinic in the Rajaie Cardiovascular Center in Tehran. In the clinic, an occupational therapist and a cardiologist assessed patients for eligibility. The inclusion criteria were as follows: ▪ between ages 18 and 65 yr ▪ left ventricular ejection fraction (EF) ≤ 40% based on echocardiography (6 mo minimum) ▪ clinical diagnosis of HF categorized by a cardiologist as New York Heart Association (NYHA) Class I, II, or III ▪ normal cognitive function (the Persian version of Mini-Mental State Examination [MMSE] score >22; Ghanbari et al., 2013) ▪ score <70 on the Persian version of Self-Care Heart Failure Index (SCHFI; scores >70 indicate sufficient HSCB; Riegel et al., 2019) ▪ ability to read, write, and fill out questionnaires.
The exclusion criteria were as follows: ▪ score >29 (severe depression) on the Persian version Beck Depression Inventory (BDI; Ahrari et al., 2013) ▪ HF due to cardiac comorbidity with an unstable medical condition, including patients who had undergone coronary artery bypass graft or heart surgery, experienced acute coronary artery syndrome in the past 2 wk, or had a myocardial infarction or pericardial effusion in the past 4 wk (based on medical record) ▪ HF caused by a treatable condition or factor, such as untreated primary valve disease (Sherwood et al., 2017), ventricular arrhythmia, myocarditis, or hypertrophic cardiomyopathy (based on medical record) ▪ history of claudication and chronic obstructive pulmonary disease (based on medical record) ▪ receipt of other occupational therapy services ▪ diagnosis of major psychiatric problems ▪ being infected with COVID-19 ▪ presence of hearing and vision problems.
The eligibility criteria (Ahmadizadeh et al., 2023) were checked by both an occupational therapist and a cardiologist. A research team member (an occupational therapist) explained the study to potential participants who met the inclusion criteria and obtained their written informed consent. All patients provided signed informed consent.
Randomization
Randomization was done via computer-generated block randomization (block sizes were 4 and 6). Generation of the allocation sequence was done by one of the authors who was not involved in the intervention. The occupational therapist notified participants of their group assignment.
Participants
In this study, 243 patients with HF were screened on the basis of inclusion criteria. According to the sample size determined for the RCT, 44 HF patients who met the eligibility criteria, as described in the RCT protocol article (Ahmadizadeh et al., 2023), participated in the study (Figure 1). These participants were randomized into two groups, and both groups received one session of usual health self-care training. The intervention group also received eight sessions of OPC intervention.
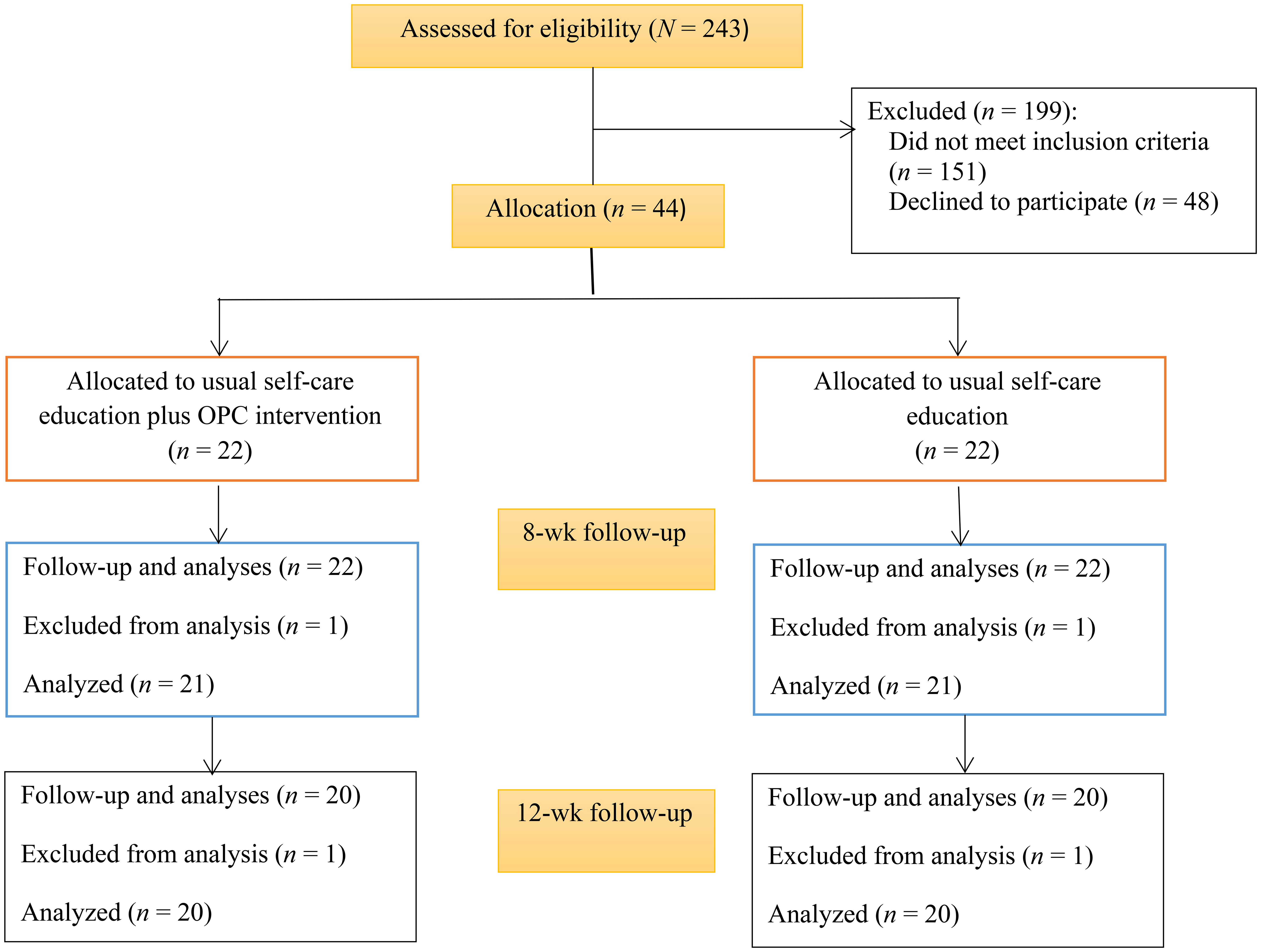
Flow of participants through the trial.
Power Analysis
The sample was calculated using G*Power 3.1 software (Faul et al., 2009). The confidence level was 95% with Cohen’s F = 0.4, the test power value was 0.8, and the sample size was calculated as 20 patients with HF in each group. The sample size was 44 HF patients, allowing for a 10% dropout probability.
Control Group: Usual Health Self-Care Education
All participants were given educational materials on HSCB for patients with HF. In the first session, both groups received 40 to 50 min of face-to-face, individual health self-care education led by a cardiac nurse. The hospital health self-care education session was based on the HF health self-care training booklet, which covered important symptoms of cardiovascular disorders, prevention of cardiovascular disorders and HF, activity, nutrition, sexual activity, risk factors for cardiovascular diseases, bathing, medication management, and how to contact their doctor if they experienced any symptoms. After the initial session, the control group received no further support. The education booklet was developed by the health self-care education team, including cardiac nurses and nursing faculty, at Rajaie Cardiovascular, Medical, and Research Center and was approved by five cardiologists. As the target audience, inpatients and outpatients with HF assessed the booklet.
Intervention Group: Health Self-Care Education Plus OPC Intervention
The intervention group received health self-care training plus eight weekly one-to-one sessions of OPC delivered by an occupational therapist. The first and last sessions were delivered face-to-face, whereas the others were delivered via phone because of the COVID-19 pandemic. In the first session, semistructured interviews were conducted using the Persian version of the Canadian Occupational Performance Measure (COPM; Dehghan et al., 2011) to guide the participants to set three activity participation goals related to their occupations. Participants were then asked to measure their satisfaction with and performance of their goals on a 10-point Likert scale (with 10 indicating higher performance or satisfaction).
After setting these goals, the problem-solving process started for the goal determined by the participant to be most important. Using the Person–Environment–Occupation (PEO) model and a diagram of the problem-solving process (Graham et al., 2020), the occupational therapist initiated the intervention using the CPA process and PEO model and guided the participant to analyze the selected goal and identify up to three required steps or activities to work toward achieving that goal (Graham et al., 2020).
The next session began by asking the participants about the activities they had done in the past week. Participants talked about whether they performed the activity, and facilitators and barriers were examined. In each OPC session, the participants and therapist determined some activities (a maximum of three) to perform for the next session that would help them achieve their goals. At the conclusion of each session, the occupational therapist scheduled the next session. All sessions were 1 wk apart. The intervention lasted for 2 mo, and all participants received eight sessions (Table 1).
8-Wk Occupational Performance Coaching Intervention Plan
Data Collection
Outcome assessments were administered at baseline and 8 and 12 wk postintervention. One of the participants in the intervention group was excluded from the 8-wk assessment because of COVID-19. One control group participant was unable to be present at the first follow-up assessment because of worsening HF symptoms. Therefore, follow-up assessments were conducted for two groups of 21 participants each. At 12 wk, 1 participant in each group did not participate in the assessment (n = 20 per group).
The primary (HSCB and participation) and secondary (depression, QOL, self-efficacy, cognition, fatigue, social support, activities of daily living [ADLs], and functional capacity) outcome measures were administered by an assessor blind to group allocation at all time points.
Primary Efficacy Outcome Measures
The Persian SCHFI (Zamanzadeh et al., 2012) measures HSCB, with scores ranging from 0 to 100 (higher values are desirable). The Persian SCHFI is acceptable and has strong reliability (r = .96) for evaluating health self-care among HF patients. Participation (satisfaction and performance) was assessed using the reliable Persian version of the COPM. The Persian COPM demonstrated strong test–retest reliability (rs = .84–.87; Dehghan et al., 2015).
Secondary Efficacy Outcome Measures
The BDI was used to assess depression. The Persian BDI showed strong internal consistency (Cronbach’s α = .91; Dobson & Mohammadkhani, 2007). The Iranian version of the Minnesota Living with Heart Failure Questionnaire was used to evaluate QOL. This questionnaire showed strong reliability (r = .9, Cronbach’s α = .96; Abbasi et al., 2016; Eskandari et al., 2015). The Persian Cardiovascular Management Self-Efficacy scale demonstrated strong test–retest reliability (r = .98, Cronbach’s α = .8; Rajati et al., 2021). The Persian version of the MMSE showed strong internal consistency (Cronbach’s α = .81; Seyedian et al., 2007). The Fatigue Severity Scale (FSS) was implemented to evaluate fatigue among patients with HF. The FSS has acceptable content validity and internal consistency (Cronbach’s α = .85) (Seifi et al., 2018). The Persian version of the Medical Outcome Study Social Support Scale was used to evaluate social support. This scale demonstrated strong internal consistency (Cronbach’s α = .96; Mohammadzadeh & Sayehmiri, 2016). The Persian version of Lawton’s Instrumental Activities of Daily Living Scale showed a high correlation coefficient (r = .9) among HF patients using the test–retest method (Hekmatpou et al., 2010). The 6-Minute Walk Test (6MWT) was used to evaluate functional capacity; it showed good reliability and moderate validity (Pollentier et al., 2010).
Statistical Analysis
Data analysis was conducted using IBM SPSS Statistics (Version 18) with a significance level of .05. To assess the normality of the data, we used the Shapiro–Wilk test, histogram, skewness, kurtosis, Q–Q plot, and means and standard deviations. Independent-samples t tests and χ2 were used compare differences at baseline between the two groups. The results of two-way repeated-measures (Time × Group) analysis of covariance (ANCOVA) for three assessment points were used to evaluate changes on the primary and secondary outcome measures. In this analysis, the dependent variable was either a primary or a secondary outcome, with the level of EF and severity of depression serving as confounding variables, and the independent variables were the three assessment points. Post hoc analyses were conducted on significant results of the two-way repeated-measures ANCOVA, which was Bonferroni adjusted to guard against Type I error. Cohen’s d was used to calculate the index of effect sizes.
Results
As shown in Table 2, 40.9% and 31.8% of the participants in the intervention and control groups, respectively, were female. The mean age of the participants was 43.82 yr (SD = 10.59) in the intervention group and 45.5 yr (SD = 11.38) in the control group. Notably, 7 participants (3 in the intervention group and 4 in the control group) were younger than age 30 yr. Most of the participants in both groups were categorized as NYHA Class I. The χ2 results showed no difference between the groups in NYHA functional class. The results of the test of normality showed that all variables could be considered normal. The result of the independent t test showed no significant differences between the two groups in blood pressure, age, gender, income, education level, EF, and hospitalization in the past year (p > .05). There were no significant baseline differences in primary and secondary outcomes between the two groups (p > .05).
Comparison of Outcomes, by Groups at Baseline
Note. Ranges in parentheses indicate possible scores. ADLs = activities of daily living; BMI = body mass index; COPM = Canadian Occupational Performance Measure; EF = ejection fraction; NYHA = New York Heart Association; QOL = quality of life; RCT = randomized controlled trial; 6MWT = 6-Minute Walk Test.
High values are desirable.
Low values are desirable.
Primary Outcomes
Using the COPM, participants in the intervention group chose 47 activity participation goals. Twenty-two (46.8%) were leisure goals, 18 (38.3%) were productivity goals, and 7 (14.9%) were health self-care goals. The participants in the control group chose 48 activity participation goals; 23 (47.9%) were leisure goals, 17 (35.4%) were productivity goals, and 8 (16.7%) were health self-care goals.
Table 3 shows the results of a two-way repeated-measures (Time × Group) ANCOVA for three assessments of HSCB and occupational performance and satisfaction. The analysis indicates a significant difference between the two groups (p < .05). The results of the post hoc analyses showed that at baseline the two groups did not differ significantly, but the follow-up assessments at 8 and 12 wk showed significant improvement in HSCB and occupational performance and satisfaction among the intervention group (p < .05).
Mean Scores at Baseline and 8- and 12-Week Follow-Up Assessments and Comparison of Outcomes by Group
Note. Ranges in parentheses indicate possible scores. ADLs = activities of daily living; 6MWT = 6-Minute Walk Test; QOL = quality of life.
High values are desirable.
Low values are desirable.
*p < .05. **p < .01.
Secondary Outcomes
The results of two-way repeated-measures (Time × Group) ANCOVA for three assessments of self-efficacy, cognitive level, fatigue, social support, QOL, functional capacity, and ADLs showed no significant difference between the two groups (p > .05). The ANCOVA showed a significant difference in depression severity between the two groups (p < .05), and the results of the post hoc analyses showed that at the baseline and 8-wk follow-up assessments, the two groups did not differ significantly (p > .05). However, at the 12-wk follow-up assessment, the intervention group showed a significant decrease in depression severity (p < .05).
Discussion
This RCT found that the OPC intervention improved HSCB, performance, and satisfaction with activity participation goals and decreased depression severity among HF patients. In addition, this RCT showed that 8 wk of OPC intervention did not improve social support, self-efficacy, cognition level, fatigue severity, QOL, ADLs, and 6MWT scores among HF patients.
The study found a positive impact on performance of and satisfaction with activity participation goals. Through OPC, HF patients are guided to identify and apply effective solutions to activity participation problems in collaboration with their therapist (Graham et al., 2020). Goal setting and the active engagement of participants during the OPC intervention provided the opportunity to learn problem-solving skills. The CPA process during OPC empowers individuals to develop strategies to overcome barriers autonomously (Graham et al., 2020) and improve their ability to address daily challenges, which is crucial in managing a chronic condition such as HF.
Achieving goals during OPC enhances meaningful participation in valued life occupations (Graham et al., 2020). Meaningful participation in activities, whether they involve work, leisure, or social interactions, can positively affect an individual’s motivation and ability to engage in HSCB because a sense of purpose and fulfillment derived from participation in activity can enhance an individual’s commitment to positive HSCB (Alcorn & Broome, 2014). During the OPC intervention, regular interaction with coaches may also increase motivation and provide the support needed for patients to change their behavior (which was advised in the health self-care education session) and engage in HSCB.
An alternate explanation may be that HF patients improved their health self-care habits and routines to enhance their activity participation. During the process of taking action to achieve goals, participants may have realized that achieving their participation goals was not possible unless they incorporated HSCB. In other words, with the OPC intervention, HF patients discovered that to lead more active and fulfilling lives, they needed to effectively manage their symptoms via performing HSCB.
Engaging in HSCB can have an impact on important occupational goals in several ways. By maintaining good physical health through practices such as regular exercise and proper nutrition, individuals are more likely to have the energy, stamina, and resilience needed to perform well in their social roles. Additionally, maintaining mental well-being through stress management techniques can enhance focus, productivity, and overall occupational performance. Overall, prioritizing HSCB may contribute to better occupational satisfaction, higher levels of productivity, and increased opportunities to advance participation. Further research is needed to examine the interaction between improving HSCB and occupational performance and satisfaction.
This study adds to the evidence for health coaching. Effective health coaching interventions are designed to change behaviors (Huffman, 2016) and emphasize health self-care skills development (Dickson et al., 2011). For example, RCT studies on telecoaching have reported improved HSCB and maintenance of blood pressure and daily weight during the intervention (Stut et al., 2015). Coaching has also reduced the severity of dyspnea and increased physical function among patients with HF (Wongpiriyayothar et al., 2011). In another study, short-term coaching significantly improved depression and HSCB but did not significantly improve self-efficacy, satisfaction, and health care use (McCusker et al., 2015). In line with these findings, Tiede et al. (2017) reported that telephone-based health coaching helped to decrease health risk behaviors among HF patients. These coaching interventions tended to report improvement in HSCB after long-term coaching and were focused more on improving health outcomes than on patients’ participation in life activity. The OPC intervention adds a focus on participation goals while incorporating behavior change and skill development; therefore, using OPC as one of the coaching interventions could improve both activity participation and HSCB at the same time.
This study also contributes to the evidence supporting the effectiveness of OPC among patients with chronic conditions. OPC was found to enhance HF patients’ activity participation and health self-care skills. Previous studies have reported that OPC could improve performance and satisfaction with participation goals among people with stroke (Kessler et al., 2017), people with multiple sclerosis (Kessler et al., 2024), and mothers of children with cerebral palsy (Ahmadi Kahjoogh et al., 2019). Given the promising impact of the OPC intervention, further research is needed with patients with chronic conditions to determine its clinical effects in both the short and long terms. This study also builds on the evidence demonstrating that OPC can be delivered remotely. Other studies have found OPC to be feasible and acceptable when delivered by telephone or video conferencing (Kessler et al., 2021).
The study’s results indicate that, although the OPC intervention did not reduce depression severity compared with usual health self-care education immediately postintervention, there was a significant decrease in depression severity at the 12-wk follow-up. Poor participation can lead to decreased emotional well-being (Egan et al., 2014). The significant improvements in COPM scores between baseline and follow-up assessments may be associated with reduced depression in the longer term. This may be due to increased opportunities for social connection and engaging in meaningful and enjoyable activities as a result of the OPC intervention. These can help increase feelings of pleasure and satisfaction with performance and consequently reduce depression among patients with HF. Hao et al. (2017) also reported that depression is related to reduced engagement in social and leisure activities.
Although increased self-efficacy was expected, the results showed no significant change in self-efficacy. This could be because engaging in HSCB can enhance self-efficacy over extended periods (Chen et al., 2014). Our intervention spanned 2 mo, whereas Askari et al. (2022) carried out their intervention over 3 mo and noted a moderate influence of OPC intervention on the self-efficacy of individuals with multiple sclerosis. Further research with a larger sample is necessary to fully assess the efficacy of OPC with HF patients. Additionally, longer-term patient follow-up is needed to determine whether participants require more time to observe improvements in these outcomes. Additionally, in this study, the duration of the OPC intervention may not have been sufficiently long to yield substantial enhancements in QOL for HF patients.
The lack of significant change observed in self-efficacy, cognitive level, fatigue, social support, QOL, functional capacity, and ADL scores among participants could be attributed to the high baseline scores of individuals in this study. Higher baseline scores can result in limited potential for significant change, particularly because a majority of the HF participants in the study were categorized as NYHA Classes I and II.
Limitations
This study was designed to compare OPC with usual care. However, usual care was limited to 1-wk follow-up and therefore did not also provide a control for attention over the intervention period. Future research should consider how the control group can be used to control for factors such as attention. In this study, the fidelity of implementation of the OPC intervention was not confirmed. Although we attempted to have treatment fidelity assessed by a trained observer, the bilingual occupational therapist assistant researcher was not able to assist and facilitate the review of sessions as planned. Therefore, measures of treatment fidelity may not be accurate. However, participants made gains in their performance and satisfaction with participation goals with the level of fidelity that was achieved.
Future Research
Future studies could delve deeper into the long-term effects of OPC on HSCB, activity participation, and other outcomes among patients with HF and include an examination of the mechanisms of action. Longitudinal studies following patients over an extended period postintervention could provide valuable insights into the sustainability of the improvements observed. Additionally, investigating the optimal frequency and duration of OPC sessions for maximizing benefits and exploring potential moderators or mediators of the intervention effects could further enhance understanding of how OPC can be tailored to different patient populations. Furthermore, comparative effectiveness research comparing OPC with other interventions or treatment modalities in HF management could offer valuable information for health care providers and policy makers in optimizing care for these patients.
Implications for Occupational Therapy Practice
Recently, participation-focused interventions have been used in populations experiencing ongoing disability or chronic health issues. In the context of individuals with HF, this research has the following implications for occupational therapy practice: ▪ OPC could be used to indirectly improve HF patients’ HSCB during the process of achieving participation goals. ▪ The OPC intervention could improve HSCB, activity participation, and depression among HF patients. ▪ OPC could be used as a client-centered and participation-focused treatment for HF patients.
Conclusion
This RCT demonstrated that the 8-wk OPC intervention can enhance activity participation and HSCB while also reducing the severity of depression among patients with HF. It is not clear whether HF patients must actively engage in HSCB to achieve their meaningful participation goals through OPC intervention or whether increased participation leads to improved HSCB. Attaining meaningful goals may also reduce the severity of depression. Participating in life activities through the OPC intervention led to reduced depression severity among HF patients 4 wk after the end of OPC interventions.
Given that some OPC sessions were held via phone, this study adds support for the successful use of this intervention in telerehabilitation. By integrating elements of OPC and HSCB, occupational therapy practitioners can offer effective interventions to improve their clients’ daily activities and overall well-being and have a potentially lasting impact.
Footnotes
Acknowledgments
We thank the manager and staff of the Cardiac Rehabilitation Department of Rajaie Cardiovascular, Medical, and Research Center. We appreciate Dr. Nasim Naderi, Masoomeh Kalaeinia, and Fatemeh Habibzadeh for their valuable assistance during the conduct of this study. We are grateful for the financial assistance from the Iran University of Medical Sciences. We declare no potential conflicts of interest with respect to the research, authorship, or publication of this article. This study was approved by the Iran University of Medical Sciences institutional review board (IR.IUMS.REC.1399.1414) and has been registered at the Iranian Registry of Clinical Trials (IRCT20120910010806N10). The study was funded by the Iran University of Medical Sciences (Grant 1400-1-1-21055). The datasets generated during or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.