
Abstract
This systematic review introduces the term early engagement to describe occupational therapy-specific interventions for patients recovering in the ICU.
Intensive care units (ICUs) are specialized hospital units that serve critically ill patients who require advanced medical support and monitoring by health care providers. In the United States, more than 5 million patients annually are admitted to an ICU, and this number is expected to increase along with the increase in the aging population (Desai et al., 2011; Society of Critical Care Medicine, n.d.). Adults needing ICU care include those experiencing respiratory insufficiency requiring mechanical ventilation, acute myocardial infarction, intracranial hemorrhage, cardiogenic shock, renal failure, and sepsis, with an overall mortality rate of 10% to 29% (Society of Critical Care Medicine, n.d.). Patients in the ICU often sustain short- and long-term effects on their health, including physical deconditioning, cognitive impairment, difficulty participating in activities of daily living (ADLs), and decreased quality of life (Desai et al., 2011; Zanni et al., 2010).
ICUs are noisy, fluorescent, and unfamiliar environments that can negatively affect patients’ mental and physical well-being (Chivukula et al., 2017). Sensory overload, sleep deprivation, isolation, and limited mobility can lead to patients experiencing ICU trauma presenting as fear, avoidance behaviors, and depression (Chivukula et al., 2017; Everson-Rose & Lewis, 2005). Patients whose ICU admission is prolonged may also experience muscle wasting, weight loss, pain, and restricted mobility because of lines and devices (Chivukula et al., 2017). These psychosocial and physical limitations can result in an increased risk for delirium, characterized by acute fluctuations in consciousness and cognitive function, and they are associated with poor health outcomes, including decreased ADL performance, cognitive impairment, longer hospital length of stay, and a higher mortality rate (Cavallazzi et al., 2012; Collinsworth et al., 2016; Green et al., 2019, Poulsen et al., 2021).
As holistic health care providers who optimize occupational participation, function, and well-being, occupational therapy practitioners play a unique role in addressing the complex physical and psychosocial needs of ICU patients (Costigan et al., 2019). In a scoping review, Costigan et al. (2019) found that occupational therapy practitioners in the ICU use various interventions, including physical rehabilitation, ADL retraining, mobility, and psychosocial support. Occupational therapy practitioners also address delirium through multisensory and cognitive stimulation, positioning, caregiver training, and environmental modifications (Tobar et al., 2017). Using these approaches in the context of occupations and meaningful activities, occupational therapy practitioners provide patients with opportunities to bridge the gaps between their former identities, current selves as patients, and potential future beyond their hospital stay.
Although occupational therapy addresses many needs of critically ill patients, a systematic review conducted by Weinreich et al. (2017) found little distinction between occupational and physical therapy services in the ICU, as well as a lack of evidence identifying and supporting specific occupational therapy ICU interventions. Recent research has focused on early mobilization, in which occupational therapists, physical therapists, or both facilitate patient movement to counter ICU-acquired weakness (Adler & Malone, 2012; Hashem et al., 2016). Although early mobilization is important, this intervention primarily targets physical deconditioning and is only one aspect of occupational therapy’s scope of practice (Costigan et al., 2019). To better capture the holistic care that occupational therapy provides beyond early mobilization, we propose the term early engagement to identify and critically examine occupational therapy–specific ICU interventions beyond what exists in the current literature.
Engagement is an emerging concept being studied in relation to health care. From their literature review of how engagement is being used in rehabilitation, Bright et al. (2015) defined engagement as “a co-constructed process and state … connecting [the patient and clinician] with each other and/or a therapeutic program, which enables the individual to become an active, committed and invested collaborator in healthcare” (p. 650). Therapists play a crucial role in engaging with patients through therapeutic listening, addressing needs, and showing empathy, all of which facilitate patients being actively engaged in their care (Bright et al., 2015). Increased engagement has been theorized to lead to greater initiation and motivation, thereby fostering less assistance with ADLs upon discharge and facilitating participation in long-term preventive behaviors to decrease complications and hospital readmissions (Maclean et al., 2000; Moua, 2020).
Expanding on this definition, we use early engagement to refer to occupational therapy interventions that specifically promote ICU patients’ participation in their care. Early engagement encompasses and goes beyond early mobilization to include interventions such as ADL retraining, psychosocial coping, functional cognition, and sensory regulation—all of which fall under occupational therapy’s scope of practice (American Occupational Therapy Association [AOTA], 2020). The purpose of this systematic review is to examine and analyze the strength of the evidence for early engagement interventions provided by occupational therapy practitioners in the ICU.
Method
This systematic review was conducted according to the Cochrane methodology (J. P. T. Higgins et al., 2019) and reported using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2010). We conducted an organized search culminating in a review of current literature to explore the research question “What is the strength of empirical evidence for occupational therapy interventions related to early engagement in the ICU?”
Search Strategy
The Cochrane Library was searched to determine whether a previous systematic review of occupational therapy’s role in the ICU had been published. Next, a systematic search strategy and search terms were developed in collaboration with a medical librarian and subject matter experts, and a literature review was conducted. Multiple databases were searched: CINAHL, PubMed, ProQuest, OTseeker, and the Cochrane Library. Databases were searched using Medical Subject Headings terms and text words to identify potential studies. For a sample search, see Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Eligibility Criteria
This review includes peer-reviewed journal articles published in English from January 2012 through December 2021. Studies were evaluated for eligibility on the basis of population, setting, levels of evidence, and intervention.
Population and Setting
Studies of patients age 18 yr or older in the ICU or critical care unit were included to focus on adult rehabilitation. Studies were included regardless of participants’ race, ethnicity, or gender. Studies conducted with patients at other levels of care or in which level of care was not specified were excluded.
Levels of Evidence
Studies were assigned levels of evidence per the Oxford Centre for Evidence-Based Medicine (2009): ▪ Level 1b: well-designed randomized controlled trials (RCTs) ▪ Level 2b: prospective cohort studies, lower-quality RCTs, and two-group, nonrandomized studies ▪ Level 3b: retrospective case-control studies, one-group, nonrandomized studies, and cohort studies.
Level 1b, 2b, or 3b studies were included, and Level 4 or 5 studies were excluded for rigor. Dissertations, theses, presentations, proceedings, instructional materials, editorials, and case studies were also excluded for lack of peer-review status.
Intervention
To be considered for inclusion, studies needed to involve specific occupational therapy interventions occurring in the ICU within the occupational therapy scope of practice per the Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; AOTA, 2020). Studies that did not specify occupational therapy treatments, discussed interventions outside occupational therapy’s scope of practice, or did not occur in the ICU were excluded.
Study Selection
Literature search results were collected, duplicates were eliminated, and articles were removed per the inclusion criteria; all of these tasks were performed manually by the first author (Morgan Smith). The remaining articles were initially screened by Smith on the basis of title and abstract; the second and third authors (Stephanie Tsai and Elyse Peterson) then screened the remaining articles on the basis of title and abstract, eliminating records not relevant to the research question or that did not meet the eligibility criteria. Articles that passed the initial screening were retained for full-text screening and reviewed by a minimum of two authors, with discrepancies resolved through discussion and consensus among all three authors.
Risk-of-Bias Assessment
We independently rated the risk of bias of each eligible study. Studies that included a control group, either randomized or nonrandomized, were assessed using the Cochrane risk-of-bias guidelines (Higgins et al., 2016); the results are provided in Table A.3. Table A.4 shows the risk-of-bias assessment for noncontrolled trials, based on the quality assessment tool developed by the National Heart, Lung and Blood Institute (2021). The risks of selection, performance, detection, attrition, and reporting biases were rated as high, moderate, or low according to the Cochrane or National Heart, Lung and Blood Institute guidelines. Discussion among us occurred to reach consensus if risk of bias was in question.
Analysis of Evidence
Smith extracted data from the final studies included in the review and entered them into an evidence table that summarized study information, including level of evidence, study design, participant characteristics, inclusion criteria, interventions, outcome measures, and results (Table A.2). All three authors independently reviewed each study and the corresponding data inputted into the evidence table to ensure thoroughness and reliability. The three authors then collaborated to analyze commonalities and group occupational therapy interventions and outcomes into broader categories. Occupational therapy domains, performance skills, and client factors according to the OTPF–4 were considered in analyses and groupings (AOTA, 2020). Descriptive summaries revealed three categories of occupational therapy intervention supporting patient engagement in the ICU: ADLs (routine personal care activities, including eating, grooming, bathing, and dressing), physical rehabilitation (exercises or functional movements to improve endurance, range of motion, strength, and motor skills), and cognition (mental functions, including attention, memory, and executive function; AOTA, 2020). Each category was analyzed for strength of evidence, as determined by the guidelines of the U.S. Preventive Services Task Force (2018), and divided into three levels: ▪ Strong: two or more Level 1b, well-designed, well-conducted studies with consistent results, indicating that the findings are unlikely to be questioned in future studies ▪ Moderate: at least 1 Level 1b study or multiple Level 2b studies supporting the current evidence and sufficient to determine effects, although confidence is limited ▪ Low: a small number of low-level studies with flaws, restricting the extrapolation of effects.
Results
A total of 5,707 studies were discovered through the database search. Duplicate records were removed (n = 223), and 4,175 studies were deemed ineligible according to the inclusion criteria through manual screening. Study abstracts were then reviewed, and an additional 1,255 studies were excluded. A total of 54 studies underwent full-text review, resulting in 9 studies included in the final review. See Figure 1 for the PRISMA flow diagram.
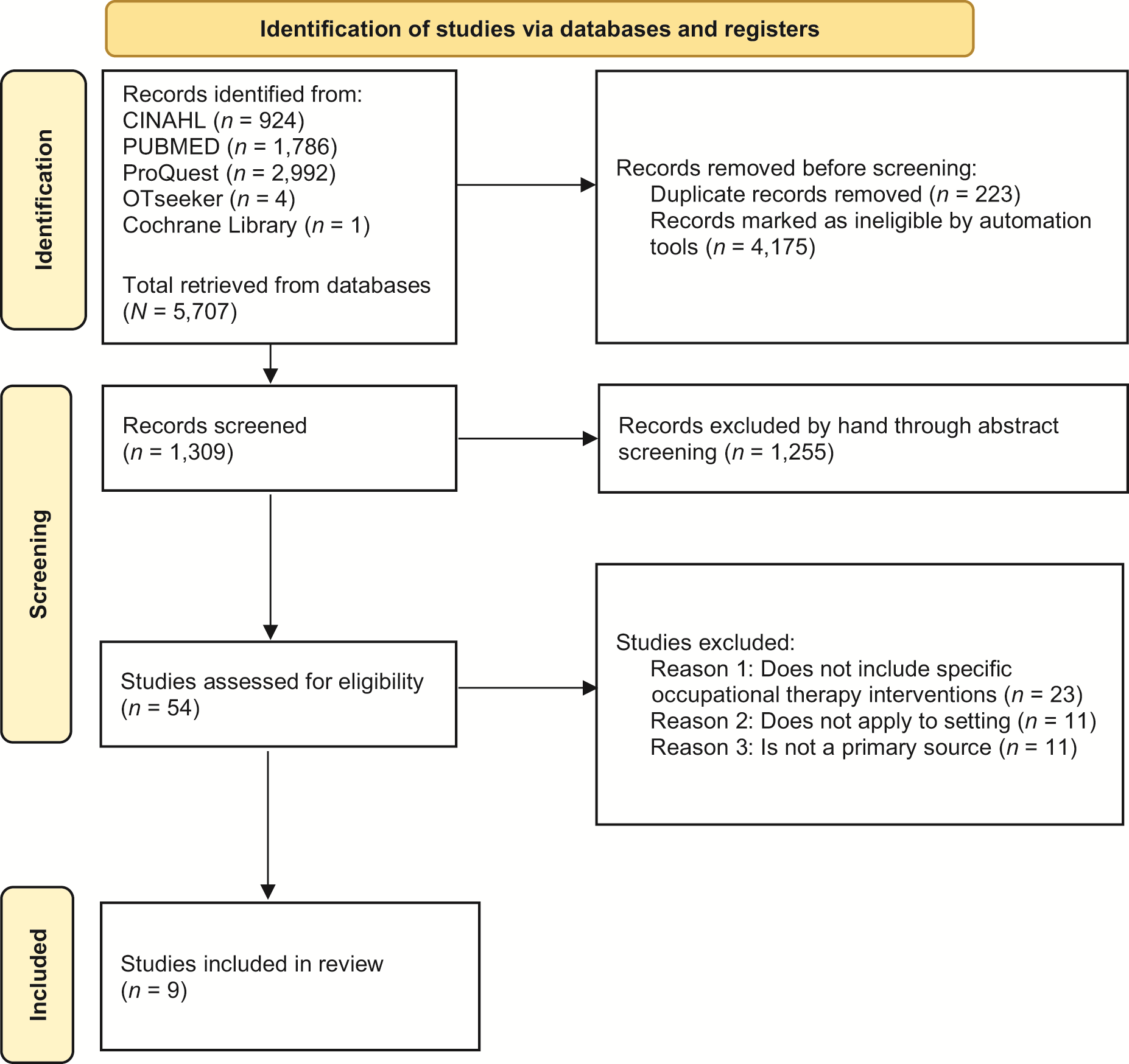
Flow of studies through the systematic review.
Risk of Bias
Risk-of-bias analyses found 5 low, 4 moderate, and no high risk-of-bias studies. See Table A.3 for Cochrane risk-of-bias analyses for controlled studies and Table A.4 for risk-of-bias analyses based on National Heart, Lung and Blood Institute guidelines for noncontrolled studies.
Populations
The 9 studies included a variety of ICU populations. Three studies focused on mechanically ventilated patients (Dinglas et al., 2013; Hsu et al., 2020; Sigler et al., 2016), 1 studied nonventilated patients (Álvarez et al., 2017), and 1 studied patients with acute respiratory distress syndrome (Jolley et al., 2017). Three studied neurological patients (Malcolm et al., 2021; Olkowski et al., 2013), with 1 specifically focusing on patients with EVDs (external ventricular drains; Moyer et al., 2017). Finally, 1 studied patients in a trauma ICU (Falkenstein et al., 2020).
Interventions
The 9 studies were examined for specific occupational therapy early engagement interventions and their targeted outcomes. Six studies included ADL interventions (Álvarez et al., 2017; Dinglas et al., 2013; Hsu et al., 2020; Malcolm et al., 2021; Moyer et al., 2017; Olkowski et al., 2013). Multiple studies explored cognitive activities, including games (Álvarez et al., 2017), writing (Hsu et al., 2020), polysensory stimulation (Álvarez et al., 2017; Malcolm et al., 2021), and problem-solving (Álvarez et al., 2017). Therapeutic exercise was used in 5 of the studies (Álvarez et al., 2017; Dinglas et al., 2013; Hsu et al., 2020; Malcolm et al., 2021; Olkowski et al., 2013). Physical rehabilitation was addressed in all 9 studies, with 5 specifically discussing early mobility interventions (Falkenstein et al., 2020; Jolley et al., 2017; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016).
Outcomes
ADL outcomes included the FIM® (Álvarez et al., 2017), Activity Measure for Post-Acute Care (Falkenstein et al., 2020), Barthel Index (Olkowski et al., 2013), and Modified Rankin Scale (Olkowski et al., 2013). Therapeutic exercise was assessed using a dynamometer to determine grip strength (Álvarez et al., 2017) and in-bed mobility activity (Jolley et al., 2017). Early mobility was assessed using mobility milestones (Falkenstein et al., 2020), out-of-bed tasks (Hsu et al., 2020; Jolley et al., 2017; Olkowski et al., 2013), time to out-of-bed activity (Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016), and mean ambulation distance (Sigler et al., 2016). Outcome measures used to assess cognition included the Mini-Mental State Examination (Álvarez et al., 2017), delirium (duration, incidence, and severity; Álvarez et al., 2017), Confusion Assessment Method for Intensive Care Unit (Álvarez et al., 2017; Dinglas et al., 2013; Hsu et al., 2020), Glasgow Coma Scale (Malcolm et al., 2021), and surveys of patients’ recall of their therapy participation (Hsu et al., 2020). The included studies also explored various medical outcomes, including severity of illness (Dinglas et al., 2013), mechanical ventilation use (Dinglas et al., 2013; Falkenstein et al., 2020; Hsu et al., 2020; Moyer et al., 2017), 30-day mortality rate (Olkowski et al., 2013), and sedation use (Sigler et al., 2016).
Descriptive Summaries
Analysis of interventions and outcomes revealed three categories of occupational therapy interventions in the ICU pertaining to early engagement: ADLs, physical rehabilitation, and cognition. Although the studies in this review also explored medical-based outcomes, these outcomes were not directly tied to early engagement or occupational therapy interventions and were therefore not included in the descriptive summaries.
ADLs
Four Level 2b studies (Álvarez et al., 2017; Dinglas et al., 2013; Malcolm et al., 2021; Moyer et al., 2017) and 2 Level 3b studies (Hsu et al., 2020; Olkowski et al., 2013) examined early engagement interventions related to ADLs for patients in the ICU. Some of these studies identified specific ADLs, including grooming (Álvarez et al., 2017; Hsu et al., 2020), eating (Álvarez et al., 2017), and commode transfers (Hsu et al., 2020; Olkowski et al., 2013). Depending on the patients’ medical and functional statuses, ADL interventions were conducted while patients were in bed (Álvarez et al., 2017), sitting at the edge of the bed (Hsu et al., 2020; Olkowski et al., 2013), or standing or sitting in a chair (Hsu et al., 2020; Olkowski et al., 2013). Other studies mentioned ADL retraining or engaging patients in ADLs, although they did not identify specific ADL or self-care interventions (Dinglas et al., 2013; Malcolm et al., 2021; Moyer et al., 2017).
Each of these 6 studies used ADL retraining in combination with other early engagement interventions, including early mobilization (Moyer et al., 2017; Olkowski et al., 2013), exercise (Álvarez et al., 2017; Dinglas et al., 2013; Hsu et al., 2020), and cognitive stimulation (Álvarez et al., 2017; Hsu et al., 2020; Malcolm et al., 2021). Although none of the included studies examined the effects of ADL interventions alone, Álvarez et al. (2017) found that, compared with the control group, patients in the occupational therapy intervention group who received ADL retraining, positioning, therapeutic exercise, and cognitive stimulation had statistically significant increases in functional independence at hospital discharge as measured with the FIM. On the basis of 4 Level 2b studies with support from 2 Level 3b studies, moderate strength of evidence exists for ADL interventions in the ICU.
Physical Rehabilitation
All 9 studies in this review—6 Level 2b (Álvarez et al., 2017; Dinglas et al., 2013; Falkenstein et al., 2020; Jolley et al., 2017; Malcolm et al., 2021; Moyer et al., 2017) and 3 Level 3b (Hsu et al., 2020; Olkowski et al., 2013; Sigler et al., 2016)—included occupational therapy interventions focused on various aspects of physical rehabilitation with early engagement. These interventions are divided into two subcategories: therapeutic exercise (foundational movements such as range of motion and strengthening) and early progressive mobilization (sequential, graded mobility activities from bed mobility to transfers and walking). Of the 9 studies, 5 combined occupational and physical therapy interventions when discussing physical rehabilitation without distinguishing between them (Falkenstein et al., 2020; Jolley et al., 2017; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016), whereas the remaining 4 studies focused solely on occupational therapy interventions (Álvarez et al., 2017; Dinglas et al., 2013; Hsu et al., 2020; Malcolm et al., 2021).
Therapeutic exercise.
Of the 9 studies addressing physical rehabilitation, 3 Level 2b (Álvarez et al., 2017; Dinglas et al., 2013; Malcolm et al., 2021) and 3 Level 3b studies (Hsu et al., 2020; Olkowski et al., 2013; Sigler et al., 2016) discussed therapeutic exercise interventions for patients in the ICU. Several studies mentioned bed-level passive or active range-of-motion exercises for upper and lower extremities for patients not yet able to participate in edge-of-bed or out-of-bed activities because of their medical status or decreased alertness (Dinglas et al., 2013; Hsu et al., 2020; Malcolm et al., 2021; Olkowski et al., 2013). In addition to range of motion, 3 studies also incorporated strengthening exercises for the upper and lower extremities to optimize functionality and prevent muscle atrophy (Álvarez et al., 2017; Dinglas et al., 2013; Sigler et al., 2016). In 2 of these studies, strengthening exercises were led by either occupational or physical therapists (Álvarez et al., 2017; Dinglas et al., 2013), whereas the study by Sigler et al. (2016) described strengthening exercises performed primarily by family members after receiving an exercise program from an occupational or physical therapist.
Early progressive mobilization.
Five studies—3 Level 2b (Falkenstein et al., 2020; Jolley et al., 2017; Moyer et al., 2017) and 2 Level 3b (Olkowski et al., 2013; Sigler et al., 2016)—included early progressive mobilization programs that use graded interventions to target patients’ overall mobility and physical activity participation while in the ICU. In these studies, occupational and physical therapists started with bed-level activity, including active or passive in-bed cycling (Falkenstein et al., 2020), raising the head of the bed or facilitating an in-bed cardiac chair position (Olkowski et al., 2013; Sigler et al., 2016), and bed mobility (Olkowski et al., 2013). The studies then described occupational and physical therapists progressing patients to sitting on the edge of the bed to address postural correction, balance, or ADL training (Jolley et al., 2017; Moyer et al., 2017; Olkowski et al., 2013), followed by standing, marching in place, transferring to a chair, and walking (Falkenstein et al., 2020; Jolley et al., 2017; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016).
Progressive mobilization programs in all 5 studies were developed by multidisciplinary teams involving occupational and physical therapists as well as nurses, respiratory therapists, intensivists, and surgeons (Falkenstein et al., 2020; Jolley et al., 2017; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016). Two studies examining the effects of early progressive mobilization programs found statistically significant decreases in length of time to patients’ first mobilization (Moyer et al., 2017) and statistically significant increases in progression to out-of-bed mobility for both mechanically and nonmechanically ventilated patients (Jolley et al., 2017). The other 3 studies found that early progressive mobilization programs were safe and feasible for patients in the ICU (Falkenstein et al., 2020; Olkowski et al., 2013; Sigler et al., 2016). On the basis of 6 Level 2b studies and consistent findings across all 9 studies, moderate strength of evidence exists for physical rehabilitation interventions in the ICU.
Cognition
Three studies—2 Level 2b (Álvarez et al., 2017; Malcolm et al., 2021) and 1 Level 3b (Hsu et al., 2020)—included cognition-based early engagement interventions for patients in the ICU. Specific cognition-based interventions included memory exercises (Álvarez et al., 2017; Hsu et al., 2020); sequencing cards and visuospatial construction games (Álvarez et al., 2017); and reading, writing, and filling out a calendar (Hsu et al., 2020). These interventions targeted various cognitive functions, including memory, problem-solving, and alertness (Álvarez et al., 2017). Although Malcolm et al. (2021) did not list specific cognitive interventions, they found that patients in a neurological ICU were 6 times more likely to receive functional–cognitive interventions because this was the category most billed by occupational therapy practitioners, at 45.1%.
In all 3 studies, cognitive interventions were often used along with other interventions, including ADL retraining and physical rehabilitation (Álvarez et al., 2017; Hsu et al., 2020; Malcolm et al., 2021). The study by Álvarez et al. (2017) found that early and intensive occupational therapy interventions targeting ADLs, cognitive tasks, and exercise were correlated with significantly lower incidence and fewer hours of delirium compared with a control group. More specifically, engagement in occupational therapy interventions twice daily was associated with statistical improvement in functional cognition as measured by the five cognitive FIM items (Álvarez et al., 2017). A moderate level of evidence supports cognitive-based interventions, considering statistically significant findings of the Level 2b and 3b studies.
Discussion
Early engagement is a term that holistically captures how occupational therapy practitioners use interventions to optimize function, coping, and quality of life for patients recovering in the ICU. Although the literature often highlights early mobilization, this is only one aspect of occupational therapy’s scope of practice and does not include other areas, such as ADL retraining, cognition, psychosocial coping, and occupational participation, that can affect patients’ recovery from critical illness. This systematic review sought to explore occupational therapy–specific interventions for patients in the ICU related to early engagement—including, and expanding on, early mobilization. Extensive review of the current literature revealed 9 studies including specific occupational therapy ICU interventions that demonstrated moderate strength of evidence across three categories: ADL retraining, physical rehabilitation, and cognition. However, no two studies were congruent in interventions, procedures, or outcomes, revealing difficulties in data comparison and extrapolation and a need for further research across all aspects of occupational therapy services in the ICU setting.
Because much of the existing literature on ICU rehabilitation focuses on early mobilization, it is unsurprising that all 9 studies in this review included physical rehabilitation interventions, such as therapeutic exercise and progressive mobilization programs (Álvarez et al., 2017; Dinglas et al., 2013; Falkenstein et al., 2020; Hsu et al., 2020; Jolley et al., 2017; Malcolm et al., 2021; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016). Patients with critical illness are at risk for ICU-acquired weakness, which is correlated with increased hospital length of stay and decreased physical function in both the short and the long term (Desai et al., 2011; Needham, 2008; Vanhorebeek et al., 2020). Therefore, it is critical for occupational therapy practitioners to use early engagement interventions that incorporate physical activity, such as range of motion, exercise, and progressive mobilization, because these have been shown to be associated with decreased hospital length of stay and improved functional outcomes (Falkenstein et al., 2020; S. D. Higgins et al., 2019; Moyer et al., 2017; Parker et al., 2013; Sigler et al., 2016).
Although physical rehabilitation is important for patients in the ICU, 6 of the 9 studies included in this review also discussed ADL participation as part of early engagement (Álvarez et al., 2017; Dinglas et al., 2013; Hsu et al., 2020; Malcolm et al., 2021; Moyer et al., 2017; Olkowski et al., 2013). Although none of the studies specifically isolated ADL outcomes or captured pre- and postintervention scores, ADL tasks were performed in conjunction with other interventions, for example, grooming while sitting on the edge of the bed (Hsu et al., 2020; Moyer et al., 2017), practicing chair and commode transfers as part of progressive mobilization (Hsu et al., 2020; Olkowski et al., 2013), and ADL retraining with cognitive stimulation activities (Álvarez et al., 2017). Addressing ADL participation in the ICU is essential because nearly all ICU patients experience decreased ADL participation and diminished quality of life after discharge from the ICU (Desai et al., 2011; Vest et al., 2011). Further research is needed to quantify the effect of early engagement in ADL interventions as well as their impact on the functional performance of ICU survivors.
Cognitive interventions were also included in early engagement and should be considered by occupational therapy practitioners working with patients in the ICU. Girard et al. (2010) found that nearly 80% of patients were cognitively impaired at the 3-mo follow-up after their ICU stay, indicating the importance of addressing functional cognition early in hospitalizations. Three studies included in this review described the use of cognitive interventions as part of early engagement (Álvarez et al., 2017; Hsu et al., 2020; Malcolm et al., 2021). Including cognitive-based interventions as part of early engagement for patients in the ICU is valuable because these interventions can affect patients’ ability to safely complete ADLs, self-manage medications, participate in social interactions, and navigate the community after discharge (Arrebola-Moreno et al., 2020; Chivukula et al., 2017; Everson-Rose & Lewis, 2005). More research is needed to examine the effectiveness of cognitive interventions and their impact on early engagement.
Interestingly, although results from this review highlight the importance of participation in ADLs, physical rehabilitation, and cognitive interventions in early engagement, these interventions do not directly address psychosocial coping or delirium. Patients in the ICU often experience high levels of depression, anxiety, and stress that affect their quality of life and mental health both during their hospital admission and for months or years afterward (Saeidi et al., 2021). Sleep disturbances and pain are also stressful experiences and can affect recovery, coping, and participation in meaningful activities (Matthews, 2011; Park & Kim, 2014). These challenges often contribute to ICU-acquired delirium, which occurs among 20% to 35% of patients and is associated with poor health outcomes and higher mortality rates (Cavallazzi et al., 2012; Collinsworth et al., 2016; Poulsen et al., 2021). Although Álvarez et al. (2017) found that patients who received occupational therapy cognitive interventions had lower incidence and fewer hours of delirium, these interventions were provided along with ADL retraining and therapeutic exercise, making it difficult to discern which interventions directly affected delirium. Further research is needed to examine interventions related to psychosocial coping and delirium management while also exploring other potential areas of early engagement that fall within occupational therapy’s scope of practice, including sleep, stress, and pain management (AOTA, 2020).
Providing occupational therapy services in the ICU is complex and challenging, given the medical acuity of patients and numerous lines and devices. Several of the studies in this review found that occupational therapy interventions in the ICU, whether engaging patients in ADL retraining, physical rehabilitation, or cognitive tasks, were performed safely across patient populations with minimal adverse events (Dinglas et al., 2013; Falkenstein et al., 2020; Hsu et al., 2020; Jolley et al., 2017; Malcolm et al., 2021; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016). More important, these interventions were often conducted in collaboration with other members of a multidisciplinary team, including physical therapists, nurses, respiratory therapists, and physicians (Álvarez et al., 2017; Falkenstein et al., 2020; Hsu et al., 2020; Jolley et al., 2017; Moyer et al., 2017; Olkowski et al., 2013; Sigler et al., 2016). Although evidence exists to support occupational therapy practitioners as valued members of multidisciplinary teams, it is imperative to continue exploring occupational therapy’s unique role in early engagement and in holistically addressing the complex needs of patients with critical illness.
Limitations
This review was limited by the small number of studies meeting the inclusion criteria and the lack of Level 1a studies. Studies were included only if they were published in English and specified occupational therapy interventions. This may have excluded studies that could have added to the strength of evidence and measurable outcomes. Four of the studies had moderate risk of bias, possibly because of extraneous patient factors, difficulty with personnel blinding, and challenges of creating randomized controlled trials in the ICU because patients cannot be excluded from routine care. Additionally, because of human error, appropriate articles for inclusion may have been excluded, and the risk of publication bias exists.
Future Considerations
Of the 9 studies included in this systematic review, only 3 had occupational therapy authors (Álvarez et al., 2017; Malcolm et al., 2021; Moyer et al., 2017). 1 study did not disclose credentials (Hsu et al., 2020). Additionally, the studies emphasized early mobilization and included only vague descriptions of ADL performance, with little focus on other factors, such as environmental barriers and sensory stimulation. Clinicians and patients may benefit from future research examining the effectiveness of occupational therapy in the ICU through high-quality studies using relevant outcome measures. Additional research should explore other forms of early engagement, including, but not limited to, environmental, psychosocial, and occupational interventions and their influences on quality of life, self-management, coping, and sleep. Although studies exploring occupational therapy’s role with patients on mechanical ventilation and with neurological conditions exist, future research opportunities include patients with cardiothoracic, organ transplant, genitourinary, gastrointestinal, and multiorgan failure diagnoses.
Implications for Occupational Therapy Practice
Occupational therapy practitioners are suited to promoting early engagement for patients in the ICU by facilitating ADL retraining, physical rehabilitation, and cognitive reasoning to improve function and self-efficacy. Occupational therapy practitioners have a unique opportunity to address numerous patient factors affecting recovery and healing for critically ill patients through evidence-based interventions. This review has the following implications for occupational therapy practice: ▪ Occupational therapy practitioners should use ADL participation, physical rehabilitation, and cognitive tasks to promote early engagement of patients in the ICU. ▪ Practitioners should consider additional areas of early engagement, such as psychosocial coping and delirium. ▪ Practitioners should grade and progress early engagement interventions on the basis of patients’ medical and functional statuses. ▪ The use of outcome measures to demonstrate the effectiveness of early engagement interventions should be increased.
Conclusion
Many patients who are admitted to the ICU face complex challenges that affect their function, coping, and quality of life. The 9 studies included in this systematic review demonstrate moderate support for occupational therapy interventions that encourage early engagement in the ICU related to ADL retraining, physical rehabilitation, and cognition. This review supports use of the term early engagement, with corroborating evidence of treatment approaches targeting functional performance, ICU-acquired weakness, and cognitive changes. There is a need for increased occupational therapy presence in ICUs to promote early engagement and better support the individualized needs of patients throughout their recovery course.
Supplemental Material
Supplementary material for Occupational Therapy Interventions and Early Engagement for Patients in Intensive Care: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050695.pdf for Occupational Therapy Interventions and Early Engagement for Patients in Intensive Care: A Systematic Review by Morgan Smith, Stephanie Tsai and Elyse Peterson in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors have no funding sources or conflicts of interest to disclose.
*Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.