
Abstract
This study highlights significant gaps faced by health care professionals in understanding and addressing challenges in toileting evaluation and intervention for children with cerebral palsy.
Toileting, an integral aspect of activities of daily living (ADLs), holds paramount significance in the occupational therapy profession (Rojas et al., 2020). It encompasses obtaining and using toileting supplies; managing clothing; maintaining toileting positions; transferring to and from these positions; cleaning the body; addressing menstrual needs; and attending to control needs, including catheters, colostomy, and administration of suppositories, as well as voluntary control of bowel movements and voiding and, if necessary, the use of devices or agents for bladder control (American Occupational Therapy Association [AOTA], 2020).
Toileting is a complex, private, multitasking activity that involves diverse functions, from motor skills to perceptual–cognitive, sensory, communicative, and psychological aspects (Burns & Matson, 2017; Sato et al., 2016). For instance, motor functions are involved in various aspects of toileting, such as reaching the toilet, donning and doffing clothing, assuming a comfortable sitting position on the toilet, maintaining balance and stability for several minutes, and participating in posttoileting hygiene practices. Individuals with intellectual disabilities may struggle with toileting skills, and psychological disorders such as toilet refusal syndrome can disrupt control over bodily functions. Sensory factors and pain influence urine and stool expulsion, and communication aids in signaling needs during toileting. The digestive system’s functionality affects stool elimination, and factors such as diet and medication affect outcomes. Urinary functions, including bladder evacuation, are intricate and may be disrupted by conditions such as neurogenic bladder (Beaudry-Bellefeuille et al., 2019; Murphy et al., 2012; Ruffini et al., 2022). Executing toileting activities is influenced by multiple factors, including physiological aspects, personal considerations (musculoskeletal, neurological, cardiovascular, sensory, cognitive–perceptual), environmental elements (toilet environment, toilet type, and sanitation equipment), and cultural or religious factors (Chu et al., 2020; Edemekong et al., 2023; Fong & Feng, 2021; Wicandra et al., 2018). These complexities emphasize the need for comprehensive evaluation and tailored therapeutic interventions.
Cerebral palsy (CP), a prevalent motor and postural developmental disability, presents enduring challenges throughout an individual’s life. The global prevalence of CP is approximately 2 per 1,000 live births, with recent data from Europe suggesting a slightly lower rate of 1.64 per 1,000 live births (Perra et al., 2021; Stavsky et al., 2017). CP results in disruptions to the stomach, lower intestine, and bladder systems, leading to toileting difficulties. These disruptions are primarily caused by central nervous system damage and associated issues, such as movement restriction and immobility. Consequently, individuals with CP commonly experience problems such as constipation and neurogenic bladder (Corcos & Przydacz, 2018; Teeple et al., 2019; Veugelers et al., 2010). Simultaneously, other disorders in movement, sensation, perception, cognition, communication, and behavior further compound challenges in toileting for children with CP (Baram et al., 2023; Murphy et al., 2012).
The repercussions of toileting difficulties extend beyond the physical realm, affecting psychosocial, spiritual, cultural, and even sexual and marital dimensions of health care. Socially, children facing toileting challenges may experience embarrassment and communication difficulties. Bladder and bowel dysfunctions can create strain in relationships by leading to intimacy issues, altering family dynamics, and causing inconsistent social interactions because of frustration and a lack of understanding by peers (Braaf et al., 2017; Mei et al., 2015; Sebesta & Reynolds, 2024). As a result, these factors significantly limit the participation of children with CP in social, academic, and other occupational activities (Marciniak et al., 2015; Wiegerink et al., 2011; Yıldız et al., 2017).
Despite these profound implications, toileting issues in the context of CP are often overlooked by medical professionals, rehabilitation specialists, clients, and caregivers alike (Millard et al., 2013). This neglect manifests in fewer evaluations and interventions for toileting-related challenges compared with other ADLs (Wang & Palmer, 2011; Yachnin et al., 2018).
Given that the performance of ADLs, including toileting, serves as an indicator of a client’s functional status and routine (Edemekong et al., 2023), it is imperative to address the existing gaps in attending to challenges associated with the evaluation of and intervention with all aspects of toileting function, based on the Occupational Therapy Framework: Domain and Process (4th ed.; AOTA, 2020). The primary objectives of this study were to identify the challenges encountered by professionals in the evaluation of and intervention with toileting for children with CP, to refine and achieve consensus on these challenges, and to uncover additional challenges through a mixed-methods investigation.
Method
Study Design
We used an exploratory sequential mixed-methods design involving two main phases to investigate challenges related to toileting evaluation and interventions with children with CP. We chose a mixed-methods approach to comprehensively address the research question because it allows for the integration of qualitative and quantitative data, thus providing a more complete understanding of the challenges (Bowen et al., 2017). The first phase focused on preparing a Delphi questionnaire through a literature review and a qualitative process involving focus groups, semistructured interviews, and an expert panel to gather in-depth insights and identify specific challenges. Feedback from these activities helped us to refine the questionnaire (Polit-O’Hara & Yang, 2016). The second phase was the Delphi study, which combined qualitative and quantitative approaches to refine and achieve consensus on the challenges identified and also to discover any other challenges through iterative survey rounds among experienced professionals. These two phases are shown in Figure 1.
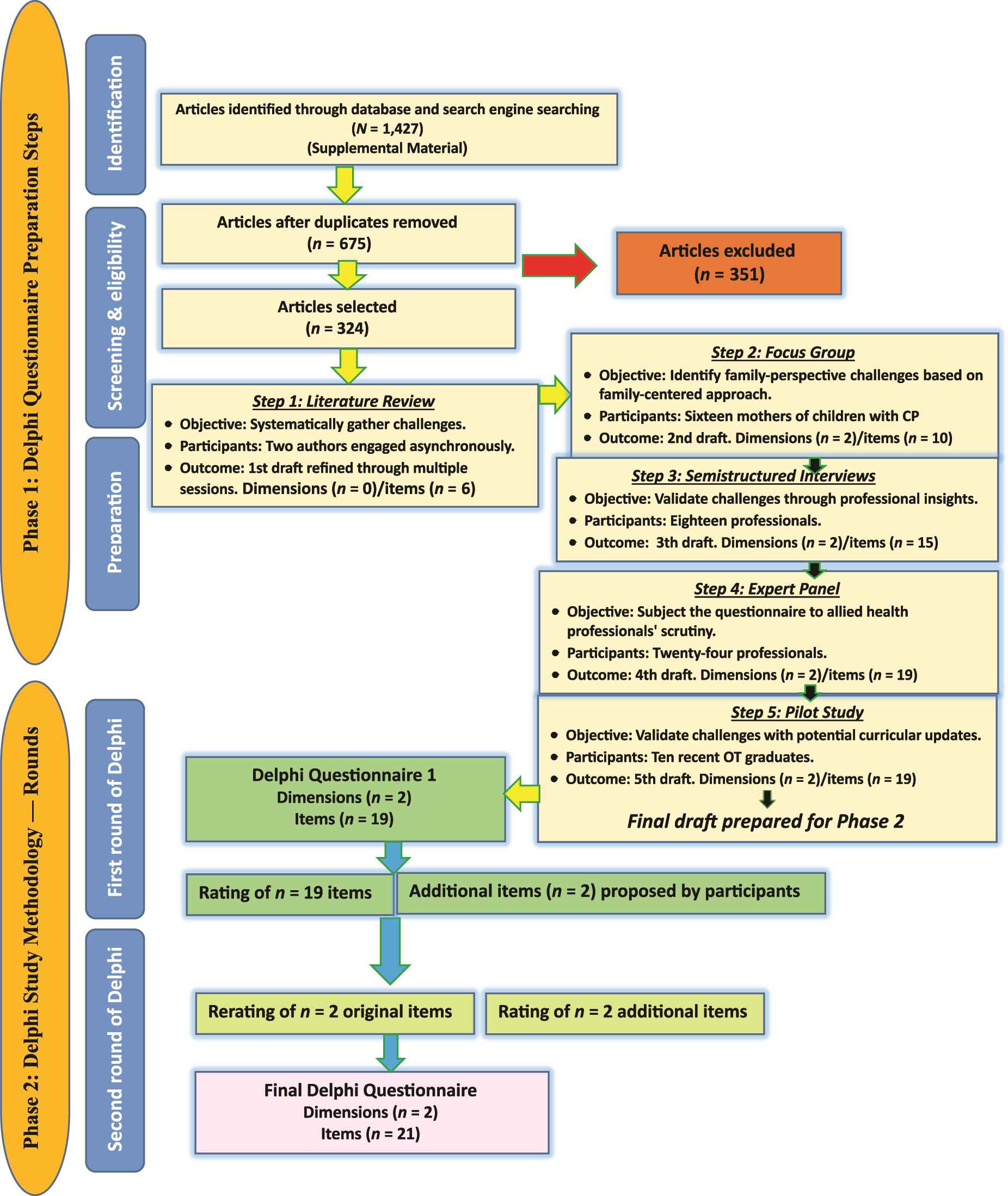
Flowchart of the Delphi questionnaire drafting process and survey rounds.
Phase 1: Delphi Questionnaire Preparation—National Phase
In this phase, we conducted a systematic database search to identify relevant articles and then followed five steps to develop a questionnaire for Phase 2 (see the search strategy in the Supplemental Material, available online with this article at https://research.aota.org/ajot). Each step is outlined in the flowchart presented in Figure 1. Participants were selected on the basis of inclusion criteria that required a minimum of 5 yr of experience working with children diagnosed with CP. Participant feedback was solicited at each step, with encouragement to identify additional challenges related to toileting evaluation and intervention. This iterative process allowed for the incorporation of new challenges into the evolving list of subsequent steps. Demographic details for the participants involved in Phase 1 are provided in Table 1.
Demographic Characteristics of Participants in Questionnaire Preparation: National Phase
Note. CP = cerebral palsy; S = specialist; SS = subspecialist.
The involvement of mothers of children with CP was integral to our family-centered approach, aimed at capturing their unique perspectives on toileting evaluation and interventions. This approach ensured that both the practical and the emotional aspects of toileting were considered from the caregiver’s viewpoint. Insights from mothers were gathered through focus groups, which were conducted using a convenience nonprobability sampling method. During these sessions, mothers actively discussed their children’s toileting challenges, identifying them and providing critical feedback. Their contributions directly influenced the development of the questionnaire, with items being retained, modified, or newly created on the basis of the consensus reached during these discussions. The significant agreement (more than 75%) among participants provided confidence that their input was effectively integrated into the final questionnaire. This ensured that the final version addressed real-world challenges from a family-centered perspective, reflecting the caregivers’ lived experiences.
Phase 2: Delphi Methodology—National and International Phase
The Delphi methodology, widely recognized in health care as a means to obtain consensus on clinical matters (Vernon, 2009), was used to agree on challenges faced in toileting evaluation and interventions for children with CP. This phase of the study consisted of two rounds, engaged national and international professionals, and was guided by Conducting and REporting DElphi Studies guidelines (Jünger et al., 2017).
Participants
Professionals from diverse CP and toileting fields were included. Criteria included educational or clinical experience in CP, experience in the toileting field, or contributions to the CP or toileting literature. Professionals were identified through academic profiles, articles, affiliations, and networks such as Research Gate and LinkedIn.
Delphi Methodology
First Round
The Delphi process involved electronically transmitting the final draft of the 19-item Phase 1 questionnaire to 162 participants. Participants were asked to anonymously rate their agreement with each item on a 5-point Likert scale, on which 5 = strongly agree, 4 = agree, 3 = don’t know, 2 = disagree, and 1 = strongly disagree. With reminders, this round garnered responses from 138 national and 24 international participants (van Balen et al., 2019; see Appendix A in the Supplemental Material).
Data Analysis and Consensus Criteria
Items with 75% or higher agreement and rated a median of 3.75 or above in the first round were included. New challenges were reviewed and incorporated into the second round. Items with 50% to 75% agreement, a median rating of 2.50 to 3.75, or both were carried to the second round. Items with less than 50% agreement or a median rating below 2.5 were excluded (Barrett & Heale, 2020; van Balen et al., 2019).
Second Round
In this round, 131 participants were presented with a new draft of the questionnaire, including items from the first round that did not meet the criteria. Participants provided their opinions, and additional challenges suggested by professionals were included. After receiving 114 national and 17 international responses, the second round was concluded (Figure 1).
Disagreements among participants were addressed using the standard Delphi approach, wherein items that did not achieve consensus were revised on the basis of feedback and reintroduced in the subsequent round. During the questionnaire preparation phase, any items that received more than 75% agreement from participants were integrated into the following steps of the process. Challenges identified through discussions were carefully reviewed by the research team. If deemed relevant, they were incorporated into the draft questionnaire. The research team then evaluated these proposed additions in the context of the study’s objectives and existing literature. Only those challenges that met the consensus threshold were included in the final version of the questionnaire. No challenges were excluded from the final draft because of the high level of agreement achieved during the validation process. This iterative method ensured that the final questionnaire comprehensively reflected the full spectrum of challenges identified in the literature and validated through participant feedback. This approach guaranteed thorough validation and inclusion of all relevant challenges identified in the literature review (see Appendix B in the Supplemental Material).
Results
Professionals from 17 countries participated in this Delphi study. Initially, 162 professionals provided insights, and 131 completed the second round. Attrition in the second round can be attributed to several factors. Some participants may have faced time constraints or increased workload, which made it difficult for them to continue their involvement. Additionally, the follow-up process and the detailed nature of the second-round tasks could have contributed to the dropout. These factors combined likely led to a reduction in the number of professionals participating in the second round. Participant details are available in Table 2.
Demographic Characteristics of Delphi Participants
Note. CP = cerebral palsy; S = specialist; SS = subspecialist.
Participants were from the following countries: Iran (n = 138), Canada (n = 4), United States (n = 4), Norway (n = 2), Turkey (n = 2), Australia (n = 1), Azerbaijan (n = 1), Brazil (n = 1), England (n = 1), Ghana (n = 1), Kuwait (n = 1), Qatar (n = 1), Spain (n = 1), Sweden (n = 1), Switzerland (n = 1), Taiwan (n = 1), United Arab Emirates (n = 1).
Participants were from the following countries: Iran (n = 114), Canada (n = 3), United States (n = 3), Norway (n = 2), Turkey (n = 2), Australia (n = 1), Brazil (n = 1), England (n = 1), Qatar (n = 1), Spain (n = 1), Switzerland (n = 1), United Arab Emirates (n = 1).
In the first round, consensus was reached on 17 items, indicating challenges in toileting evaluation or interventions. Values for these items were above 75%, with a median rating of between 4 and 5. Two items had a consensus level of 50% to 75% with a median rating of 4. Two items not reaching consensus in the first round were entered into the second round after modification. During the revision process, each item was carefully evaluated and modified on the basis of participant feedback to ensure clarity, relevance, and comprehensiveness. For example, the original item “Insufficient scientific evidence and literature on toileting compared to other functional areas” was revised to “Limited resources, such as books and evidence-based articles, in the toileting function domain compared to other functional areas like sensory–motor and perceptual–cognitive.” This change was made to more accurately reflect the specific resources that were lacking and to draw a clearer comparison with other well-researched areas. Another example involved the item “Reluctance among specialists, therapists, parents, and individuals with CP to address toileting questions due to cultural taboos and resulting embarrassment.” This was revised to “Treatment team hesitancy to address issues related to bladder and bowel control, toileting performance, and menstruation, including concerns about potential embarrassment and shame among individuals with CP and their parents due to cultural taboos.” The revision was intended to broaden the scope of the issue and explicitly include related concerns, such as menstruation.
At the end of the first round, participants added two new items: challenges in providing education on toileting evaluation and interventions, which highlighted the absence of appropriate assessment environments, simulated scenarios, and sanitation facilities, and ambiguity in identifying members of the toileting management team. By the end of the second round, no further items were added, indicating that the revisions had addressed the concerns. The final list of challenges was comprehensive, with all items receiving approval from more than 75% of participants and a median rating of 4 or 5 (Table 3). This iterative refinement process ensured that the final questionnaire effectively captured all relevant challenges, with each item thoroughly vetted and validated by the participants.
Delphi Consensus Process Results: Challenges in Evaluation and Intervention of Toileting Performance
Note. CP = cerebral palsy.
Agreement: strongly agree percentile + agree percentile.
In this study, 159 individuals were surveyed regarding concerns related to toileting issues (3 individuals were excluded because they reported no concerns about toileting). These participants included clinical practitioners and faculty members with educational backgrounds, all of whom possessed clinical experience. The demographic question included a question with five response options that allowed participants to self-report their commitment level. Commitment levels varied among rehabilitation professionals, with 10.57% reporting very high commitment, 21.14% reporting high commitment, 38.21% reporting medium commitment, 26.02% reporting limited commitment, and 4.06% reporting disregarded commitment. Similarly, commitment levels varied among medical professionals, with 17.95% reporting very high commitment, 20.51% reporting high commitment, 46.15% reporting medium commitment, 12.82% reporting limited commitment, and 2.56% reporting that they didn’t attend. Further details can be found in Figure A.1 in the Supplemental Material.
Discussion
Toileting is one of the most important ADLs. When challenges arise in its implementation, they not only diminish an individual’s independence and quality of life but also impose significant psychological, social, and economic burdens on the individual, their family, and society at large. Despite its importance, the existing literature indicates that toileting has been less studied compared with other ADLs. To address this gap, our study is the first to comprehensively explore specific challenges in the evaluation of and intervention with toileting for children with CP. The study examined these challenges across three dimensions: academic challenges, clinical challenges, and their intersection, all focused on the investigation of toileting performance.
Academic Challenges
This study emphasizes a critical academic challenge: insufficient training for toileting issues, particularly in evaluating and implementing therapeutic interventions for children with CP. It underscores the need for meticulous education of the toileting management team in medicine and rehabilitation.
In terms of disciplinary training disparities, a notable academic divide exists, with medical training focusing on certain functions, such as urological, nephrological, neurological, and nutritional aspects and rehabilitation training concentrating on sensory–motor, cognitive, psychological, and communication functions. The multifaceted nature of toileting necessitates a more nuanced approach that is often overlooked in current training paradigms.
Neglect of toileting-specific therapies in current academic approaches leans toward a bottom-up orientation, emphasizing body structures and functions. This neglect hampers the occupation-based perspective crucial for addressing toileting intricacies, contributing to deficiencies in functional aspects in medical and rehabilitation education. To address these deficiencies, it is essential to incorporate treatments that place greater emphasis on functional aspects and occupation-based interventions specifically in the area of toileting.
The current study identified significant deficiencies in educational curricula, particularly the insufficient emphasis on toileting-related education. Although medical curricula extensively cover bowel, bladder, and digestive issues, discussions in rehabilitation fields predominantly focus on pelvic floor muscle rehabilitation and control. In a similar vein, occupational therapy curricula tend to address broader ADLs but fall short in providing specific and comprehensive training in the functional aspects of toileting. This gap underscores the urgent need to enhance the educational content of entry-level occupational therapy programs to better prepare professionals to effectively address toileting challenges.
In concordance with earlier studies, this study underscores the persistent issue of insufficient toileting training in medical and rehabilitation education (Millard et al., 2013). Notably, the identification of disciplinary training disparities is consistent with the work of Wu et al. (2019), emphasizing the need for a more nuanced approach to address the multifaceted nature of toileting (Wu et al., 2019). To address these gaps, it is recommended that policies and educational curricula be updated to include comprehensive toileting education.
Clinical Challenges
Clinical challenges in toileting management manifest in imbalanced prioritization, heavily emphasizing sensory–motor, cognitive–perceptual, and psychological functions in clinical settings. Time constraints further compound this issue, resulting in deferred attention to toileting. Adopting a client-centered approach reveals challenges such as insufficient time allocation for toileting and delayed consideration by the treatment team and parents. Participants argued that this stems from systemic oversight, exacerbated by prioritizing goals such as walking and school activities in line with a client-centered approach.
Adding to the complexities, inadequate family training exacerbates challenges in promoting independence, despite parental requests (Gronski, 2021). The prospect of expanded insurance coverage for medical services, including toileting-related ones, holds promise for increased accessibility. However, a significant challenge arises from the absence of a specific code for toileting in the Current Procedural Terminology (CPT ®) relative values booklet, as voiced by 76.5% of professionals. This underscores the need for a distinct code in the CPT framework to ensure comprehensive coverage and improved accessibility.
A significant challenge lies in the absence of explicit mention of toileting considerations in routine medical and rehabilitation intervention forms. For goals to be set effectively, the processes for evaluating toileting performance and planning appropriate interventions need to be clearly defined. However, because of a lack of research in this area, particularly regarding the assessment and treatment of toileting performance, it is difficult to set SMART (Specific, Measurable, Achievable, Relevant, and Time-Bound) goals and implement effective goal-setting strategies. This oversight reveals a critical gap in systematically addressing toileting-related challenges, particularly in the care of children with CP. Although some studies, such as those by Belva et al. (2011) and Matson et al. (2011), have examined toileting issues through the Profile of Toileting Issues, they do not explore how these considerations can be integrated into SMART goals. Our study highlights this gap and underscores the need for targeted research to address this issue effectively (Belva et al., 2011; Matson et al., 2011).
Deficiencies in interdisciplinary collaboration are emphasized by specialists, citing a lack of specialized centers for toileting dysfunction treatment. Insights from professionals and mothers reveal the sensitive nature of issues related to bowel and bladder control, toileting functions, and menstruation. These private matters evoke feelings of embarrassment, shame, reluctance, and hesitation, emphasizing the need for supportive environments to comprehensively address such concerns.
Aligning with the literature (Dreher et al., 2022), this study corroborates the challenges of an imbalance in priorities and time constraints in clinical settings. Yet, the exploration of the need for a distinct code for toileting in the CPT framework to ensure comprehensive insurance coverage and improved accessibility and deficiencies in interdisciplinary collaboration offers novel insights. This aligns with recent discussions by Bendowska and Baum (2023), emphasizing the economic factors influencing the quality of care and the need for enhanced interdisciplinary cooperation. Addressing these issues requires improvements in interdisciplinary cooperation and better integration of toileting considerations in clinical practice.
Common Academic and Clinical Challenges
Common challenges persist in both academic and clinical settings, encompassing the underuse of creative educational methods, a deficiency in culturally validated assessment tools, and insufficient scientific evidence and resources dedicated to toileting. Bridging these gaps necessitates collaborative efforts to enhance toileting education and research outcomes. The identification of underuse of creative educational methods and the deficiency in evaluation tools resonates with findings in the works of Lam et al. (2021) and Mota and Barros (2008). Nevertheless, this study adds specificity by highlighting the pressing need for standardized assessment tools and creative educational methodologies.
This study highlights widespread oversight of innovative educational methods, including virtual reality, video modeling, the brain–computer interface, and computer technology, in addressing toileting challenges at both academic and clinical levels (Choi & Lo, 2014; Fatmawati et al., 2020; Lee et al., 2003; Mruzek et al., 2019; Zanona et al., 2022). Parental involvement is crucial because of the private nature of toileting, underscoring the need for creative and accessible training methods. The shared challenge of lacking culturally validated assessment tools, particularly at the academic level, impedes comprehensive evaluations. Globally, the academic sector faces a significant challenge because of the lack of sufficient scientific evidence and limited recognition of toileting issues in curricula. Clinically, the scarcity of available studies and in-service training workshops highlights the urgent need for localized guidelines. The challenges related to insufficient resources in this study are not universal but context-specific. Our review, which focused on Persian and English sources, uncovered a noticeable disparity in the availability of resources on toileting compared with other ADL areas. This disparity is influenced by geographic and contextual factors, with resource availability varying on the basis of the ability to access and use sources in different countries. This disparity underscores the necessity for localized guidelines and targeted efforts to bridge the resource gaps in toileting education and research in various contexts.
Allied health and medical professionals show limited engagement with toileting-related skills and disorders. Family perspectives often underestimate the need for specific toileting training, relying on the misconception that walking alone resolves toileting issues, neglecting the crucial role of education and practice. This study introduces novel challenges, such as limited training environments and unclear roles within the toileting management team, offering fresh perspectives on the toileting literature. These challenges resonate with broader discussions by Holland et al. (2017) and Horan et al. (2024), emphasizing the necessity of a holistic approach to address multifaceted issues in toileting management. To overcome these challenges, a collaborative effort is needed to enhance education, research, and practice in toileting management.
Considering the prominent role of occupational therapy in toileting and the importance of a family-centered approach, it is imperative to acknowledge the hurdles faced by families in this realm. The challenges articulated by families encompass several dimensions, yet further research is warranted to comprehensively delineate this domain (Beisbier & Laverdure, 2020). Among the highlighted challenges are the absence of formal training in toileting despite familial requests, insufficient prioritization of toileting concerns, delayed responsiveness to such issues by families, and pervasive feelings of embarrassment and shame that hinder open communication about toileting and menstruation.
Menstruation, which is closely associated with toileting, presents unique challenges for individuals with CP and their families, affecting participation in ADLs. These challenges include managing menstruation timing, ensuring proper hygiene, addressing discomfort, and formulating effective management strategies (AOTA, 2020). Clinical challenges related to menstruation include reluctance and apprehension within the treatment team, driven by concerns about potential embarrassment and cultural taboos that affect both individuals with CP and their parents.
The health implications of menstruation necessitate comprehensive education and training for both families and individuals with CP. Despite its integral role in health and hygiene management, menstruation remains inadequately addressed in the existing literature, revealing a critical gap that warrants attention and further investigation.
Limitations
Limitations of this study include a lack of diverse international representation among toileting professionals, potentially limiting its global applicability. Additionally, restricted access to non-English articles imposes limitations on the study’s scope and introduces a potential language-based bias. A further limitation of this study pertains to the restricted access to children with CP for direct input. This limitation stemmed from specific requirements, including age and cognitive ability, which hindered a comprehensive understanding of their perspectives. Additionally, this study exclusively focused on mothers as the primary caregivers of children with CP. The inclusion of other caregivers, such as fathers and grandparents, could potentially provide a better understanding of this issue and enhance the findings of this study from other perspectives.
Future Research Suggestions
Future research on these challenges for children with CP should focus on enhancing global collaboration among professionals, developing effective solutions to these challenges, addressing response timing issues, overcoming language barriers, implementing educational initiatives and interdisciplinary learning approaches to improve professional awareness, and quantitatively measuring the impact of these initiatives. Additionally, there is a need for the development of culturally sensitive toileting assessment tools, rigorous investigations into the efficacy of therapeutic interventions, and comprehensive studies involving families to understand their perspectives on these challenges. Finally, exploring the reasons for the difference in commitment levels among professionals should be considered an important avenue for future research, because it can provide valuable insights into factors influencing engagement and collaboration in addressing toileting challenges for children with CP.
Implications for Occupational Therapy Practice
This study highlighted vital implications for occupational therapy in enhancing toileting for children with CP. Occupational therapy professionals and educators should ▪ foster robust interdisciplinary collaboration among health care professionals for effective toileting issue resolution; ▪ incorporate assessment and training methods in occupational therapy education programs for addressing toileting challenges among children with CP; ▪ advocate for recognition of toileting function within broader health care contexts through active involvement in policy discussions; ▪ actively contribute to research on toileting outcomes for children with CP, including participation in studies and development of assessment tools; ▪ prioritize family-centered care, collaborating with parents and caregivers to offer tailored support and resources for toileting challenges; ▪ proactively engage in ongoing education and professional development, and stay updated on the latest research for improved toileting outcomes and enhanced quality of life for children with CP; and ▪ recognize and address cultural attitudes and sensitivities related to toileting, menstrual hygiene management, and other private matters. It is important to integrate cultural humility and sensitivity into all aspect of training, evaluation, and therapeutic interventions. This approach aims to ensure that care is not only clinically effective but also respectful of the diverse cultural backgrounds and specific needs of individuals and their families. This culturally informed approach will help ensure that occupational therapy practices are holistic, comprehensive, and attuned to the varied and unique experiences of children with CP and their families.
Conclusion
This study tackled challenges in investigating toileting performance, providing valuable insights into informed interventions that contribute to enhanced independence and improved quality of life for children with CP. It further clarified the roles of professionals on the toileting management team, with a focus on occupational therapy in ADLs. This approach nurtures a collaborative and holistic framework, optimizing intervention effectiveness and elevating the standard of care for those facing toileting-related issues.
Supplemental Material
Supplementary material for Challenges in Toileting Evaluation and Interventions for Children With Cerebral Palsy: A Delphi Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050717.pdf for Challenges in Toileting Evaluation and Interventions for Children With Cerebral Palsy: A Delphi Study by Azade Riyahi, Afsoon Hassani Mehraban, Mehdi Rassafiani, Zahra Pournasiri and Malahat Akbarfahimi in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We extend our heartfelt gratitude to all those who contributed to the successful execution of this study. Approval was obtained from the Research Ethics Committee of Iran University of Medical Sciences (IR.IUMS.REC.1400.1111). The datasets generated or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.