
Abstract
This study evaluated the efficacy of an elastomeric fabric orthosis to improve manual dexterity for people with Parkinson’s disease.
The common motor symptoms of Parkinson’s disease (PD), such as muscle rigidity, tremors, bradykinesia, and impairments in manual dexterity, defined as the skill and precision of fine motor and coordinated movements of the hands and fingers, significantly affect people’s ability to perform activities of daily living (ADLs) that require fine motor skills and their quality of life (QoL; Bloem et al., 2021). A decline in manual dexterity affects the functional use of the upper limb (UL) in tasks such as reaching, grabbing, and manipulating objects (Heffner & Masterton, 1983; Poirier, 1988). Manual dexterity serves as a strong predictor of the level of functional independence for people with PD (Bloem et al., 2021; Poewe et al., 2017).
The primary approach to motor symptoms in PD is pharmacological, primarily with levodopa and dopamine agonists. Although medication temporarily improves symptoms, there is currently no cure for PD (Connolly & Lang, 2014). Over time, patients often develop motor complications, such as dyskinesia and fluctuations in medication response, limiting its long-term effectiveness (Choi et al., 2017). In most cases, PD treatment is multifaceted, combining pharmacological treatment with other nonpharmacological approaches to improve the patient’s QoL. Various nonpharmacological interventions, such as exercise, acupuncture, and physiotherapy, among others, have been developed, with exercise especially resulting in improvements in QoL (Ahn et al., 2017; Van de Weijer et al., 2018).
Innovative nonpharmacological therapies, such as motor imagery, action observation, dual therapy, virtual reality, and robot-assisted therapy, are emerging to address functional issues in PD, although there remain a lack of studies and uncertainty regarding the optimal intervention dosage for effectiveness (Fusco et al., 2019; Righi et al., 2022; Ryan et al., 2021; Strouwen et al., 2015; Wang et al., 2019). Although some orthoses have proven effective in reducing motor symptoms in the UL, existing devices are often bulky and heavy, resulting in low treatment adherence (Fromme et al., 2019).
Dynamic elastomeric fabric orthoses (DEFO) are individually designed, custom-made Lycra garments that provide traction forces, aligning the limb biomechanically, leading to reduced muscle tone and edema and improved proprioception (Betts, 2015; González-Bernal et al., 2017). These orthoses can be crafted as individual gloves or sleeves, full-body suits, vests, or ankle–foot wraps (Betts, 2015; Powell et al., 2021). Although DEFO has proven effective for people with conditions such as stroke, pediatric cerebral palsy, multiple sclerosis, and complex regional pain syndrome, with positive results in motor function, muscle strength, manual dexterity, and reach (Alexander et al., 2022; Giray et al., 2020; Miller et al., 2016), its effectiveness among people with PD remains uncertain.
The main goal of occupational therapy is to promote and enable meaningful contextual occupational performance. The impairment in fine motor skills caused by PD leads to a decline in the person’s ADL performance and independence. Therefore, because of the lack of devices or treatments and the promising research on DEFO for people with other neurological conditions, the aim of this study is to assess the effectiveness of this device on UL manual dexterity of people with PD.
Method
Participants
A longitudinal study was undertaken involving a control group (CG) and an experimental group (EG). Recruitment of patients diagnosed with PD at any stage and experiencing motor symptoms in at least one UL took place between September and October 2021 through consecutive nonprobabilistic sampling at the Neurology Department of the University Hospital of Burgos. Exclusion criteria were tremor resulting from another neurological disease, a Montreal Cognitive Assessment (MoCA) score of 26 or lower, or both (Postuma et al., 2015).
PD diagnosis was based on criteria established by the International Parkinson and Movement Disorder Society, which require the presence of bradykinesia along with rigidity, resting tremor, or both. Additionally, at least two of four supportive criteria (dramatic improvement with dopaminergic therapy, dyskinesias, loss of smell, resting tremor, or cardiac sympathetic denervation on myocardial scintigraphy) needed to be met (Armstrong & Okun, 2020; Postuma et al., 2015).
The study adhered to ethical principles outlined in the Helsinki Declaration, and participants provided informed consent. The study was approved by the Clinical Research Ethics Committee of the Health Area of Burgos and Soria (Spain; Reference CEIM-2119/2019) and registered with ClinicalTrials.gov (NCT04815382).
Procedure
The sample size calculation was based on the main variables of improvement in rigidity and tremor. With an α risk of .05 and a β risk of .20, using a two-tailed test, we estimated that 40 participants (20 in each group) would be needed to detect a minimum difference of .50 in rigidity and tremor of the most affected UL as measured with the Motor Subscale of Part III of the Unified Parkinson’s Disease Rating Scale (UPDRS; Winter et al., 2022). Finally, because of participants’ availability and interest, the number of participants in the EG was increased to 40, resulting in a total sample size of 60 (EG = 40, CG = 20).
At the first visit, participants who met the established criteria signed the informed consent. Occupational therapists (including María Jiménez-Barrios and Mirian Santamaría-Peláez) collected sociodemographic and clinical data. One month before DEFO implementation, exact measurements of the UL were taken by an occupational therapist (who was also a physical therapist) for customization of the orthosis. The professionals who carry out these measurements must be specifically trained to do so.
The orthosis used in this study is an UL DEFO that covers the entire arm and therefore acts on the entire UL, providing proprioceptive stimulation. Because tremor in people with PD subsides with activity, muscle contraction, and support, the orthosis activates the finger extensors, wrist extensors, radial deviators, supinators, and external rotators; thus, the UL is positioned with the musculature in contraction, such as when the UL is placed in a support-and-load position. To manufacture the orthosis, computer-aided design and manufacturing technology was used along with traditional manufacturing techniques to guarantee that each product matched the patient’s exact measurements. The power net reinforcement panels were strategically placed to position the UL in better postural alignment (see Appendix A in the Supplemental Material, available online with this article at https://research.aota.org/ajot).
Participants were randomly assigned to the CG or EG with the Epidat 4.2 program (https://www.sergas.es/saude-publica/epidat-4-2?idioma=es). The treatment protocol involved implementing the DEFO on the most affected UL for 2 mo. Participants in the CG continued with their usual daily activities. The EG participants wore the orthosis from the moment they got up until they went to bed. They took it off only to sleep and shower. They were instructed to use it in all their usual activities and to try to carry out those activities that they had stopped doing because of their motor symptoms, such as fishing, sewing, or gardening. All participants continued with their usual pharmacological treatment. The effects were evaluated during both the on state (under the effects of levodopa) and the off state (1 hr before the next levodopa dose) because PD’s motor symptoms fluctuate significantly (Martin et al., 2010). The on state refers to periods when medication is effective, and patients experience significant improvement in their motor function. The off state refers to periods when medication is not effective, and Parkinson’s motor symptoms reappear or worsen significantly, with patients experiencing increased rigidity, bradykinesia, and tremors. In this research, it is important to evaluate the effect of the DEFO in both states because of the significant difference in motor symptoms between them.
During the 2 mo of treatment, two scheduled calls were made to participants, the first after 1 wk and the second after 1 mo of wearing the orthosis, to obtain information about adherence to treatment; they were also asked about adherence at the 2-mo evaluation. All participants reported that they had worn the orthosis for the amount of time indicated.
Motor assessments were conducted by occupational therapists at two time points, immediately before (T1) and after (T2) the 2-mo intervention window. At both times, two assessments were performed, one before and one after implementation of the DEFO, to check for its immediate effects and its potential long-term benefits (Figure 1). The results were analyzed by occupational therapists (Santamaría-Peláez and Jiménez-Barrios). Neither participants nor evaluators were blinded.
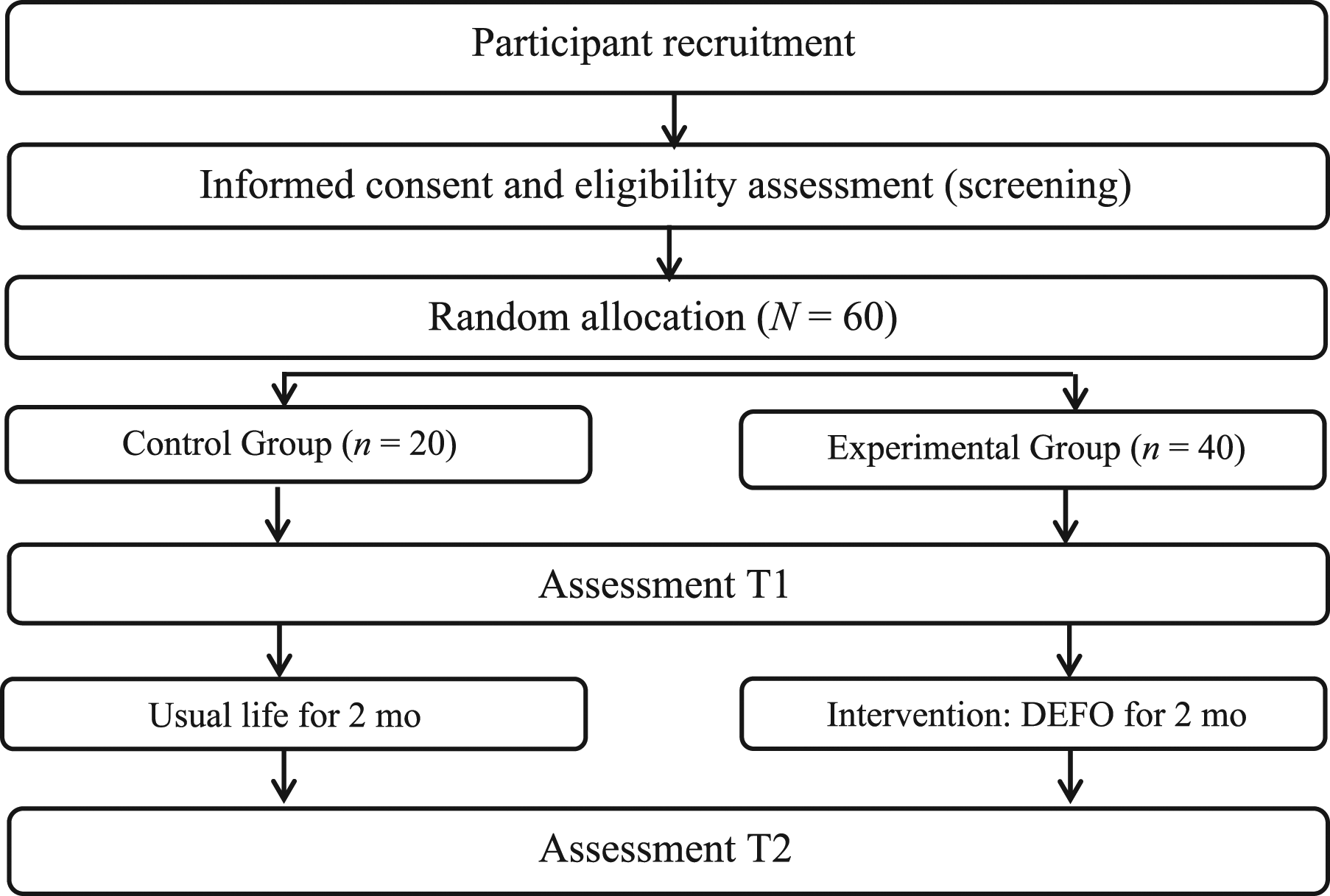
Flow of participants through the study.
Manual dexterity was assessed with three different tests, the Purdue Pegboard Test (PPT), the abbreviated version of the Minnesota Manual Dexterity Test (MMDT), and the Square Test (ST), following standard testing procedures.
The PPT consists of a rectangular wooden board with 50 holes in two parallel columns and a set of pegs, washers, and collars placed in four cups at the top of the board. It has four subtests that evaluate the use of the right hand, use of the left hand, use of both hands (alternating movements), and the combination of all three. The score for each subtest is the number of pieces placed. All subtests were performed three times, and scores were averaged to obtain the total score. Higher scores indicate greater manual dexterity. The PPT has high test–retest reliability, with an intraclass correlation coefficient (ICC) of ≥.90 (Lo et al., 2022; Proud et al., 2019).
The MMDT consists of a rectangular board with 60 holes in 15 columns and four rows, with 60 circular pieces with one side red and other black. It has two subtests, Displacement and Rotation, that are performed four times, and the total score is the average of them (see Figures B.1 and B.2 in Appendix B of the Supplemental Material). The less time taken in the tests, the better the manual dexterity. It is a reliable and valid measure, with high test–retest reliability, and an ICC of .79–.88 (Rane et al., 2017; Wang et al., 2018).
The ST consists of a sheet of paper with four printed grids, each consisting of 20 squares. The patient is given 30 s to make a mark with a pen inside as many squares as possible. The score is the number of marks made without touching the lines. A higher score indicates better manual dexterity. This is a reliable and valid test with excellent test–retest reliability for both hands (ICC ≥ 0.93; Desrosiers et al., 1997; Soke et al., 2019).
Statistical Analysis
The data were analyzed using IBM SPSS Statistics (Version 28), with p < .05 considered statistically significant. Means and standard deviations were calculated for quantitative variables, and frequency and percentages were determined for categorical variables. To analyze the differences between not wearing and wearing the orthosis at both T1 and T2 in the EG, the paired t test for related samples was used, with a Bonferroni correction to control for the family-wise error rate. Four tests were taken into account as adjustment (two time points and two medication conditions); thus, the corrected p value was 0.0125 (0.05/4). To analyze the differences between CG and EG after 2 mo wearing the DEFO, means between the two groups were compared using analysis of covariance (ANCOVA), with group (CG or EG) as a fixed factor, differential scores of the analyzed variables as dependent variables, and the pretest scores of each group as covariates. Both Student’s t tests and ANCOVA were performed for participants in the on and off states.
Results
The sample was composed of 60 individuals with a mean age of 71 yr. Of the participants, 88% lived with someone (n = 53), 10% lived alone in their homes (n = 6), and one person (2%) lived in a religious community. Other sociodemographic data are shown in Table 1. Table 2 shows the observed differences in the comparative analysis of motor dexterity assessments (PPT, MMDT, and ST) at baseline (T1) with and without the orthosis in both off and on states. Table 3 presents the observed differences in the comparative analysis of motor dexterity assessments (PPT, MMDT, and ST) in the evaluation conducted 2 mo postimplementation of the DEFO (T2), both with and without the orthosis in both on and off states. No differences were observed between the CG and the EG on the PPT, MMDT, or ST without orthosis after the EG had worn the orthosis for 2 mo (see Table B.1 in the Supplemental Material).
Baseline Characteristics
Comparative Analysis of Motor Dexterity Assessment at Baseline With and Without the Orthosis: Paired t Test for Related Samples (N = 40)
Note. Means are the mean difference between the groups with and without orthosis. Boldface indicates significant results. MMDT = Minnesota Manual Dexterity Test; on = under levodopa effects; off = 1 hr before next levodopa dose; PPT = Purdue Pegboard Test; ST = Square Test.
Comparative Analysis of Motor Dexterity Assessments After 2 Mo Postimplementation of the DEFO, With and Without the Orthosis: Paired t Tests for Related Samples (N = 40)
Note. Means are the mean difference between the groups with and without orthosis. Boldface indicates significant results. MMDT = Minnesota Manual Dexterity Test; off = 1 hr before next levodopa dose; on = under levodopa effects; PPT= Purdue Pegboard Test; ST = Square Test.
Discussion
Among motor symptoms, bradykinesia, rigidity, resting tremor, and impaired motor dexterity are prominent and can manifest themselves in varying degrees as the disease progresses, but they are highly bothersome and disabling, affecting performance of ADLs and QoL (Bloem et al., 2021; Postuma et al., 2015). The main results of this study indicate that improvements in certain aspects of motor dexterity occur when participants wear the orthosis. However, after using the orthosis regularly for 2 mo, no differences were observed in manual dexterity of the UL when the orthosis was removed.
In recent years, the effectiveness of these devices has been tested in other conditions. Alexander et al. (2022) explored their implementation with stroke patients, observing an improvement in function and dexterity in the UL and promotion of participation in repetitive activities. Studies conducted with people with cerebral palsy have demonstrated the effectiveness of these devices in improving manual dexterity (Giray et al., 2020; Pavão et al., 2018), functionality, and alignment of the affected UL (Yasukawa & Uronis, 2014).
These results partially align with those obtained in the current study because an immediate effect of the orthosis was observed for some subtests at both T1 and T2. Therefore, improvements in certain aspects of motor dexterity are observed when the orthosis is being used. However, after using the orthosis for 2 mo, no differences were observed between the CG and EG when the tests were performed without the orthosis, which may be explained, in part, because although PD is a degenerative condition, stroke and cerebral palsy are not.
Various orthoses have shown positive effects on reducing involuntary movement, but they were also heavy and unattractive, leading to reluctance to use them (Fromme et al., 2019; Mo & Priefer, 2021). Therefore, a need exists to design orthoses that are lighter and more appealing to patients while also providing an improvement in manual dexterity.
This research must be considered in the context of its strengths and limitations. Implementation of and patient adherence to DEFO have proven to be easy, resulting in improvements in some aspects of manual dexterity, in both the on and the off states of the disease. Although no differences in manual dexterity were found after the orthosis was removed, occupational performance improved with the orthosis on. Furthermore, orthoses are a nonpharmacological treatment with no contraindications for patients.
The results show a tendency toward greater differences between wearing or not wearing the orthosis in the on state; however, they lack statistical significance after the Bonferroni correction is applied. At first glance, there does not seem to be an obvious reason for medication state to interact with orthosis use in this way; however, the role of medication state and its interactions with the findings should be addressed in more depth in future research. Understanding the orthosis response in both states allows for optimization of its use, adjusting the timing to maximize its benefits during on periods and minimize symptoms during off periods.
The observational nature of the study and not having blinded evaluators or patients are limitations of this study. Additionally, because of the study’s limited duration, it was not possible to ascertain whether longer-term treatment might lead to further improvements or whether it could slow down the progressive deterioration of the disease. However, although participants reported that they had worn the orthosis for the amount of time indicated because they were able to perform their activities better and they had less tremor, these devices do not include a sensor that allows objective data on patient adherence to be obtained. Although this information was obtained through telephone calls made during the intervention period as well as at the 2-mo evaluation, obtaining objective data about both adherence and participation would be useful.
The use of the Bonferroni correction has some advantages and disadvantages to consider. It is easy to apply and understand, and it minimizes the risk of false-positive errors, and it is a robust and conservative adjustment that does not depend on the nature or distribution of the data or tests and works for any number of statistical tests. However, it may be too conservative, reducing the power of each test and increasing the risk of false-negative errors; it is also not flexible, because it does not take into account the dependence or correlation between tests. All of this must be taken into account when interpreting our results because when the corrected α value is applied, some results that would be positive at a significance level of .05 are lost; future research will have to addressed this.
Furthermore, this orthosis was implemented during the winter months in a city with a cold climate, so it did provide warmth to the participants. It would, however, be interesting to manufacture it in a breathable material because the orthosis may be less comfortable in warmer climates and thus affect adherence to wearing it.
Currently, effective orthopedic devices that can be implemented as a nonpharmacological treatment among people with PD are lacking. The results obtained in the current study can be a starting point for research on these devices for people with PD or for encouraging the development of new ones that are easy to implement and lightweight, improve patient adherence and manual dexterity, and thus allow greater participation in ADLs, as well as improving patients’ functionality and quality of life. Given that no effects were found when the device was removed, in future research with a longer duration of orthosis use, it could be interesting to have patients wear it only while performing activities that are relevant to them. Furthermore, given that the biggest problem with current orthoses is patients’ lack of adherence because the orthoses are heavy, including a sensor in the orthosis could allow adherence to be checked and provide objective data.
Although we found no differences in manual dexterity after removal of the orthosis, it is possible that differences could occur in other variables not studied, such as occupational performance, daily use of the arm and hand, and so forth. These would be interesting variables for future research.
Implications for Occupational Therapy Practice
Currently, the primary treatment for PD is pharmacological; however, occupational therapy is of great relevance to patients’ occupational performance and QoL. Studies such as this one can encourage greater involvement of occupational therapy with this and other populations. This research shows an alternative nonpharmacological treatment that could reduce patients’ motor symptoms, improve their functionality, and increase their QoL without adverse side effects.
In clinical practice, the implications of implementing DEFO could lead to a reduction in bothersome motor symptoms such as tremors and rigidity, thereby enhancing functionality and fostering greater autonomy in patients’ daily lives. Moreover, such interventions have the potential to substantially improve patients’ QoL, fostering a positive self-image and reducing embarrassment and insecurity associated with symptoms such as tremors. By enabling individuals to participate more fully in social activities and group outings without fear of functional limitations, these interventions could enhance social integration and rekindle interest in activities that patients may previously have abandoned. This, in turn, could bolster motivation to explore new activities and experiences without the burden of apprehension or the fear of failure, ultimately promoting a more fulfilling and enriching lifestyle for patients.
Conclusion
The DEFO is an easy-to-implement device that may improve manipulative dexterity when worn, and it may therefore be a nonpharmacological adjunct to standard treatment to improve the motor aspects of PD. Few studies have been conducted with the DEFO among people with PD; thus, further research is needed to verify its efficacy with people with PD as well as to determine whether these possible improvements in manipulative dexterity translate into improvements in occupational performance and participation. Including treatment adherence variables in future research would also be of interest.
Supplemental Material
Supplementary material for Impact of a Dynamic Orthosis on Manual Dexterity Among People With Parkinson’s Disease: A Randomized Trial
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050723.pdf for Impact of a Dynamic Orthosis on Manual Dexterity Among People With Parkinson’s Disease: A Randomized Trial by María Jiménez-Barrios, Jerónimo González-Bernal, Mirian Santamaría-Peláez, Carla Collazo-Riobo, Esther Cubo, José María Trejo Gabriel-Galán, Martin J. A. Matthews and Josefa González-Santos in The American Journal of Occupational Therapy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.