
Abstract
The study examined the impact of engagement in meaningful activities on quality of life among community-dwelling older adults during COVID-19.
Healthy aging encompasses successfully maintaining functional capabilities despite the physical and health challenges that older adults may encounter (Beard et al., 2016; Rowe & Kahn, 2015). Over the past 50 yr, life expectancy has increased significantly, resulting in more individuals who are age 65 and older (World Health Organization [WHO], 2015). This demographic shift is projected to continue, increasing the proportion of older adults (Bloom & Luca, 2016). The changing population structure and the biopsychosocial changes affecting older adults’ health pose new challenges for health care systems and the economy. In response, efforts are being made to promote vaccination, independence, and overall healthy aging (Aronson, 2020; Friedman et al., 2019), along with psychosocial factors that can predict older adults’ quality of life (QoL; Bowling & Iliffe, 2011).
QoL is defined as an individual’s perception of their position in life in the context of the culture and the value system they inhabit in relation to expectations, patterns, and concerns (World Health Organization Quality of Life Group, 1995). The concept of QoL includes physical, psychological, social, and environmental factors. The concept of QoL is often used interchangeably with health (Karimi & Brazier, 2016) because they are closely associated (Silva et al., 2014). As adults age, they may face unique QoL-related issues (Burks et al., 2021), such as living alone, missing people significant to them, reduced physical and mental health, and less social and emotional support, all of which generally affect QoL (Dana et al., 2022; Van Leeuwen et al., 2019). Another important factor associated with QoL and better health is participation, which reduces levels of depression and the prevalence of diseases among older adults (Punyakaew et al., 2019; Stav et al., 2012).
The International Classification of Functioning, Disability, and Health Framework defines participation as involvement in life situations within the familial, social, and occupational environments to which an individual belongs (WHO, 2001). Participation naturally occurs when a person engages in activities or experiences that hold purpose and personal meaning (American Occupational Therapy Association, 2020). Engaging in activities consists of an objective dimension (e.g., frequency, duration, diversity) and a subjective dimension encompassing the occupational experience, including meaningfulness, involvement, and choice in activity performance (Hammell, 2004). The significance of engaging in activities is also relevant for older adults, who may be susceptible to functional deterioration because of the convergence of biopsychosocial factors (Jessen-Winge et al., 2018).
Biopsychosocial factors, such as health conditions, mental functions, and environmental factors, could also be affected by global crises, such as the coronavirus disease 2019 (COVID-19) pandemic. During the COVID-19 pandemic, Israel implemented a range of restrictions, including lockdowns and mandatory quarantine, to control the spread of the virus. These measures evolved in response to the pandemic’s severity and the success of vaccination efforts. Thus, the pandemic affected almost all aspects of daily life, requiring social distancing, isolation, changes in life routines, and heightened health risks (Lipskaya-Velikovsky, 2021). The pandemic’s effects were more severe on older adults, who were more vulnerable to illness and mortality because of underlying health conditions (Shahid et al., 2020). Older adults also experienced psychological symptoms, reduced social interactions, increased ageism, and physical deterioration (Lebrasseur et al., 2021). The social restrictions, physical distancing, isolation, and limited access to health care services led to less physical activity, poorer health management, and loneliness, all of which were associated with decreased mental and physical health (Abbaspur-Behbahani et al., 2022; Oliveira et al., 2022; Santini et al., 2020; Seifert & Hassler, 2020). These studies’ findings underscore the importance of identifying protective factors to mitigate risks faced by older adults during challenging times, including various aspects of the pandemic, such as health threats or extreme environmental restrictions.
A recent study examined the changes in activities of older adults during the pandemic and found, for instance, a reduction in the number of out-of-home trips and social interactions during the restrictions (Gough et al., 2023). Two longitudinal studies reported worsened physical health symptoms, deteriorating mental health, and reduced QoL among older adults during the pandemic (Herrera et al., 2021; Zaninotto et al., 2022). However, these studies did not explore possible mitigating effects of meaningful activities. Other studies only examined the effect of specific activities, such as physical activity (Callow et al., 2020) or volunteering (Dumont et al., 2023), on community-dwelling older adults’ health or QoL. Our study aimed to examine the relationship between engagement in meaningful activities (EMA) and QoL via two research questions: (a) What did EMA contribute to the QoL of older adults beyond sociodemographic variables and health conditions during the COVID-19 crisis? (b) How did older adults experience the effects of the pandemic on their health and QoL?
Method
Research Design and Participants
We used a cross-sectional correlative mixed-methods design (quantitative and qualitative). A total of 302 community-dwelling older adults (mean age = 75.05 yr, SD = 7.45) were recruited during the fourth to sixth waves of the COVID-19 pandemic in Israel (from July 1, 2021 to July 31, 2022), a period characterized by mask mandates and vaccination recommendations. Inclusion criteria were age 65 and older and no hospitalization in the previous month. Participants’ demographic and health characteristics are presented in Table 1.
Demographic and Health Characteristics of the Sample (N = 302)
Data were missing for five cases.
Data were missing for 12 cases.
Measurements
Engagement in Meaningful Activities Survey
The Engagement in Meaningful Activities Survey (EMAS; Goldberg et al., 2002) is a self-report questionnaire assessing a person’s degree of involvement in meaningful activities. It consists of 12 items on a 5-point scale from 1 (never) to 5 (always), yielding a total score ranging from 12 to 60. A high score indicates high involvement in meaningful activities (Goldberg et al., 2002). The EMAS has high internal consistency, convergent validity, and acceptable test–retest reliability; it has been used with older adults (Eakman et al., 2010). Internal consistency in this study was excellent (Cronbach’s α = .93).
World Health Organization Quality of Life Scale
This self-administered abbreviated version of the World Health Organization Quality of Life scale (WHOQOL-BREF; WHO, 2004) assesses self- perceptions of QoL in the context of one’s cultural values and personal goals, expectations, standards, and concerns. The WHOQOL-BREF contains 26 items that assess physical health, psychological health, social relationships, and environment. Items are measured on a 5-point scale, yielding a transformed total score ranging from 0 to 100, with higher scores indicating higher QoL. It has good discriminant validity, internal consistency, and test–retest reliability among the general population and older adults (Goes et al., 2021). The internal consistency in our sample was also good (Cronbach’s α = .82).
Four-Item Patient Health Questionnaire for Anxiety and Depression
The four-item Patient Health Questionnaire (PHQ–4) for anxiety and depression (Kroenke et al., 2009) is a self-report questionnaire that uses a two-item Depression scale and a two-item Anxiety scale. The items are rated on a 4-point scale from 0 (never) to 3 (almost constantly), yielding scores ranging from 0 to 12; higher scores indicate greater psychological distress. The PHQ–4 has displayed good internal consistency and validity in measuring depression and anxiety symptoms (Löwe et al., 2010). Good internal consistency was also observed in this study (Cronbach’s α = .88).
Sociodemographic Questionnaire
We developed a questionnaire for this study that included questions about the participants’ demographics (e.g., age, gender, family status, ethnicity), financial status (e.g., “How well does your household make ends meet?”), and perceived health status (e.g., “Do you suffer from long-term health problems?”). In addition, three open-ended questions sought to explore how COVID-19 affected the participant’s health, QoL, and activities (“Were there any changes in your daily activities due to COVID-19?” “How did the COVID-19 pandemic affect your health?” “How did the COVID-19 pandemic affect your QoL?”)
Procedure
After ethical approval from the Hebrew University of Jerusalem institutional review board (No. 24052021), we used a convenience sampling method to recruit participants via social media and snowball sampling. Participation was voluntary and anonymous. After consenting, the participants completed the questionnaires either face-to-face on paper or online in their preferred format, font size, and language (Hebrew, Arabic, or English). In addition, graduate occupational therapy students were available physically and online to assist, such as reading the questions aloud or writing the responses if needed.
In adherence to established guidelines for questionnaire translation (WHO, 2010), all questionnaires used in this study that did not already have a validated translation to Hebrew or Arabic were rigorously translated according to a scientific translation protocol. The translation process followed the recommended steps, including forward translation by bilingual translators, back-translation to the original language, and validation by bilingual experts.
Data Analysis
We performed quantitative statistical analyses using IBM SPSS Statistics (Version 28), with significance set at p < .05. We analyzed descriptive statistics of the demographic data and scores of all the measures. Some of the variables were not normally distributed, as assessed by Shapiro–Wilk test (p < .05); therefore, we calculated Spearman’s rank-order correlations. There was linearity, as assessed by partial regression plots and a plot of studentized residuals against the predicted values. Residuals were independent (Durbin–Watson statistic = 2.104). A visual inspection of a plot of studentized residuals versus unstandardized predicted values showed that there was homoscedasticity. There was no multicollinearity (tolerance values > 0.1), no studentized deleted residuals greater than ±3 SD, no leverage values greater than 0.2, and no values for Cook’s distance above 1. The assumption of normality was met, as assessed by a Q-Q (quantile–quantile) plot. Therefore, we used hierarchical multiple regression to evaluate the association of sociodemographic data, health status, and EMA with the QoL of older adults, using mean imputation for missing values (4% or less).
We conducted qualitative analysis using the structured tabular thematic approach for brief texts (Robinson, 2022) with a hybrid (inductive–deductive) design. The responses were initially coded into four themes based on the study’s aims and the open-ended questions. The author (Haya Fogel-Grinvald) and a research assistant read all responses independently and assigned code words accordingly, followed by discussion and refinement. Further consultation with the other authors (Adina Maeir and Anat Golos) produced agreement on the final themes and subthemes. Afterward, Fogel-Grinvald and the research assistant tabulated the themes against data segments, reviewed the results, and discussed any remaining disagreements. A sufficient interanalyst agreement was reached (96.4%), and theme frequencies were calculated. Finally, we developed a thematic map to integrate the themes.
Results
Quantitative Findings
Most of the 302 participants were female (70.9%), and about half reported no long-term health problems (Table 1). Participants generally exhibited a sufficient degree of EMA, with relatively high QoL and low levels of depression and anxiety, as indicated by the means in Table 2; however, the standard deviations and ranges suggest a heterogeneous sample. As can also be seen in Table 2, there were negative significant correlations between perceived health variables (has a long-term health problem and PHQ–4) and QoL, as well as a positive, strong, and significant correlation between EMA and QoL, indicating that better perceived health and higher levels of engagement were associated with higher QoL.
Descriptive Statistics and Spearman’s Correlations Between the Study Measures
Note. N = 302. PHQ-4 = four-item Patient Health Questionnaire for anxiety and depression; EMAS = Engagement in Meaningful Activities Survey; WHOQOL-BREF = World Health Organization Quality of Life.
Data are missing for five cases.
***p < .001.
We conducted a hierarchical multiple regression model to answer the first research question and to determine whether adding the EMA variable improved the prediction of QoL beyond sociodemographic and perceived health variables. We included sociodemographic characteristics in the first model, perceived health variables in the second model, and EMA in the third model. As shown in Table 3, the addition of EMA to the prediction of QoL led to a statistically significant increase in R 2 of .13, F(1, 292) = 92.45, p < .001. The complete model (Model 3) of sociodemographic characteristics, perceived health, and EMA to predict QoL was statistically significant, R 2 = .60, F(9, 292) = 47.85, p < .001, adjusted R 2 = .58. Age, financial status, and perceived health were also significant in the final model. Incidentally, Models 1 and 2 were also statistically significant.
Hierarchical Multiple Regression Predicting Quality of Life From Sociodemographic Characteristics, Perceived Health, and Engagement in Meaningful Activities
Note. N = 302. WHOQOL–BREF = World Health Organization Quality of Life; PHQ–4 = four-item Patient Health Questionnaire for anxiety and depression; EMAS = Engagement in Meaningful Activities Survey.
Degrees of freedom: Model 1, F(6, 295); Model 2, F(8, 293); Model 3, F(9, 292).
*p < .05. **p < .01. ***p < .001.
Qualitative Findings
To answer the second research question and gain deeper insights into the impact of COVID-19 on the health and QoL of older adults, we invited participants to describe how the pandemic influenced their daily activities, health, and QoL. Initially, 369 responses were analyzed, and 9 responses were excluded because they were unclear or unrelated to the questions asked. The structured tabular thematic approach analysis revealed four themes and nine subthemes from participants’ responses. Figure 1 depicts all themes and subthemes with their reported frequencies and examples of the responses. Numbers were assigned to themes based on their frequency.
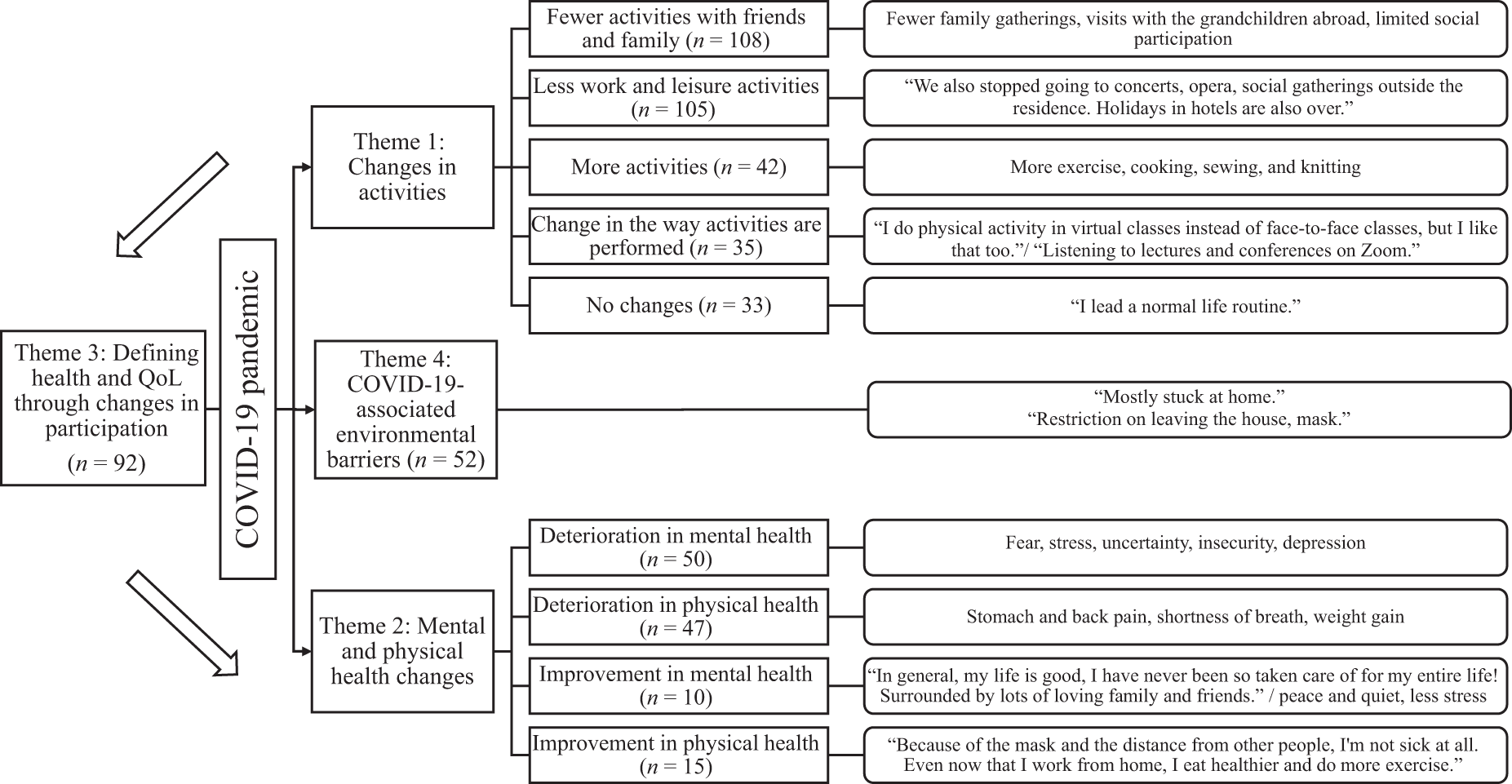
Thematic map: Effect of the COVID-19 pandemic on participants’ activities, health, and quality of life and their qualitative responses
Theme 1, changes in activities, and five subthemes were derived from the question, “Were there any changes in your daily activities due to COVID-19?” The two most frequently cited subthemes were fewer activities with friends and family (n = 108, 30.0%) and less work and leisure activities (n = 105, 29.2%). Only 21.4% (n = 77) reported more activities or a change in how activities were performed. The three additional themes were derived from the questions, “How did the COVID-19 pandemic affect your health/QoL?” Theme 2, mental and physical health changes, included four subthemes, and most participants described a deterioration in physical and mental health (n = 97, 26.9%), but a few described improved physical and mental health (n = 25, 6.9%). Theme 3, defining health and QoL through changes in participation, accounted for 92 responses (25.6%). Examples of responses within this theme included statements such as “Life has changed, in terms of employment, leisure, meetings,” “It was difficult to do what I used to do before the pandemic,” and “Less meetings with friends and family and less cultural events.” These responses demonstrate how having limited access to, or engaging in meaningful activities, during the pandemic was perceived as affecting health and QoL, thus emphasizing the importance of EMA in the lives of community-dwelling older adults during the COVID-19 pandemic in Israel. Theme 4, COVID-19-associated environmental barriers (n = 52, 14.4%), described the restrictions imposed during the pandemic and their effects on participants’ health and QoL. The thematic map presented in Figure 1 integrates the four themes, illustrating the complex interplay between the COVID-19 pandemic and its effects on the participants. The pandemic directly influenced participants’ activities and health (Themes 1 and 2). Changes in access to or frequency of engagement in activities due to COVID-19 environmental barriers (Theme 4) contributed to a different perception of health and QoL, which further influenced mental and physical health. In addition, there was an indirect effect on health and QoL through the restrictions that impeded participation (Theme 3). The arrows in the figure depict the directionality of these relationships, indicating both direct and indirect pathways.
Discussion
This study investigated the impact of EMA on community-dwelling older adults’ QoL during the COVID-19 pandemic. The results indicated that EMA was positively associated with QoL and contributed to the overall QoL of older adults beyond their sociodemographic background or perceived health status during the pandemic. Our research supports evidence for the positive effect of EMA on mental health during COVID-19 and adds to the body of knowledge about adults over age 65. Previous studies (Cruyt et al., 2021; Tigershtrom & Boyraz, 2022) examined the effect of EMA on mental health and psychological distress during the pandemic but among adults over 18. Costenoble et al. (2023) supported our findings, but they only studied octogenarians.
Most studies focused on specific activities and their effects on older adults’ health and QoL during the pandemic. For example, Rivera-Torres et al. (2021) examined the effects of leisure activities on the mental health of older adults during the pandemic and reported mental health benefits from various activities. However, during a crisis such as a pandemic, with its rapidly changing routines and environmental restrictions, focusing on EMA rather than tracking a specific activity may provide a more general picture. This approach acknowledges that not all activities can continue uninterrupted, and the subjective nature of EMA allows individuals to find meaningful activities despite environmental or personal constraints and limitations. Furthermore, Hooker et al. (2020) supported the idiographic assessment of meaningful activities such as EMAS rather than the nomothetic approach that predetermines the significance of activities.
The study’s second aim was to gain deeper insights into older adults’ experiences of the pandemic’s impact on their health and QoL. The three most frequent qualitative themes reported by our sample substantiated and complemented the results of the quantitative analysis. These themes specified the changes in activities, the changes in health and QoL, and most important, the integration of engagement in activities in participants’ responses to the general questions about the impact of COVID-19 on health and QoL.
First, we gained a more in-depth understanding of the impact of COVID-19 on activity patterns, with details of what people did more, less, or differently during the pandemic. Theme 1 revealed a change in participants’ activities, primarily, fewer leisure activities and fewer social gatherings with friends and family. These findings align with the study of Heid et al. (2021), which also used a mixed-methods approach to investigate the challenges of social distancing.
Second, our study provided insights into older adults’ perceptions of health and QoL during the COVID-19 pandemic. Participants expressed mixed subjective views regarding the pandemic’s effect on their health. In Theme 2, most participants reported a deterioration, but some reported improvement. Similar mixed experiences of older adults were reported by Xie et al. (2021), who highlighted the complexities of older adults’ lived experiences during the pandemic.
Last, and most important, participants in the study used their engagement in activities, or lack thereof because of pandemic-related environmental barriers, to express how COVID-19 had affected their health and QoL. This led to the finding of a clear link between EMA, health, and QoL. This conclusion reinforced the findings of McKinlay et al. (2021) that the inability to engage in activities that protect well-being was a threat to the mental health of older adults. Thus, the qualitative analysis added a novel aspect of the subjective definition of health through participation in activities.
In summary, this study’s quantitative and qualitative findings complemented one another. The correlations observed between EMA, health, and QoL were mirrored in open-ended responses detailing the direct impact of the pandemic as well as the influence of changes in participation, affected by environmental constraints, on health and QoL. Thus, the findings demonstrated that the role of EMA seemed to have an impact on older adults’ health and QoL and should be considered, especially in times of adversity when environmental constraints or personal stressors are intensified.
Limitations
The study had several limitations. First, we used a convenience sample; most participants completed the questionnaires online. Consequently, the participants were predominantly from a sociodemographic category with internet access and basic computer knowledge. Second, the data were collected during the fourth to sixth waves of the COVID-19 pandemic (July 1, 2021 to July 31, 2022) when restrictions were less severe than the first three waves and there were no travel restrictions or an obligation to stay home; thus, the participants could have already adjusted to the limitations. To further assess EMA’s effects on older adults’ QoL, future research should be conducted during various times of a crisis. Ideally, research would include pre- and postcrisis data collection to examine changes in EMA and QoL. In addition, studies should encompass diverse sociodemographic backgrounds and other health-related factors that may influence EMA.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ Supporting EMA during times of crisis can potentially improve community-dwelling older adults’ perceived psychological health and QoL. ▪ When there are environmental restrictions on participation, occupational therapy practitioners may have a unique role in partnering with older adults to find alternative ways to engage in new meaningful activities or increase their involvement in activities they currently enjoy and can engage in.
Conclusion
Our study provided insights into the impact of EMA on the QoL of community-dwelling older adults during the COVID-19 pandemic. We found a positive association between EMA and QoL, which remained robust even when controlling for sociodemographic factors and perceived health status. The study’s qualitative analysis shed light on the direct effects of pandemic-related restrictions on participation in activities, health, and QoL. Notably, participants explicitly identified changes in their participation in activities as adversely affecting their health and QoL during the pandemic. The convergence of quantitative and qualitative findings highlighted the interconnectedness of EMA, health, and QoL, emphasizing the pivotal role of occupation in older adults’ QoL, particularly in times of heightened adversity, and offering valuable insights for future research and policy efforts to support this population’s health.
Footnotes
Acknowledgments
We are grateful to the following Master’s students for their invaluable assistance with this research: Miriam Frankl Naor, Haia Khourieh, Noa Wities, and Shira Zecharia. This study was supported by The Israel National Institute for Health Policy Research (2021/92/ר/) and The Minerva Center on Intersectionality in Aging (#49478).