
Abstract
This scoping review describes literature on the practice of cultural humility in occupational therapy services.
Inequities in health systems and health outcomes are a common and growing concern in the Canadian and U.S. health care systems (Comeau et al., 2023; Dickman et al., 2017). Diverse, evolving factors such as social, economic, environmental, and structural disparities perpetuate health inequities, influencing variations in clients’ health care and outcomes (Gillispie-Bell, 2021). Notably, it has become more apparent that social and cultural factors, such as ethnicity, gender, and immigration status, can affect one’s health and the quality of care received (Hernandez & Blazer, 2006). Culture encompasses not only individual beliefs, values, and practices but also broader societal, economic, and political contexts that shape people’s identities, behaviors, and experiences (Ross, 2009). It includes the customs, traditions, languages, arts, and social institutions of a particular group or community, as well as the power dynamics and structural inequalities embedded within these systems (Ross, 2009; Spencer-Oatey & Franklin, 2012). Culture influences how individuals perceive and interact with the world around them, including their access to resources, opportunities, and health care services (Spencer-Oatey & Franklin, 2012; Vaughn et al., 2009). Therefore, understanding culture requires recognizing its multidimensional nature and its impact on various aspects of people’s lives, including health outcomes.
Health care providers are increasingly being urged to adopt culturally sensitive care within rehabilitation services, including occupational therapy, physical therapy, and speech-language pathology (Agner, 2020; Chipps et al., 2008; Evans et al., 2005; Handtke et al., 2019; Hyter & Salas-Provance, 2021; Perrin et al., 2010; Reis et al., 2022; Riquelme, 2007; Vaughn et al., 2022). In this review, we define rehabilitation services as a range of interventions designed to facilitate the recovery, restoration, and enhancement of physical, cognitive, emotional, and functional well-being among individuals who have experienced injury, illness, or disability, such as those found in occupational therapy, physical therapy and speech-language pathology (Kokorelias et al., 2023). Within this definition, rehabilitation practice involves understanding and respecting clients’ diverse needs, including cultural factors that can affect their health and health care (Butler et al., 2016).
The integration of cultural relevance, humility, and competence into health care promotes inclusive and equitable rehabilitation service delivery (Hampton et al., 2017). Cultural relevance refers to the extent to which health care practices and interventions are meaningful and appropriate to the patient’s cultural context (Dutro et al., 2008). This is distinct from cultural competence, which involves acquiring specific knowledge, skills, and attitudes to provide effective care across different cultures. The challenges of cultural competence include the risk of stereotyping and the assumption that one can fully understand another’s culture through training alone (Kleinman & Benson, 2006).
These challenges highlight the need for cultural humility, an approach that emphasizes ongoing self-reflection, lifelong learning, and recognizing the limitations of one’s own cultural understanding (Tervalon & Murray-García, 1998). We define cultural humility as the practice of acknowledging the intricate tapestry of client diversity and recognizing the profound influence of cultural elements on health and health care outcomes (Foronda et al., 2022). This definition encompasses both individual actions and practices as well as the critical role of systems and policies in shaping cultural humility. By integrating these dimensions, we aim to address not only how practitioners engage with diverse populations but also how broader structural factors contribute to effective and inclusive health care. Health care professionals can mitigate negative client experiences and outcomes by engaging in openness to learning about clients’ cultural identities and experiences (Jones et al., 2020). However, to accomplish this, there needs to be greater clarity on what cultural humility entails within the context of rehabilitation services (Singh et al., 2022).
Cultural competence has been recommended for several decades to guide culturally relevant rehabilitation services (Lewis et al., 2009; Montgomery, 2020). Cultural humility is a synergy of behaviors, attitudes, and policies in systems or among professionals that fosters effective work in cross-cultural situations (Greene-Moton & Minkler, 2020). However, some scholars argue that one cannot be completely competent in another’s culture because of its inherent complexity, and, thus, it may not be possible to truly achieve cultural competence (Greene-Moton & Minkler, 2020; Lekas et al., 2020).
Cultural competence and cultural humility both aim to foster a deeper understanding of and respectful engagement with diverse cultural perspectives and experiences (Danso, 2018). The concept of cultural humility was introduced in 1998 to guide culturally relevant care (Tervalon & Murray-García, 1998), which refers to health care practices and services that are tailored to the cultural, social, and linguistic backgrounds of individuals and communities (Tucker et al., 2015). Although cultural competence traditionally focuses on health care providers acquiring a set of skills, knowledge, and attitudes to interact effectively with individuals of diverse races, ethnicities, cultures, socioeconomic statuses, ages, gender identities, sexual orientations, abilities, and geographic locations (Garneau & Pepin, 2015), cultural humility involves an awareness of one’s own biases and a lifelong learning–oriented approach to learning about clients and communities with whom health care providers interact (Agner, 2020). In addition, cultural humility encourages practitioners to recognize, learn, and manage power dynamics with their clients over time, allowing for client-centered care (Agner, 2020; Beagan, 2015).
Although some view cultural competence and humility as complementary and synergistic, others argue that cultural competence is reductive and view culture as stagnant (Isaacson, 2014). Cultural humility is an ongoing practice and mindset (Agner, 2020). It offers the advantage of fostering a deeper understanding of and respect for diverse cultural perspectives, enhancing therapeutic relationships and promoting more effective care delivery (Isaacson, 2014; Paparella-Pitzel et al., 2016; Singh et al., 2022). However, it also poses the challenge of navigating power dynamics and addressing implicit biases, which may require ongoing self-reflection and commitment to personal growth (Gallardo, 2013). By situating cultural humility within the broader context of justice and occupational therapy practice, it is important to consider its benefits and complexities in promoting equity and inclusivity in health care settings.
There has been growing interest in the principles of cultural humility in rehabilitation services (Agner, 2020; Bangs et al., 2022; Brown et al., 2021; Paparella-Pitzel et al., 2016). Occupational therapists, in particular, need to become skilled in working with patients with a range of demographics and identities (Sue et al., 2022). Cultural humility applies well to occupational therapy practice and the holistic approach to client care that occupational therapists use because it can aid in informing the therapeutic process that clients experience (Agner, 2020; Hammell, 2013; Mahoney & Kiraly-Alvarez, 2019; Reberg, 2019). However, occupational therapists need to be aware of and critically reflect on their own implicit biases and engage in dialogue with clients to better understand their unique lenses, experiences, and needs (Reberg, 2019). The 2021 Competencies for Occupational Therapists in Canada stress the vital role of cultural humility, urging therapists to honor clients’ cultural perspectives and lived experiences in their practice (Association of Canadian Occupational Therapy Regulatory Organizations et al., 2021).
Although cultural humility has been well examined by other health care professions (e.g., nursing, public health), understanding of its nuanced implementation in occupational therapy practice is limited (Anderson, 2022; Singh et al., 2022, 2023). Across the rehabilitation professions, there exists a shared commitment to providing patient-centered and culturally relevant care (Reichert et al., 2023). Limited knowledge of cultural humility in occupational therapy practice necessitates exploring shared principles across rehabilitation, enhancing nuanced understanding and application in occupational therapy processes. A review of the published literature on cultural humility in rehabilitation services and its alignment with occupational therapy practice as defined by the Canadian Practice Process Framework (CPPF; Townsend & Polatajko, 2013), an established occupational therapy framework, has the potential to support education, research, and professional practice resources. We chose the CPPF because of its comprehensive and widely recognized structure, which encompasses various stages of occupational therapy practice, including assessment, intervention, and evaluation. Its principles, which emphasize client-centered care, collaboration, and evidence-based practice, are applicable across various rehabilitation professions. By using the CPPF, we aimed to provide a structured and holistic examination of cultural humility practices, allowing for the exploration of the CPPF’s integration at different points in the occupational therapy process. These outcomes may further promote culturally humble care, align with professional standards, and enhance client-centered health care, ultimately contributing to improvement in the health and well-being outcomes of patients representing a range of demographics and identities.
Method
This article presents a substudy of a larger scoping review conducted of the existing health services literature on cultural humility (Singh et al., 2022). The protocol for the larger review has been published to ensure our review methodology was transparent. However, given the extent of the literature found in our database search and the opportunity to look more closely at occupational therapy practice, we report on the extent and nature of published literature on cultural humility in rehabilitation services as a separate study. Deviations from the protocol (Singh et al., 2022) that are specific to this substudy are outlined. The results of the larger scoping review will be published elsewhere. We present a brief overview of our methods, following the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al., 2018).
Step 1: Identifying the Research Question
In this article, our emphasis is on the specific findings related to occupational therapy. We identified three research questions for this substudy: What is the extent and nature of the published literature on the practice of cultural humility in rehabilitation services? Based on practitioner data, what recommendations have researchers made for the practice of cultural humility in rehabilitation? How do the key concepts, descriptions, definitions, and recommendations related to the practice of cultural humility align with occupational therapy practice as defined by the CPPF?
Step 2: Identifying Relevant Studies
A medical information specialist from the University of Toronto created a preliminary search strategy based on the inclusion criteria to identify relevant peer-reviewed studies on cultural humility. The larger study included all articles related to cultural humility and health care, including health education and training articles. In the subset analysis, the exploration of cultural humility was conducted across articles within specific thematic focuses across various health settings, encompassing but not confined to occupational therapy, physical therapy, and speech-language pathology. The database search did not apply design, date, or language limitations but focused on peer-reviewed literature.
Before implementing the search strategy in several databases, it was peer reviewed to correspond with the Peer Review of Electronic Search Strategies guidelines (McGowan et al., 2016); no changes were made as a result of the peer review (see Appendix A in the Supplemental Material, available online with this article at https://research.aota.org/ajot). The information specialist translated and ran the search in Ovid MEDLINE, Ovid Embase, Ovid PsycINFO, EBSCO CINAHL Plus, ProQuest ASSIA, ProQuest Sociological Abstracts, ProQuest ERIC, and WOS conference proceedings. The results of the review were supplemented with bidirectional citation searching (i.e., forward and backward screening) of included articles (Hinde & Spackman, 2015) and hand searching for articles in Google Scholar (first 200 pages) and related journals (American Journal of Occupational Therapy, Archives of Physical Medicine and Rehabilitation, Disability and Rehabilitation, Journal of Rehabilitation Medicine, American Journal of Physical Medicine and Rehabilitation, Clinical Rehabilitation, and Journal of Occupational Rehabilitation).
Step 3: Study Selection
The results of the database literature search were deduplicated using reference management and systematic review management software (EndNote and Covidence; Bramer et al., 2016). After the elimination of duplicate articles, the titles and abstracts of the retrieved articles underwent additional deduplication and screening for inclusion using Covidence (Babineau, 2014). To be included in this substudy, studies had to have a primary objective of defining, discussing, debating, or testing the concept of cultural humility in the context of rehabilitation services (i.e., occupational therapy, physical therapy, or speech-language pathology). The determination of whether an article was focused on cultural humility within this context was based on the primary objective and content of the study as outlined in the title, abstract, and full text. Studies that focused on education in cultural humility were not included in this substudy because our sole focus was the practice of the concept in rehabilitation. We incorporated studies that included rehabilitation areas outside of occupational therapy, physical therapy, and speech-language pathology as long as they included at least one of these three core professions. There were no restrictions regarding the population’s demographics, age, health status, or gender. Each article was assessed by two reviewers (from among Kristina M. Kokorelias, Vania Wu, Meena Ramachandran, and Hardeep Singh; Level 1 screening) and full-text screening (Level 2 screening) for eligibility using the aforementioned criteria. A third reviewer (Heather Colquhoun or Hardeep Singh) and team discussion were used to resolve any disagreement (i.e., study eligibility).
Step 4: Charting the Data
The research team developed an a priori data-charting guide and form on Covidence that was used during literature extraction. The chart was used to log study descriptors from the relevant literature to answer the research question, such as study characteristics, sample characteristics, practice context, study aims, methodology, key findings, and aspects of cultural humility (Singh et al., 2022). To ensure the a priori data-charting form was effective, pairs of researchers (Kokorelias, Wu, an occupational therapy student, and Singh) independently trialed the form by extracting data from a subset of the included articles (i.e., 5–10 articles; Levac et al., 2010). Their extractions were subsequently compared (Levac et al., 2010), and the form was continuously updated to most accurately reflect the research questions of the substudy.
Step 5: Collating, Summarizing, and Reporting Results
The research team initially conducted a detailed analysis of the extracted data, examining various aspects of and identifying key findings related to cultural humility through a series of team meetings and discussion. The research team used the extracted data to map the findings on cultural humility onto the CPPF to better comprehend its application and utility within occupational therapy clinical practice interactions (Townsend & Polatajko, 2013). Mapping refers to the process of aligning extracted data with each stage of the occupational therapy practice process and the social and practice context in which practice occurs. The CPPF was selected because it guides the occupational therapy practice process (Fazio et al., 2008), enabling a dynamic incorporation and adaptation of cultural humility practices across various action points of occupational therapy practice (Singh et al., 2022). Moreover, the research team explored the elements of cultural humility by deductively coding the data on the basis of the definition created by Tervalon and Murray-García (1998).
Articles were numbered, described, and summarized on the basis of study descriptors, clinical practice recommendations, and limitations using the a priori data chart. To apply the extracted data related to practice recommendations to the CPPF, studies were uploaded onto a qualitative analysis software (NVivo, Version 12; Dhakal, 2022) and reviewed and deductively coded using a content analysis approach (Bengtsson, 2016). Each component of the CPPF had a unique code to denote the relevant descriptors that aligned with it (see Appendix B in the Supplemental Material). For example, any text related to actions (e.g., obtaining consent for occupational therapy services, identifying occupational challenges) conducted during the first action point (i.e., “enter/initiate”) was coded as 1. Data that did not align with the CPPF were not coded. Researchers independently reviewed and coded the relevant information (Bengtsson, 2016; see Appendix C in the Supplemental Material). Coding schemes were reviewed at research team discussions and presented to the team for agreement after a review of uncertainties.
Results
Duplicates were first removed. Next, we used a stepped screening approach in which articles were initially excluded if they did not specifically include the term cultural humility, with 1,123 studies advancing to title and abstract screening and 855 studies graduating to full-text review. During the full-text review stage, we further assessed articles for inclusion on the basis of their relevance to rehabilitation because we noticed a significant number of relevant articles at this stage. Studies that did not have a primary objective of defining, discussing, debating, or testing the concept of cultural humility in the context of rehabilitation services were excluded. Two additional studies were identified through the supplemental searching techniques (i.e., hand searching, forward and backward citation searching; see Figure 1 for the PRISMA flow diagram). In total, 11 studies were analyzed and included in this scoping review (see Appendix D in the Supplemental Material for study details).
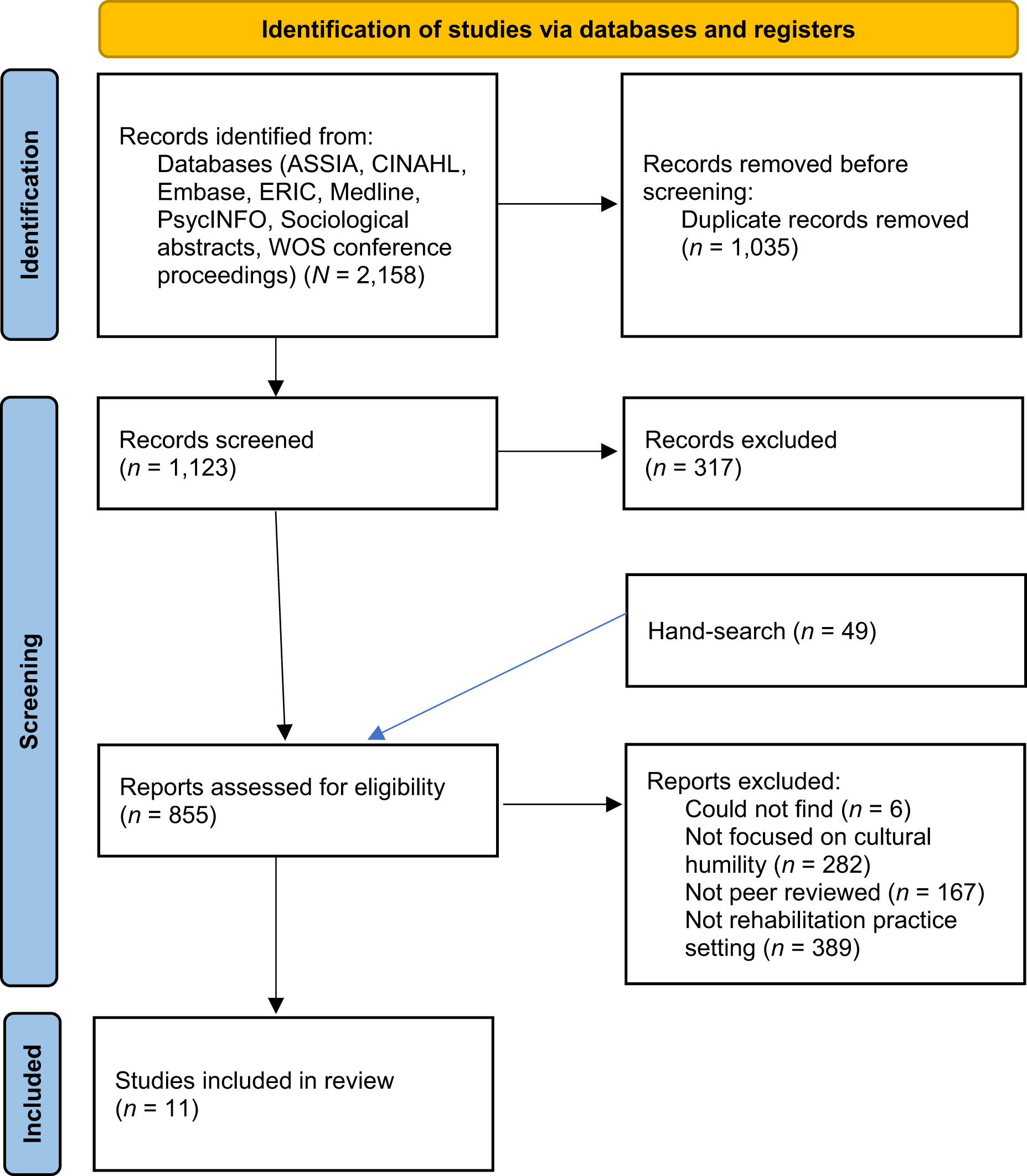
Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram for new systematic reviews that included searches of databases and registers only.
Study Characteristics
Approximately half of the 11 articles were commentary or opinion articles (n = 6; 54.5%). Most studies were published between 2020 and 2021 (n = 5; 45.4%), with others published between 2012 and 2017 (n = 4; 36.4%) or 2022 and 2023 (n = 2; 18.2%). The articles were published in the United States (n = 6; 54.5%), Canada (n = 4; 36.4%), and United Kingdom (n = 1; 9.1%). Practice settings across the 11 articles included palliative and hospice care, dysphagia management, pain management, and global health involvement. Four articles (36.4%) had the stated focus on occupational therapy, 4 (36.4%) focused on physical therapy, and 2 (18.2%) focused on speech-language pathology. One study (9.1%) focused on eight areas of rehabilitation: audiology, occupational therapy, physical therapy, rehabilitation medicine, psychology, prosthetics and orthotics, rehabilitation nursing, and speech-language pathology.
Key Concepts, Descriptions, Definitions, and Recommendations for the Practice of Cultural Humility
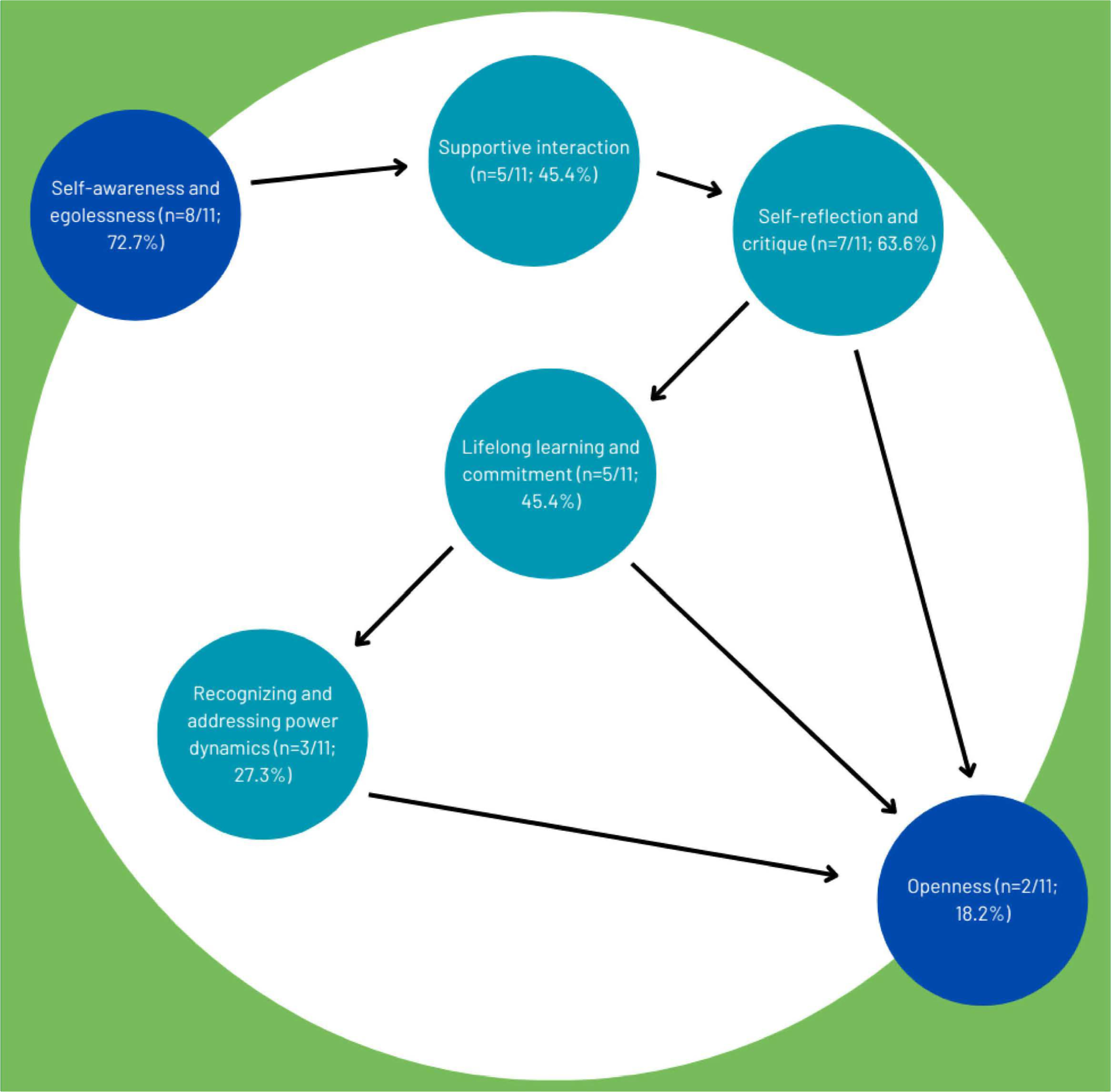
The description of the shared components of cultural humility presented here related to the definition created by Tervalon and Murray-García (1998), resulting in six interrelated concepts and recommendations described in Table 1. All elements were discussed in at least two of the included studies. It is important to acknowledge that some of these elements may overlap or share common aspects. Recognizing this overlap is crucial because it underscores the complexity and interrelated nature of the cultural humility concepts. This understanding helps in critically evaluating how these elements are applied and interpreted, ensuring a more precise and effective application of cultural humility strategies in practice. At the same time, nuances exist. For example, Element 3 centers on self-reflection regarding personal attitudes and beliefs, and Element 6 emphasizes a willingness to engage with and learn about biases, including systemic issues, thereby highlighting the distinct yet interconnected nature of these concepts in our analysis.
Cultural Humility Practices Discussed in the 11 Studies (Informed by Tervalon & Murray-García, 1998)
Element 1: Self-Awareness and Egolessness
Self-awareness and egolessness involves recognizing one’s own cultural biases, privileges, and limitations and being willing to set aside preconceived notions or assumptions in interactions with others (Tervalon & Murray-García, 1998). This element was discussed the most in the included studies (n = 8; 72.7%) and was described as acknowledging one’s privilege, knowledge, and advantages as a professional and how one’s thought processes are a product of one’s history and the values promoted in society. Therapists should acknowledge their limited perspective, emphasizing self-awareness in understanding cultural roles. Cultural humility, as noted in the studies, entails actively integrating diverse perspectives to foster genuine and respectful connections in the client–therapist relationship.
Element 2: Supportive Interaction
Another element of cultural humility discussed was supportive interaction (n = 5; 45.4%), which refers to engaging with others in a manner that demonstrates respect, empathy, and openness (Tervalon & Murray-García, 1998). Included studies described supportive interactions as relinquishing the role of the expert to the client to create client–therapist relationships that were mutually beneficial and nonpaternalistic. Authors noted that therapists should respect their clients’ desires and needs rather than imposing their desires for them; this can open up opportunities and solutions that are not readily apparent.
Element 3: Self-Reflection and Critique
Self-reflection and critique entails regularly examining one’s own attitudes, beliefs, and behaviors, particularly in relation to cultural diversity and equity (Tervalon & Murray-García, 1998). This element was discussed in seven studies (63.6%) and was described as critically examining and reflecting on one’s beliefs, biases, and actions.
Element 4: Lifelong Learning and Commitment
Lifelong learning from clients, colleagues, communities, and oneself and commitment to developing an awareness of cultural differences and inequalities were discussed in five studies (45.5%). This element emphasizes the importance of ongoing education and self-development in understanding and addressing cultural differences and inequalities (Tervalon & Murray-García, 1998). It involves actively seeking out opportunities to learn from diverse sources, including clients, colleagues, communities, and personal experiences and incorporating this knowledge into one’s practice (Tervalon & Murray-García, 1998).
Element 5: Recognizing and Addressing Power Dynamics
Recognizing and addressing power dynamics involves acknowledging the unequal distribution of power and privilege within social interactions and institutions, particularly in relation to cultural diversity (Tervalon & Murray-García, 1998) and was one of the two least-discussed elements (n = 3; 27.3%). Studies described the importance of identifying the possible power dynamics in the client–therapist relationship and in the therapist’s workplace that could contribute to health disparities.
Element 6: Openness
Openness to learning about one’s own biases, racism, and blind spots was the other least-discussed element (n = 2; 18.2%). It refers to maintaining an open mind and willingness to engage with diverse perspectives, experiences, and ways of knowing (Tervalon & Murray-García, 1998).
Recommendations Related to the Practice of Cultural Humility as Defined by the CPPF
We identified recommendations for both societal and practice contexts, as well as frames of reference within the practice of cultural humility, following the CPPF structure (see Figure 2; Fazio et al., 2008). Supporting data and examples are listed in Table 2. Through the mapping process, we found that the majority of studies discussed cultural humility practices relating to the societal (n = 11; 100%) and practice (n = 10; 90.9%) contexts of the CPPF. Expanding beyond the client–therapist dynamic, practice recommendations in the studies emphasized therapists’ societal understanding of cultural humility. This includes acquiring knowledge of current practices and issues and maintaining critical reflexivity. As described in the included studies, the practice context involved both the therapist’s and the client’s personal and environmental factors.
Findings related to the Canadian Practice Process Framework structure.
Findings Related to Cultural Humility Practices Identified in the Included Studies Mapped to Occupational Therapy Practice Using the CPPF
Note. CPPF = Canadian Practice Process Framework.
Practice recommendations pertaining to CPPF that were less represented in the studies included Action Point 1 (enter and initiate; n = 2; 18.2%), Action Point 2 (set the stage; n = 4; 36.4%), Action Point 5 (implement the plan; n = 3; 27.3%), Action Point 6 (monitor and modify; n = 1; 9.1%), and frames of reference (n = 3; 27.3%), each of which was discussed in fewer than 40% of the included studies. CPPF Action Points 3 (assess and evaluate; n = 6; 54.5%) and 4 (agree on objectives and plan; n = 4; 36.4%) were discussed moderately, with more than 40% of studies providing cultural humility practice recommendations for these action points.
In cultural humility’s practical application, therapists, as noted in the studies, entered and initiated by reviewing the client’s history, avoiding assumptions, and ensuring effective communication for shared decision-making and obtaining consent (Barnes et al., 2020; Leslie et al., 2021). The studies described the practice of cultural humility in Action Point 2 (set the stage) as effective communication; the therapist’s attitude when interacting with clients; and involving the family when discussing the client’s cultural background, goals, and preferences for making clinical decisions and involvement in the client’s care (Bangs et al., 2022; Hall & Johnson, 2020; Leslie et al., 2021). For CPPF Action Points 3 (assess and evaluate) and 4 (agree on objectives and plan), the studies described the practice of cultural humility as a collaboration between the client and therapist to determine the client’s goals and interventions on the basis of in-depth assessments of the client (i.e., person, environment, occupation; Townsend & Polatajko, 2013) and person-centered communication during assessments (e.g., asking open-ended questions, addressing how systemic pressure affects the client, and active listening). Some studies (Agner, 2020; Bangs et al., 2022; Bostick et al., 2021; Hall & Johnson, 2020; Leslie et al., 2021) emphasized the importance of therapists adopting sensitive attitudes. Some studies described the practice of cultural humility in Action Point 4 as related to clinical reasoning and decision-making (e.g., creating nonpaternalistic solutions that may not be apparent by engaging in cultural humility, considering nurturing and passive treatment rather than prioritizing independence and autonomy, coming to a compromise with the client and family when making decisions; Bostick et al., 2021; Cleaver et al., 2016; Hall & Johnson, 2020; Leslie et al., 2021). In addition, the practice of cultural humility described in the studies acknowledged the importance of involving the family in the decision-making process and promotion of treatment adherence (Leslie et al., 2021).
For Action Point 5 (implement the plan), studies described the practice of cultural humility as involving family and incorporating cultural factors into the intervention, such as integrating the client’s cultural values, beliefs, and traditional ideas about wellness and addressing barriers to communication, all of which can affect participation and engagement (Bangs et al., 2022; Bostick et al., 2021).
One study (Bostick et al., 2021) described the practice of cultural humility in Action Point 6 (monitor and modify) as checking in often on the client’s progress, reassessing, and making changes to the intervention as needed. No data from the included studies pertained to Action Points 7 (evaluate outcome) and 8 (conclude and exit).
Frames of reference related to the practice of cultural humility that were discussed in the included studies included considering culture within models of occupation, cultural processes and the influence they have on illness and health, challenging dominant models that depict cultural environments as external to and divisible from the person, and discussing occupational therapy using a justice lens (Aldrich et al., 2017; Hammell, 2013; Leslie et al., 2021).
Discussion
This scoping review aimed to provide a comprehensive synthesis of the peer-reviewed rehabilitation services literature on the practice of cultural humility and to align these findings to occupational therapy practice using the CPPF. In total, the review included 11 articles. We identified several elements that inform the definition of cultural humility in the context of rehabilitation services. Moreover, we identified only six of the eight action points, societal and practice contexts, and frames of reference components of the CPPF. In light of our findings, it is evident that integrating cultural humility into CPPF Action Points 7 and 8 is crucial to assessing and concluding therapeutic relationships in a culturally relevant manner. Interestingly, Element 5, which addresses broader systemic and structural injustices, was less frequently discussed in the articles. This finding highlights a potential limitation in the practical application of the framework, in which individual-level interactions are prioritized over confronting systemic issues. This observation aligns with our broader critique of the framework, suggesting that although individual self-reflection is crucial, it cannot be fully effective without addressing the structural forces that shape inequities in health care. By considering and incorporating cultural humility, occupational therapists can ensure that outcomes are evaluated and therapeutic relationships are concluded in a manner that respects and embraces the diversity of clients’ cultural backgrounds and experiences.
In our examination, we found that discussions of cultural humility predominantly focused on elements such as self-awareness, supportive interaction, and self-reflection. Conversely, less attention was given to aspects such as lifelong learning, commitment, recognizing and addressing power dynamics, and openness. Our review suggests that cultural humility entails recognizing one’s privilege, knowledge, and advantages as a professional while also acknowledging the influence of personal history and societal values on one’s perspectives. Cultural humility emphasizes self-awareness (Barnes et al., 2020; Beagan & Chacala, 2012; Beamish et al., 2024; Hammell, 2013), openness to diverse perspectives, and the acknowledgment of not being all-knowing (Aldrich et al., 2017; Cleaver et al., 2016; Hammell, 2013; Leslie et al., 2021). Many studies in the health care literature, including those beyond the scope of rehabilitation, corroborate our finding that cultural humility encompasses both an awareness of cultural differences and a recognition of the limits of one’s understanding of another culture (Agner, 2020; Ahmed et al., 2018; Campinha-Bacote, 2019; Hilty et al., 2021; Hook et al., 2013). Because cultural humility is being adopted by several health disciplines, short-term, immediate recommendations may involve allowing for time in scheduling to allow the clinician to partake in active listening that prioritizes clients’ stories and concerns, fostering a culture that values linguistic and cultural diversity through use of interpreters (Butow et al., 2011), and mandating the development of culturally tailored care plans that respect clients’ values and identities (Torres-Ruiz et al., 2018). These recommendations point to the necessity for system-level changes that would yield benefits not only for occupational therapists but also for other rehabilitation professionals. We also recognize that our study findings could contribute to a continuum of education on cultural humility for occupational therapy students and practitioners. The conclusions drawn from our study may inform educational approaches aimed at integrating cultural humility into clinical practice.
As conceptualized by Tervalon and Murray-García (1998), cultural humility has evolved significantly in its application to occupational therapy practice. Although their core principles of self-reflection, addressing power imbalances, and lifelong learning remain relevant, the occupational therapy context necessitates some adaptations (Anderson, 2022). Recent scholarship has expanded on these ideas, emphasizing the need for occupational therapists to critically examine their own cultural assumptions and biases within the specific framework of occupation-based practice (Agner, 2020). Furthermore, the field has moved beyond simply acknowledging power differentials to actively working to dismantle them through client-centered goal setting and intervention planning (Greene-Moton & Minkler, 2020). Current understandings of cultural humility in occupational therapy also place greater emphasis on the therapist’s role in advocating for systemic change to address health disparities, going beyond the individual patient–provider interaction that Tervalon and Murray-García (1998) initially focused on (Lekas et al., 2020). This evolution reflects occupational therapy’s holistic view of health and well-being, as well as its commitment to social justice and equity in health care delivery.
Our review revealed a significant gap in the identification of cultural humility practices aligning with the CPPF Action Points 7 (evaluate outcomes) and 8 (conclude and exit). Integrating cultural humility within these action points is key to assessing and concluding therapeutic relationships in a culturally relevant manner. As research has ascertained, cultural factors can significantly influence how people perceive and measure success (Chipulu et al., 2014), and, without a culturally humble approach, there is a risk of misinterpreting or undervaluing the outcomes from the client’s perspective (Choe et al., 2023; Sandage et al., 2016). Moreover, cultural factors can influence how individuals approach, perceive, and expect the conclusion of therapeutic interventions (Comas-Díaz, 2006). A culturally humble approach ensures that the decision-making process respects and integrates diverse cultural perspectives, fostering a more respectful and effective conclusion to the therapeutic relationship. By considering and incorporating cultural humility, occupational therapists can ensure that outcomes are evaluated and therapeutic relationships are concluded in a manner that respects and embraces the diversity of clients’ cultural backgrounds and experiences.
In recognizing the limitations of assuming that individual actions alone, such as incorporating cultural humility, can fully address systemic barriers in health care systems, it is imperative to acknowledge and address broader institutional policies, funding structures, and societal factors that contribute to disparities in health care access and delivery. Although cultural humility may support more effective therapeutic relationships and improve outcomes on an individual level, it is imperative to recognize that it alone is not a sufficient response to address ingrained sociocultural structures of inequity (Alegría et al., 2010). These structures encompass systemic biases, discriminatory policies, unequal access to resources, and historical injustices that disproportionately affect marginalized communities (Alegría et al., 2010; Egede et al., 2024). Although cultural humility can facilitate more equitable interactions in therapeutic settings, it does not address the root causes of these structural inequities. Instead, policy should, for example, promote equity in health care access, such as expanding Medicaid coverage (Artiga et al., 2015), implementing antidiscrimination laws, and ensuring culturally competent care standards (Anderson et al., 2003).
Although improvement in cultural humility may be a difficult concept to measure through empirical means (Foronda et al., 2018), researchers have suggested that the process of developing cultural humility can be characterized by a transformation in attitudes, beliefs, and behaviors (Patallo, 2019). In the context of rehabilitation practice, a pragmatic approach to evaluating the ongoing development of cultural humility could involve mixed-methods research designs that combine qualitative approaches, such as in-depth interviews and participant observations, with quantitative self-assessment tools, such as the Cultural Humility Scale (Gonzalez et al., 2021) or the Intercultural Development Inventory (Hammer et al., 2003). Longitudinal studies that track changes in cultural humility can provide a nuanced understanding of its developmental trajectory across providers’ careers (Choe et al., 2023). In the context of occupational therapy, the use of standardized measures for cultural humility can serve as a valuable tool to assess the adoption of cultural humility practices. However, it is essential to emphasize that for this approach to be effective, occupational therapists must thoroughly comprehend the concept and be genuinely committed to its significance (Piernik-Yoder & Beck, 2012).
In keeping with the CPPF, we found that the available literature was most abundant in the context of recommendations regarding the societal and practice contexts of the CPPF, rather than a single stage of the process. This emphasis underscores the intricate nature of cultural humility’s integration and the challenge of isolating discrete recommendations tailored to distinct therapeutic stages (Tervalon & Murray-García, 1998). The ethos of cultural humility asserts a continuous learning trajectory that permeates every facet of therapeutic engagement—before, during, and after the therapeutic process (Tervalon & Murray-García, 1998). As such, each therapeutic stage requires attention to culture, because cultural humility’s essence lies in its perpetual relevance across all action points of therapeutic processes. Although the CPPF presents a valuable foundation for comprehending how cultural humility is currently operationalized in existing occupational therapy practice frameworks, it might be helpful to support its integration in other practice models commonly used by occupational therapists worldwide.
The intercultural caring abductive model emphasizes community and family involvement and describes caring and culture across three dimensions: ontology, phenomenon, and care activities (Wikberg & Eriksson, 2008). Similar to relational definitions of cultural humility, the model emphasizes that caring occurs within the clinician–client relationship, influenced by both parties’ cultural backgrounds and the client’s family (Haora, 2020; Listerfelt et al., 2019; Wikberg & Eriksson, 2008). This alignment suggests that occupational therapists could draw from the model’s perspective to effectively craft interventions that align with clients’ experiential understanding of care, ensuring meaningful and culturally relevant engagement. Furthermore, the focus on care activities highlights the concrete actions that facilitate care delivery (Wikberg & Eriksson, 2008). Recent studies have highlighted the importance of family-centered care and inclusive care in the context of cultural humility (Lechner et al., 2024; Parente et al., 2023). Therapists can draw parallels between this dimension and the inclusive approach of family-centered care, acknowledging the impact of cultural beliefs and expectations on care interpretation while also recognizing variations in power dynamics. Data from our review focusing on family involvement addressed multiple action points of the CPPF, including Action Points 2 (set the stage), 4 (agree on objectives and plan), and 5 (implement the plan). This finding suggests the possibility of incorporating the intercultural caring abductive model and other family-centered occupational therapy models with cultural humility practices into clinical practice to meaningfully involve the family in the therapeutic process. For example, occupational therapists should consider drawing parallels between the inclusive approach of family-centered care and cultural humility, recognizing that the family’s cultural beliefs and expectations significantly influence their interpretation of care activities. Moreover, by recognizing the family’s cultural background, values, and contributions, occupational therapists can create a holistic care plan that extends beyond the individual client to encompass the broader support network.
Strengths and Limitations
This study involved a rigorous search of the literature for relevant studies, including having a medical librarian search several databases. The large research team involved in conducting this study had a diverse range of experiences, cultures, ethnicities, ages, and educational backgrounds. Thus, the analysis and findings of this scoping review were enriched through rigorous peer review and conversations among the research team.
Rather than aiming to search and analyze all health literature, we focused on rehabilitation practice settings. One limitation of our study is the narrow focus on core rehabilitation services, namely occupational therapy, physical therapy, and speech-language pathology, which may have excluded valuable insights from related but noncore rehabilitation services. Another limitation of this study is the potential lack of generalizability of our findings to the broader field of occupational therapy because of the inclusion of articles from other rehabilitation services.
During coding, interpretation issues were resolved in regular team meetings, preventing the exclusion of relevant studies. Studies equating cultural humility with competence were excluded to maintain the study’s cultural humility focus. There is a possibility that pertinent studies were missed because our research team determined whether articles were focused on cultural humility, potentially leading to the exclusion of relevant research.
Data that did not align with the CPPF were not coded for inclusion in the analysis. However, we recognize the importance of thoroughly examining all data and will conduct further analysis to explore any insights that may inform the refinement of the CPPF or suggest areas for future study. Future research should consider evaluating different frameworks and models to assess their applicability in capturing the full scope of cultural humility in rehabilitation practice. Future research should also involve a more detailed exploration of how cultural humility can be incorporated into Action Steps 7 and 8. Although the CPPF was selected for its relevance to rehabilitation practice settings, some literature may have been better captured by alternative frameworks that may offer a more comprehensive understanding of cultural humility. Specifically, the lack of literature related to CPPF Action Steps 7 and 8 suggests that these steps may not fully align with or address the complexities of cultural humility as discussed in the broader literature. This could indicate a need to explore other models that might provide a more nuanced view and better capture the diverse aspects of cultural humility. Another area of future research is to examine studies related to cultural humility education. Early in the screening process, the research team identified an overwhelming number of articles that exceeded the scope of analysis for a single article; thus, we decided to focus this substudy solely on rehabilitation service practice-related articles. It is important to capture not only how cultural humility is practiced but also how it is integrated into the education of the next generation of therapists.
Implications for Occupational Therapy Practice
The findings of this review highlight the importance of integrating cultural humility into occupational therapy practice to enhance client-centered care and align with professional standards, particularly through the lens of the CPPF. The review has the following implications for occupational therapy practice: ▪ By emphasizing self-awareness, supportive interactions, and reflective practice, occupational therapists can foster respectful and collaborative therapeutic relationships. This includes acknowledging and addressing power imbalances, incorporating clients’ cultural values and beliefs into care plans, and adopting lifelong learning approaches to better understand cultural diversity. ▪ Additionally, the findings underscore the need to integrate cultural humility into underrepresented areas of the CPPF, such as evaluating outcomes and concluding therapeutic relationships, to ensure culturally relevant practices across all stages of care. These insights can guide the development of educational and practice resources, ultimately contributing to improved health outcomes for diverse client populations.
Conclusion
This scoping review aligns cultural humility practice recommendations with an established occupational therapy framework, offering valuable guidance for occupational therapy clinicians and researchers. Cultural humility should permeate occupational therapy practice, enhancing service quality, cross-cultural interactions, and client outcomes through shared research and knowledge development.
Supplemental Material
Supplementary material for Cultural Humility Practices in Occupational Therapy Services: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050738.pdf for Cultural Humility Practices in Occupational Therapy Services: A Scoping Review by Kristina M. Kokorelias, Vania Wu, Heather Colquhoun, Ruheena Sangrar, Sachindri Wijekoon, Michelle L. A. Nelson, Holly Assaf, Meena Ramachandran and Hardeep Singh in The American Journal of Occupational Therapy
Footnotes
*Indicates studies included in the scoping review.
Acknowledgments
We acknowledge Erica Nekolaichuk for her assistance with the search.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.