
Abstract
The inclusion of medical improvisation in occupational therapy education can better prepare students to build and maintain therapeutic relationships.
Effective use of interpersonal communication skills such as empathy, adaptability, and collaboration within client–practitioner relationships results in improved health care outcomes for clients and their families (Paterick et al., 2017; Yazdani et al., 2021). The application of these skills is considered therapeutic use of self, a pillar of occupational therapy practice and a required competency for occupational therapy program completion (American Occupational Therapy Association [AOTA], 2020). The Accreditation Council for Occupational Therapy Education (ACOTE®; 2018) Standards and Interpretive Guide (2018) requires students to “(d)emonstrate therapeutic use of self, including one’s personality, insights, perceptions, and judgments, as part of the therapeutic process in both individual and group interaction” (B.4.1l; ACOTE, 2018). Many educational institutions for health professions have adopted a training approach that utilizes the principles and exercises of improvisational theater, termed medical improv, to enhance professional competencies such as communication, empathy, and team building, with promising results (Fessell et al., 2020; Gao et al., 2019). No known studies exist that examine the use of medical improv in building the therapeutic use of self in occupational therapy students.
Medical Improv
Medical improv was introduced to health professions education as a novel way to address communication and interpersonal skills. This approach works to build interpersonal competencies by helping medical professionals develop the ability to listen closely to patients, focus on lived experiences and present circumstances, accept others’ ideas, and support one another through practice (Gao et al., 2019; Mehta et al., 2021). Theatrical improvisation involves a predetermined structure or foundational understanding followed by actors working together to react spontaneously and develop a cohesive scene. Typically, occupational therapy practice also follows a predetermined pattern of care with the interpersonal skills of instinct and improvisation guiding frequent adjustments in conscious communication and decision-making (Krusen, 2012).
Medical improv does not create actors of medical professionals but strengthens their abilities to respond to unexpected situations and interact with others who are different from themselves (Mehta et al., 2021). The Alda Center for Communicating Science (Bass, 2016) approach, or the Alda Method, focuses on connecting with and responding to others, knowing your audience and goal, empathy, and clarity. It uses verbal and nonverbal improvisation exercises, role-playing, and storytelling to teach students empathic communication (Kaplan-Liss et al., 2018). Individualized improv exercises are chosen to build awareness of self and others, developing empathy while cementing the ideas of communication, partnership, and connection (Alda, 2017). Gao et al.’s (2019) scoping review on the role of improv in health care identified components of best practice for improv program design: development and facilitation with combined theatrical and health care expertise; creating a safe and low-stakes environment; and using reflection, feedback, and guiding questions to explicitly connect medical improv to clinical practice.
In a recent program evaluation of the Alda Method, Preis et al. (2022) suggest that medical improv can improve communication in patient–practitioner relationships and recommend including occupational and physical therapists in medical improv training to improve communication and health care team cohesion. After the pilot inclusion of medical improv in an occupational therapy seminar, Krusen (2012) identified improvisation as an adaptive skill that blends art and science to meet the demands of dynamic, unpredictable health care environments.
Intentional Relationship Model
The intentional relationship model (IRM; Taylor, 2020) is the central conceptual model for the therapeutic use of self within occupational therapy education and practice and systematically outlines interpersonal aspects of the treatment process (Popova et al., 2022; Yazdani et al., 2021). The IRM suggests that competence in six therapeutic modes—advocating, collaborating, encouraging, empathizing, instructing, and problem-solving—is required for client and family-centered practice (Taylor, 2020). Each mode is a way of interaction, delivered verbally or nonverbally as intentional and dynamic communication guided by client and environmental characteristics (Yazdani et al., 2021). Appropriate mode choice and use involves a therapist’s ability to recognize 12 interpersonal characteristics, such as need for control, capacity for trust, preference for touch, and capacity for reciprocity. The IRM also identifies 11 inevitable interpersonal events, such as expression of strong emotion, power dilemmas, contextual inconsistencies, and boundary testing, which, dependent on the therapist’s appropriate management, may positively or negatively affect the therapeutic relationship (Taylor, 2020). Self-efficacy of therapeutic use of self is shaped by therapists’ perceptions of IRM components: effective therapeutic mode use, recognition of interpersonal characteristics, and management of interpersonal events (Yazdani et al., 2021).
Experiential Learning
This study assesses perceptions of occupational therapy students’ therapeutic use of self within a standardized patient (SP) experience (SPE). SPEs can have a positive effect on occupational therapy students’ performance skills and perceptions of fieldwork readiness (Sakemiller & Toth-Cohen, 2020). Hands-on experiential opportunities, such as SPEs, foster development of critical reasoning and therapeutic communication (Goldbach & Stella, 2017). Experiential learning in addition to academic coursework may combat clinical educator and student concerns with regard to inadequate hands-on experience, communication, and confidence levels in fieldwork students (Goldbach & Stella, 2017; Yazdani et al., 2021). This integration of experiential learning activities can blend academic concepts with the active decision-making required for fieldwork and clinical practice, facilitating competence and confidence. Student confidence in required competencies directly affects performance in clinical practice (Wolden et al., 2019). Application of learning to a real-life context, both within the medical improv intervention and the SP encounter, will support student self-efficacy and fieldwork and career readiness as students rehearse learned skills within a safe, simulated environment.
Purpose
Researchers hypothesized that the addition of medical improv to academic coursework would increase perceptions of occupational therapy students’ therapeutic use of self. A comparison of occupational therapy students randomized into intervention and waitlist control groups provides information about the effect of medical improv on student therapeutic use of self.
Method
Study Design
A randomized controlled waitlist design was used to examine the effect of medical improv on occupational therapy students’ therapeutic use of self. The University of Oklahoma Health Science Center Institutional Review Board approved all study procedures. Participants provided signed informed consent.
The study occurred within an occupational therapy education program. The waitlist design allowed for a comparison of an intervention group and a control group while remaining equitable and ensuring that all participants have the same experiential learning opportunities at different points in the study (Luttenberger et al., 2015; Peters et al., 2022).
Power Analysis
An a priori power analysis was completed using assumptions of effect size and variability reported in a similar study (Hussain et al., 2018). The results indicated that a minimum sample size of 13 participants per group would be required to achieve statistical power.
Procedures
The study was completed in four stages (see Figure 1).
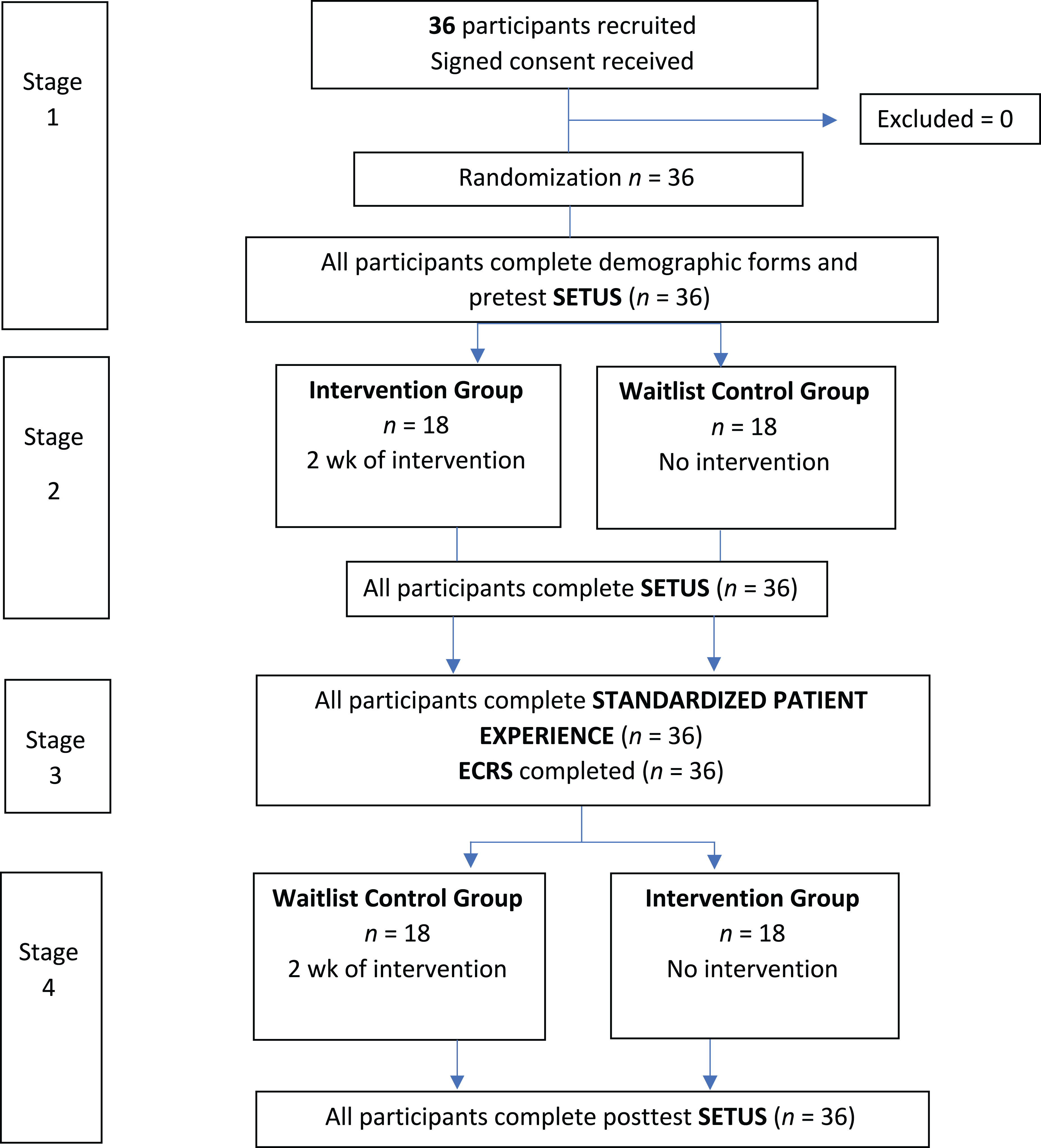
Study stages.
▪ Stage 1: All participants met for the course and study introduction and provided informed consent. A blind randomized block design randomized the cohort into two equal-sized groups.
▪ Stage 2: The 6-wk course required participation in five weekly lectures, 2 consecutive weeks of laboratory, and one SPE. The medical improv intervention served as the laboratory. The intervention group participated in the laboratory during Weeks 2 and 3 of the course.
▪ Stage 3: A family-centered SPE was completed during the fourth week of the course. Participants were provided with a case study of a child who was recently diagnosed with autism, and they were asked to complete an occupational profile with a SP acting as the parent of the child. The participants were blindly randomized to one of six SPs who were blinded to group assignment.
▪ Stage 4: The waitlist group participated in 2 consecutive weeks of 2-hr medical improv exercises. The intervention group met for lecture only.
Participants
A cohort of 36 third-year occupational therapy students were asked to participate in this study. The students varied in age, race, gender, and earned educational level and represent an occupational therapy cohort in the southwestern United States. Each student had previously completed a two-credit intentional relationship course, IRM application within lifespan and practice-setting courses, as well as three Fieldwork I and one 12-wk Fieldwork II experiences.
Intervention
The primary researcher (Cynthia Selim), an occupational therapist and educator with improv experience and training, developed and facilitated the intervention. It was influenced by the Alda Method (Bass, 2016), followed Gao et al.’s (2019) best practice for improv program design, and was guided by a future research recommendation to integrate medical improv into an existing curriculum rather than a stand-alone elective (Fessell et al., 2020).
The intervention consists of two 2-hr sessions of medical improv applied to occupational therapy practice and included four areas of relevant improvisational exercises (Alda, 2017; Kaplan-Liss et al., 2018; Muldoon, 2022). See Table 1 for the medical improv series and the suggested reflection questions. Each exercise required participants to work with a new partner, allowing them to interact with a variety of personalities, comfort zones, and communication preferences. A critical component of the medical improv intervention was the debrief between each exercise. These reflections allowed the facilitator to make explicit connections between an improv exercise and occupational therapy practice.
Medical Improv Series
Note. Improv = improvisation. Potential reflection questions include the following: How did eye contact influence your connection with your partner? What nonverbal communication did you notice? How did this affect your experience? What challenges did you experience? Were you able to overcome them? Which aspects of this exercise applied to therapists? To clients? To families? How did you respond to what your partner was sharing? What did you notice about yourself when you were listening? What insights did you gain about a client’s perspective in therapy?
Outcome Measures
This study assessed outcomes using the Self-Efficacy for Therapeutic Use of Self (SETUS) and the Empathy and Clarity Rating Scale (ECRS).
The SETUS is a self-report questionnaire and includes three scales: Self-Efficacy for Therapeutic Mode Use (SETUS modes), the Self-Efficacy for Recognizing Interpersonal Characteristics (SETUS traits), and the Self-Efficacy for Managing Interpersonal Events (SETUS events). It was found to be valid and reliable with English, Irish, and Norwegian students (Hussain et al., 2018; Yazdani et al., 2021), where each scale was found to be unidimensional, have good internal consistency (Cronbach’s αs of .85, .95, and .96, respectively), and strongly correlated (with rs ranging between .74 and .83; all ps < .001). It includes 29 individual questions with responses scored on a 10-point Likert scale. All participants completed the SETUS as a baseline measurement, before the SPE and after the waitlist intervention.
The ECRS was developed to measure the effectiveness of medical improv on communication and interpersonal skills of health profession students (Terregino et al., 2019). It measures four domains: Fostering Relationship–Supporting Emotion, Gathering Information, Providing Information, and Helping the Patient Make Decisions. Seven areas are scored on a 5-point scale with an option to provide qualitative comments. It has preliminary evidence of validity and reliability, with 84% agreement across raters, intraclass correlation = .53, and internal consistency with a Cronbach’s α of .95 (Terregino et al., 2019). The SP scored each participant after the SPE.
Statistical Methods
Descriptive statistics were computed for all variables of interest. Differences in ECRS scores for each subscale and total score were compared using Wilcoxon rank-sum tests. Differences in SETUS scores during Stage 2 were compared between intervention groups using independent-samples t tests. A mixed between-subjects and within-subject analysis of variance (ANOVA) contained associations between time, intervention group, and the Time × Intervention Group interaction. Last, an exploratory multivariate model was constructed using the SETUS total score to assess any variable that was unbalanced from the randomization process. All statistical tests assumed a 5% chance of a Type 1 error, and SAS, Version 9.4, was used for computations.
Results
Baseline Comparison
The randomization of the intervention and waitlist control groups was balanced in all demographic variables except for race (see Table 2). At baseline, there was no difference between the SETUS mode scores (p = .50), SETUS traits scores (p = .51), or SETUS events scores (p = .90).
Comparison of Descriptive Statistics Between Groups
Note. Approximate age was computed as 2023 − year of birth.
*Computed from Student’s t test; t = 0.25. **Chi-square analysis p value. ***Fisher’s test p value. ****Significant.
Outcomes
Between Groups
Analysis of the ECRS found the scores were heavily skewed to the right, with mean scores of 33.6 (for the intervention group) and 33.3 (for the waitlist control group). The intervention group had slightly higher means in three individual areas and the total score; however, the p values were not significant (see Table 3). Eighteen of the 36 participants received the maximum score.
Wilcoxon Signed-Rank Statistics for ECRS Comparisons Between Intervention Groups
Note. ECRS = Empathy and Clarity Rating Scale.
An independent-samples t test comparing the SETUS scores at Stage 2 revealed a significant difference between the means of the intervention group and the waitlist control group for the SETUS modes score (d = .93, p = .004), the SETUS traits score (d = .57, p = .04), and the SETUS total score (d = .64, p = .03). The SETUS events score (p = .07) was not significant, with a moderate effect size (d = .48; see Table 4).
SETUS Independent Comparison of Means and Effect Size at Stage 2
Note. CI = confidence interval; SETUS = Self-Efficacy for Therapeutic Use of Self.
Significant.
Between and Within Groups
A mixed between-subjects and within-subject ANOVA found a significant interaction effect for the SETUS mode scores between intervention and time (p = .03). From Stage 1 to Stage 2, the intervention group showed a significant 5.3-point change—95% confidence interval (CI) [2.4, 8.2], p < .001—whereas the waitlist control group showed an insignificant 0.9-point change (95% CI [−2.0, 3.7], p = .83). The intervention showed a 4.4-point increase (95% CI [0.4, 8.5], p = .03) in SETUS modes score from Stage 1 to Stage 2, indicating that the medical improv intervention was effective in improving self-efficacy of therapeutic use of self in therapeutic mode use.
The interaction effect of the SETUS total score was trending toward significance, with a p value of .06. From Stage 1 to Stage 2, the intervention group showed a significant SETUS total score change of 28.2 points, 95% CI [15.2, 41.2], p < .001; whereas the waitlist control group showed an insignificant change of 10.7 points, 95% CI [−2.3, 23.7], p = .10. This difference of 17.5 points, 95% CI [−8.5, 31.3], between the intervention and waitlist control groups from Stage 1 to Stage 2 did not reach significance, p = .06. There was also no significant interaction effect for the SETUS traits or SETUS events subtests, ps = .12 and .13, respectively.
There was a significant change within both groups (intervention group and waitlist control group, n = 36) from Stage 1 to Stage 4 (p < .001), showing a significant increase in self-efficacy after intervention in each subtest area (SETUS modes, SETUS traits, SETUS events, and SETUS total scores). The intervention group showed significant change from Stage 1 to Stage 2 in each subtest area (p < .001) and from Stage 1 to Stage 4 (p < .001). The waitlist control group had insignificant change from Stage 1 to Stage 2 (ps = .83, .06, .14, and .10, for SETUS modes, SETUS traits, SETUS events, and SETUS total scores, respectively) and significant change from Stage 1 to Stage 4 (p < .001).
Exploratory Multivariate Model
The only collected demographic that was not balanced by the randomization process was race. This variable was added to a longitudinal multivariate model using SETUS total scores, and a backward selection process was used. The Group × Time × Dichotomous Race interaction (f = 0.15, p = .95), Group × Race interaction (f = 1.01, p = .32), Time × Race interaction (f = 0.31, p = .74), and race (f = 0.29, p = .60) were removed. This result indicates that, although race was not balanced in the randomization process, it was not a factor in SETUS scores.
Discussion
All participants demonstrated a significant increase in self-efficacy of therapeutic use of self after the medical improv intervention. At Stage 2, there was a significant difference between the intervention group and the waitlist control group in the SETUS modes, SETUS traits, and SETUS total score subtests and a significant interaction effect in the SETUS modes subtest. Effect sizes for the SETUS subtests ranged from large to moderate (ds = .93, .57, .48, and .64, for SETUS modes, SETUS traits, SETUS events, and SETUS total scores, respectively). The waitlist control group responded with comparable increases in self-efficacy of therapeutic use of self after their intervention stage of the study. These findings provide the first evidence for the positive effects of medical improv in building self-efficacy of therapeutic use of self in occupational therapy students.
To our knowledge, this is the first study that addresses medical improv using a controlled design. Analysis of the SETUS within-group change only produced outcomes like those of the Hussain et al. (2018) article, the basis for the a priori power analysis. This study produced a positive response to medical improv that was similar to the responses from other health care professions who consider the components of therapeutic use of self as fundamental to their practice (Solman & Clouston, 2016). Obstetrics and gynecology residents (Cai et al., 2019), medical students (Neel et al., 2021), and occupational therapy students in this study demonstrated increased confidence in communication and empathy from pre- to posttest after medical improv intervention. This research further contributes to the body of literature by including increased rigor in study design and application of medical improv to occupational therapy.
The ECRS scores did not show a significant difference between the groups and may have been affected by a ceiling effect and social desirability bias. Because of the generous scoring by the SPs, there was limited room to demonstrate change. The SPs reported that they were “easy graders” and “wanted to help the students feel ready to become OTs.” Future studies could include increased training of SPs to establish interrater reliability or have blinded, trained researchers watch the recording of the experience and score the participants.
The mixed-methods ANOVA identified a significant interaction effect in the SETUS modes scores and not the SETUS traits or events subtests. The participants reported they were most familiar and comfortable with the intentional relationship model (IRM) concept of therapeutic modes. The other components of the IRM—interpersonal characteristics and interpersonal events—were not taught as explicitly throughout the curriculum, and many participants required explanations and practice examples. This may have affected participant perceptions of self-efficacy of interpersonal characteristics and events. An IRM review and the selection of improv exercises targeted toward these components of the IRM model may be helpful in achieving improvements in these areas. A larger sample size may also be beneficial in increasing power in comparisons between groups.
Although 36 may be a relatively small sample size, it represents an entire cohort of occupational therapy students, potentially increasing generalizability to other occupational therapy programs. Participants included students who were intrigued by improv and those who reported that it was well out of their comfort zones. The inclusion of the medical improv intervention within a required course reduced self-selection bias, allowing the researchers to gather data from those who were interested in improv and those who may not have agreed to participate in an external improv study.
The waitlist control group participated in a replication of the intervention, allowing for a comparison of the intervention and waitlist control groups’ response to medical improv intervention. Both groups demonstrated a positive change in self-efficacy of the therapeutic use of self with similar increase in scores. This similarity suggests that the study is reproducible. A manualized intervention may be helpful in supporting successful application of medical improv in educational settings. A medical improv manual could provide structure and procedures that also allow for individualization and student-centered practice (Blanche et al., 2011).
Implications for Occupational Therapy Practice
Therapeutic use of self is a distinguishing feature of occupational therapy, a cornerstone of the occupational therapy process, and integral to occupational therapy outcomes (AOTA, 2020). However, there is limited focus within occupational therapy education and a lack of clarity in its practice (Solman & Clouston, 2016). Medical improv provides an opportunity to increase the emphasis on the development of therapeutic use of self by integrating theory and practical experience. This study has the following implications for occupational therapy practice: ▪ The inclusion of medical improv in required coursework could enhance IRM delivery within occupational therapy programs, supporting ACOTE (2018) Standard B.2.1. ▪ Components of improv, such as connecting with and responding to others, using verbal and nonverbal communication, and making your partner look good (Bass, 2016), complement the IRM and its focus on self-awareness, empathy, intentionality, interpersonal characteristics, and client-centered relationships (Taylor, 2020). ▪ This study also identified IRM content in the occupational therapy program was focused on therapeutic mode use. Educators could utilize medical improv to provide practical exposure to interpersonal characteristics and inevitable interpersonal events to improve student competencies in the recognition and management of IRM components. ▪ Medical improv can support the ACOTE (2018) requirement to demonstrate therapeutic use of self (B.4.1) as students begin to assess, adjust, and modify interactions in a safe and secure environment.
Conclusion
The study findings provide preliminary evidence for the effectiveness of medical improv and suggests that its inclusion in occupational therapy education will support the development of the therapeutic use of self and build the adaptive skills required to provide high-quality health care for clients and their families.
Footnotes
Acknowledgment
We thank Jonathan Baldwin for his statistical assistance and the Midwestern University Class of 2023 for their participation.