
Abstract
The study findings highlight the need for occupational therapists to support families in reducing sensory accommodations while helping children with autism spectrum disorder build independence and coping skills.
Families raising a child with autism spectrum disorder (ASD) often redesign their lives to minimize their child’s distress, which can be triggered by multiple sources, among them sensory overresponsiveness (SOR). SOR is a sensory processing disorder that manifests as atypical, negative reactions to mundane sensory stimuli, such as certain textures, touch, sounds, lights, foods, and odors. It can be idiopathic or occur alongside another developmental disorder. The child often responds to a lower threshold of stimuli with a stronger intensity and for a longer duration than people with typical sensory reactivity. Common reactions consist of avoidance, aggressive behavior, resistance, stress, impulsivity, rigidity, irritability, and anxiety (Miller et al., 2007). SOR is also associated with difficulties in participation in social and academic activities (Ben-Sasson et al., 2009). Children with SOR often avoid or resist performing daily activities that involve bothersome sensations, such as dressing and eating (Reynolds & Lane, 2008).
Studies indicate that individuals with ASD and those with sensory processing disorders have atypical sensory patterns compared with typically developing (TD) individuals (Crasta et al., 2020; Tavassoli et al., 2018). Some research has reported that children with sensory processing disorders (including SOR) had more sensory issues—in specific, they had greater tactile sensitivity compared with children with ASD (Crasta et al., 2020) but less sensitivity to taste and smell (Schoen et al., 2009). Other studies have not reported differences in SOR between these groups (Tavassoli et al., 2018). Hence, we hypothesized that children with ASD or SOR (the clinical groups) would show more SOR symptoms than TD children.
SOR is associated with an increased prevalence of child internalizing symptoms (e.g., anxiety, depression, and withdrawal; Carter et al., 2011) and externalizing symptoms (e.g., hyperactivity, resistance, aggression, and oppositional behaviors; Gunn et al., 2009). There is a clear relationship between SOR and anxiety symptoms in the general pediatric population (Carter et al., 2011; Lane et al., 2012), such as among children seeking outpatient anxiety services (Conelea et al., 2014) and children with ASD (Green et al., 2012; Lane et al., 2012). To control and regulate these emotions, children often use maladaptive strategies that may restrict their own, and their family’s, daily functioning (McMahon et al., 2019).
In addition to disturbing the child’s well-being, SOR limits family participation, creating secondary circles of challenges with ASD (Bagby et al., 2012; Schaaf et al., 2011). SOR contributes immensely to impaired family functioning (Carter et al., 2011) and parental stress (Carter et al., 2011; Gourley et al., 2013). Families of children with SOR report more restrictions in their social activities (e.g., avoiding visiting friends and relatives) and personal lives (e.g., difficulty changing daily routines and excessive parent tiredness) compared with families of TD children (Carter et al., 2011). These restrictions are part of the family’s efforts to control disturbing sensory stimuli and to reduce stress, anxiety, and withdrawal.
When associated with ASD, the impairments related to SOR are even greater and can influence social interactions, environmental exploration, and independence in various daily functions, such as eating, sleep, and play (Schoen et al., 2009). Among children with ASD, elevated SOR symptoms are associated with heightened levels of parental stress (Bagby et al., 2012; Ben-Sasson et al., 2013; Schaaf et al., 2011), psychopathology (Griffin et al., 2022), and restricted family participation in daily activities (Ben-Sasson et al., 2013). Sensory symptoms of children with ASD dictate the family’s choice of whether to participate in or avoid certain activities inside and outside the home (Bagby et al., 2012; Kirby et al., 2019; Schaaf et al., 2011).
Among the responses to a child’s distress is family accommodation. Family accommodation consists of various changes, including making adjustments to a family’s activities and routines, actively participating in the symptoms or rituals characteristic of the disorder, providing assurance, and helping children to avoid related fears (Shimshoni et al., 2019). These accommodations are common among families of children with obsessive–compulsive disorder (OCD) and anxiety disorders and have primarily been studied with populations with these disorders (Lebowitz et al., 2014; Shimshoni et al., 2019). The high levels of anxiety found among both people with SOR and those with ASD suggest that they will similarly lead to family accommodation.
Families naturally aim to reduce both their child’s and their own distress. However, the instinct to implement accommodations that shield the child from stress can fuel a negative cycle of reinforcement, fostering increased reliance on family support and hindering independent coping, ultimately exacerbating symptoms (Kagan et al., 2017; Shimshoni et al., 2019). Adjustments of this type can worsen symptoms and cause a decrease in the child’s general functioning (Lebowitz et al., 2013; Storch et al., 2015).
Families of a child with ASD report a high incidence of family accommodation (e.g., 75.6% of families in Koller et al., 2022 and 97.5% of those in Storch et al., 2015). Family accommodation of children with ASD has been associated with a low response to treatment and impaired self-regulation, difficulties in functioning, and maladaptive behavior (Feldman et al., 2019; Koller et al., 2022; Storch et al., 2015). These accommodations can exacerbate anxiety symptoms (Storch et al., 2015); OCD (Griffiths et al., 2017); disruptive behaviors, such as irritability, hyperactivity, noncompliance, and inappropriate speech (Koller et al., 2022); and repetitive and restricted behaviors and interests (RRBI; Feldman et al., 2019). Note that the RRBI domain in the ASD criteria of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association, 2013) consists of repetitive and restricted speech, movements, rituals, routines, and interests, as well as unusual sensory behaviors. Therefore, the documented family accommodation of RRBI is probably also a factor in unusual sensory behaviors.
Family accommodation, as defined in the mental health literature, consists of responses in which the family cooperates with the child’s anxiety-driven thoughts and behaviors, responses that impede participation and well-being in the long run (Lebowitz et al., 2013). In contrast, in the occupational therapy literature, accommodations are responses enabling participation and are not synonymous with the mental health construct of family accommodation. Occupational therapists often recommend accommodations in family routines, environments, and activities to promote the participation of a child with SOR. Therefore, it is important to emphasize that the types of accommodations deemed family accommodation are those aiming to host the symptoms and alleviate distress (Lebowitz et al., 2013, 2014). Each family should undergo a personalized assessment to determine whether accommodations, including those recommended by providers, exacerbate distress and limit child and family well-being in the long run.
The Family Accommodations Scale for Sensory Over-Responsivity (FASENS; Ben-Sasson et al., 2020) was created on the basis of the strong association between SOR and anxiety (e.g., Green et al., 2012) and parental distress (e.g., Schaaf et al., 2011). As a disorder involving fear, SOR is likely to lead over time to family accommodation, as defined earlier. The FASENS was developed to enable providers’ assessment of family accommodation for children with SOR. The results from this parental questionnaire have confirmed the correspondence between high scores on standardized sensory questionnaires and greater family accommodation (Ben-Sasson et al., 2022, 2025). Children’s SOR and anxiety levels significantly predicted families’ FASENS scores (Ben-Sasson et al., 2025). Compared with families with children who have medical or developmental conditions, families of TD children reported fewer accommodations and greater interference of the accommodations with the well-being of the child and family.
Parental distress tolerance refers to a parent’s ability to persist with goal-oriented activities despite witnessing their child’s distress, especially during stressful tasks (Carpenter et al., 2014; Morford et al., 2017). It affects parents’ self-regulation and influences their child’s development (Morford et al., 2017). Poor parental stress tolerance can limit children’s independence and confidence, decreasing their ability to handle challenges (Firoozi, 2020). Parents with low stress tolerance often resort to accommodations to alleviate stress for themselves and their children (Kagan et al., 2017; Morford et al., 2017; Selles et al., 2018). A few studies have associated high frequency of family accommodation with poor parental distress tolerance both in the general pediatric population and among children with anxiety disorders (Birk et al., 2022; Settipani & Kendall, 2017). Additionally, lower parental stress tolerance is significantly associated with poor outcomes of family accommodation interventions for youth with OCD (Selles et al., 2018). It is likely that parental distress tolerance indirectly influences the relationship between child anxiety symptoms and family accommodation.
The evidence highlights that children with idiopathic SOR or ASD often experience significant sensory challenges that increase their anxiety symptoms and interfere with family dynamics. Research shows that SOR is linked to increased parental stress and family avoidance. Family accommodation for anxiety exacerbates symptoms in the long run and creates greater dependency on external coping. Additionally, parental distress tolerance has been identified as a potential factor influencing the extent of family accommodation. The objective of this study was to characterize family accommodation to sensory sensitivities and its interference with child and family well-being, as reported by families of children with ASD, children with SOR, or TD children. We also examined the associations among the quantity of bothersome sensations, sensory-related family accommodation, and parental distress tolerance. We hypothesized that children with SOR would experience greater family accommodation and that parental stress tolerance would mediate the relationship between the sum of bothersome sensations and family accommodation. The current study is unique in characterizing FASENS scores for distinct clinical groups and in evaluating the contribution of parent-related distress tolerance.
Method
Research Design
This study used a cross-sectional, case-control design involving nonrandomized sampling and a survey methodology. This design is suited to the descriptive inquiries related to the distribution of a relatively new measure in different clinical groups and its association with other constructs.
Participants
Inclusion criteria were as follows: parents of children ages 3 to 13 yr who were living with their child and proficient in Hebrew or Arabic. Children were recruited into one of three groups: ASD, SOR, or TD. The ASD group included children reported by their parents to have an ASD diagnosis and to learn in an educational setting designated for ASD children. For the SOR group, inclusion was based on a Short Sensory Profile 2 (SSP–2; Dunn, 2014) total score 1 or 2 SD above average on both the Sensitivity and the Avoidance subscales or a score 2 SD above average on either of these scales (Little et al., 2017). The TD group included children without (1) SOR on the basis of their SSP–2 scores, (2) ASD or intellectual or developmental disability, (3) genetic syndromes, (4) neuromuscular disorders, (5) psychiatric disorders, or (6) regular medication intake other than Ritalin.
The final sample included 159 mothers with children in one of three groups: ASD, n = 57; SOR, n = 54; and TD, n = 48. See Table 1 for child and family characteristics by group. Groups were matched on age and ethnicity (p > .05).
Child and Family Characteristics
Note. Groups with subscripts a or b were significantly different based on Bonferroni post hoc tests or χ2-adjusted z tests. ASD = autism spectrum disorder; SOR = sensory overresponsiveness; TD = typically developing.
Measures
SSP–2
The SSP–2 is a parental questionnaire that evaluates the frequency of atypical responses to daily sensory stimuli among children ages 3 to 14 yr. The questionnaire includes 34 items rated on a 5-point Likert scale ranging from 1 (never) to 5 (almost always). Items are classified into four subscales: Sensitivity, Avoidance, Seeking, and Low Registration. The Sensitivity and Avoidance subscales are SOR dimensions. Each dimension yields a summary score, with higher scores indicating greater frequency. Cutoffs are applied to compute dimension scores: −2 SD, less than others; −1 to −2 SD, less than others; −1 to 1 SD, like others; 1 SD, more than others; and 1 to 2 SD, more than others.
The SSP–2 has high internal reliability (sensitivity, α = .75; avoidance, α = .83; seeking, α = .69; registration, α = .75) and high convergence validity. In the current study, internal reliability was α = .97 for the total scale, and the Avoidance and Sensitivity scores were strongly correlated (r = .82, p < .001).
Adapted SensOR Inventory
The Adapted SensOR Inventory (Schoen et al., 2008) is intended for use with children ages 3 yr or older. Parents are requested to rate a list of 69 stimuli as bothersome or not to their child (47 stimuli are from the original SensOR Inventory measure). Daily stimuli are grouped by items of clothing, self-care, tactile, visual, smells, sounds, places, and movement. The total SOR score is the sum of the bothersome sensations.
The Adapted SensOR Inventory has good content validity and high discriminant and convergent validity (Schoen et al., 2008). In the current study, internal reliability as measured by Cronbach’s α was high for both the original set of items (α = .94) and for the adapted set of items (α = .91).
FASENS
The FASENS (Ben-Sasson et al., 2020) is a caregiver questionnaire that consists of three scales used to evaluate family members’ behaviors in response to their child’s sensory sensitivities. The first scale includes 12 items asking about the frequency of different types of assistance provided to avoid sensory stimuli, along with changes in family behaviors, activities, and routines (e.g., “How many times have you given your child items that help reduce his/her sensory sensitivity?”). These items are rated as 0 (none), 1 (1–3 times a month), 2 (1–2 times a week), 3 (3–6 times a week), or 4 (daily). The second scale includes two items asking about the emotional impact of accommodating the child’s overresponsivity on parents and family (e.g., “Did you experience distress because of the modifications you made because of your child’s sensory sensitivity?”). The third scale consists of four items asking about the functional and emotional impact on the child (e.g., “Was your child distressed when you did not help in the ways you mentioned?”). Responses to the latter two scales are rated as 0 (no), 1 (mildly), 2 (moderately), 3 (severely), or 4 (extremely). The FASENS is scored as three mean scores: frequency, family impact, and child impact. Higher frequency scores imply engaging in more types of accommodations, more times, or both. Higher family impact or child impact scores imply greater interference with well-being or functioning.
The FASENS was originally based on the Family Accommodation Scale–Anxiety (Lebowitz et al., 2013) and includes similar wording and rating scales. Items were adapted to SOR symptoms and the documented family challenges with them. The FASENS has high content validity; high internal reliability (α = .94); and good discriminant, convergent, and construct validity (Ben-Sasson et al., 2022). In the current study, the FASENS’ internal reliability was α = .93 for frequency of accommodation items and α = 0.93 for child impact and family impact items. For this study, the measure was translated into Arabic using back-translation.
Parental Distress Tolerance Scale
The Parental Distress Tolerance Scale (P–DTS; Pochtar, 2014) is a caregiver questionnaire that evaluates the degree of parent tolerance of the child’s distress. The questionnaire includes 15 items (e.g., “My child’s feelings of distress are so intense that they completely overwhelm me”). Items are rated on a scale ranging from 1 (strongly agree) to 5 (strongly disagree). The scale yields a mean score, with higher scores reflecting higher tolerance. The scale has high internal reliability (α = .92) and good predictive validity relative to dysfunctional parenting (Pochtar, 2014). For this study, the questionnaire was back-translated into Hebrew and Arabic. In the current study, the scale had high internal reliability (α = 0.87).
Background Questionnaire
Parents were asked to provide child and family background information (e.g., mother’s years of education, family ethnicity). Three questions related to ASD severity inquired about (1) educational setting; (2) verbal ability; and (3) level of support needed for functional performance in dressing, eating, and self-hygiene, ranked as independent, partial, or full support.
Procedures
After approval from the Ethics Committee of the University of Haifa, families were recruited for the study. The TD group was recruited through social media and friends and family. The clinical groups were recruited via social media, clinics, and special education settings. Consent and measures were completed online through the Qualtrics platform. Parents could connect to the questionnaires via the link in advertisements and choose whether to complete the internet survey anonymously or not and whether to complete it in Hebrew or Arabic. Parents of children in all groups received a gift card for completing the questionnaire. The mean age and percentage of each ethnicity for each group were monitored, and recruitment efforts were targeted to ensure the groups were matched according to age and ethnicity.
Data Analysis
FASENS scores were not normally distributed, with Kolmogorov–Smirnov tests of p < .06 for most of the scores and groups. P–DTS and total SOR scores were normally distributed (p > .07). FASENS scores were compared among the three groups using Kruskal–Wallis tests, and pairwise comparisons were performed using Mann–Whitney U tests. P–DTS and total SOR scores were compared using a one-way analysis of variance (ANOVA), followed by Bonferroni post hoc tests. Three PROCESS moderation mediation models (Model 8) were conducted for each of the three FASENS scales: Total SOR predicted FASENS score with P–DTS as a mediator, clinical group (i.e., TD vs. ASD+SOR) as a moderator, and mother’s years of education as a covariate. Mother’s years of education was selected as a proxy for socioeconomic status.
Results
Descriptives
See Table 1 for a comparison of groups across demographic variables. ANOVA results showed significant differences in mother’s and father’s years of education, F(2, 150) = 7.58, p < .001, η2 =.08, and F(2, 149) = 7.95, p <.001, η2 =.08, respectively. Bonferroni post hoc tests indicated significantly higher parent education for the TD group relative to both clinical groups (p < .001). Chi-square tests showed significantly different family income levels between groups, χ2(4) = 33.97, p <.001, Cramer’s V = .33. In particular, higher rates of lower income were observed in the clinical groups versus the TD group.
The severity of the SSP–2 SOR scores (sum of Avoidance and Sensitivity) was similar in the clinical groups (ASD, M = 63.70, SD = 15.27; SOR, M = 62.76, SD = 12.0) relative to the TD group (M = 32.81, SD = 9.70), F(2, 156) = 96.50, p <.001. Note that 84.2% of the ASD group met the SSP–2 criteria for the SOR group (see Table 2).
Comparison of Total SOR, FASENS, and P–DTS Scores Between Groups
Note. Groups with superscripts a or b were significantly different from one another. ASD = autism spectrum disorder; FASENS = Family Accommodations Scale for Sensory Over-Responsivity; P–DTS = Parenting Distress Tolerance Scale; SOR = sensory overresponsiveness; TD = typically developing.
Figure 1a presents the percentage of families by group who engaged in FASENS items at least monthly. Figure 1b shows the percentage of families by group who reported moderate to extreme levels of the impact of accommodation on the family, the child, or both. More than 20% of both the ASD and the SOR groups reported engaging weekly in family accommodations (see Figure A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot). In the SOR group, the most common accommodations made at least weekly were assisting activity avoidance (64.9%), providing items (64.8%), and taking actions (55.6%). In the ASD group, accommodations implemented at least weekly included taking actions (56.1%), making schedule modifications (54.4%), and requesting consideration (54.4%). In contrast, the TD group predominantly remained below 4.2% for engaging in an accommodation at least once a week.
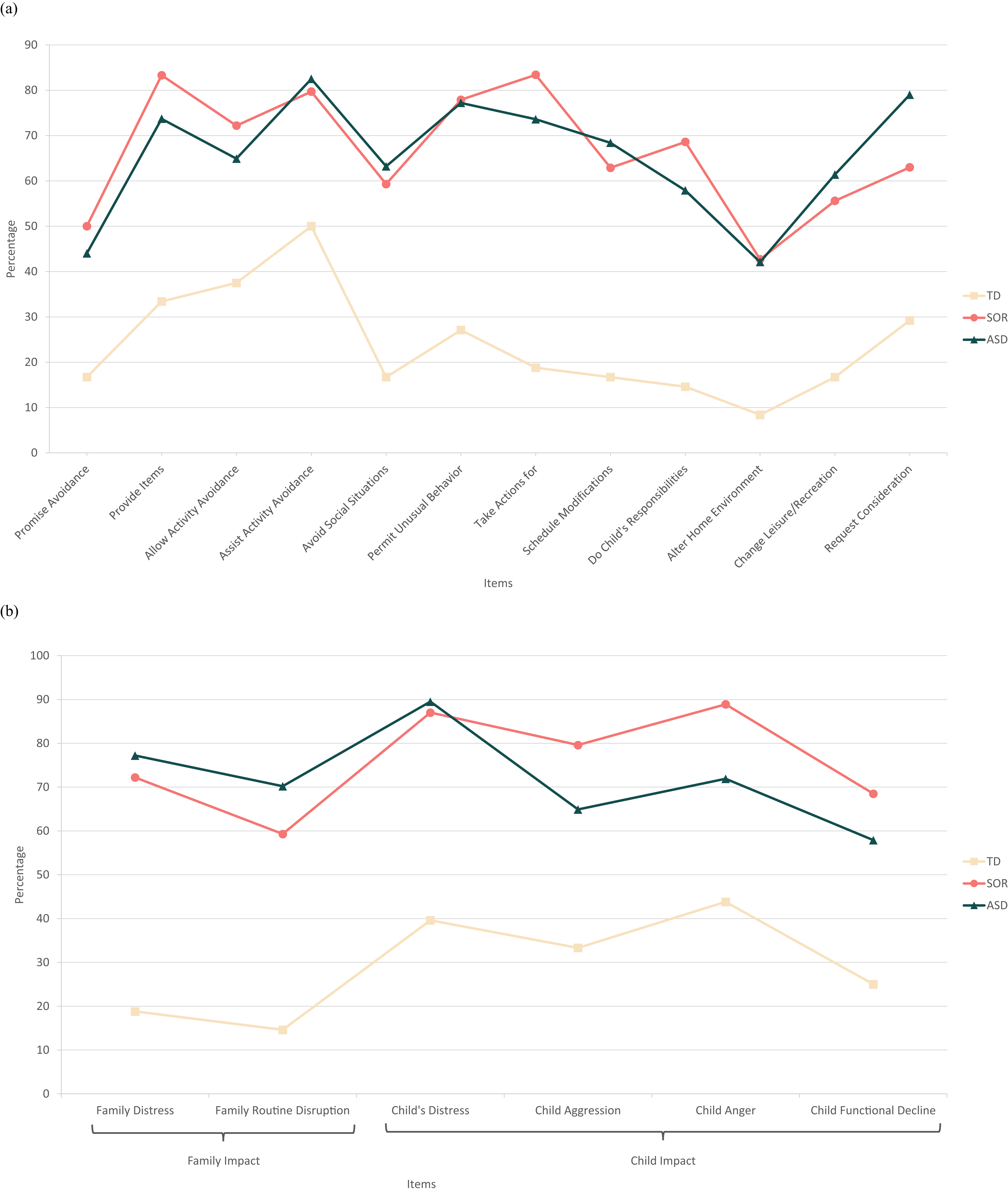
Percentage of FASENS items by group: Frequency scale (a) and Impact scale (b).
Group Comparisons
Kruskal–Wallis tests showed significant differences between the three groups on each FASENS scale: for frequency, H(2) = 63.28, p < .001, ε2 = .40; family impact, H(2) = 46.21, p < .001, ε2 = .29; and child impact, H(2) = 41.73, p < .001, ε2 = .26 (see Table 2). Mann–Whitney tests showed that the TD group had significantly lower FASENS scores than the ASD and SOR groups (p < .001), but the ASD and SOR groups did not differ significantly. An ANOVA showed significant group differences on total SOR, F(2, 156) = 33.53, p < .001, η2 = .30, and P–DTS scores, F(2, 156) = 9.37, p < .001, η2 = .11; see Table 2). Bonferroni pairwise comparisons showed that the TD group had significantly lower total SOR scores and significantly higher P–DTS scores compared with the ASD and SOR groups (p < .001), but the ASD and SOR groups did not differ from each other.
Correlations
Further analyses were conducted with the ASD and SOR groups combined, given the similarities between clinical groups across dependent variables. Table 3 presents Spearman ρ correlations between FASENS, total SOR, and P–DTS scores for the TD and clinical groups. All FASENS scores showed significant correlations with total SOR score (rs = .31–.64). P–DTS had significant negative moderate to high correlations (rs = –.39 to –.54) with FASENS scores in the clinical group (see Table 3).
Spearman ρ Correlations Between SOR, FASENS, and P–DTS by Group
Note. The clinical group included the SOR and ASD groups. ASD = autism spectrum disorder; FASENS = Family Accommodations Scale for Sensory Over-Responsivity; P–DTS = Parenting Distress Tolerance Scale; SOR = sensory overresponsiveness; TD = typically developing.
*p < .05. **p < .01.
Moderation Mediation Analysis
The three models showed significant mediation (see Figures 2a–2c). For the clinical groups, SOR symptoms positively affected FASENS frequency, family impact, and child impact (indirect model) by lowering parental distress tolerance capacity, which in turn increased accommodation frequency and impact (frequency point estimate = .005, 95% bootstrap confidence interval [CI] [.001, .010]; family impact point estimate = .010, 95% bootstrap CI [.004, .018]; child impact point estimate = .010, 95% bootstrap CI [.004, .017]). Independent of this mechanism (direct model), families of children in the clinical groups with higher total SOR had significantly more family accommodations (point estimate = .036, SE = .006, p < .001, 95% bootstrap CI [.025, .048]) and significantly greater child impact (point estimate = .025, SE = .007, p = .001, 95% bootstrap CI [.011, .039]).
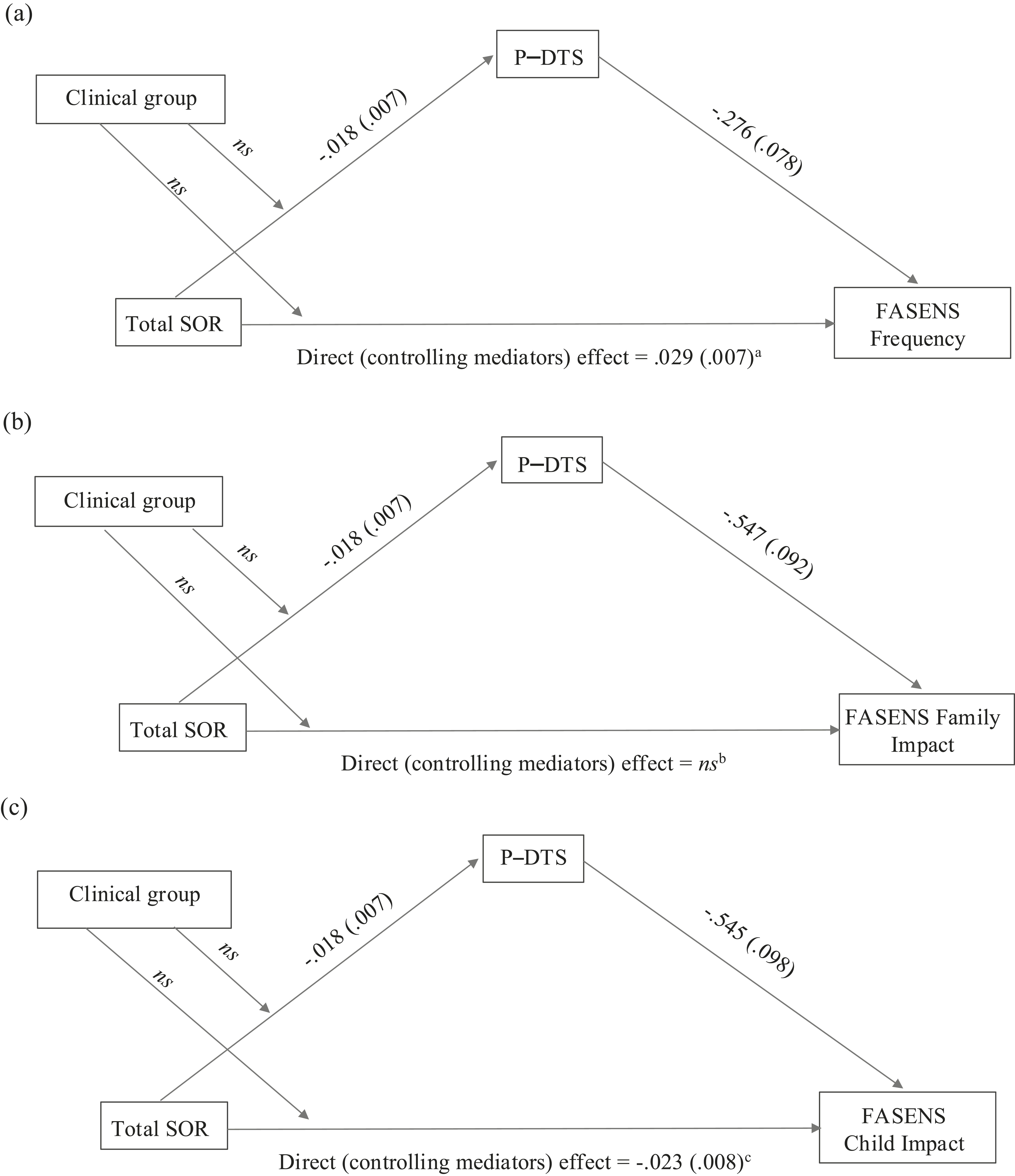
Moderation mediation model: FASENS Frequency (a), FASENS Family Impact (b), and FASENS Child Impact (c).
Across models, mother’s years of education did not significantly explain P–DTS or outcome variables (p > .33). In addition, in all models the clinical group did not significantly explain the relation between total SOR and P–DTS or between total SOR and outcome.
Discussion
This pioneering study characterizes sensory family accommodation for children with ASD and children with SOR, shedding light on the family dynamics surrounding sensory sensitivities. The results revealed more family accommodation and greater negative impact on family and child well-being in both clinical groups (ASD and SOR) compared with TD children. Parents with children in the clinical groups reported that their child experienced more bothersome sensory stimuli. Additionally, parents of these children exhibited lower tolerance for parental distress compared with parents of TD children. Notably, in the clinical groups, parental distress tolerance mediated the relationship between total SOR and FASENS scores regardless of socioeconomic status. These findings emphasize the importance of identifying family accommodation, particularly among families with children experiencing SOR and ASD, to mitigate the ongoing effects of avoidance on child and family well-being and participation.
The severity of SOR had a moderately strong correlation with more frequent family accommodations across groups and with their increased negative impact on both the child’s and the family’s well-being, supporting previous research (Bagby et al., 2012; Ben-Sasson et al., 2013; Carter et al., 2011; Dickie et al., 2009; Kirby et al., 2019; Schaaf et al., 2011). This pattern mirrors the findings of studies that found family accommodation was associated with greater severity of psychopathology symptoms among children with various disorders, such as anxiety disorders, OCD, eating disorders, ASD, tic disorders, and posttraumatic stress disorder (Iniesta-Sepulveda et al., 2021; Shimshoni et al., 2019).
The association between SOR severity and family accommodation can be interpreted in two ways. First, more bothersome sensations lead to increased child distress, prompting more accommodation. Second, frequent accommodation may paradoxically exacerbate symptoms by reinforcing avoidance behaviors. The heightened levels of child anxiety associated with SOR symptoms in both children with SOR and those with ASD (Ben-Sasson et al., 2025; Green et al., 2012) may contribute to the emergence of family accommodation. Further research is needed to explore the roles of child and parent anxiety in the development and maintenance of accommodations.
Across all groups, the percentage of participants engaging in accommodations at least once a month varied similarly between accommodation items (Figure 1a). Nonetheless, the clinical groups had 20% to 50% higher percentages of at least monthly engagement across items compared with the TD group (see Figures 1a–1b). FASENS accommodation items reported by more than 70% of parents in the clinical groups (see Figure A.2 in the Supplemental Material) included providing items to reduce sensitivities, aiding avoidance of stimuli, allowing atypical behavior due to sensitivity, and performing actions the parent would not have otherwise done. Conversely, the TD group rarely had a moderate to very extreme impact of accommodation on the family; however, they had an up to 20% moderate to extreme impact of accommodation on the child. Rates of moderate to extreme child and family impact in the clinical groups ranged from 40% to 60%. Interestingly, FASENS impact scores did not significantly differ between clinical groups, suggesting similar levels of family avoidance driven by SOR and its associated distress. Further research is needed to determine whether families in the ASD group engage in more accommodations that are triggered by nonsensory sources.
Surprisingly, the ASD and SOR groups had similar levels of SOR, P–DTS, and FASENS scores compared with the TD group. Both clinical groups had higher mean FASENS scores than those reported for children with a mixture of medical and developmental conditions (Ben-Sasson et al., 2022). The resemblance between clinical groups can be accounted for by the finding that 84.2% of the ASD group also met the SSP–2 criteria for the SOR group. This is consistent with previous studies that found that both children with SPD and children with ASD had sensory sensitivity but that it differed in clinical expression (Schoen et al., 2009; Tavassoli et al., 2018). Sensory sensitivities and their associated anxiety can explain similarities in rates and impact of their related family accommodation in both clinical groups.
Lower parental distress tolerance correlated moderately to highly with higher FASENS scores in the clinical groups, aligning with evidence linking lower distress tolerance to family anxiety accommodation (Birk et al., 2022). This contrasts with lower correlations observed among youth with OCD (Selles et al., 2018), possibly because of the significantly higher FASENS and P–DTS scores in these groups, along with heightened child and parent stress levels. Family accommodation reflects both the child’s distress and the parent’s capacity to handle it. Understanding of the persistence of SOR symptoms and their associated psychopathology may be enhanced by examining family accommodation, which is influenced by the family’s emotional regulation and distress tolerance (Russell & Lincoln, 2016). Our findings underscore the importance of assessing sensory family accommodation as well as parental distress tolerance. Beyond parents’ own self-regulation, parental distress tolerance moderates the child’s psychopathology by providing models for effective stress management (Birk et al., 2022; Russell & Lincoln, 2016; Selles et al., 2018). In both clinical groups, P–DTS scores significantly mediated the relationship between total SOR and FASENS scores, indicating that more SOR symptoms led to higher FASENS frequency and greater negative family and child impact by reducing parental distress tolerance. This mediation corresponds with evidence relating greater child negative affectivity to poorer parent distress tolerance (Morford et al., 2017). Although TD families had significantly higher socioeconomic status than clinical families, mother’s education level did not explain mediation or P–DTS scores. The current study highlights that the combination of elevated SOR symptoms and poor parental distress tolerance leads to increased use of family accommodation, resulting in greater interference with family and child well-being.
Implications for Occupational Therapy Practice
As providers, occupational therapists frequently help families adjust their environment and routines to meet their children’s needs. This study underscores the importance of monitoring these adaptations to determine their effect on child and family well-being. Although these changes can improve caregiver–child relations and activity participation and provide short-term distress relief, they may also breed long-term avoidance and caregiver strain (Schaaf et al., 2011; Walbam, 2023). The results of this study underscore the importance of identifying families (especially parents of children with ASD, SOR, or both) who have low distress tolerance. These families may benefit from interventions such as mindfulness strategies and emotional regulation techniques (Salem-Guirgis et al., 2019) to better manage their child’s distress and decrease reliance on accommodation. Several intervention programs (Frank et al., 2022) have been effective in reducing these types of accommodations among families who have children with ASD or other disorders involving anxiety (Shimshoni et al., 2019), providing valuable resources for enhancing family well-being and functioning as well as the management of their child’s and their own distress. A home-based sensory intervention program was found to be beneficial for children with ASD (Padmanabha et al., 2019). Although a few studies have explored family coaching for sensory challenges (Allen et al., 2021; Reynolds et al., 2017), addressing family accommodation (as defined in this study and in the mental health literature) has not been incorporated into these methods. The findings presented in this study highlight the need to embrace a family-centered approach to address SOR, acknowledging that SOR symptoms, along with their associated anxiety, affect both child and family dynamics.
Limitations
This internet survey study recruited clinical groups from clinics and special education settings and relied on parental reports for clinical diagnosis. Although parents provided information on their child’s ASD severity and educational setting, a standardized ASD severity index was not used. Additionally, for the SOR group, we applied SSP–2 scoring criteria but lacked information on their attention deficit hyperactivity disorder diagnosis, specific learning disabilities, and ASD traits, which are crucial for understanding similarities between clinical groups. This study collected data from mothers in two-parent families. Fathers’ perspectives regarding accommodation may differ. Further research including fathers and diverse families is important for understanding the dynamics surrounding sensory problems.
In addition, this study lacked in-depth cross-cultural research on the distribution of FASENS and P–DTS between Hebrew- and Arabic-speaking families. Future research in these areas will be important to unveil different response patterns to child distress to enable culturally competent, family-centered care. Additional limitations are that maternal anxiety levels and sensory sensitivities were not measured. These are also necessary for understanding family responses, given that mothers with elevated anxiety tend to respond with accommodation (Settipani & Kendall, 2017). Additionally, mothers of children with SOR (Gafni-Lachter et al., 2022; Turner et al., 2012) or ASD (Uljarević et al., 2014) may exhibit avoidance patterns because of their own sensory sensitivity.
Differences in parent education and income levels between the TD and clinical groups relate to the recruitment of the TD group from among friends and family as opposed to the broader recruitment of clinical groups. Although we balanced the groups for ethnicity, we did not match on socioeconomic status. Mother’s education was entered as a covariate and found to be nonsignificant. Further research with a representative sample would enable a better analysis of the contribution of socioeconomic status to a family’s response to extreme sensitivities.
Conclusion
The FASENS effectively distinguishes clinical from nonclinical groups, making it a useful tool to study how families respond to children with unique sensory needs. Among the family changes in response to clinical levels of SOR, it is important to note the most common: Giving children items to reduce their sensitivities, helping them avoid stimuli or situations that provoke sensitivity, enabling them to behave oddly or inappropriately because of their sensitivity, and performing actions that parents would not do if their children did not have SOR symptoms. Beyond the finding of more frequent changes in family life, these changes have a negative impact on the well-being of families with children with SOR or ASD. Elevated SOR results in distress, which starts a cycle of family responses, known as family accommodation. To fully understand the course of impairment associated with SOR, there is a need to understand the avoidance and increasing dependency that they create. This study emphasizes the need for occupational therapists to assess the family climate surrounding SOR, including family accommodation and parental distress tolerance, as a foundation for understanding the dynamics that contribute to its intractability.
Supplemental Material
Supplementary material for Sensory Family Accommodation for Autistic and Sensory Overresponsive Children: The Mediating Role of Parenting Distress Tolerance
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050790.pdf for Sensory Family Accommodation for Autistic and Sensory Overresponsive Children: The Mediating Role of Parenting Distress Tolerance by Ayelet Ben-Sasson and Adi Zisserman in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Ms. Maisa Haj for her assistance with data collection and Ms. Sandra Zukerman for her guidance with statistical analyses. Our gratitude to the families who took the time and effort to share their personal experience with us.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.