
Abstract
This case report describes how occupational therapy practitioners used external pelvic floor biofeedback as an adjunct conservative treatment strategy when providing care for pediatric children with recent incomplete spinal cord injury.
Every year, approximately 12,000 people experience spinal cord injury (SCI) in the United States (National Spinal Cord Injury Statistical Center [NSCISC], 2011), with children accounting for 8.5% of those cases (NSCISC, 2020). Pediatric SCI can be congenital or acquired and traumatic or nontraumatic (Powell & Davidson, 2015). Causes of nontraumatic acquired SCI can include diagnoses such as acute myelitis, tumor, spinal cord edema, vascular condition, or congenital disorders (Molinares et al., 2022). Traumatic-acquired pediatric SCI most commonly occurs because of motor vehicle accidents, diving, falls, and sports injuries (Mandadi et al., 2022).
The American Spinal Injury Association (ASIA) recommends using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) to classify not only the spinal injury level but also the degree of completeness (Rupp et al., 2021). The degree of completeness is determined by evaluating the most caudal section of the spinal cord for sensation and antigravity muscle function along with an ASIA Impairment Scale (AIS) score that indicates the SCI degree of completeness (Rupp et al., 2021). The AIS is considered more reliable for children age 5 yr and older (Mandadi et al., 2022). Following complete SCI, sensory and motor functions are absent below the level of injury (ASIA & International Spinal Cord Society International Standards Committee, 2019). With an incomplete SCI, a child may still have partial sensory or motor function below the level of injury (Ho et al., 2007).
Numerous comorbidities are associated with SCI. The two most impactful on quality of life and social participation are neurogenic bowel and neurogenic bladder (Gater, 2020). Bowel and bladder motility and function include sensory and motor components (de Groat et al., 2015). As a result of bowel and bladder dysfunction, alternative methods for toileting management for individuals with SCI may be required (Tate et al., 2016). Bowel and bladder dysfunction can have significant negative impacts if left unmanaged, including emotional dysregulation and adverse effects on social participation, sexual function, work activities, and quality of life (Varni et al., 2023).
Occupational therapy practitioners play a unique role in the management of neurogenic bowel and bladder secondary to SCI for children. Bowel and bladder management are considered aspects within the broader occupation of toileting. According to the American Occupational Therapy Association (AOTA; 2020)
Occupational Therapy Practice Framework: Domain and Process (4th ed.), toileting is defined as obtaining and using toileting supplies, managing clothing, maintaining toileting position, transferring to and from the toileting position, cleaning the body, caring for menstrual and continence needs (including catheter, colostomy, and suppository management), maintaining intentional control of bowel movements and urination and, if necessary, using equipment or agents for bladder control. (p. 30)
Therein, toileting encompasses numerous performance patterns, performance skills, and body functions. Bladder management can be considered “maintaining intentional control of urination” within the context of toileting (AOTA, 2020). Occupational therapy practitioners play a salient role in bladder management with SCI, considering the client factors, performance patterns, performance skills, environment, and context (AOTA, 2020). This role may include biofeedback, interoception, positioning, durable medical equipment, child-centered goals, and child–family education (Kane, 2022). Children benefit from a multimodal approach that connects them to when and how toileting will occur (Gronski & Doherty, 2020).
Various medical management techniques address bowel and bladder management for complete and incomplete SCI. Conservative bowel management could include fluids, oral supplements, stomach massage, or rectal digital stimulation (Johns et al., 2021). Conservative management approaches following SCI for neurogenic bladder include timed voiding, Valsalva maneuver, medication, intermittent catheterization, or indwelling urinary catheter (Taweel & Seyam, 2015). External pelvic floor biofeedback uses surface electromyography (EMG) electrodes and visual feedback to illustrate muscle activity, aiding in gaining control through on-screen animations that visualize muscular contraction and relaxation (Buckley et al., 2019; Kopru et al., 2020; Xu et al., 2020). Additional conservative bladder management approaches for neurogenic bladder consist of pelvic floor muscle retraining, electrical stimulation, and external biofeedback; however, studies have included only adult clients and have had small sample sizes (Elmelund et al., 2018; Gamal et al., 2022; Shendy et al., 2015; Vásquez et al., 2015).
Adults with incomplete SCI have safely used biofeedback to address bladder management (Elmelund et al., 2018). External pelvic floor biofeedback is commonly used as a supplemental therapeutic intervention to treat bladder management among children with nonneurogenic bladder dysfunction (Qi et al., 2022). Pelvic floor biofeedback has been advantageous for children with nonneurogenic voiding issues, such as urinary tract infection or constipation, when assessed against typical interventions (Qi et al., 2022). Currently, to our knowledge, there is no existing literature detailing the use of external pelvic floor biofeedback for children with neurogenic bladder following an incomplete SCI. Therefore, this case series aimed to describe the implementation of external pelvic floor biofeedback for bladder management within the context of toileting for children with neurogenic bladder dysfunction following a recent incomplete SCI.
Method
This retrospective case series investigated the use of external pelvic floor biofeedback to improve children’s bladder management following acquired or traumatic incomplete SCI. Epic Systems, the electronic medical records system, at a large midwestern children’s hospital (Nationwide Children’s Hospital), retrospectively supplied all data through chart reviews performed on patients admitted to our inpatient rehabilitation (IPR) unit between June and November 2022. Inclusion criteria were older than 4 yr old, neurogenic bladder and incomplete SCI documented by the medical team, and more than one external pelvic floor biofeedback session. Each child received occupational therapy services from one of two occupational therapy practitioners (Meredith ten Brink or Laura Rucki). Before initiating external pelvic floor biofeedback intervention, the occupational therapy practitioners received clearance from physiatrists, verbal consent from caregivers, and assent from the child. We completed this case series in accordance with the institution’s policy. The institutional review board of the hospital approved this retrospective case series (STUDY00003123).
Participants
This case series described 3 children admitted to the IPR unit of Nationwide Children’s Hospital following acute admission with newly acquired incomplete SCI. Patient characteristics considered by therapists for the implementation of biofeedback during IPR included receiving occupational therapy services on the IPR unit, diagnosis of incomplete SCI, documented or reported bladder management concerns, and participant and caregiver willingness to participate in biofeedback sessions. Children were considered appropriate for external pelvic floor biofeedback if they met the following criteria: (1) documented motor incomplete SCI on the ISNCSCI scale or corresponding diagnosis; (2) diagnosis of neurogenic bladder; (3) cognitively appropriate or ability to understand and follow directions to cooperate with biofeedback training; (4) behaviorally appropriate or demonstrating sustained attention, emotional regulation, and patience to allow for time required to set up and complete biofeedback training; and (5) no contraindications to external biofeedback. Direct intervention for bladder management was not provided by the acute care occupational therapist before transitioning to IPR. A chart review revealed subjective reporting of bladder dysfunction affecting all 3 children’s ability to engage in rest, sleep, play, leisure, or social participation. Evaluations within the IPR setting were completed, and standard occupational therapy treatment was initiated. For all 3 children, occupational therapy was the only therapeutic discipline to address bladder management within their plan of care. Routine medical techniques used during IPR admission to improve bladder management included toileting schedules, medication, and the presence of indwelling catheters. During the IPR admission, external pelvic floor biofeedback was chosen as an adjunct treatment modality when routine bladder management strategies were unsuccessful.
Participant 1 was an African American female (8 yr) with no significant medical history. She sustained trauma to her right flank of L1 (first lumbar vertebra) caused by a gunshot wound. Her SCI was classified as incomplete L2 AIS D. When initiating external pelvic floor biofeedback, her toileting schedule was every 4 hr while awake. She had physician-ordered bladder scans two times a day and received intermittent catheterization for bladder volumes greater than 100 ml. She required total assistance for catheterization. External pelvic floor biofeedback began during Week 3 of her rehabilitation stay (6 wk from injury). Biofeedback continued for 4 wk through discharge, during which she completed three external pelvic floor biofeedback sessions.
Participant 2 was a White male (12 yr) with a history of dyslexia and attention deficit hyperactivity disorder. He had an acquired, incomplete SCI with findings of C3-6 inflation and subtle inflammation extending to his T2 vertebra because of acute flaccid myelitis. Early in his admission, he sustained a urethral injury and pressure injury from his indwelling catheter that ultimately prolonged his need for a foley catheter. When initiating external pelvic floor biofeedback interventions, he required scheduled intermittent catheterizations five times daily. He could verbalize his sensation of the urge to void, and his bladder volumes increased; however, he was unable to void independently. He experienced incontinent episodes between catheterization times and was taking Ditropan to assist with bladder management. External pelvic floor biofeedback began during Week 3 of his IPR stay (11 wk from injury), and he completed two external pelvic floor biofeedback sessions during the 2 wk before discharge.
Participant 3 was a White female (13 yr) with no significant medical history. She had sustained a SCI during a gymnastics accident with resultant bilateral dislocation of her cervical spine. This acquired SCI was classified as a C5 AIS D. She spontaneously began to void on her own the evening before initiating external pelvic floor biofeedback intervention. Although she no longer required catheterization, intervention was still completed because of her inconsistent timing with urination and voiding volumes. She was taking Ditropan to assist with bladder management. External pelvic floor biofeedback began during Week 5 of her IPR stay (6 wk from injury) and continued for 2 wk through discharge. During this time, she participated in two external pelvic floor biofeedback sessions.
Outcome Assessments
There is currently no established outcome assessment for the pediatric population with incomplete SCI regarding the use of biofeedback for bladder management. Therefore, we analyzed outcome measures used as a standard of care within IPR. In addition, as a standard of occupational therapy care during IPR admissions, a holistic assessment of toileting was completed. This evaluation included the Activity Measure for Post Acute Care (AM-PAC) Daily Activities Short Form and Pediatric Spinal Cord Injury Activity Measures (PEDI–SCI AM) Short Forms. To more specifically assess bladder management, we used the Functional Independence Measure for Children (WeeFIM®), and voiding characteristics were obtained through data extraction via the patient’s electronic medical record. PEDI–SCI AM data were gathered through a written questionnaire. The treating occupational therapist determined the WeeFIM and AM-PAC scores during the child’s admission. Data was also gathered from subjective reports from each child and treatment notes written by the treating therapist after each biofeedback session. All three assessments were completed at IPR admission (prebiofeedback) and at IPR discharge (postbiofeedback), and data extraction was completed following discharge.
AM-PAC Daily Activity Short Form
The AM-PAC Daily Activity Short Form is a six-question instrument focusing on self-care and daily activities (Jette et al., 2014). Each of the six questions is scored on a scale ranging from 1 to 4 based on the difficulty or level of assistance that is required for the child or the caregiver to perform the daily activity task, with higher scores indicating greater independence in daily activities (Jette et al., 2014). The lowest possible total score is 6, denoting the greatest need for assistance, and ranges up to 24, indicating the least assistance needed (Denlinger et al., 2021). The AM-PAC Daily Activity Short Form has good interrater reliability for children in acute care (Denlinger et al., 2021). The AM-PAC is valid for the mobility section for children (Gates et al., 2022). For this study, we used only the raw score of the toileting item from the Daily Activity Short Form, including the level of assistance needed for clothing management, toilet transfer, and completing toileting hygiene.
PEDI–SCI AM
The PEDI–SCI AM is a child or caregiver self-report measure of activity performance for children with SCI (Slavin et al., 2016). The PEDI–SCI AM can assess four domains: General Mobility, Wheeled Mobility (Power and Manual), Ambulation, and Daily Routines. The child or family rates items from 0 = cannot do to 4 = easy (Slavin et al., 2016). Strong reliability and internal consistency for the complete item banks and short forms exist for children of all lesion levels but notably with tetraplegia (Slavin et al., 2016). The PEDI–SCI AM is a valid and reliable outcome assessment for the pediatric population with both traumatic and nontraumatic spinal cord injuries (Slavin et al., 2016). This study used the Daily Routines domain by assessing the perceived assistance needed to complete clothing management and bowel programs.
WeeFIM
The WeeFIM is an 18-item instrument that measures a child’s ability to complete activities of daily living (Wong et al., 2002). One of the three domains is self-care. Ratings are scored on a seven-level ordinal scale (Wong et al., 2002). Level 7 requires no assistance for the child to complete a task, and Level 1 requires dependent assistance from a caregiver to complete the task (Wong et al., 2002). The WeeFIM has been shown to be valid and reliable with clients following a burn injury or when diagnosed with cerebral palsy (Jang et al., 2022; Niemeijer et al., 2012). This study used the bladder management section to highlight the level of assistance needed for toileting and the frequency of incontinent episodes.
Voiding Characteristics
Voiding outcomes were documented in real time by the nursing and care assistant staff within the electronic medical record output flowsheet during IPR admission. Data extracted from the flowsheet included urine occurrences, urine status, output volumes, and postresidual void volumes. Urine occurrence indicates the number of voids per day. Urine status refers to the method with which the child voids and was categorized by the following documentation options within the flowsheet: bathroom privileges/voiding, catheterization sterile, diaper, self-catheterization, straight catheterization, and incontinent in brief. We classified the flowsheet entry of bathroom privileges/voiding as continent for this case series; all others were considered incontinent. Output volume data included volumes documented as urine (noncatheterization), urine (straight catheterization), or urine (diaper). Postresidual void was also recorded as occurrence and volume.
Intervention
During IPR admission, all children participated in occupational therapy sessions at least 60 min daily Monday through Friday and 30 min on Saturdays. If appropriate, the two occupational therapy practitioners (ten Brink and Rucki) and nurses collaborated to implement routine bladder management techniques and the physicians-led medication dosing.
External pelvic floor biofeedback was used as a treatment modality after implementation of the routine bladder management techniques. The two occupational therapists used the Prometheus EMYO® 200B biofeedback system for each external pelvic floor biofeedback treatment session. Skin electrodes were placed externally on the child’s perineum at 10 o’clock and 2 o’clock positions to assess contraction and relaxation of the pelvic floor muscles through surface external pelvic floor biofeedback. The reference electrode was placed on the child’s gluteal or thigh musculature. The child placed the external electrodes if able, under direct coaching from the therapist. If the child was unable to place the electrodes themselves, the therapist or caregiver placed the electrodes with the child’s and caregiver’s permission. Positioning for external pelvic floor biofeedback was either on the toilet, with adaptive equipment available as appropriate for the child, or in supine position with legs fully supported at approximately 90° of hip flexion and knee flexion. Electrodes correlated to animated biofeedback on a computer screen visible to the child and therapist. The screen displayed an object of interest to the child (balloon, butterfly, or spaceship) within a visually engaging background. As the object moved across the background from left to right, the position of the object raised or lowered in response to the contraction or relaxation of the child’s pelvic floor captured by the external pelvic floor biofeedback. A baseline activation reading was obtained for two repetitions of 6 min for the therapist to determine individualized contract and relax thresholds and to allow adequate time for the child to understand the biofeedback system. Each child completed 10 s of pelvic floor muscle contraction followed by 10 s of relaxation. At a minimum, the child completed three repetitions of 120 s during an occupational therapy session. Additional repetitions were completed as the child tolerated and as time allowed during the treatment session. Tracings of working contraction and relaxation minimum and maximum values (measured in microvolts) and average rest were obtained from the EMYO system. The occupational therapy practitioners provided verbal and tactile cuing for each child and adjusted the environment and positioning to optimize postural stability and pelvic floor relaxation. In some cases, durable medical equipment supported positioning, stability, and child safety. Contraction and relaxation quality were observed. Electrodes were removed by the individual who placed them, and a skin assessment was completed at the conclusion of each session. Detailed procedures can be found in the Appendix.
Results
All 3 children in the case series participated in external pelvic floor biofeedback, completing between two to four sessions (Table 1). The time to initiate external pelvic floor biofeedback from initial injury was 6.0 to 7.5 wk across children (Table 1). No adverse events or skin integrity concerns were reported related to external pelvic floor biofeedback treatment. All children tolerated external pelvic floor biofeedback intervention, and no session ended prematurely.
Participant Characteristics
Note. AIS = American Spinal Injury Association Impairment Scale; ICD-10 = International Classification of Diseases, 10th Revision; SCI = spinal cord injury.
The result of each outcome assessment at the following times is described in Figure 1: (1) before initiating external pelvic floor biofeedback and (2) at discharge from IPR. The assessments captured a more holistic view of the patient’s performance skills and patterns with bladder management in the context of toileting. The AM-PAC and PEDI–SCI AM focused on the more global aspects of the routine of toileting, and the WeeFIM and subjective data captured bladder management more specifically within the context of toileting. All 3 children improved their raw scores on the AM-PAC Daily Activity Short Form toileting item with increase in scores by 2 to 3. The WeeFIM scores illustrated improvements in bladder management for only 1 child, initially requiring total assistance and improving to modified independent at discharge from IPR. The PEDI–SCI Daily Routine score improved for 2 children from admission to discharge.
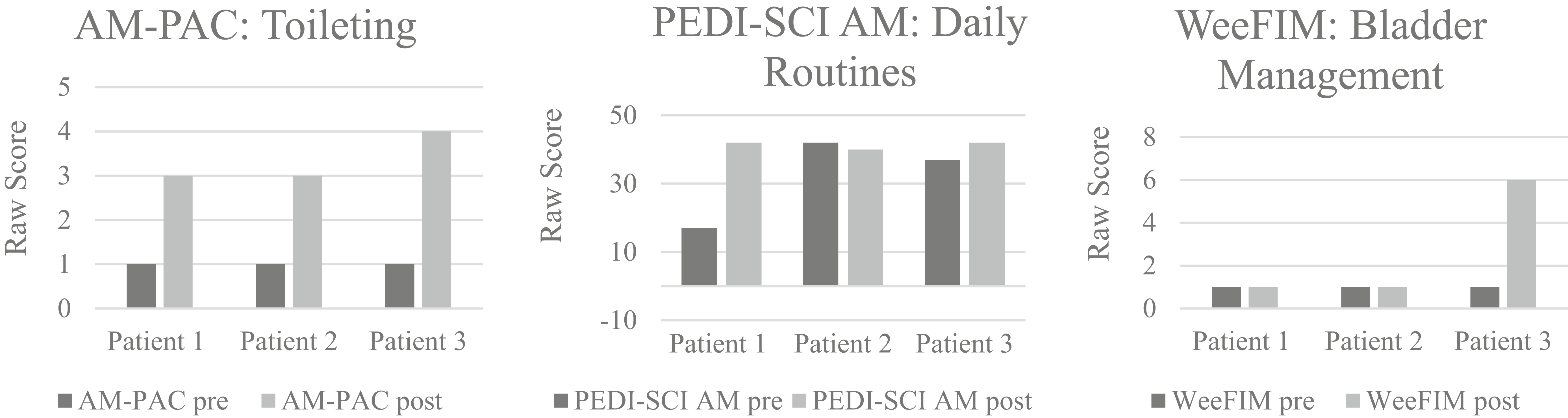
Outcome assessment raw scores.
For bladder management, the voiding outcomes were extracted from voiding characteristics of each child during IPR admission (Figures 2–4). Participant 1 required fewer catheterizations, experienced fewer incontinent occurrences, and had greater continent episodes from prebiofeedback to discharge from IPR (Figure 2). Participant 2 required fewer catheterizations and had greater daily continent occurrences; however, he had increased his average incontinent occurrences (Figure 3). Participant 3 had the most improved outcomes, with no incontinence episodes or catheterizations required at discharge from IPR (Figure 3). For subjective characteristics, therapist-documented or participant-reported subjective outcomes regarding external pelvic floor biofeedback, collected from notes via chart review, are reported in Table 2.
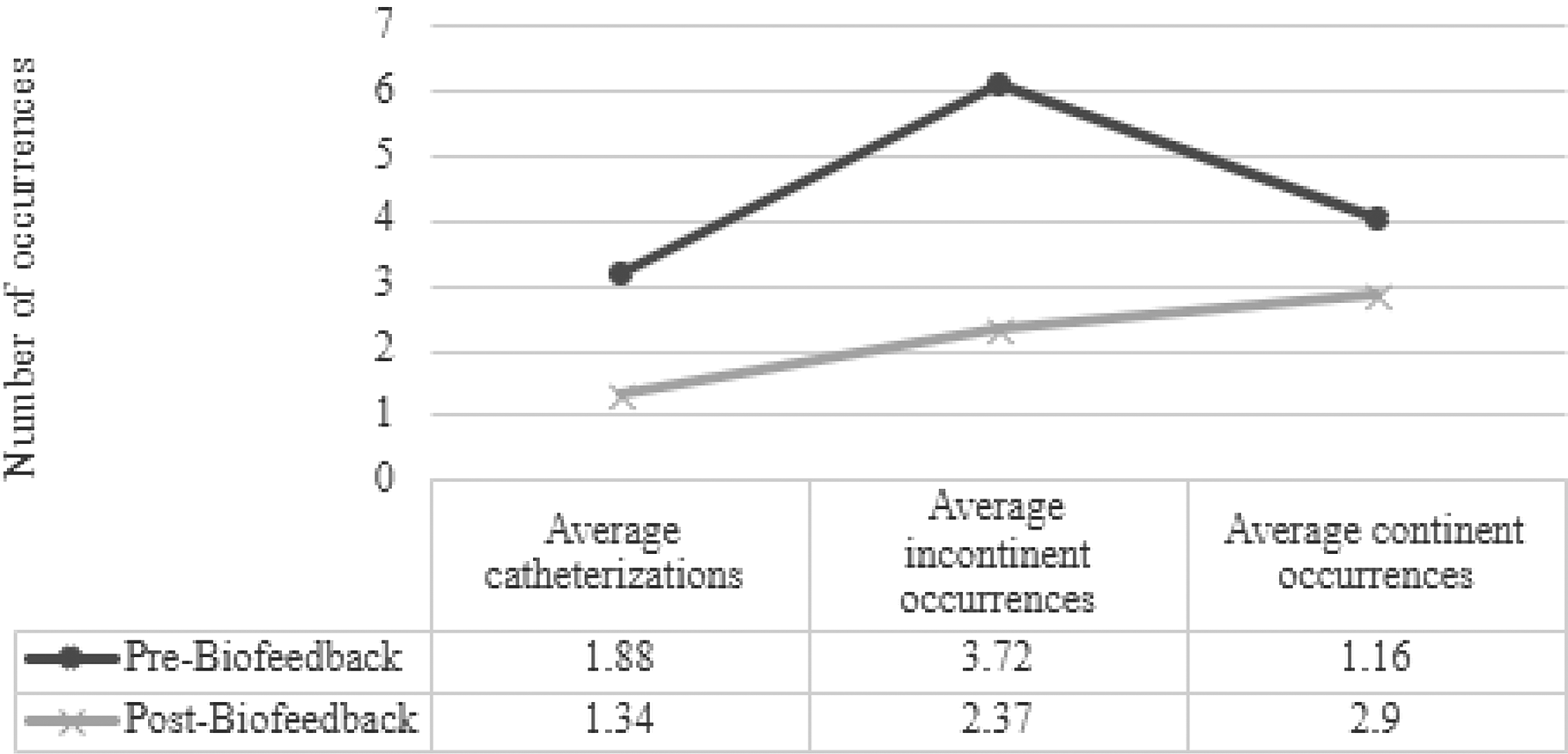
Voiding outcomes for Participant 1.
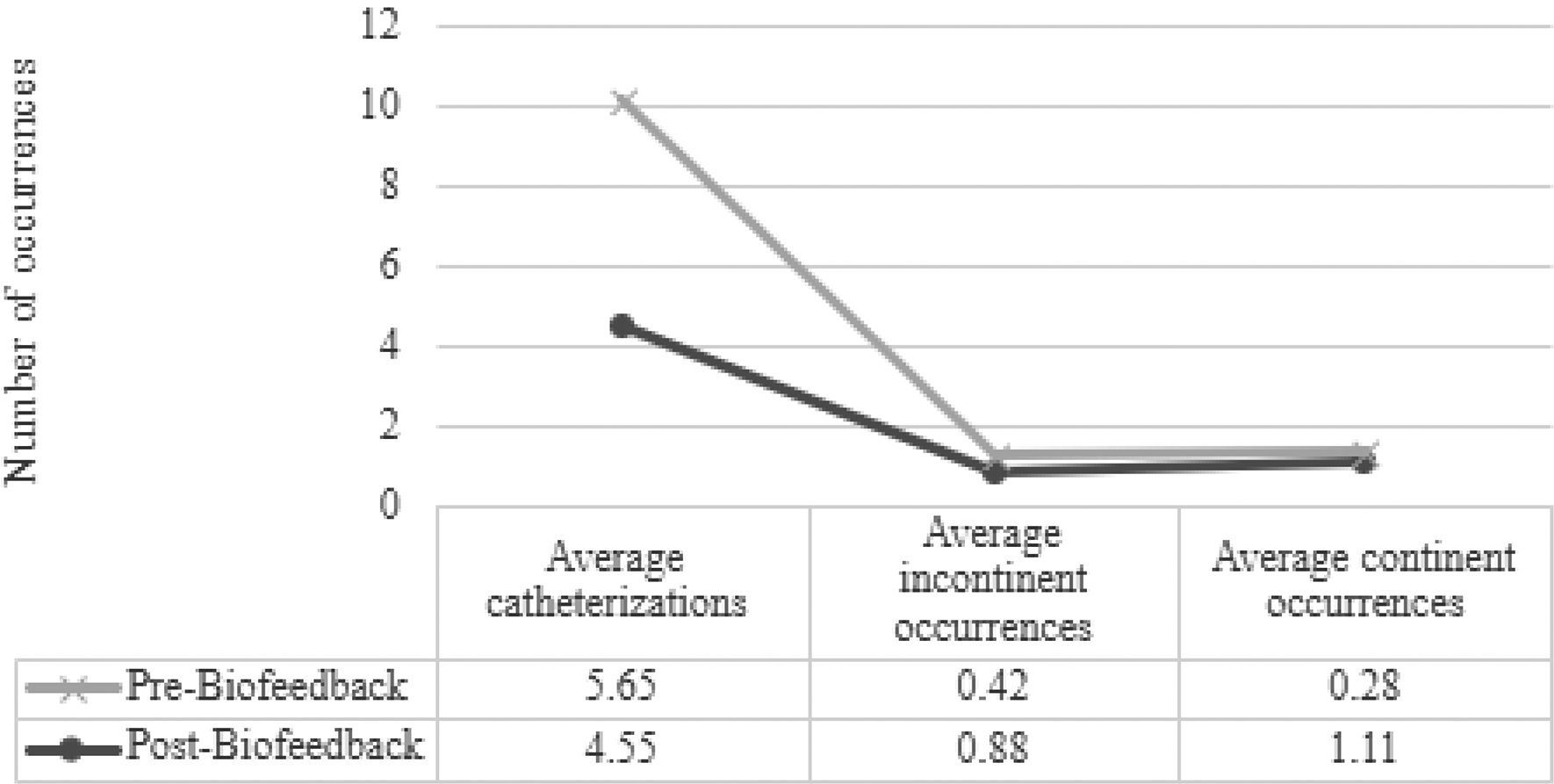
Voiding outcomes for Participant 2.
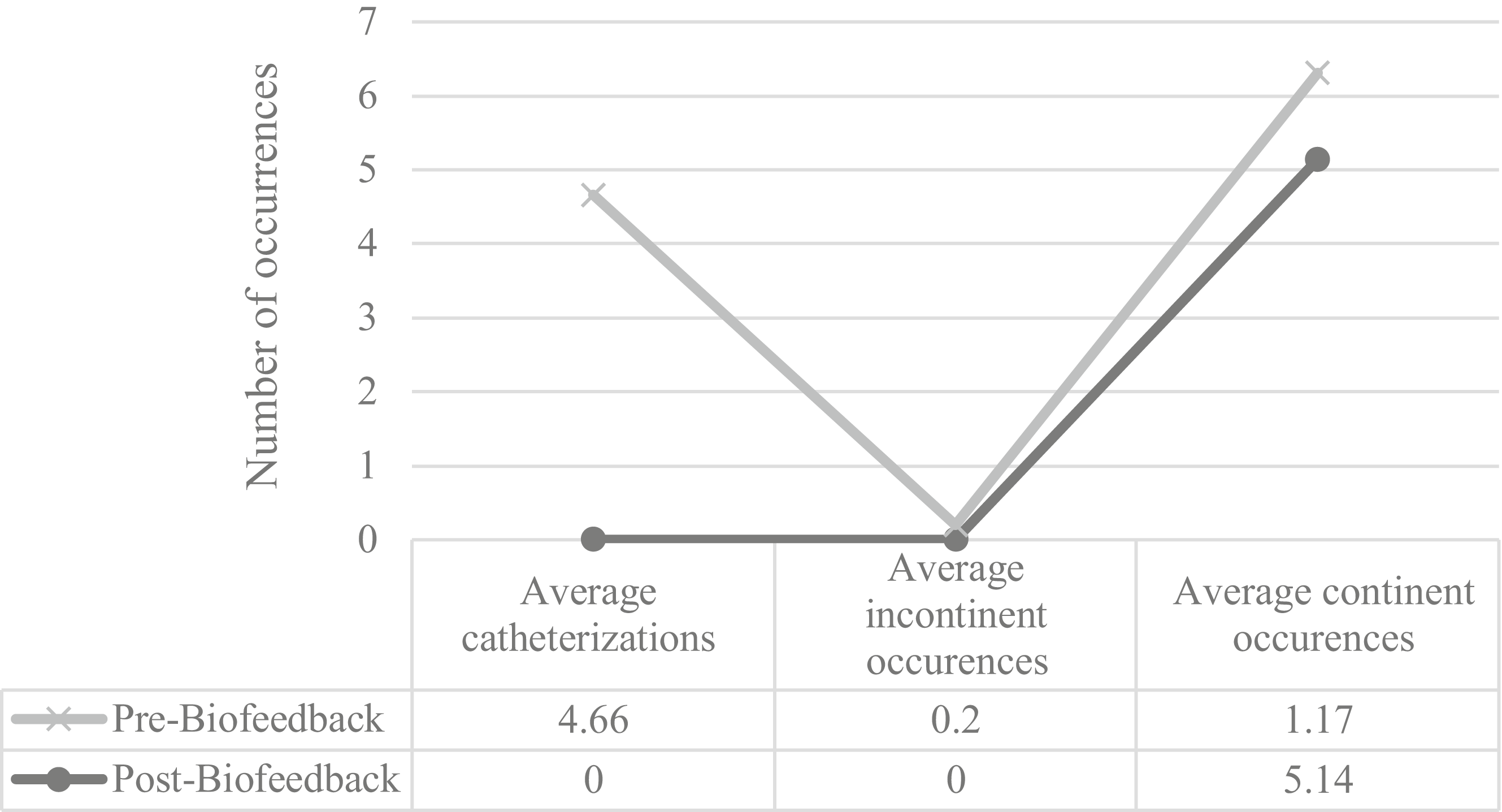
Voiding outcomes for Participant 3.
Clinician Observations and Patient Reporting
Discussion
To our knowledge, this study is the first to describe using external pelvic floor biofeedback with children with neurogenic bladder following incomplete SCI. Occupational therapy interventions aimed to improve independence with bladder management in the context of toileting. Findings from this case series suggest that external pelvic floor biofeedback could be a supportive adjunct to standard occupational therapy treatment during IPR for children with incomplete SCI.
Studies focusing on adults with neurogenic bladder and children with nonneurogenic bladder have determined the safety of external pelvic floor biofeedback within their respective populations (Alyami et al., 2019; Buckley et al., 2019; Vásquez et al., 2015). Consistent with these studies, no adverse events occurred with external pelvic floor biofeedback during this case series. Catheterization for bladder management can lead to secondary consequences, including urinary tract infections, development of false tracts, and scarring (Mohamed et al., 2022). For all 3 children, catheterization frequency decreased, and each child no longer required bladder scanning for postresidual void volumes by discharge. This result suggests that bladder management strategies, including external pelvic floor biofeedback, may result in fewer medical interventions, such as catheterizations, and allow for potential reduced risk of secondary complications.
Specific biofeedback tracing measurements (in microvolts) of each session were not extracted for this article because of poor validity between sessions. Slight changes in electrode placement between sessions along the specified muscle groups may account for these differences (Siracusa et al., 2015). The patient’s length of stay and other medical precedencies limited the total number of sessions. The number of biofeedback sessions needed to demonstrate improvement in voiding characteristics varies within the literature. Combs et al. (1998) reported 3.7 sessions, whereas Das et al. (2023) found clinical improvement after 11 sessions, with sessions occurring weekly or every other week and extending treatment time into months. This variability exists throughout the surface EMG biofeedback literature for children with non-neurological dysfunctional voiding (Combs et al., 1998; Das et al., 2023; Li et al., 2024). During IPR at our institution, the average length of stay was 4 to 6 wk, which does not align with the recommended treatment frequency and dosing. Although their study not used on pelvic floor musculature, Brucker and Buylaeva (1996) found that for patients following SCI, using biofeedback on the triceps significantly increased voluntary EMG activity after only one biofeedback session and with each subsequent intervention. In our study, each child received two to four biofeedback sessions and demonstrated positive voiding characteristics after the initial session. Outcome assessment results for each child in the AM-PAC Daily Activity Short Form, toileting, and WeeFIM bladder management exhibited improved raw score trends from admission to discharge from IPR (Figure 1). PEDI–SCI AM scores revealed 2 children who perceived improved ease in daily routines with the self-care activities of fixing clothing and completing a bowel program. Child 2’s decrease in his daily routine score on the PEDI–SCI AM was interpreted as a perceived increase in difficulty with self-care tasks. This difficulty may have been related to the child receiving less assistance from caregivers, resulting in increased active participation in the tasks, thus leading to more perceived difficulty. Given the absence of outcome assessments specifically focused on pediatric neurogenic bladder management, the inclusion of all relevant assessments provides a thorough representation of the care plan for each child in this case series and encompasses bladder management within the context of toileting.
The influence of virtual reality with animated biofeedback may be an effective tool to engage the pediatric population. Huang et al. (2022) proposed that virtual reality increase engagement and physiologic effort during nonimmersive virtual reality gaming. Virtual reality in animated biofeedback uses visually captivating backgrounds, featuring characters or objects in motion across the screen to represent muscle activity. A few studies have investigated external pelvic floor biofeedback and the impact of nonanimated (chart or graph only) versus animated biofeedback and found comparable successful results with both groups (Kaye & Palmer, 2008; Oktar et al., 2018). However, the animated groups demonstrated a decrease in the time needed to see results (Kaye & Palmer, 2008). In addition, each child displayed subjective improvement in attention and engagement (Oktar et al., 2018). Although this case series did not directly examine these specific outcomes, animated pelvic floor biofeedback was used and seemed to motivate and enhance attention for each child. Therefore, using animated external pelvic floor biofeedback for children following incomplete SCI may be valuable in maintaining interest and increasing participation.
Although objective measures and subjective child reports in this case series indicated improvements in self-care following external pelvic floor biofeedback, determining whether biofeedback was the sole cause was difficult. We must consider other reasons for improvement across the child’s continuum of recovery. Interoception or interoceptive awareness is an emerging concept and is defined as the input and recognition of sensory experiences happening inside the body, leading to increased awareness of the body, mental functions, and self (Mahler et al., 2020). Practitioners can use interoceptive practices to help children interpret sensory messages from the bladder, potentially influencing bladder management (Schmitt & Schoen, 2022). In addition to the muscular control developed through external pelvic floor biofeedback, developing interoceptive awareness through other standard occupational therapy interventions may have promoted Child 3’s ability to notice, give meaning to, and respond to internal or physiological sensations such as a full bladder and the need to void. Time from initial injury and emergence from spinal shock may have also played a role in improved consistency with catheterizations, volitional bladder emptying, and muscle control. For many children with incomplete SCI, the natural sequence of recovery may include regaining some degree of bladder function or other physical function following emergence from spinal shock independent of treatment modalities (Ko et al., 1999).
The key demographic characteristics of children with neurogenic bladder examined in this case series are the same demographic characteristics often excluded from other literature because of age or diagnosis (Ladi-Seyedian et al., 2020; Pekbay et al., 2019; Qi et al., 2022). Lack of evidence for children with neurogenic bladder following an incomplete SCI may limit occupational therapists from implementing external pelvic floor biofeedback within this population. Therefore, no standardized frequency or duration is available specifically for this population. Current frequency within adult studies for neurogenic bladder management for incomplete SCI supports that one time per week for 6 to 12 wk may improve control of neurogenic detrusor overactivity and decreased incontinence (Vásquez et al., 2015). Further research on this pediatric population is needed to find the most effective frequency and duration of external pelvic floor biofeedback.
Limitations
This study had several limitations. The outcomes of this case series must be interpreted with caution because of the small, localized cohort. The selection of participants based on the limited number of patients with incomplete SCI, the therapist’s perception of the patient’s willingness to participate in biofeedback sessions, and use of subjective information therapists document may have introduced biases. Because of the nature of the retrospective study design, interventions were not standardized for administration times of external pelvic floor biofeedback. Limitations with the consistency of time to initiate biofeedback may be attributed to the following: (1) other individualized or prioritized goals within a child’s plan of care, (2) child and family acceptance of sequelae of injury and need for adapted toileting strategies, (3) building rapport with children before initiating treatment on a vulnerable topic, and (4) staff and child availability. Because of the retrospective nature of the study, other limitations include the variability of factors, such as child positioning, the intervention location (bathroom, hospital room), treatment time, scheduling constraints, and optimizing parameters and theme of images. Given the essence of the self-report measures, patients’ recall of responses and insight may limit the reliability of outcome responses. Data review and analysis were also subject to limitations because of inconsistency in documenting outputs between various nursing and patient care assistance staff and the potential for inaccuracies of obtained and recorded postresidual void volumes and total volumes of urine.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ Occupational therapy practitioners should consider integrating external pelvic floor biofeedback into care plans for children with incomplete SCI to support bladder management. ▪ Biofeedback may help children improve their toileting independence and reduce the need for catheterization, leading to greater autonomy and quality of life in the home, community, and school settings.
Conclusion
Within the context of toileting, animated external pelvic floor biofeedback intervention during occupational therapy during IPR may be an effective adjunct treatment modality for bladder management following incomplete SCI. No adverse events occurred using external pelvic floor biofeedback in this case series. All 3 children also demonstrated functional improvements in toileting independence, self-care participation, and daily catheterization requirements following external pelvic floor biofeedback. This case series highlights the important role of occupational therapy in toileting and innovative bladder management strategies for children, enhancing their quality of life and pelvic health. Future prospective, controlled research studies are recommended to continue assessing the optimal frequency and benefits of occupational therapy intervention with the use of external pelvic floor biofeedback for bladder management of children following incomplete SCI.