
Abstract
The authors assess the effect of cognitive therapeutic exercise and mirror therapy combined with task-oriented training for people with subacute stroke.
Stroke is a significant public health issue that affects quality of life (QoL; Owolabi et al., 2022). According to the World Stroke Organization, there are 12.2 million new strokes each year, with 80% of individuals experiencing various sequelae afterward. These sequelae, which significantly affect the upper limbs, can result in impairment of function in the upper limbs, affecting fine and gross motor skills, and the ability to perform activities of daily living (ADLs; Poltawski et al., 2016). Another important sequela that is observed is learned nonuse (Marquardt et al., 2017), in which individuals avoid using the affected upper limb because of motor difficulties even though they have some residual functional capability. Functional independence is also affected, which has a direct impact on QoL (Sivan et al., 2011). Addressing these sequelae is fundamental to improving QoL (Feigin et al., 2022).
Implementing a comprehensive rehabilitation approach to address the various sequelae of stroke is essential for optimal recovery, and personalized treatment tailored to the unique needs of each individual is crucial (Teasell et al., 2022). Achieving this personalized treatment requires an emphasis on pre- and posttreatment assessments with specific assessment tools to objectively measure outcomes (Colomer et al., 2023; Fernández-Concepción et al., 2008; Fernández-Solana et al., 2022; Furuta et al., 2022; H. C. Hsieh et al., 2021; Santamaría-Peláez et al., 2022). Evidence-based rehabilitation therapies are key to ensure that the treatments applied are effective and supported by scientific research (Langhorne et al., 2011). Examples of such therapies include mirror therapy (MT), cognitive therapeutic exercise (CTE), and task-oriented training (TOT; Diaz Castro & Rodriguez Lopez, 2019a; Lee et al., 2022; Lisalde-Rodríguez & García-Fernández, 2016; Teasell et al., 2022).
In MT, a mirror is used to create a visual illusion to enhance motor function in the affected limb (Muñoz-Gómez et al., 2023). The mirror reflects the unaffected limb, and the affected one remains hidden behind it. When the healthy limb is moved, its reflection creates the appearance of movement in the affected limb, tricking the brain into perceiving normal movement. Various studies have shown that MT is effective in improving motor function and neuroplasticity among patients with stroke (Kundi & Spence, 2023; Nogueira et al., 2021; Seyyah & Topuz, 2023).
CTE, also known as the Perfetti method, is a neurorehabilitation approach that provides personalized and specific treatment to each patient. Its goal is to recover lost or altered movement, and it involves assigning the patient the task of solving a specific problem that can be addressed through movement independent of each body segment, assisted by the therapist (Diaz Castro & Rodriguez Lopez, 2019; Parra Horta, 2018; Serrat et al., 2021). For example, a patient performs fragmented upper limb movement tasks with the therapist’s assistance, identifying the positioning of their upper limb in space in relation to nearby objects identified in advance. In a systematic review of the recovery of motor and functional capacity among patients with stroke sequelae, Vaca Garcés and Figueredo Villa (2023), as well as Domínguez Ferraz et al. (2014), determined that this technique has resulted in cognitive- and motor-level improvements among patients with hemiplegia.
TOT is an effective method for developing motor skills and brain plasticity through the repetition of specific and practical tasks that simulate everyday actions (Almhdawi et al., 2016; Alsubiheen et al., 2022; Preissner, 2010). Almhdawi et al. (2016) demonstrated significant and clinically meaningful functional improvements as measured with the Motor Activity Log (MAL–30; Santamaría-Peláez et al., 2022), Canadian Occupational Performance Measure (Yang et al., 2017), and Wolf Motor Function Test (Pometti et al., 2025) after 3 hr/wk of clinical upper limb functional training for 6 wk. Alsubiheen et al. (2022) indicated that 8-wk task-oriented ADL training improves upper limb functions and gross manual dexterity.
Finally, it is important to emphasize that in rehabilitation, prioritizing the optimization of functional recovery by balancing factors such as time, resources, and intervention effectiveness is essential. Combining therapies that have been proven effective can significantly enhance treatment effectiveness. Recent research has demonstrated that combining these therapies activates neuroplasticity more effectively than applying them separately (Bayón-Calatayud et al., 2014; Cano-de-la-Cuerda et al., 2015). For example, Bai et al. (2019) combined conventional therapy (physiotherapy focusing on motor function and ambulation and occupational therapy focusing on upper limb functional training and ADL training) with movement-based MT and task-based MT, which target different motor functions. Both forms of MT were found to be effective in improving function, with movement-based MT showing superior results. In a double-blind randomized controlled trial involving 30 patients with hemiparesis, progressive reach-to-grasp training combined with trunk restraint for arm recovery in the experimental group (EG) resulted in greater functional improvements 1 mo postintervention compared with the control group (CG), which received progressive reach-to-grasp training without trunk restraint (Michaelsen et al., 2006). This highlights the importance of combining interventions that address multiple aspects of motor function to achieve optimal rehabilitation outcomes.
We hypothesized that the combination of MT + TOT or CTE + TOT would be more effective in improving upper limb function after a stroke compared with isolated TOT therapy. However, as yet, no study has directly compared these combinations of techniques, highlighting the need for further research. Therefore, we aimed to assess the effectiveness of combining these techniques on overall motor function of the affected upper limb, fine and gross motor skills, use of the affected arm, functional independence in ADLs, and QoL among patients with stroke.
Method
Participants
Participants were 120 patients with stroke. The inclusion criteria were as follows: (1) subacute phase of stroke, defined as the period from symptom onset to hospital discharge, with less than 3 mo elapsed since symptom onset (Mah et al., 2022); (2) residual hemiparesis due to ischemic or hemorrhagic stroke; (3) mobility in the affected upper limb at Stages 2–4 of the Brunnstrom scale (Waghavkar & Ganvir, 2015); (4) Montreal Cognitive Assessment (MOCA; Gomez-Moreno et al., 2022; Ramírez-Moreno et al., 2022) score ≥26; (5) age 18 yr or older; and (6) signed informed consent. Exclusion criteria were (1) visual deficit or homonymous hemianopsia, (2) Wernicke or mixed aphasia, (3) hemineglect, and (4) cognitive deficit (MOCA score < 26).
This multicenter longitudinal study was conducted in collaboration with the University Hospital of Burgos (HUBU; Burgos, Spain), San Juan de Dios Hospital (Burgos), Reina Sofía Hospital (Córdoba), and the University of Burgos (Burgos). The study received approval from the Institutional Review Board Approval Committee of HUBU (2134/2019). Data collection was conducted at participating centers by designated personnel, and the data were anonymized before being shared with the research team to maintain anonymity and confidentiality. The trial was registered on ClinicalTrials.gov (NCT04163666, “Effects of Home-Based Mirror Therapy and Cognitive Therapeutic Exercise on the Improvement of the Upper Extremity Functions in Patients With Severe Hemiparesis After a Stroke: A Protocol for a Pilot Randomized Clinical Trial”).
Procedure
Participants in this study were selected upon discharge from the Stroke Unit and the Neurology Service using a consecutive selection method. Using G*Power, we determined that the sample should include 81 stroke participants.
The study design was a randomized, controlled, single-blind clinical trial with three groups: a CG and two EGs. EG1 received MT + TOT, and EG2 received CTE + TOT. The CG received only TOT (5 days/wk) as usual. The evaluators conducting the assessments were blinded to the study conditions.
The study was conducted during the participants’ outpatient rehabilitation, and they received no intervention before the start of the study. Participants were recruited by the rehabilitation physician of each participating center. The initial selection was based solely on the presence of upper limb impairment after a stroke; a second selection applying the study’s inclusion and exclusion criteria was carried out during the participants’ initial assessment. This assessment occurred 1 mo after the stroke event. Participants were then randomly assigned to groups through a masking process in a 1:1:1 ratio. The randomization was centrally generated by an independent investigator using Epidat 4.2, an open-access software for epidemiological analysis that facilitates random allocation, before participant inclusion.
Different researchers administered the therapies to the EGs. The MT and CTE were administered in the aforementioned hospitals by occupational therapists specialized and trained in the techniques used. The intervention spanned 20 sessions, conducted for 1 hr/day, 5 days/wk, for 4 wk (Luo et al., 2020; Pérez-Cruzado et al., 2017; Saavedra-García et al., 2021). As noted earlier, participants in EG1 received MT + TOT, and participants in EG2 received CTE + TOT. Therapies were structured in segments, with 30 min allocated to MT or CTE and the remaining 30 min to TOT. The CG received 60 min of TOT only. Therefore, all three groups received TOT, which was the usual therapy prescribed by the rehabilitation physician.
After both EGs completed the experimental treatment, a second assessment was conducted using the same evaluation tools as in the initial assessment. This second assessment occurred 1 mo after the first assessment, consistent across all three groups. Additionally, a third follow-up assessment was conducted for all three groups 3 mo after the second assessment. The flowchart in Figure 1 summarizes the procedure.
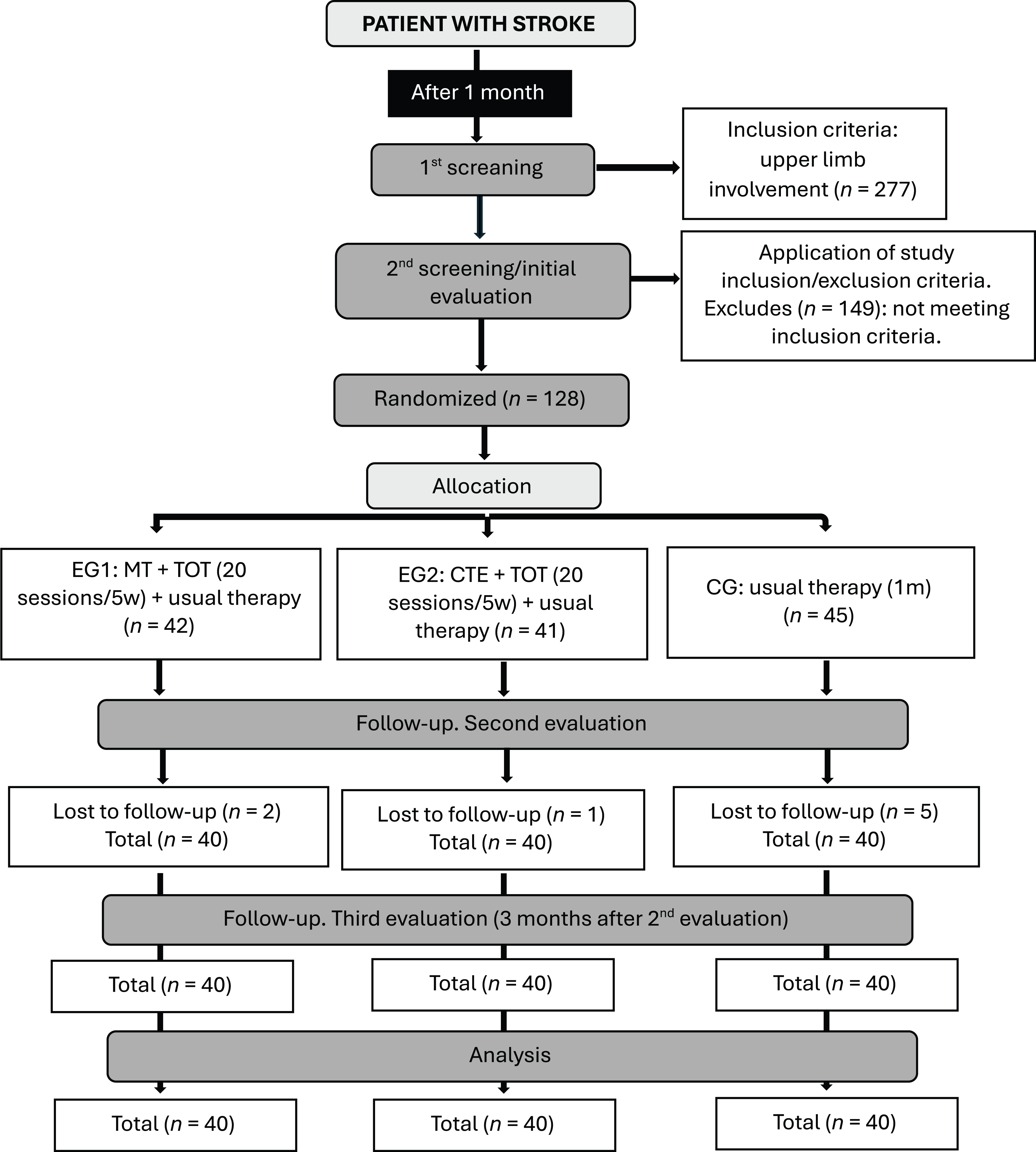
Flowchart of the study procedure.
Instruments
Sociodemographic data, such as age and sex, and poststroke clinical variables, such as affected side, dominant side, and type of stroke, were collected to describe the sample. Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot) lists the instruments or scales used in this study and the variables measured by each of them.
To measure the functionality of the upper limb, fine motor skills, and gross motor skills of the hand, we used the Action Research Arm Test (ARAT; Fernández-Solana et al., 2022) and the Box and Block Test (BBT; Angelos Nomikos et al., 2018). The ARAT has been translated and validated with the Spanish stroke population (α = .96), with a good test–retest reliability of .78. It consists of 19 items divided into four subscales (Grasp, Grip, Pinch, and Gross Movement), with scores ranging from 0 (unable to complete the task) to 3 (normal performance) on an ordinal scale. Total scores range from 0 to 57 (Pike et al., 2018). This scale is recognized as appropriate, valid, and sensitive for assessing individuals who have experienced a stroke (Lang et al., 2006; Pike et al., 2018).
The BBT (Chen et al., 2019; Desrosiers et al., 1994; Y. W. Hsieh et al., 2020) requires moving 150 wooden blocks within 1 min from one compartment in a box to another, using first the unaffected upper limb and then the affected one. The score is determined by manually counting the number of blocks moved. It has high test–retest reliability, with intraclass correlation coefficients ranging from .89 to .97.
Quantity and quality of use of the affected arm was measured using the MAL–30 (Santamaría-Peláez et al., 2022). This tool evaluates how much and how well individuals use their affected upper limb in ADLs and instrumental activities of daily living (IADLs) after a stroke. The tool has two subscales, Quantity and Quality, each of which consists of 30 items. Scores range from 0 (the affected arm is never used for the activity) to 5 (the affected arm is able to perform the activity at the same level as before the stroke). A higher score indicates better movement quality and more normalized use of the affected upper limb (Arlette Doussoulin et al., 2013; Sada et al., 2021; Taub et al., 2011; Van Der Lee et al., 2004). This instrument has been translated and validated for use with the Spanish-speaking stroke population (αs = .990 and .991 for the Quantity and Quality subscales, respectively), and it has a test–retest reliability of more than .86 (Uswatte et al., 2005).
Functional independence in ADLs is assessed using the FIM™–Functional Assessment Measure (FIM–FAM; Law et al., 2009; Martínez-Martín et al., 2009; Nayar et al., 2016; Turner-Stokes & Siegert, 2013). This global disability measure consists of 18 items from the FIM and 12 items from the FAM. Each item is scored on a scale ranging from 1 (total dependence) to 7 (total independence), yielding a total score ranging from 30 to 210. The FIM–FAM demonstrates high internal consistency (α = .94), and it has excellent interrater reliability, with correlations above .990 for all subscale domains (Colomer et al., 2023).
Finally, QoL was assessed using the Stroke-Specific Quality of Life (SS–QoL; Ramírez & Alvarez, 2008) questionnaire, specifically designed for evaluating the QoL of stroke patients. The Spanish version of this questionnaire has been validated and shown to be reliable and practical. It consists of 38 items grouped into eight domains: physical function, communication, cognition, emotions, social role, ADLs, IADLs, and social/family role. Additionally, it includes two questions about sexual function and employment status. Responses are rated on a scale ranging from 1 (no difficulty) to 5 (extreme difficulty), with total scores ranging from 38 to 190. Lower scores indicate better QoL. The SS–QoL (Fernández-Concepción et al., 2008) has demonstrated strong psychometric properties, with α = .95, and a good test–retest stability with interclass correlation coefficients of .89 to .98 (Ramírez Pérez et al., 2005).
Intervention
MT
For MT, the patient sat in a chair with their forearms on a table, and a mirror was placed between the arms at a right angle to the torso. The affected limb was positioned behind the mirror, out of the patient’s field of view. The healthy limb was adjusted so that the reflection matched the position of the affected limb (see Figure A.1 in the online supplement).
MT was executed in three different modes. In the first mode, the patient attempted to replicate the movement of the healthy hand synchronously with the affected hand. In the second mode, the patient imagined themselves performing the mirrored movement of the healthy hand with the affected hand. In the third mode, the therapist assisted the patient’s affected hand in imitating the movement of the healthy hand. Progression was individually tailored to the patient’s recovery.
Studies have shown that MT not only improves the function of the affected limb during the specific training task but can also have a positive impact on other everyday activities. For example, a study has shown that MT can induce brain changes in the motor area, leading to generalized functional improvement in the use of the affected limb (Ramachandran & Altschuler, 2009). Additionally, another study found that patients who participated in MT not only improved in the direct therapy tasks but also experienced improvements in untrained activities, such as grasping and manual dexterity (Wen et al., 2022). This suggests that the effects of the intervention may extend beyond the specific activities worked on during treatment.
CTE
CTE was structured in three progressive levels—primary, secondary, and tertiary—that guide the therapeutic process through perceptual motor tasks of increasing complexity. Each level focused on specific aspects of movement control, from the management of spasticity to the automation of voluntary motor patterns. Initially, all patients participated in primary-level exercises to acquire proficiency in managing the stretch reflex. Once they achieved this proficiency, they advanced to secondary-level exercises. Later, tertiary-level exercises were introduced, focusing on modifying movements on the basis of perceptual hypotheses, with the aim of automating the control of secondary-level abnormal motor behaviors.
At the primary level, the focus was on addressing spasticity, with the therapist guiding the patient’s movements. At the secondary level, abnormal irradiation (involuntary activation of muscle groups not directly related to a specific action, resulting from alterations in the regulation of the central nervous system) was addressed, and patients performed movements with minimal assistance from the therapist. At the tertiary level, emphasis was placed on controlling voluntary movements, aiming to achieve complete automation of movements without therapeutic assistance.
Studies indicate that the benefits gained through CTE extend beyond the exercises directly targeted during therapy. For instance, CTE has been found to significantly improve motor skills not only in the exercises practiced but also in daily functional tasks. The changes achieved at the tertiary level, where movements are automated, contribute to the patient’s greater independence in real-world situations (Diaz Castro & Rodriguez Lopez, 2019). This suggests that the effects of CTE go beyond the specific tasks, promoting improvements in broader, untrained activities.
TOT
TOT was structured sequentially, adapting in each session to simulate everyday situations, such as ADLs (eating, dressing, toileting), IADLs (making food, washing clothes, handling money, etc.), work, or leisure. Complex activities were divided into simpler tasks to facilitate learning. For example, when performing the ADL of feeding, the task was divided into simple steps in which shoulder flexion, forearm pronation, wrist deviation, and different types of grips (cylindrical grip, palmar grip, interphalangeal grip, subterminal grip, etc.) were worked on independently. These exercises were carried out with different materials, and the difficulty of the tasks was progressively intensified to enhance performance, increasing the joint range, weight, task speed, or accuracy of each simple task and then combining them before performing the complex task. Brief rest periods were interspersed.
Research has suggested that the benefits of TOT extend to functional improvements in various activities beyond those directly practiced in therapy. For instance, a study demonstrated that patients who underwent TOT showed significant improvements in performance of ADLs and IADLs that were not explicitly trained during sessions. The structured, progressive nature of the training helped individuals adapt to and perform complex tasks in their daily lives, thereby enhancing their overall functional independence (Choi & Kang, 2015). This suggests that the effects of TOT can transfer to real-life activities, promoting broader functional gains.
Statistical Analysis
Descriptive analyses of sample characteristics were conducted, with categorical variables presented as absolute frequencies and percentages and continuous variables as means and standard deviations. The normality of the dataset was assessed using the Kolmogorov–Smirnov test (Macía Soler & Moncho Vasallo, 2021).
To analyze differences between groups regarding the various assessments conducted during the intervention, we used analysis of covariance. In this analysis, the treatment group to which participants belonged was considered a fixed factor; the differential scores of the evaluated variables served as dependent variables, and the initial values of these same variables were used as covariates.
To quantify the effectiveness of the interventions carried out, the effect size for each variable was detailed using η2 p, according to the values established by Cohen (1988), in which η2 p < .059 indicates a small effect; η2 p ≥ .059, a medium effect; and η2 p ≥ .138, a large effect.
Statistical analysis was performed using IBM SPSS Statistics (Version 28). A significance level of p < .05 was considered indicative of statistical significance.
Results
The data were collected from 120 patients 1 mo after they had experienced a stroke. Table 1 presents data collected on the sociodemographic and clinical variables. Note that at baseline, there were no statistically significant between-groups differences. All groups were on an equal level before the intervention.
Participants’ Sociodemographic and Clinical Data (N = 120)
Note. CG = control group; CTE = cognitive therapeutic exercise; MT = mirror therapy.
Between the first and second evaluation, the treatment group showed statistically significant differences in functionality, as well as in gross and fine motor skills of (1) the affected upper limb, (2) the quantity and quality of use of the affected upper limb, (3) level of functional independence in ADLs, and (d) QoL (Table 2). Significant differences were observed between the scores of the CG and the two EGs on all evaluated variables, but not between the two EGs.
ANCOVA Analysis of the Treatment Group From the First to the Second Evaluation
Note. EG1 received mirror therapy; EG2 received cognitive therapeutic exercise. ANCOVA = analysis of covariance; ARAT = Action Research Arm Test; BBT = Box and Block Test; CG = control group; FIM–FAM = FIM–Functional Assessment Measure; MAL–30 = Motor Activity Log; SS–QoL = Stroke-Specific Quality of Life Scale.
* p < .05. **p < .001.
Statistically significant between-groups differences were obtained for the ARAT, F(2, 116) = 13.513, p < .001, η2 p = 0.189; BBT, F(2, 116) = 10.741, p < .001, η2 p = 0.156; MAL–30 Quantity and Quality subscales, Fs(2, 116) = 9.850 and 6.143, ps < .001 and .003, η2 ps = 0.254 and 0.096, respectively; FIM–FAM, F(2, 116) = 5.288, p = .006, η2 p = 0.084; and SS–QoL, F(2, 116) = 7.331, p < .001, η2 p = 0.112.
Statistically significant differences, shown in Table 3, were observed between the first and second evaluations for the functionality, as well as the gross and fine motor skills, of (1) the affected upper limb, (2) the quantity and quality of use of the affected upper limb, and (3) QoL. However, no statistically significant differences were observed in functional independence in ADLs. Significant differences were also observed between the scores of the CG and the two EGs on all significant variables mentioned, but not between the EGs. Statistically significant differences were obtained on the ARAT, F(2, 116) = 8.138, p < .001, η2 p = 0.123; the BBT, F(2, 116) = 11.987, p < .001, η2 p = 0.171; the MAL–30 Quantity and Quality subscales, Fs(2, 116) = 7.978 and 8.958, ps < .001, η2 ps = 0.121 and 0.134, respectively; and SS–QoL, F(2, 116) = 10.244, p < .001, η2 p = 0.150. However, no statistically significant differences were observed for the BBT, F(2, 116) = 1.674, p = .197, η2 p = 0.058, or for the FIM–FAM, F(2, 116) = 2.088, p = .129, η2 p = 0.035.
ANCOVA Between the Treatment Group and the First and Third Evaluation
Note. EG1 received mirror therapy; EG2 received cognitive therapeutic exercise. ANCOVA = analysis of covariance; ARAT = Action Research Arm Test; BBT = Box and Block Test; CG = control group; FIM–FAM = FIM–Functional Assessment Measure; MAL–30 = Motor Activity Log; SS–QoL = Stroke-Specific Quality of Life Scale.
* p < .05. **p < .001.
No statistically significant differences were found between the second and third assessments for any of the variables analyzed, indicating that the long-term results of the interventions were maintained.
Discussion
The participants demonstrated a significant improvement in scores from the first to the second evaluation after the application of complementary treatment, as well as in the long term. This indicates that both EGs showed greater improvement on all variables analyzed.
Statistically significant differences were observed for the functionality and fine and gross motor skills of (1) the affected upper limb, as measured with the ARAT and BBT; (2) the quantity of use of the affected upper limb, measured with the MAL–30 and FIM–FAM; and (3) QoL, measured with the SS–QoL. Other studies using the same assessment instruments have also suggested that MT is beneficial for improving motor functionality of the affected upper limb (Carayol et al., 2019; Damsbo et al., 2020; Koevoets et al., 2022). Additionally, mirror neurons are activated when observing, imagining, or attempting to execute movements (Van Vulpen et al., 2016).
Although we have found no previous studies that use the same combination of therapies used here, our research provides evidence that rehabilitation using this combination of techniques leads to improvements in motor performance among patients who have had a stroke. This finding is supported by other research (Kim & Shim, 2015; Lim et al., 2016; Mirela Cristina et al., 2015; Park et al., 2015).
Furthermore, QoL in the EGs was higher than in the CG. These results are consistent with other studies indicating that the use of MT and CTE improves QoL (Damsbo et al., 2020) and that various forms of intervention significantly enhance QoL (Alsubiheen et al., 2022; Oberlin et al., 2017; Ren et al., 2022). Statistically significant differences were also observed for the variables of quality of use of the affected upper limb (p = .003) and level of functional independence in ADLs (p = .006). Previous studies have shown that specific rehabilitation interventions improve motor capacity and functionality (Carayol et al., 2019; Damsbo et al., 2020; Koevoets et al., 2022; Van Vulpen et al., 2016).
Similarly, statistically significant differences were observed between the two EGs and the CG, indicating superior improvement in both EGs compared with the CG. However, no statistically significant differences were found between the two EGs. Therefore, it appears that undergoing rehabilitation through a combination of techniques aimed at restoring the mobility and functionality of the affected limb, regardless of its nature, is more effective than implementing a more conventional program (Oberlin et al., 2017; Ren et al., 2022; Van Vulpen et al., 2016).
Moreover, significant differences were observed in the quantity and quality of use of the affected upper limb, a result that is supported by other studies indicating that, after a stroke, many patients continue to use their affected upper limb in ADLs, achieving normal performance (Lundquist et al., 2022).
The study has certain limitations that warrant consideration. First, the small sample size suggests that expanding it would enhance its representativeness and statistical power. Second, regarding the inclusion and exclusion criteria, potential adjustments could involve broadening the age range or including participants with milder cognitive impairments because these factors could increase the pool of eligible participants while still maintaining the study’s integrity. Third, the study commenced before the pandemic, which affected recruitment efforts over an extended period.
Some future research directions include long-term follow-up of patients to assess outcomes over an extended period. Additionally, integrating interventions with other therapeutic methods could be explored. Last, exploring emotional variables such as anxiety, depression, and motivation could be valuable in future research, because these factors often influence recovery and patient engagement in rehabilitation.
Implications for Occupational Therapy Practice
Occupational therapy plays a crucial role in the functional recovery and enhancement of QoL for patients with stroke. However, evidence concerning many rehabilitation techniques and their optimal combination remains incomplete. The study presented here introduces an additional tool for rehabilitation, demonstrating various patient benefits, including improved hand functionality, fine and gross motor skills of the hand, level of functional independence in ADLs, and QoL through a combination of therapeutic techniques. This trial has the following implications for occupational therapy practice: Practitioners can support the inclusion of specific and gradual tasks tailored to the individual needs of the patient, promoting functional recovery. The integration of specific techniques, such as task simulations in TOT, is essential for patients with stroke to regain practical and functional skills. Practitioners need to adopt comprehensive rehabilitation approaches that address multiple dimensions of poststroke recovery.
Conclusion
The results of this study demonstrate that the combination of MT or CTE with TOT is effective in improving the functionality of the affected upper limb, fine and gross motor skills, functional independence in ADLs and IADLs, and the QoL of patients in the subacute phase after a stroke. At postintervention and the 3-mo follow-up intervention, both EGs showed significant improvements on all measured variables compared with the CG, with no significant differences between the EGs. Both techniques produced positive outcomes in improving the studied variables. Therefore, both combinations are viable options for promoting functional recovery for stroke patients in the subacute phase.
These findings are particularly relevant for occupational therapists because they provide empirical evidence supporting the use of these combined techniques in clinical practice. The integration of these interventions allows for personalized treatments tailored to each patient’s specific needs, optimizing their functionality and QoL. Additionally, it facilitates the implementation of evidence-based strategies that promote neuroplasticity and recovery of the affected upper limb. Furthermore, the findings enable occupational therapists to adopt a comprehensive approach to addressing the physical, emotional, and social dimensions of poststroke recovery.
Supplemental Material
Supplementary material for Effect of Mirror Therapy Versus Cognitive Therapeutic Exercise on Upper Limb Functionality, Autonomy, and Poststroke Quality of Life: A Randomized Trial
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050834.pdf for Effect of Mirror Therapy Versus Cognitive Therapeutic Exercise on Upper Limb Functionality, Autonomy, and Poststroke Quality of Life: A Randomized Trial by Jessica Fernández-Solana, Rodrigo Vélez-Santamaría, Adrián Moreno-Villanueva, Sergio Álvarez-Pardo, Jerónimo González-Bernal, Mirian Santamaría-Peláez and Josefa González-Santos in The American Journal of Occupational Therapy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.