
Abstract
The study results support the efficacy of a dynamic orthosis in muscle strength training for stroke patients.
Stroke is the leading cause of death and dysfunction among adults (Chronic Disease Prevention and Control Team, 2024; Feigin et al., 2021). Statistics indicate that 51.72% of stroke survivors still present with dysfunction after 6 mo, and a major problem among poststroke individuals is upper limb dysfunction (Chronic Disease Prevention and Control Team, 2024), which is usually accompanied by spasticity, weakness, and abnormal muscle coactivation. In fact, 35% of stroke patients present upper limb weakness, and 46% experience impairments in upper limb coordination (Dalton et al., 2024). The capacity of dexterous finger movements of stroke patients contributes to functional independence and can serve as outcome predictors for activities of daily living (Lodha et al., 2010; Patel et al., 2020; Veerbeek et al., 2011). Stroke patients may experience the inability to actively extend their fingers to release objects held in their hand during grasp-and-release tasks. They may also experience incoordination in fine motor control. For patients who lack the capacity for voluntary movement in their paretic hand, the use of the dynamic spring-loaded hand orthosis during rehabilitation may provide additional benefits. The dynamic spring-loaded hand orthosis has been shown to facilitate upper limb recovery among stroke patients (Butler et al., 2006; Franck et al., 2013; Hoffman & Blakey, 2011). The use of dynamic orthoses can increase motivation, the amount of practice, and wrist and finger strength, as well as lead to small improvements in upper limb performance of stroke patients (Barry et al., 2012; Chang & Lai, 2015; Franck et al., 2013; Kerr et al., 2020).
In a grasp-and-release task, the steel wire springs in the dynamic spring-loaded hand orthosis provide a passive extension force for straightening the fingers to overcome spasticity or to compensate for weakness. Simultaneously, the springs also provide resistance during finger flexion. This resistance can be used to strengthen hand muscles and thereby reduce weakness. The springs in a dynamic spring-loaded hand orthosis can also provide variable resistance. There are two advantages of variable resistance with regard to improving muscle strength. First, the resistance can be adjusted to the individual’s points of difficulty (the most challenging angles during movement) based on the individual’s movement speed (i.e., less resistance at slower speeds). Variable resistance is the favored modality for assisting individuals to overcome difficulty points (Kompf & Arandjelović, 2016). Second, variable resistance is known to improve concentric resistance training of finger flexors and eccentric resistance training of finger extensors during grasping. Evidence has shown that more paretic muscular activation after stroke is induced in eccentric resistance training than in concentric resistance training (Clark & Patten, 2013). Studies have confirmed that variable resistance can provide greater improvements than constant resistance in muscle strength and neuromuscular activity among healthy adults (Lin et al., 2022; Smith et al., 2019; Walker et al., 2013). To our knowledge, changes in muscular activity and muscular coactivation of stroke patients with the use of the dynamic spring-loaded hand orthosis have not been thoroughly studied yet.
This study aimed to analyze EMG signals to understand the changes in muscular activity and muscular coactivation during the execution of hand activities when the dynamic spring-loaded hand orthosis was used. This study involved two experimental conditions: the orthosis condition and the hand condition. In the orthosis condition, we examined the differences in muscular activity and muscular coactivation, including the extensors and flexors, between wearing and not wearing the orthosis. In the hand condition, we used the unaffected hand as a control to understand the muscle activity and muscular coactivation in the affected hand.
Method
Participants
Patients were invited to participate if they met the following inclusion criteria: diagnosis of first-time stroke, older than age 18 yr, ability to provide consent, partial finger movement (defined as ≥10° of active finger flexion), and time since stroke onset of at least 3 mo. Participants were excluded if they were able to extend the fingers fully, had deficits in cognition or communication that would impede participation (determined by a Mini-Mental State Examination score of less than 24 out of 30; Folstein et al., 1975), or had severe comorbidities or other health conditions that were counterindications of upper limb rehabilitation. In this study, a total of 32 participants were invited; however, 2 were excluded because of musculoskeletal discomfort in their unaffected hands. Ultimately, 30 participants took part in the study. All participants received explicit information about the experimental design and gave signed informed consent before the experimental procedures began. This study was approved by the Research Ethics Committee of the Research Ethics Committee of Fu-Jen Catholic University, New Taipei City, Taiwan (FJUH112295). The protocol was in accordance with the Declaration of Helsinki and followed institutional ethics board guidelines for research on humans.
Instruments
Orthosis
The special feature of our dynamic orthosis is that it can provide resistance during finger flexion and assistance during finger extension, as well as resistance during grasping and assistance during releasing. This dynamic orthosis was customized by occupational therapists with more than 2 yr of clinical experience. It comprises one elastic wire with a diameter of 1.2 mm. The distal ends of the wires have Velcro loops for the thumb, index finger, and middle finger (Figure 1).
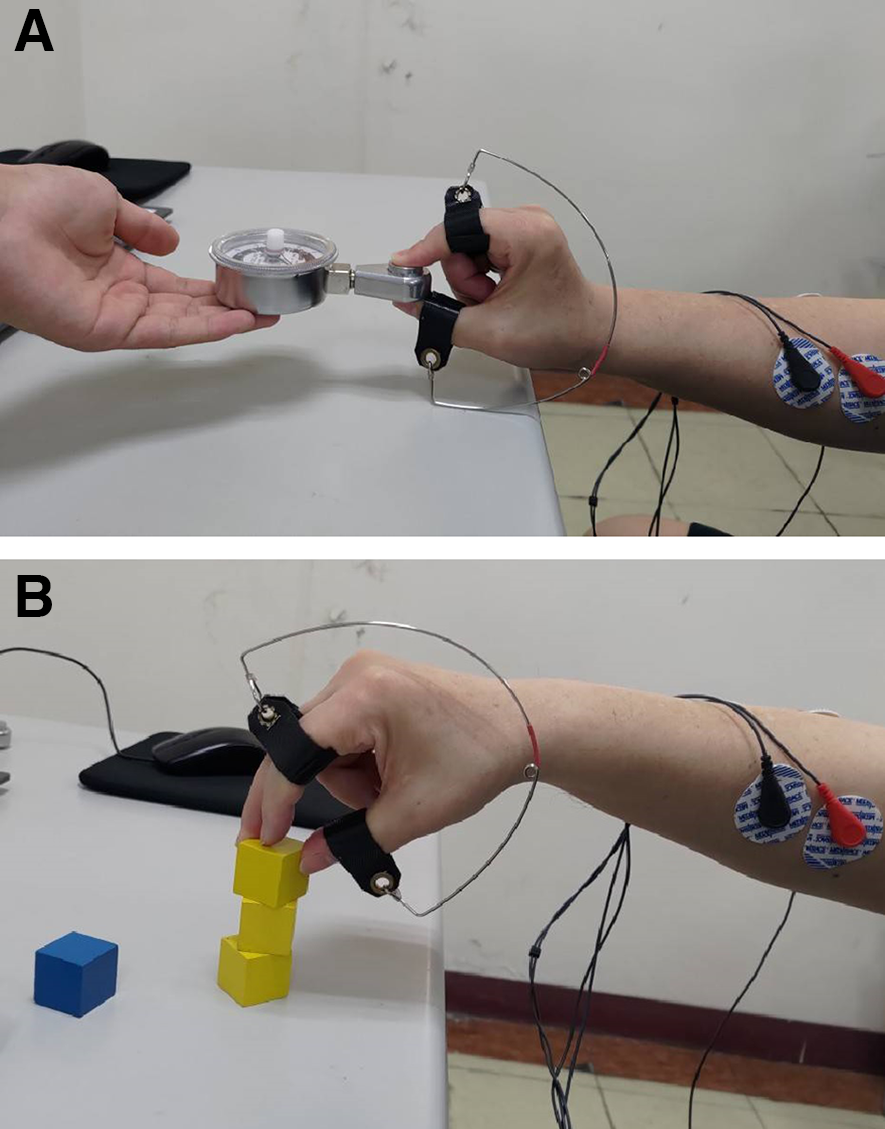
Surface electromyography was recorded during (a) the isometric task and (b) the dynamic task while the orthosis was worn.
Collection and Processing of EMG Signals
We collected the EMG signals by using surface EMG with a Nexus-10 device (Mind Media BV, Roermond, the Netherlands) at 1,024 Hz. The EMG signals were processed in the BioTrace+ software packaged with NeXus systems (MindMedia, Herten, the Netherlands). The raw EMG signals were digitally amplified by a gain of 500, bandpass filtered to 20–500 Hz, full-wave rectified, and smoothed with a 100-ms average window. We used root-mean-square (RMS) to quantify the EMG signals of muscle exertion in the middle 3 s of each trial. The EMG amplitude was processed by integrating the RMS during specific time periods.
Pinch Gauge
A dynamometer (a 50-lb Baseline hydraulic pinch gauge; Baseline, New York, NY) was used to measure the maximal pinch strength and to execute the exam in the isometric task (Figure 1a).
Experimental Design
We conducted a 2 (orthosis condition) × 2 (hand condition) mixed repeated measures experimental design. To investigate the effect of wearing the orthosis on muscle activity, we used two experimental conditions: the wearing condition and the free condition. We used the hand condition to compare the affected hand and unaffected hand. The orthosis condition was a within-subject variable, and the hand conditions was a between-subject variable.
Procedure and Tasks
Experimental Procedure
Participants sat comfortably at a table in a quiet room. After appropriate skin preparation, the surface electrodes were placed on the participant. We recorded the surface EMG of the flexor digitorum superficialis (FDS) and extensor digitorum common (EDC). We placed the surface electrodes over the skin surface of the muscle belly of the FDS and EDC, according to the configuration specified in Hermens et al. (2000). Then we collected the EMG signals of maximal voluntary contractions (MVC) of the FDS and EDC for normalization during signal processing. The maximal pinch strength was measured as an exertion indicator in the isometric task. Two experimental tasks (an isometric task and a dynamic task), the orthosis condition (wearing condition vs. free condition), and the hand condition (affected hand vs. unaffected hand) were arranged in randomized order. The whole experiment lasted approximately 2 hr (Figure 2).
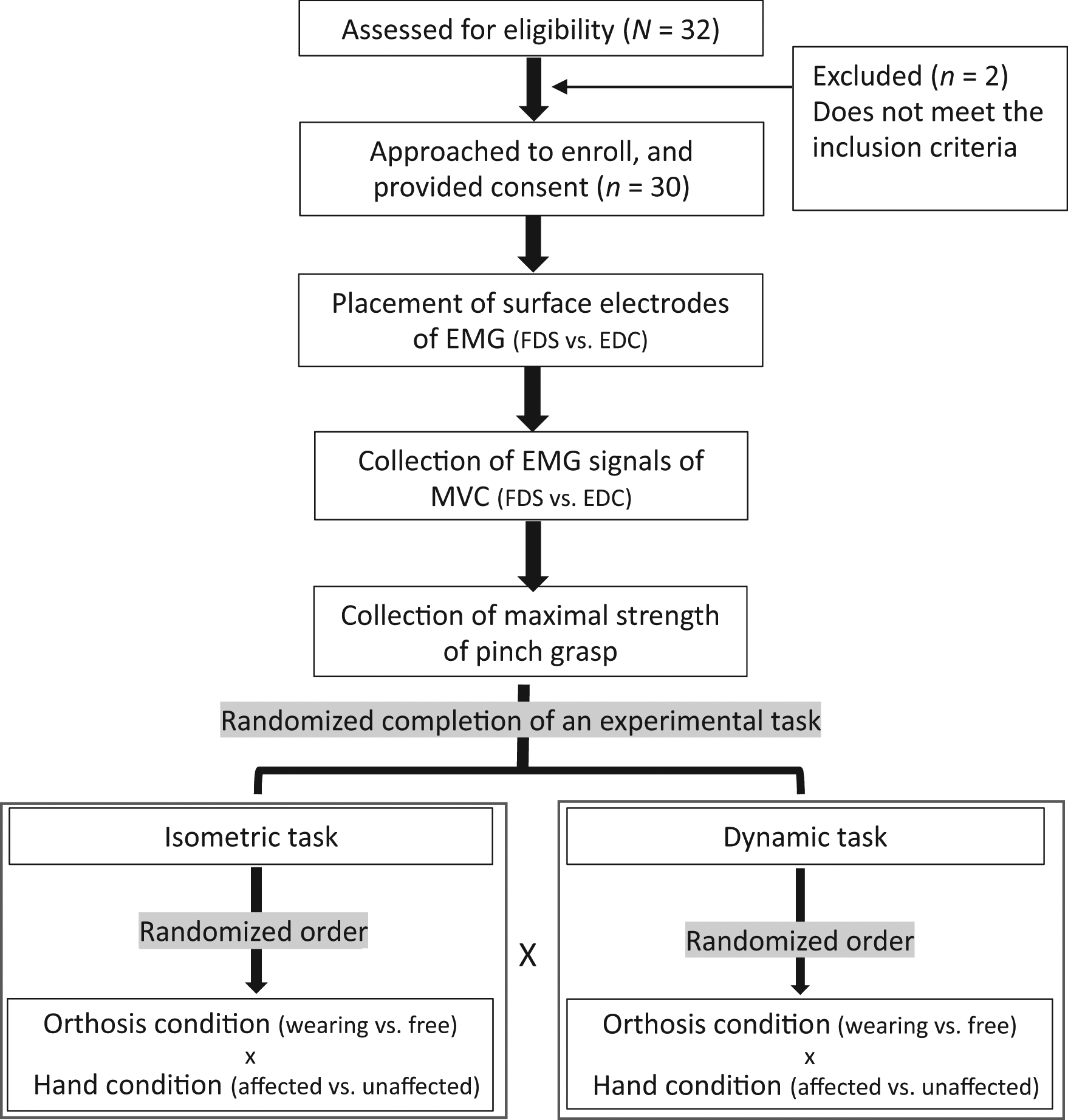
Flow chart and experimental procedure of the study.
MVC
Participants were instructed to perform maximal isometric voluntary contraction to resist the force exerted by the examiner for the FDS and EDC separately. Each contraction lasted 5 s and was performed three times with 1-min intervals between contractions. The EMG amplitude of the MVC was processed by averaging the three integrated RMS during a 3-s window encompassing the center of each contraction.
Maximal Pinch Strength
We measured maximal pinch strength with a three-jaw chuck grasp on a pinch gauge. Participants were instructed to perform the pinch task with maximal effort three times, with 1-min breaks between trials. The maximum pinch strength score was averaged from the three trials. Then we used 30% of the maximal pinch strength of each participant as the exertion indicator in the following isometric task because 30% of maximal grip strength is required in the largest group of general activities of daily living (Faes et al., 2006). In a previous study, Brookham et al. (2010) used this amount to simulate an exertion task with a light hand tool.
Isometric Task
In the isometric task, isometric contraction was exerted with a three-jaw chuck grasp. We instructed participants to grasp the pinch gauge with a three-jaw chuck grasp and maintain the grasping action for 5 s (Figure 1a). Participants were told to increase the force until it reached their personal 30% of maximal pinch strength. Visual feedback (a red target) was shown on the window of the pinch gauge. Participants practiced the task in two familiarization trials before the experiment began. During the experiment, the three contractions each lasted 5 s and were separated by 1-min intervals. The EMG signals were collected synchronously, and signals during the central 3-s window were used. We processed the EMG amplitude of the isometric task by averaging the three integrated RMS of the constant three-jaw chuck grasp.
Dynamic Task
In the dynamic task, participants were asked to pick up one block at a time and stack the blocks on top of one another, for a total of five blocks (Figure 1b). A familiarization phase of two stacking trials was performed before the experiment began. During the experiment, the stacking of five building blocks was regarded as a single cycle, and three cycles were executed with 30-s rest periods between cycles. The EMG signals were collected synchronously, and signals during a 3-s central window were used. We processed the EMG amplitude of the dynamic task by averaging the three integrated RMS of the grasp-and-release contractions.
Dependent Variables
We calculated two dependent variables—normalized electromyography (nEMG) and cocontraction index (CCI)—from the EMG amplitudes of the EDC and FDS according to the assigned experimental conditions.
nEMG
nEMG refers to the integration of muscular activity divided by the integration of maximum voluntary muscular contraction activity (MVC). For example, the nEMG of EDC equals the integrated EMG activity of the EDC in an assigned experimental condition divided by the integrated EMG activity of the EDC in the maximum exertion condition.
CCI
We used the CCI to measure the amount of cocontraction between agonists and antagonists during limb movements (Frost et al., 1997). In this study, we used the overlap of the linear envelopes of the FDS and EDC as an indicator of cocontraction during upper limb movements. The CCI was calculated with the following formula:
where Aij (t) is the overlapping activity of EMG linear envelopes for FDSi and EDCj. The CCI value varied from 0 to 1, with 0 representing complete absence of overlap between the two signal segments and 1 indicating complete overlap between the two signal segments.
Statistical Analysis
The demographic data are presented as means or percentages. For all dependent variables, including nEMG and CCI, we first tested the normal distribution with the Shapiro–Wilk test. The results indicated that the data had a nonnormal distribution (p > .05). Thus, nonparametric analysis was chosen. We conducted Mann–Whitney U test on the hand condition (affected vs. unaffected) for between-subject differences and the Wilcoxon signed rank test on the orthosis condition (wearing vs. free) as a within-subject variable. Significance was set at p < .05. Results were analyzed in IBM SPSS Statistics (Version 20).
Results
Thirty people with stroke (M age = 63.567 yr, SD = 10.566 yr) participated in this study. Demographics and clinical information of participants are listed in Table 1.
Demographic and Characteristic Information of the Stroke Participants (N = 30)
Note. FMA-UE = Fugl–Meyer Assessment for upper extremity; MAS = Modified Ashworth Scale.
Muscle Activity in the Isometric Task
The nEMG–FDS results were significantly higher in the wearing condition than in the free condition (p = .034) for the affected hand condition and in the wearing condition than in the free condition (p = .004) for the unaffected hand condition. No differences were found between the affected and unaffected hand conditions in the wearing (p = .130) or free (p = .167) condition (Table 2).
Means (Standard Deviations), Medians (Interquartile Ranges), 95% Confidence Intervals, and Statistical Results of nEMG for Hand and Orthosis Conditions
Note. CI = confidence interval; FDS = flexor digitorum superficialis; EDC = extensor digitorum common; IQR = interquartile range; Mdn = median; nEMG = normalized electromyography.
The nEMG–EDC results were significantly higher in the wearing condition than in the free condition (p < .001) for the affected hand condition and in the wearing condition than in the free condition (p = .001) for the unaffected hand condition. No differences were found between the affected and unaffected hand conditions in the wearing (p = .058) or free (p = .707) condition (Table 2).
Muscle Activity in the Dynamic Task
The nEMG–FDS results were significantly higher in the wearing condition than in the free condition for the affected hand condition (p = .002) but not for the unaffected hand condition (p = .456). No significant differences were observed between the affected and unaffected hand conditions for the wearing (p = .316) or free (p = .786) condition (Table 2).
The nEMG–EDC results were significantly higher in the wearing condition than in the free condition for the affected hand condition (p = .008) and the unaffected hand condition (p = .002). In the wearing condition, the nEMG of EDC was significantly higher in the affected hand condition than in the unaffected hand condition (p = .010) as well as in the free condition (p = .019; Table 2).
Cocontraction in the Isometric Task
The results showed that the CCI was significantly lower in the affected condition than in the unaffected condition in the wearing condition (p = .005), but no difference was found in the free condition (p = .213). No differences were found between the wearing and free conditions in the affected hand condition (p = .477) or the unaffected hand condition (p = .177; Table 3).
Mean (Standard Deviation), Median (Interquartile Range), 95% Confidence Interval, and Statistical Results of CCI for Hand Condition and Orthosis Condition
Note. CCI = cocontraction index; Mdn = median.
Cocontraction in Dynamic Task
No significant differences in CCI were found between the wearing and free conditions in the affected hand condition (p = .797) and in the unaffected hand condition (p = .062). For the wearing condition, the results indicated no significant differences in CCI between the affected and unaffected hand conditions (p = .641) nor for the free condition (p = .709; Table 3).
Discussion
This study aimed to analyze EMG signals to understand the changes in muscular activity and muscular coactivation during the execution of hand activities with the use of a dynamic spring-loaded hand orthosis. The results indicated that, in both isometric and dynamic tasks, the muscle activity of the affected hand was significantly higher when the orthosis was worn than when it was not. In the comparison of muscle activity between the unaffected and affected hands, significant differences were found only in the muscle activity of the EDC during the dynamic task. The EDC activity of the affected hand was significantly higher than that of the unaffected hand during the dynamic task. The results of cocontraction indicated that only in the isometric task was the cocontraction level of the affected hand significantly lower than that of the unaffected hand when the orthosis was worn. No differences in cocontraction levels were found in the other experimental conditions.
Enhanced Muscle Contraction of the Affected Hand During Orthosis Use
Our study found that the muscle activity of the affected hand (including FDS and EDC) was significantly higher with the orthosis than without it. This result was in line with those of studies by Clark and Patten (2013) and Morris et al. (2004), which showed that resistance training can improve muscle strength (Morris et al., 2004) and muscular activity (Clark & Patten, 2013) among stroke patients. Chang and Lai (2015) reported improvements in wrist and finger strength after a 1-mo dynamic orthosis intervention. In our study, the resistance was provided by the steel wire springs of the dynamic orthosis, and the resistance of the springs enhanced muscle contractions as would occur in resistance training.
Intense Muscular Activity in the EDC During Dynamic Tasks
Our findings indicated that the muscular activity of the EDC of the affected hand was significantly higher than that of the unaffected hand during dynamic activities, whereas no such phenomenon was noted during isometric activities. The affected hand of stroke patients requires greater muscle activity than the unaffected hand to overcome the same level of loading (Suresh et al., 2015). Hu et al. (2007) applied mechanical active assistance to stroke patients and found a significant increase in muscular activity of the affected hand; moreover, the increase was significantly higher in the extensor (antagonist) than in the flexor (agonist). Clark and Patten (2013) found that for stroke patients, eccentric contraction training elicited greater muscle activity than did concentric contraction training. In our dynamic tasks, the resistance borne by the EDC (antagonist) during grasping was indeed eccentric resistance training. Our results support the effectiveness of the steel wire springs in the dynamic orthosis in providing eccentric resistance training of the affected hand.
Coactivation Activation in Orthosis Condition
Our results indicated that the cocontraction level was significantly lower in the affected hand than in the unaffected hand with orthosis use in the isometric task. No differences in cocontraction levels were found in the other experimental conditions. Therefore, the coactivation patterns our participants exhibited were more abnormal in the affected hand than in the unaffected hand. These abnormal coactivations are related to pathological synergistic movements (Dewald et al., 1995). It is known that the pathological synergistic movements in the affected hands of stroke patients, which exhibit characteristics such as movement delays and high intensity, differ from those of healthy individuals (Simkins et al., 2014). Previous studies have indicated that the agonists and antagonists involved in synergistic movements of the affected limbs of stroke patients are different from those of healthy individuals (Hu et al., 2006). In addition, the abnormal coactivation in the muscle groups occurs around adjacent joints, such as the coactivation between elbow flexors and wrist extensors during wrist extension (Hu et al., 2006). Our study investigated only the coactivation between the FDS and EDC. It will be necessary to measure the coactivation of other adjacent muscle groups in future studies.
Strengths and Limitations
Our research shows the benefits of dynamic spring-loaded hand orthoses on forearm muscular activation. However, our study had several limitations, including the small sample size, the lack of longitudinal follow-up, and the lack of compliance beyond motivation, amount of practice, and ease of use. The participants in our study meet tight selection criteria, and therefore the findings of this study are applicable only to stroke patients whose motor abilities allow minimal voluntary finger extension. After taking these limitations into consideration, the clinical application and potentially meaningful improvements with regard to daily activities will be confirmed. An extensive study of a conventional rehabilitation program should be conducted to further validate the finding that wearing a dynamic orthosis can increase the antagonist’s activation of the hemiplegic hand.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ The dynamic spring-loaded hand orthosis could facilitate the muscular activity of stroke patients’ affected hand in both isometric and dynamic tasks. ▪ The muscle activity of the EDC of the affected hand was significantly higher than that of the unaffected hand during the dynamic task. ▪ Application of a dynamic spring-loaded hand orthosis in rehabilitation programs can improve stroke patients’ voluntary hand movement.
Conclusion
To our knowledge, this is the first study to use EMG to investigate the myoelectric phenomena of upper extremity muscles of stroke patients wearing a dynamic spring-loaded hand orthosis. We found that muscular contractions were significantly higher when the orthosis was worn than when it was not. Our results support the efficacy of variable resistance in muscle strength training for stroke patients. In addition, EDC contraction was significantly enhanced during dynamic orthosis use, supporting the inference that dynamic orthoses can strengthen the antagonist through eccentric contraction training. For greater understanding of the muscular coactivation patterns and pathological synergy during the use of dynamic orthoses, other muscles around adjacent joints should be investigated.
Footnotes
Acknowledgments
We thank the participants and researchers who took part in this study. We also thank the Fu Jen Catholic University Hospital, New Taipei City, Taiwan, for their financial support (PL-202308040-M).