
Abstract
The findings of this study serve as the foundation for occupational therapists to design and develop novel clinical interventions to address role participation after mild to moderate stroke.
Roles are defined as sets of behaviors, responsibilities, and principles guiding how people engage in and participate in vital occupations. Role participation reflects a balance between social expectations, personal desires, and needs, providing a sense of purpose to daily activities (Kielhofner, 2008). This purpose is grounded in people’s sense of responsibility toward their roles (Bonsaksen, 2018), which, in turn, contributes to defining their personal identity (Vendrusculo-Fangel et al., 2019). Personal identity enables people to feel represented by their actions and interpret feedback from others through the lens of their own values. Roles shape this identity by providing people with a context for their performance, which is closely linked to their personal values (Bonsaksen, 2018). Understanding how people manage their role participation and fulfill their responsibilities on the basis of their values provides valuable insights into their desires, needs, and expectations (American Occupational Therapy Association, 2020).
The level of role participation often declines after a stroke, partly because of cognitive factors (Stolwyk et al., 2021). Cognitive impairment is often a strong predictor of engagement in daily activities for 6 to 12 months poststroke (Mole & Demeyere, 2020). Specifically, research has shown that cognitive deficits, such as those in memory, executive function, and attention, are associated with reduced levels of activity participation (Spitzer et al., 2011). The mechanisms’ involvement in this association may result from role participation demanding high cognitive effort, because it requires performing complex activities, adaptability, responsibility, and social interaction with others (Viscogliosi et al., 2011). However, whether other underdiagnosed cognitive deficits, such as apraxia, are related to role participation remains unexplored.
Upper limb apraxia (ULA) is a cognitive impairment that hinders the ability to perform deliberate movements in response to environmental demands (Buxbaum & Randerath, 2018). Apraxia exhibits a wide spectrum of manifestations, affecting movements involving objects (transitive), movements without objects (intransitive), meaningful gestures (symbolic), gestures without cultural sense (nonsymbolic), and imitating and pantomime (Vanbellingen et al., 2010). ULA is characterized by errors in action execution, including issues with timing, spatial orientation of the upper limb, and hand or arm positioning (Scandola et al., 2021). Stroke is the leading cause of ULA, with a prevalence estimated to be between 28% and 54% among survivors (Zwinkels et al., 2004). ULA can affect daily life by posing challenges in the execution of tasks and activities. For this reason, ULA affects the person’s independence, participation, and community reintegration (van Heugten et al., 2000).
Considering that ULA interrupts essential daily movements, clinical reasoning indicates that it could influence role participation in patients with stroke. This potential relationship could be explained because ULA often leads to imprecise or absent movements, increasing dependence on activities of daily living (ADL; van Heugten et al., 2000). On the other hand, apraxic errors can affect an person’s perception of self-efficacy (Sánchez-Bermejo et al., 2023), which is associated with the ability to engage in roles poststroke (Lo et al., 2022). Furthermore, ULA has been shown to have an influence on particular roles, such as the ability to return to work (Wang et al., 2014). Despite these connections, the association between ULA and role participation in patients with stroke remains unexamined. Therefore, in this study, we aim to evaluate whether ULA is related to role participation in patients with mild to moderate stroke.
Method
Study Design
A cross-sectional correlational study was conducted.
Setting
Patients with stroke were recruited from randomly selected public primary care centers in the province of Granada (Andalusia, Spain). The assessment of role participation and ULA was conducted by a researcher with specialized training in poststroke evaluations and 10 years of clinical expertise in ULA. The study protocol received approval from the Ethics Committee for Biomedical Research CEI-Granada in the province of Granada under Reference Number 1503-N-21. This research study adhered to the ethical guidelines outlined in the Declaration of Helsinki, ensuring ethical conduct throughout the research process.
Study Size and Participants
G*Power was used to determine the sample size. We conducted a priori computed required sample size estimation using an F test family with a linear multiple regression fixed model. The analysis included seven predictors and an R2 deviation from zero. The estimated sample size required to ensure the representativeness of the study’s results was determined to be 153 participants, considering a moderate effect size of f 2 = .15 (Cohen, 2013; Fey et al., 2023), a desired statistical power of 95%, and a significance level of .05.
To be included in the study, participants had to have a confirmed stroke diagnosis, be at least 18 years old, and be fluent in Spanish. Exclusion criteria were as follows: ▪ a diagnosis of brain damage other than stroke ▪ severe stroke sequelae, as assessed by the most recent reported scores on the National Institutes of Health Stroke Scale (NIHSS; Montaner & Álvarez-Sabín, 2006) ▪ current hospitalization for stroke or in the acute phase (less than 3 mo since the stroke; Bernhardt et al., 2017) ▪ severe cognitive impairment reported in the clinical history by the Mini-Mental State Examination (Lobo et al., 1999) ▪ spatial neglect, as determined with the Star Cancellation test (Sánchez-Cabeza et al., 2017) ▪ a diagnosis of severe intellectual disability ▪ a diagnosis of severe mental disorder ▪ musculoskeletal disorders (Walker-Bone et al., 2004) ▪ peripheral nervous system injuries (Khan & Perera, 2020) ▪ uncorrected sensory impairments.
Study Variables and Measurement Instruments
Sociodemographic Data, Lifestyle Behaviors, and Clinical Characteristics
We collected sociodemographic data and lifestyle behaviors using an ad hoc questionnaire. This included information about gender, age, marital status, educational level, smoking, alcohol and caffeine consumption, daily sleep duration, and physical activity. Clinical characteristics were compiled that covered the dominant hand, stroke type, affected hemisphere, time since stroke onset, presence of hemiplegia, and whether the participant had received occupational therapy rehabilitation after the stroke.
Role Participation
Role participation was assessed using The Role Checklist, which consists of two parts. The first part includes 30 items assessing role participation in the past, present, and expected future participation within 10 roles: student, worker, volunteer, caregiver, home maintainer, friend, family member, religious participant, hobbyist–amateur, and participant in organizations. The responses are dichotomous, with yes or no options for each temporal assessment. The second part comprises 10 items that measure the value or importance that each participant assigns to each role, using a 3-point scale with responses ranging from 1 (not valued at all) to 3 (highly valued). The Spanish translation from the English version demonstrated a strong idiomatic correlation, with a κ index of .91 for the first part of the instrument and .80 for the second part (Colón & Haertlein, 2002). From this checklist, six indices were extracted on the basis of previous evidence (Vendrusculo-Fangel et al., 2019), as explained in the following text. Additionally, Table 1 provides a detailed description of each index in the instrument.
Summary of Role Checklist Indices
Note. X indicates that the index is directly based on the specific data of the Role Checklist. For indices involving comparisons between two timepoints, the minuend is the number from which another number is being subtracted and the subtrahend is the number being subtracted. Dashes indicate “no use” in the calculation of that index.
▪ Level of current role participation: This index measures the number of roles in which people participate. The score ranges from 0 to 10 points, with higher scores indicating participation in a greater number of roles.
▪ Changes in role participation after stroke: This index compares pre- and poststroke role participation. Scores range from −10 to 10 points; positive scores indicate a decrease in role participation, and negative scores indicate an increase in the number of roles in which people participate. A score of 0 points indicates no change in role participation after a stroke.
▪ Expectations of future role participation: This index measures the number of roles that participants expect to take on in the future. Scores range from 0 to 10 points; higher scores indicate a greater expectation of role participation.
▪ Comparison between future expectations and current role participation: This index measures the gap between future role expectations and current role participation. Scores range from −10 to 10 points. Positive scores indicate an increase in expected future participation, whereas negative scores indicate a decrease in expected future role participation. A score of 0 points indicates that future expectations are equal to current role participation.
▪ Comparison between future expectations and prestroke role participation: This index measures the difference between expectations for future participation and participation before the stroke. The score ranges from −10 to 10 points. Positive ratings indicate increased expectations for future participation compared with pre-stroke levels, whereas negative scores reflect decreased expectations. A score of 0 points indicates that future expectations are the same as prestroke participation.
▪ Assigned value or importance to role participation: This index measures the value that participants assign to roles. Score range from 0 to 20 points, with higher scores indicating a greater value placed on roles, regardless of whether respondents are actively participating in them.
Upper Limb Apraxia
ULA was evaluated in this study across nonsymbolic imitation, intransitive imitation, transitive imitation, nonsymbolic pantomime, intransitive pantomime, transitive pantomime, and praxis function in daily life activities. ULA was registered with the Test of Upper Limb Apraxia (TULIA) and the ADL Observations scale. Before assessing upper limb apraxia, we conducted observational assessments of the tone, strength, and muscular endurance of both limbs. In cases in which the participant exhibited hemiparesis or hemiplegia in the dominant limb, the movement was first requested with the dominant limb and then with the nondominant limb.
The TULIA Apraxia test includes 48 items divided into six subtests: ▪ nonsymbolic imitation (meaningless actions) ▪ intransitive imitation (communicative gestures) ▪ transitive imitation (tool-related actions) ▪ nonsymbolic pantomime ▪ intransitive pantomime ▪ transitive pantomime.
Each item is scored on a Likert scale with scores ranging from 0 to 5 points, with a score of 5 points indicating the absence of apraxic errors. The total score ranges from 0 to 240 points, with lower scores indicating a higher level of apraxia. Participants completed the TULIA Apraxia test using their dominant limb. The TULIA Apraxia test has demonstrated strong psychometric properties, including satisfactory internal consistency of its subtests, with Cronbach’s α values ranging from .67 to .92 (Vanbellingen et al., 2010). In terms of reliability for the present study sample, it is acceptable, with Cronbach α values of .83 for nonsymbolic imitation, .75 for intransitive imitation, .72 for transitive imitation, .78 for nonsymbolic pantomime, .70 for intransitive pantomime, and .79 for transitive pantomime.
The ADL Observations scale was used to evaluate praxis function in daily life activities. This instrument consists of 16 items, administered through the request for the patient to simulate four daily activities. Each activity is evaluated on the basis of four parameters of praxis function: independence, initiation, execution, and control. The four activities include personal hygiene (washing the face and upper body), dressing (putting on a shirt), feeding (preparing a sandwich), and a fourth activity chosen by the evaluator (brushing teeth). Each parameter of praxis function is scored from 0 to 3 points, with 0 indicating that the person has an adequate praxis ability and no requirement for assistance during the activity. The total score ranges from 0 to 48 points, with higher scores indicating lower levels of praxis performance. The ADL Observations scale exhibits adequate validity and strong internal consistency, with a Cronbach’s α of .94 (van Heugten et al., 2000). For the study sample, the internal consistency was also high, with Cronbach’s α of .94.
Statistical Methods
The analyses of this study were performed using IBM SPSS Statistics (Version 28.0). We summarized sociodemographic data, lifestyle behaviors, and clinical variables using the following descriptive statistics: means, standard deviations, frequencies, and percentages. The TULIA Apraxia test and the ADL Observations scale responses were summarized using ranges, minimums, maximums, and percentiles. To evaluate whether ULA was associated with role participation, we conducted analyses using six stepwise linear regression models. Each model corresponded to a different dependent variable, which covers each the six role participation indices. The main independent variables were the seven ULA measures (nonsymbolic imitation, intransitive imitation, transitive imitation, nonsymbolic pantomime, intransitive pantomime, transitive pantomime, and the score from the ADL Observations scale). Additionally, sociodemographic, lifestyle, and clinical variables were also considered in the analysis. In this line, the regression models were structured in blocks as follows: Block 1 included the sociodemographic variables gender, age, marital status, and educational level. The reference categories were male gender, being married, and having a university education. Block 2 involved the following self-reported lifestyle behaviors: number of cigarettes smoked per day, number of alcohol units consumed per day, number of cups of coffee or tea consumed per day, hours of sleep, and minutes per day of physical activity. Block 3 integrated the following clinical characteristics: stroke type, affected hemisphere, and months since stroke. The reference categories in this block were ischemic stroke and the right hemisphere. Block 4 combined significant variables from the previous blocks along with ULA outcomes. A 95% confidence interval was estimated for the unstandardized coefficient (B), and significance was determined with p < .05. We assessed the normality of the variable distributions before the regression analysis. Also, we analyzed the presence of multicollinearity using the variance inflation factor.
Results
Participants
A total of 332 participants were approached in this study. From this potential sample, 153 patients with stroke were included in the study. Figure 1 depicts the flow diagram selection.
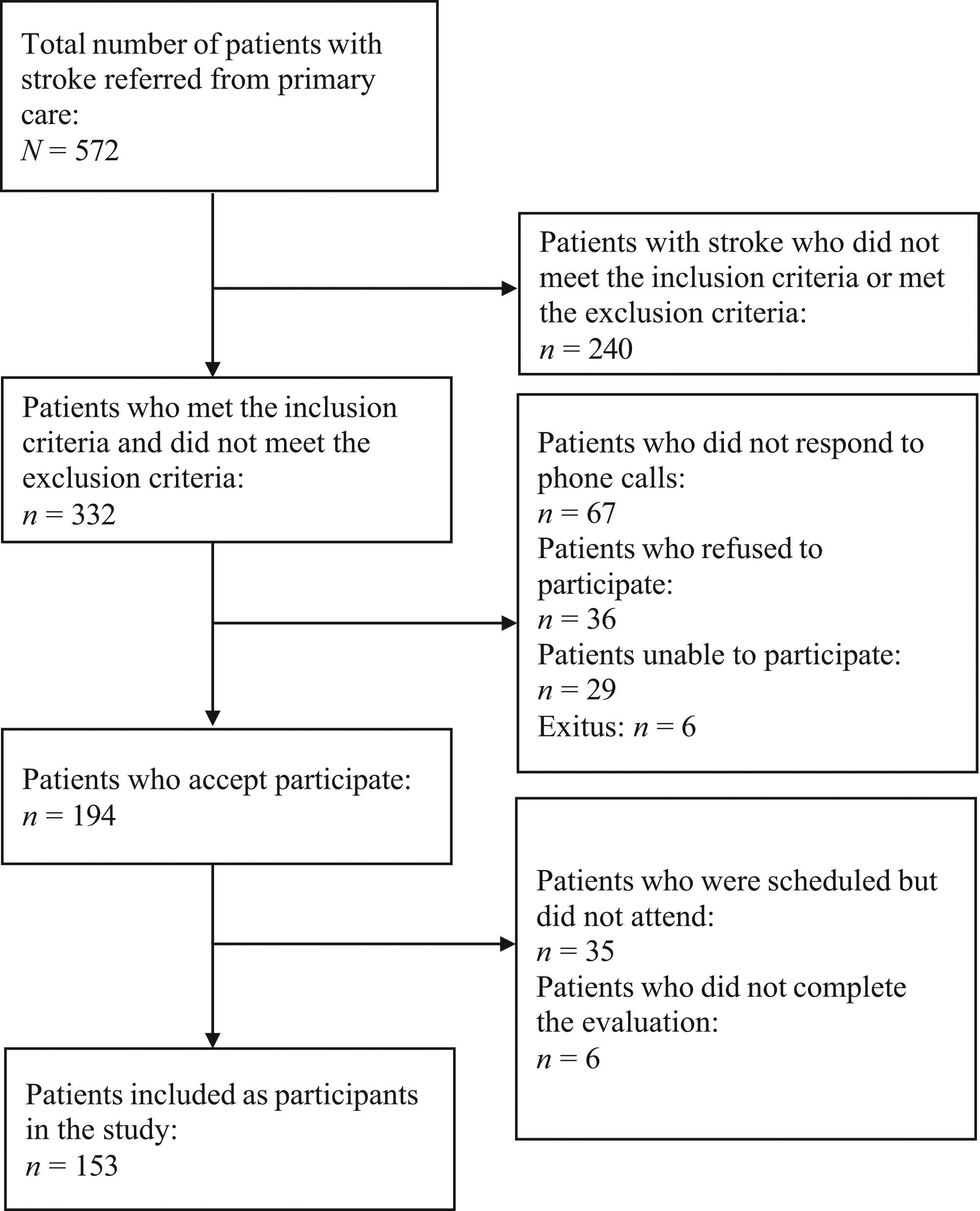
Flowchart of the study population.
Descriptive Data
Of the entire sample, 70% were men, with an average age of 63 yr. Only 16% had undergone occupational therapy rehabilitation. Hemiplegia was present in 12 participants, and although it was not an exclusion criterion, no participant exhibited difficulties with walking abilities. Table 2 shows the baseline characteristics of the participants. The descriptive statistics presented in Table 3 depict the scores of role participation and ULA among the sample.
Sociodemographic, Lifestyle, and Clinical Characteristics of the Sample
Note. OT = occupational therapy.
Descriptive Statistics for Role Participation and ULA
Note. ADL = activities of daily living; ULA = upper limb apraxia.
Relationship Between ULA and Role Participation
The multiple linear regression analyses revealed significant associations between ULA and role participation in patients with stroke, as shown in Table 4. Age (β = −0.170), university education (β = 0.228), and transitive pantomime (β = 0.284) were related to current role participation, predicting 20.5% of its total variance (R 2 = .205), F(3, 152) = 12.795, p < .001. Smoking habit (β = −0.234), hemorrhagic stroke (β = −0.236), nonsymbolic imitation (β = −0.392), and transitive imitation (β = 0.308) predicted 15.8% of the variance of the changes in role participation after stroke (R 2 = .158), F(4, 152) = 6.957, p < .001. Age (β = −0.317), hours of sleep (β = −0.197), and intransitive pantomime (β = 0.174) were associated with expectations for future role participation, explaining 17.8% of its variance (R 2 = .178), F(3, 152) = 10.776, p < .001). Age (β = 0.262), smoking habit (β = −0.165), and time since stroke onset (β = 0.199) predicted 14.4% of the variance of the expectations for future role participation regarding the past (R 2 = .144), F(3, 152) = 8.356, p < .001. Furthermore, coffee habit (β = −0.216), both hemispheres affected (β = 0.181), and both nonsymbolic imitation (β = −0.317) and intransitive pantomime (β = 0.395) were related to the degree of value assigned to the total number of roles, accounting for 16.2% of the variance (R 2 = .162), F(4, 152) = 7.170, p < .01).
Multiple Regression Models for Role Participation and ULA
Note. Dashes indicate nonsignificant findings (p > .05). B = regression coefficient; CI = confidence interval; R 2 = coefficient of determination.
Discussion
This study aimed to explore whether ULA is related to role participation among patients with mild to moderate stroke, and the findings revealed significant associations between these health and occupational constructs. Specifically, in terms of the current level of role participation and future expectations for participation, these were associated with difficulties in performing pantomimes. On one hand, the current level of role participation can be explained by the communicative nature of pantomimes (Goldenberg, 2017), because these gestures are intended to communicate information concerning object use or meaningful actions (Finkel et al., 2018). Communicative tasks require the ability to execute precise movements for effective expression. Therefore, pantomimes may play a key role in promoting social interactions (Osiurak et al., 2023). On the other hand, concerning future expectations for role participation, increased expectations for participation were linked to better abilities to perform pantomimes. This result may suggest that the ability to execute precise pantomimes implies a mastery of complex cognitive functions involving understanding, representing, and communicating actions (Goldenberg, 2017). These abilities are closely tied to functional independence (Unsal-Delialioglu et al., 2008) and life satisfaction after a stroke (Hartman-Maeir et al., 2007). Therefore, increased life satisfaction could improve confidence to engage in roles and assume responsibilities gradually.
In terms of poststroke changes in role participation, lower participation was associated with worse nonsymbolic imitation abilities but better transitive imitation abilities. This finding could be explained by the relationship between imitation abilities and perceived self-efficacy. In a previous study, higher levels of nonsymbolic imitation were correlated with increased self-efficacy levels (Sánchez-Bermejo et al., 2023), which is directly linked to poststroke participation (Chau et al., 2021). Conversely, the inverse relationship between poststroke changes in role participation and transitive imitation does not align with what is typically expected in the clinical context. A plausible explanation could be that patients who perform worse in transitive gestures may be more inclined to focus on roles that involve indoor activities because of limitations in engaging in activities outside the home, which could lead to an overall increase in the number of roles in which the sample participated after the stroke (Ashaie & Castro, 2022). Additionally, these patients might have reduced their engagement in work-related activities, resulting in a restructuring of their time and a shift toward different roles (Norlander et al., 2022).
Regarding the value assigned to roles, higher levels of importance assigned to them were associated with better intransitive pantomime abilities but poorer nonsymbolic imitation abilities. In terms of pantomime, this result could be explained by various reasons, such as levels of motivation, cognitive abilities, emotional well-being, and treatment adherence. First, people who assign greater importance to their roles may be more motivated (Gingrich et al., 2023). This heightened commitment could translate into improved performance in activities involving pantomimes. Second, the significance attached to roles may be linked to cognitive functioning, which enables them to effectively execute tasks involving the representation of actions. Third, people who feel satisfied and fulfilled in their roles may experience a better overall mood (de Graaf et al., 2022), which could contribute to enhanced performance in pantomimes (Lanctôt et al., 2020). Fourth, people who assign high importance to their roles may be more inclined to invest time and effort in activities aimed at improving their cognitive functions, including praxis (Aguilar-Ferrándiz et al., 2021). On the other hand, the association between higher levels of importance assigned to roles and lower performance in nonsymbolic imitation could be seen as an adaptive strategy. After a stroke, patients might shift their vital priorities or reevaluate their activity participation (Baumard et al., 2020). Faced with cognitive limitations, they may refocus their attention and assign greater value to roles they perceive as more meaningful (Lee et al., 2023). Therefore, despite experiencing challenges in nonsymbolic imitation, these patients may prioritize roles that provide a greater sense of personal identity (Park & Lee, 2022).
The findings of this study show that the alteration of the praxis function explains, in some cases, up to 20.5% of the role participation construct. Role participation is a complex and multidimensional concept influenced by multiple factors that can contribute to low levels of participation in patients with stroke that are not yet well understood. In this line, different models of understanding role participation, along with existing scientific evidence, suggest that various factors are also responsible for the unexplained percentage of variance in the model in this study. These factors include motivation (Fujita et al., 2024), emotional status (Lee et al., 2023), and community access or environmental opportunity, among others (Gingrich et al., 2023; Williams & Murray, 2013). Therefore, the present findings provide evidence of another cognitive function that contributes to understanding why a stroke patient experiences a negative impact on role participation after the event.
Limitations
This study presents some potential limitations. First, the sample was limited to patients from a single region, which may reduce the generalizability of the results. Second, this study did not stratify participants by lesion size, which may have provided valuable insights into how the extent of brain damage influences the relationship between upper limb apraxia and role participation. Third, the NIHSS is primarily used to assess stroke severity in acute patients. However, in this study, we used the instrument to exclude patients with severe stroke from a sample of patients with chronic stroke. It is important to consider this decision when interpreting the characteristics of the recruited sample, because the NIHSS may not fully capture the long-term sequelae and the functional variations present in patients with chronic stroke.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy education: ▪ Our findings provide essential information about the ability of patients to participate in vital roles after a stroke. ▪ The measures used in this study help identify patients with stroke at risk for losing autonomy in role participation. ▪ Our findings emphasize the importance of assessing ULA in patients with stroke. ▪ Our findings guide occupational therapists to plan patient-centered interventions.
Conclusion
The study findings indicate that ULA is related to role participation levels after a stroke. Transitive pantomime appeared to be associated with current role participation. Both nonsymbolic imitation and transitive imitation are linked to changes in role participation after a stroke. Intransitive pantomime showed a relationship with expectations for future role participation. Moreover, nonsymbolic imitation and intransitive pantomime were related to the value or level of importance assigned to roles. Understanding these relationships may be relevant to enhancing comprehension of how apraxia may affect role participation in these patients.
Footnotes
Acknowledgments
We sincerely acknowledge the participants, who generously dedicated their time and effort to participate in this research study. This study is part of Laura Sánchez-Bermejo’s doctoral thesis.