
Abstract
This study assessed the effectiveness of using an escape room as a teaching tool in a clinical skills class for occupational therapy and occupational therapy assistant students.
Effective intraprofessional collaboration among occupational therapy (OT) practitioners is essential for delivering high-quality patient care. Despite the emphasis on collaborative skills in educational standards, there remains a significant gap in how these skills are taught and reinforced within OT curricula. This study addresses one innovative educational approach that can enhance intraprofessional teamwork, critical thinking, and active learning among OT and occupational therapy assistant (OTA) students.
Incorporating Intraprofessional Collaboration in Curricula
The Accreditation Council for Occupational Therapy Education (ACOTE®; 2018) has included specific standards for addressing intraprofessional collaboration in occupational therapy (OT) education, emphasizing its importance and necessity. Although intraprofessional collaboration has been emphasized with the ACOTE standards over the past decades, a recent study surveyed 465 OT and OT assistant (OTA) practitioners to investigate where and how they developed competencies for intraprofessional collaboration. The findings revealed that both OT and OTA practitioners overwhelmingly identified work experience and field work as the main learning contexts for the development of intraprofessional competencies (Pitonyak, Corsilles-Sy, et al., 2020). There is a remaining gap in how academic programs can incorporate intraprofessional learning opportunities in curricula.
Multiple studies have indicated that integrating opportunities for intraprofessional teamwork within didactic courses would enhance students’ collaboration abilities (Dennehy, 2022; Pitonyak, Corsilles-Sy, et al., 2020). Fan et al. (2021) demonstrated that students’ perceived importance of intraprofessional collaboration and their ability to engage in collaborative learning improved after participating in a structured two-phase learning module. Dennehy (2017) conducted a longitudinal study involving OT and OTA students, highlighting the preference for face-to-face interactions over distance methods in fostering collaboration skills. Building on Dennehy’s (2017) findings regarding the preference for face-to-face interactions, recent studies have also explored innovative approaches such as educational escape rooms to enhance intraprofessional learning and teamwork collaboration further. Two pilot studies used educational escape rooms to enhance intraprofessional learning between OT and OTA students. Carpenter et al. (2023) showed that students perceived that the escape room activity promoted their understanding of role delineation, facilitated teamwork, and supported effective intraprofessional communication. Fan (2023) examined OT and OTA students’ retained knowledge of course contents and intraprofessional collaboration skills with online and in-person escape rooms. Her results showed that both escape room formats significantly improved students’ intraprofessional teamwork and collaboration and facilitated positive professional identity. In addition, both OT and OTA students’ knowledge retention significantly improved, with a moderate effect size, after participating in the educational escape rooms (Fan, 2023). These findings underscore the need for academic programs to create structured, interactive opportunities that promote intraprofessional collaboration within their curricula.
Gamification in Higher Education
Gamification is defined as the use of game design elements in nongame contexts to enhance users’ engagement and motivation (Deterding et al., 2011). Given the successful implementation of escape rooms in recent studies (Carpenter et al., 2023; Fan, 2023) to enhance intraprofessional learning among OT and OTA students, in the present study, we sought to build on this evidence by investigating the specific effects of the educational escape rooms on knowledge acquisition, readiness for intraprofessional collaboration, and perceived active learning and critical thinking skills.
Gamification in higher education has been shown to foster motivation and improve academic performance, with empirical evidence supporting these claims (Hamari et al., 2014; Ozturk & Korkmaz, 2020; Yildirim, 2017). One review study showed that most educational escape rooms were used in higher education, especially in science, technology, engineering, and mathematics (STEM) and health care professions (Taraldsen et al., 2022). Gamification in education has been a developing instructional approach to enhance students’ motivation and engagement (Ratinho & Martins, 2023). It incorporates the learning objectives and interweaves difficult learning materials into game components. A prior study showed that game-based competition significantly influences students’ learning performance (Xu et al., 2022). Additionally, when incorporating games, students had higher motivation to spend longer time in the learning management systems, such as Canvas and Blackboard, especially for OT and nursing students (Sáiz-Manzanares et al., 2021).
Although gamification has grown in popularity in higher education (Khaldi et al., 2023; Taraldsen et al., 2022), the evidence about how to apply the gamification components (e.g., elements such as point scoring, leaderboards, badges, and interactive challenges) in concert with the specifics of the education context is still limited (Dichev & Dicheva, 2017). One review study highlighted the need to rigorously test gamification approaches and confirm their educational benefits (Dichev & Dicheva, 2017). Additional studies are needed to share gamification designs to increase transparency and methods for data collection and analysis (Taraldsen et al., 2022). Integrating gamification into curricula provides greater student engagement and fosters critical thinking and active learning methodologies in OT education (Dugnol-Menéndez et al., 2021).
Critical Thinking and Active Learning
Critical thinking is the thoughtful and rational process that centers on determining personal beliefs or actions (Ennis, 2018). A systematic review examined 28 articles published over the past 30 yr regarding how OT education teaches critical thinking (Pitonyak, Nielsen, et al., 2020). The authors found that most OT educational research addressed critical thinking in instructional methods, such as guided questioning, simulations, and problem-based approaches; however, most studies used qualitative inquiry to evaluate students’ feedback, which lacked adequate quantifiable outcome measurements. Additionally, the same study emphasized that OT is a unique profession that values participation and doing rather than solely thinking. Therefore, active learning in instructional methods should be used to foster critical thinking (Pitonyak, Nielsen, et al., 2020).
Active learning involves instructional activities that engage students in hands-on learning while prompting them to reflect and think about their actions (Michael, 2006). Participating in educational escape rooms can facilitate active learning and critical thinking skills (Adams et al., 2018). A recent study interviewed special education master’s-level students who completed an educational escape room (Manzano-León et al., 2021). The students indicated that escape rooms increased their problem-solving and critical thinking skills and helped them learn to work under pressure. Furthermore, they indicated that learning acquired in the escape room was more significant than in traditional education (Manzano-León et al., 2021). Another study found that implementing escape rooms after instruction is more effective in promoting learning than playing escape rooms before instruction (Buchner et al., 2022).
In this study, intraprofessional collaboration was identified as a critical area for development in alignment with ACOTE standards. The escape room was selected as an innovative method to enhance teamwork and communication between OT and OTA students because of its ability to engage students in a dynamic, hands-on learning environment that promotes collaborative problem-solving under time constraints. Therefore, in the present study, we aimed to examine the effectiveness of using an educational escape room in a clinical skills class for OT and OTA students. The escape room was designed to reinforce key concepts and skills covered in the course while promoting active learning and intraprofessional collaboration. The research questions guiding this study were as follows: ▪ Does participation in an educational escape room enhance OT and OTA students’ knowledge levels in clinical skills? ▪ Does participation in an educational escape room affect students’ perceived importance and ability for intraprofessional collaboration? ▪ Does participation in an educational escape room influence students’ perceived active learning and critical thinking skills?
Method
Study Design
This study used a one-group, pre-experimental study design with convenience samples. The enrolled participants were assessed 2 wk before and immediately after the educational escape room experience.
Participants
The escape room was designed and embedded within targeted clinical skills classes OCTH540: Applied Clinical Skills for the 1st-yr OT students and OCTH117: Patient Care Skills in Occupational Therapy for the 1st-yr OTA students at AdventHealth University. All students enrolled in these courses were invited to participate, and no exclusion criteria were used. Data were collected across three cohorts from March 2022 to March 2024.
Clinical Skills Course
The OT and OTA students took the clinical skills course together with the same instructor (although with different course numbers), and the same teaching approaches were used for both groups. Before each class, students were required to watch an online PowerPoint presentation, complete assigned readings, and take a quiz. In class, they worked in intraprofessional groups of two to three OT students and one to two OTA students to practice and demonstrate competency in various skills, which were evaluated by OT and OTA faculty. Throughout the trimester, students practiced essential clinical skills such as infection control, wheelchair management, assistive device use, vitals assessment, body mechanics, bed mobility, transfer skills, and draping and positioning for different patient scenarios. This structured preparation, embedded in the course content over the trimester, ensured that students had a solid foundation and proficiency in the necessary clinical skills before participating in the escape room experience while also promoting psychological safety.
Escape Room Development
In this study, we created an escape room as an innovative review session to enhance students’ understanding of the course materials. The project’s lead faculty (Chia-Wei Fan) and the course instructor (Vicki Case) identified the key topics in the targeted courses based on a combination of factors. Over the years, we observed that certain topics consistently posed challenges for students. This observation was supported by data from prior competency checks, exams, and student feedback. To specifically address these areas, we designed the escape room with puzzles and scenarios focused on these challenging topics. Figure 1 illustrates how these core topics were integrated into the structure of the escape room, ensuring alignment between the identified learning needs and the educational intervention.
Puzzle flow and map of the escape room.
Then, on the basis of the chosen topics, we designed original escape room puzzles to help students review these course contents. The best practice simulation standards for simulation design (INACSL Standards Committee, 2021c) were adopted to ensure that the puzzles were well structured to meet the learning objectives and provide realistic scenarios. Both the OT and OTA clinical skills courses share the following learning objectives: ▪ provide recommendations and training in techniques that enhance functional mobility, including physical transfers, wheelchair management, and mobility devices ▪ demonstrate understanding of basic clinical skills and their application to clients with diverse needs and contexts ▪ grade and adapt the environment, tools, materials, and interventions to meet clients’ evolving needs within their sociocultural context ▪ use critical reasoning to justify the selection of compensatory strategies when life tasks cannot be performed ▪ exercise sound judgment and adhere to safety regulations throughout the OT process.
The puzzles created for the escape room were directly aligned with these course objectives.
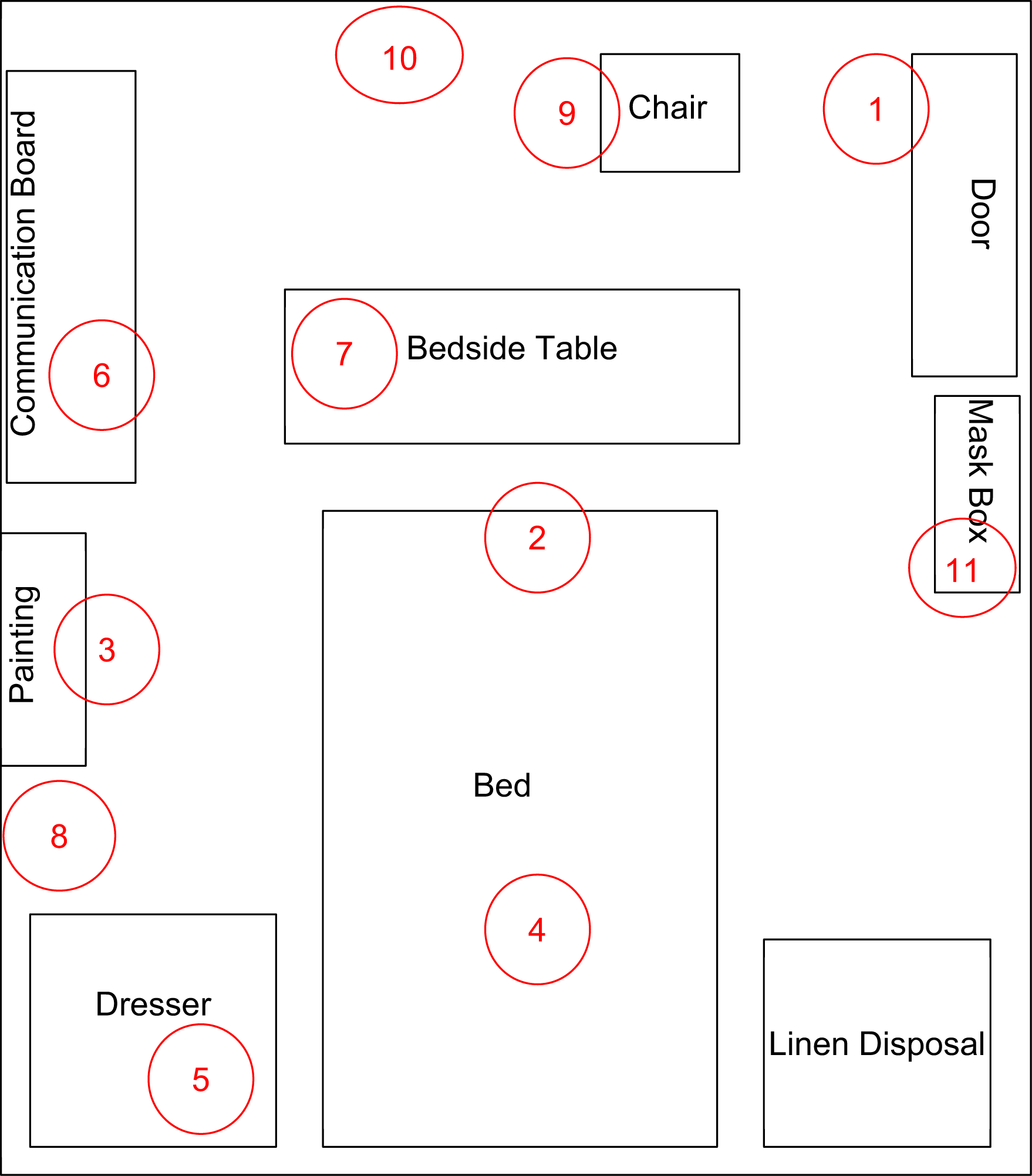
The escape room experience occurred in the realistic hospital setting simulation laboratories on the school campus (Figure 2). Each puzzle was strategically placed to encourage students to navigate the simulation room and engage with a realistic clinical environment. The social setup promoted collaboration between OT and OTA students, with mixed groups designed to develop teamwork and communication skills, key aspects of intraprofessional collaboration. The activity was timed, giving each group 1 hour to complete all puzzles, simulating the urgency and pressure of real clinical settings and encouraging efficient decision making under stress.

Simulation room.
Ten puzzles were in the escape room, each tied to a scenario presented to students on entering the room. The initial scenario read: You all suddenly wake up in a hospital room with no memory of how you got there or your names. The doors are locked, and you can’t find the key. Where can you go to find more information about yourselves, the patients?
Students would then discover a puzzle attached to a patient chart with their names shown on a donor list. A sticky note on the chart instructed, “Protect these patients from HIPAA violations! Cross through any sensitive information, and maybe it’ll lead somewhere.” Solving this puzzle allowed students to unlock a box at the end of the bed, revealing the next clue.
All groups received the same scenario and were required to solve the same 10 puzzles. Students were not expected to solve any puzzles independently; instead, they were instructed to work as a team to solve all 10 puzzles and escape within 1 hr. This collaborative approach was designed to promote intraprofessional collaboration by requiring students to rely on each other’s skills and knowledge, fostering teamwork and communication. Additionally, they were instructed to solve the puzzles in order, as each puzzle would give them a new clue leading to the next puzzle.
Procedure
The best practice simulation standards of prebriefing (INACSL Standards Committee, 2021b) were adopted in this study. The prebriefing session provided clear expectations and objectives to better prepare students for the escape room activity. At the beginning of the trimester, the course instructor introduced the escape room concepts and how they would be used in the courses. The instructor emphasized that the escape room was an innovative way to review important course materials, and the activity was built into the class time. Therefore, participating in the escape room experience was mandatory for all students, but completing the pre- and postassessments was voluntary.
To ensure the psychological safety of the students, we implemented several strategies. Two weeks before the escape room activity, a comprehensive prebriefing session was conducted. This session included an overview of the escape room activity to prepare students mentally and reduce anxiety. In addition, this session included both an overview of the study and a review of the learning objectives for the escape room simulation (INACSL Standards Committee, 2021b). We emphasized the collaborative nature of the escape room activity and reassured students that the focus was on learning the course materials and teamwork rather than individual performance.
Additionally, students were informed that their performance in the escape room would not be graded or linked to their class grades. During the prebriefing session, we explicitly encouraged a supportive and nonjudgmental environment in the escape room. Steps to ensure psychological safety were highlighted, such as allowing students to call out for hints if they felt stuck between the puzzles. Each group was allowed up to three hints during the activity to ensure the activity remained challenging yet supportive. To maintain academic integrity, we ensured that the research teams securely handled all puzzles, solutions, and other relevant materials. Students were instructed not to look up answers online and to work within their groups to find solutions.
At the end of the prebriefing session, the students were given time to ask questions, which were answered before they consented to participate. If the students chose to participate in the study, they signed and dated the consent form and returned it to the research team. They could also choose not to participate in any of the assessment parts with no penalty or associated consequences. Those students who agreed to participate then completed three pretest assessments: Readiness for Interprofessional Learning Scale (RIPLS), Self-Assessment Scale for Active Learning and Critical Thinking (SSACT), and a researcher-developed knowledge assessment (KA). Please see the “Measurements” section for the assessment details. Then, all the students were randomly assigned into groups of about four to five members, consisting of one to two OTA students and two to three OT students.
Two weeks later, the escape room experience occurred in the realistic hospital simulation laboratories. Before the escape room experience, the researchers quickly reviewed the study and learning objectives, the importance of teamwork, and the guidelines for active participation. Any last-minute questions were answered before the students were sent into the escape room. Then, the students entered the escape room with the assigned group of OT and OTA students. They were instructed to begin with the first puzzle and continue in order until all 10 puzzles were solved, and they found the key to escape in 1 hr. The best practice simulation standards for facilitation (INACSL Standards Committee, 2021a) were used during the escape room experience to support students’ learning, ensuring that instructors provided guidance while allowing students to take ownership of their problem-solving process.
Immediately after completing the escape room, the same assessments (i.e., RIPLS, SSACT, and KA) were distributed and completed by the enrolled participants. The pre- and postassessments were printed and completed in paper format. Each participant was labeled with a four-digit number to ensure anonymous responses. Debriefing was conducted within 1 wk of the escape room experience and lasted approximately 30 min. The process adhered to the INACSL Standards of Best Practice for Debriefing, using the Promoting Excellence and Reflective Learning in Simulation framework (Eppich & Cheng, 2015). This evidence-based model was selected to facilitate structured reflective learning, allowing students to analyze their experiences, consolidate learning outcomes, and identify areas for improvement (Morse et al., 2020). This project was approved by the AdventHealth Institutional Review Board (number 2132107-1).
Measurements
Self-assessments promote participants’ reflective practice (Siles-González & Solano-Ruiz, 2016). Additionally, students’ self-efficacy, “beliefs about their capability to perform a task” (Pintrich et al., 1993, p. 176), explained the largest amount of variance in their academic achievement, even after individual intelligence and prior grades were controlled (Steinmayr et al., 2019). Therefore, in this study, we adopted two self-assessment tools to evaluate students’ active learning, critical thinking, and readiness for intraprofessional collaboration. Additionally, one objective measurement was created to evaluate students’ knowledge levels.
RIPLS
We used the RIPLS to assess the participants’ self-perception for their OT and OTA intraprofessional learning readiness. This assessment contains 19 questions with four subscales: Teamwork and Collaboration (nine items), Negative Professional Identity (three items), Positive Professional Identity (four items), and Roles and Responsibility (three items; McFadyen et al., 2005). It is rated with a 5-point Likert scale that ranges from 1 (strongly disagree) to 5 (strongly agree). Items in the Negative Professional Identity and Roles and Responsibilities subscales were reverse-coded for data analysis (McFadyen et al., 2006). Previous studies suggested viewing the overall scale as a whole instead of looking at the subscale level (Mahler et al., 2015). Therefore, participants’ scores of the four domains were combined for a total score. Higher scores indicate higher levels of readiness for intraprofessional collaboration. Kerry et al. (2018) used the RIPLS on medical and nursing students, and the results supported that the RIPLS is sensitive to changes in a prelicensed health care student population.
SSACT
The SSACT measured students’ self-perception of their active learning and critical thinking skills with problem-based learning (Khoiriyah et al., 2015). The SSACT contains 14 questions in two subscales: Active Learning (seven items) and Critical Thinking (seven items). All items are rated with a 7-point Likert scale ranging from 1 (not very true of me), to 7 (very true of me). Higher scores indicate higher levels of active learning and critical thinking.
KA
The research team developed the KA. It was designed to test the participants’ knowledge level of the topics covered in the clinical skills class. Two OT faculty who were not involved in item development conducted content validity. The KA was shared with OT faculty by e-mail, and they had 2 wk to review and give feedback. Then, a face-to-face meeting was conducted to discuss each question until reaching a consensus. This assessment consists of 20 multiple-choice questions, each with only one correct answer.
The following is a sample KA question: When transferring a patient who has had a stroke from a wheelchair to a commode, how should you position the wheelchair? A. 45-degree angle with armrest removed B. 45-degree angle with leg rests forward C. 180-degree angle with armrest removed D. 90-degree angle with leg rests forward.
The correct percentage of the total 20 questions was calculated to represent students’ knowledge level; the higher the correct percentage, the greater the understanding of the topics.
Data Analysis
The data were entered from the paper assessments into an Excel spreadsheet, and 20% of the data were randomly selected for double-checking to ensure accuracy. To ensure that natural group characteristics did not influence differences in the assessments, we used the χ2 and independent-samples t tests to examine the demographic characteristics and baseline assessments between OT and OTA students; equal variances were not assumed. The χ2 analysis was used to check the nominal data, and the results showed that gender did not have significant differences between OT and OTA students, χ2(1) = 0.82, p = .06. The independent-samples t test was used to examine differences between participants’ age, t(54.4) = 1.48, p = .14; SSACT scores, t(58.1–78.2) = 1.85 to 2.51, ps = .02 to .19; and RIPLS scores, t(62.2) = 0.93, p = .16, at baseline. Most results were comparable, except that OT students had higher critical thinking compared with OTA students at baseline (Table 1). Additionally, significant differences were found on the KA between the two groups. Given the known differences, we conducted separate pre- and postassessment comparisons for the OT and OTA student groups.
Participant Demographics and Baseline (Pretest) Comparisons Between OT and OTA Students
Note. N = 114. KA = Knowledge Assessment; OT = occupational therapy; OTA = occupational therapy assistant; RIPLS = Readiness for Interprofessional Learning Scale; SSACT = Self-Assessment Scale on Active Learning and Critical Thinking.
Chi-square value is presented for gender; all other values in this column are t values.
*p < .05. **p < .001.
Given the ordinal ratings on the RIPLS and SSCAT, we used the Wilcoxon signed-rank test to examine changes; additionally, we analyzed the KA using the parametric paired-sample t test (Simpson, 2015). Last, Cohen’s (1988) effect size (d) was calculated using the following criteria: .20 = small, .50 = moderate, and .80 = large.
Results
Of the 81 OT and 48 OTA enrolled students in the corresponding courses from 2022 to 2024, 76 OT and 38 OTA students agreed to participate, and they completed the pre- and postassessments (response rate = 93.8% for OT students and 79.2% for OTA students). Ten (8.8%) participants were male, and 104 (91.2%) were female. The age range of the participants was 18 to 39 yr, with an average age of 23.99 yr (SD = 3.82). Individual group information can be found in Table 1. On the basis of the SSACT results, the escape room experience significantly improved students’ active learning for both OT students, Z = −4.65, p < .001, and OTA students, Z = −6.00, p < .001. Critical thinking skills also significantly improved for OT students, Z = −3.42, p < .001, and OTA students, Z = −4.67, p < .001. According to the results of the RIPLS, both OT students, Z = −3.81, p < .001, and OTA students, Z = −4.29, p < .001, had increased perceived readiness for intraprofessional learning. Last, after the educational escape room experience, knowledge levels were also significantly improved for OT students, t(75) = −5.16, p < .001, and OTA students, t(37) = −4.50, p < .001 (Table 2). KA changes showed a moderate effect size for OT (d = .59) and OTA students (d = .64).
Changes in Three Targeted Outcomes at Pretest and Posttest
Note. KA = Knowledge Assessment, used to evaluate participants’ knowledge levels; RIPLS = Readiness for Interprofessional Learning Scale, used to evaluate participants’ intraprofessional collaboration readiness; OT = occupational therapy; OTA = occupational therapy assistant; SSACT = Self-Assessment Scale on Active Learning and Critical Thinking, used to evaluate participants’ active learning and critical thinking skills.
t values are presented for KA; all other values are Z values.
**p < .001.
Discussion
Despite the emphasis on having quantified outcomes for evidence-based practice in OT (Lin et al., 2010), a notable limitation of the educational research is its adoption of mostly qualitative methods for assessing student feedback (Pitonyak, Nielsen, et al., 2020). Also, a discrepancy exists between the actual acquisition of content knowledge in educational escape rooms (Veldkamp et al., 2020). The present study provided an example of how escape rooms can be used in didactic courses to promote OT–OTA collaboration and facilitate active learning and critical thinking skills. The outcomes of this research supported the conclusions drawn in earlier studies that educational escape rooms are beneficial in OT education (Carpenter et al., 2023; Dugnol-Menéndez et al., 2021; Fan, 2023). Specifically, in this study, participants increased perceived active learning, critical thinking, and intraprofessional collaboration. Additionally, to the best of our knowledge, this is the first study that examined and quantified participants’ knowledge changes after participating in an educational escape room in OT education.
Active learning is a broad educational approach that emphasizes student engagement in the learning process (Michael, 2006). Experiential learning, as a specific type of active learning, focuses on learning through direct experience. Grounded in Kolb’s (1984) experiential learning cycle, it involves four stages: concrete experience, reflective observation, abstract conceptualization, and active experimentation. Escape rooms, as an educational tool, exemplify experiential learning by providing students with immersive, hands-on experiences where they apply knowledge in real time, solve puzzles, and collaborate in a simulated environment. Although all experiential learning is a form of active learning, not all active learning includes the hands-on, reflective process characteristic of experiential learning. Therefore, educational escape rooms effectively foster both active engagement and practical, reflective learning through real-time problem solving and collaboration.
In the present study, the design and execution of the escape room puzzles were purposefully structured to complement traditional instructional methods. We found that both the OT and OTA students had significantly improved knowledge with a moderate effect size, which aligned with the results of using educational escape rooms for other professionals. For example, Lopez-Pernas et al. (2019) used a pre-experimental design to evaluate the effectiveness of the educational escape room in 84 students with the telecommunications engineering major. The results showed that students improved their knowledge and grades with a medium effect size (d = 0.75). Another study used a randomized controlled trial to conduct educational escape rooms to improve knowledge and collaboration among students of health professions (nursing, pharmacy, and physical therapy). The results showed that engaging in escape rooms significantly enhanced students’ immediate recall of knowledge, and this retention of knowledge persisted during subsequent simulations (Fusco et al., 2022).
Integrating escape rooms into the curriculum not only incorporates learning objectives of the course contents to improve students’ knowledge levels but also provides gamification components to keep students engaged and motivated. By creating a simulated yet realistic environment within the educational escape rooms, students were challenged to use a hands-on approach to apply their knowledge and critical thinking skills. This active participation led to a deeper understanding of course materials. Michael (2006) emphasized experiential learning in promoting deeper understanding and concept application when considering active learning strategies in education. This finding aligned with the principles fundamental to educational escape rooms that help participants to engage actively with puzzles and clues relevant to course contents and apply their knowledge in real-time scenarios.
Additionally, in the present study, we assessed students’ perceived active learning and critical thinking skills, encouraging them to reflect on their learning processes. This self-reflection helped students become more aware of their learning strategies and active education roles (Ambrose et al., 2010). Perceived active learning also reflected the students' engagement and involvement in the learning process. If students perceived the experience as actively engaging, it indicated that the learning activity successfully captured their interests and participation. Ultimately, this information allows educators to identify strengths and areas for improvement in the instructional design (Harackiewicz et al., 2016). Therefore, measuring perceived active learning provides an additional layer of validation for the effectiveness of the active learning pedagogy.
In addition, the nature of teamwork and collaboration in the escape rooms promoted the development of intraprofessional collaboration. Multiple studies have confirmed teamwork and collaboration improved after the educational escape room experience (Carpenter et al., 2023; Fan, 2023; Fusco et al., 2022). The escape room was specifically designed to foster collaboration by requiring students to work together to solve complex, multistep puzzles. The immersive environment encouraged participants to rely on each other, share ideas, and build on each other's strengths. The puzzles were structured so that no single student could complete them alone within the 1-hr timeframe; therefore, it is necessary to rely on teamwork and collaboration.
Additionally, the competitive and engaging nature of the escape room motivated students to participate and collaborate actively to achieve a common goal. For the clinical skills courses in this study, both OT and OTA students had similar roles and responsibilities in implementing foundational clinical skills. As a result, during the escape room activities, OT and OTA students were not explicitly tasked with challenges that required them to use their distinct skills and roles. Instead, the focus was on collaborative problem-solving, effective communication, and teamwork. During the debriefing sessions, some students shared that OT students tended to lead problem-solving efforts related to clinical reasoning, whereas OTA students contributed hands-on skills and task-specific knowledge, which created a balanced and collaborative team effort.
However, escape rooms are heavily team-based games; a prior study also indicated that instructors must ensure that every team member actively contributes to the teamwork (Wiemker et al., 2015). The course instructors should closely monitor and facilitate effective team dynamics and ensure active participation from all team members to optimize the collaborative learning experience in escape rooms. Additionally, although in-person escape rooms increased engagement and facilitated collaboration and hands-on learning, they required more resources than virtual escape rooms (Helbing et al., 2022). A significant drawback of incorporating in-person escape rooms into curricula is the financial investment and faculty commitment to create and set up puzzles that tailor course objectives (Lee et al., 2018). Therefore, some studies suggested using virtual escape rooms, which could reduce expenses and minimize ongoing maintenance. For virtual escape rooms, instructors should choose the user interface carefully, because it can significantly affect the students’ experience and engagement levels (Gerber & Fischetti, 2022). After the initial development of the virtual escape room, it can be used over multiple years (Barrickman et al., 2023).
Limitations
The present study used a convenience sample within a single institution. Therefore, the generalization of the results needs to be cautious. We used the students’ self-assessments as the two major assessments in the study, and they could vary in accuracy (Baxter & Norman, 2011). A previous study showed that lower performers tend to overestimate their ability, whereas higher performers underestimate it (Hartwig & Dunlosky, 2014). Therefore, self-perceived active learning, critical thinking, and intraprofessional collaboration readiness should be interpreted carefully. In addition, perceptions of the skill levels cannot directly represent the actual performance level (Ehrlinger et al., 2008). Therefore, how the students’ self-perceptions would transfer to actual behaviors should be further examined in future studies. In addition, a previous study suggested using a mixed-methods design to capture quantitative and qualitative information (Gómez-Urquiza et al., 2022), which should be incorporated into future studies.
Also, in this study, we used a preexperimental design, which is insufficient for making causal inferences. More rigorous experimental designs, such as randomized controlled trials, are needed to establish causality. Several factors beyond the escape room experience itself may have contributed to the improved outcomes that need to be considered. For example, the OT and OTA students already knew each other from previous coursework; they may have had an existing rapport that facilitated smoother interactions. Also, consistent guidance and support from faculty throughout the trimester likely reinforced the importance of active learning and collaboration. Future studies should include control groups to better isolate the specific effects of the escape room intervention and examine student learning and collaboration.
Furthermore, a significant limitation of this study is the lack of a validated assessment tool specifically designed for intraprofessional collaboration. Although the RIPLS provided valuable insights into collaborative skills, it primarily focuses on interprofessional interactions. For better evaluation of intraprofessional collaboration between OT and OTA students, there is a clear need to develop assessment tools that are tailored to intraprofessional contexts. Future research should focus on creating and validating such tools to enhance the accuracy and relevance of assessments in this area.
In addition, the present study did not consider the learning style of the enrolled participants. Although gamification has been proven to enhance students’ engagement, other studies also commented that students’ learning styles would influence the effectiveness of gamification techniques on learning outcomes (Buckley & Doyle, 2017). Furthermore, a recent systematic review found that novel gamification and extrinsic rewards promoted students’ short-term motivation (Ratinho & Martins, 2023); however, long-term exposure could diminish its effectiveness (Bilbao-Quintana et al., 2021). Therefore, future studies should investigate the long-term effectiveness of educational escape rooms. Last, time restriction during the educational escape rooms appears to be an ambiguous factor in student learning (Veldkamp et al., 2021), which should be further investigated.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ Intentional intraprofessional learning opportunities can be created and incorporated into didactic courses. ▪ The innovative educational escape rooms provide a unique learning experience for OT and OTA students, and it increases students’ motivation and engagement. ▪ The educational escape rooms effectively improved students’ perception of active learning, critical thinking, and intraprofessional collaboration. Course learning objectives can also be incorporated to increase students’ knowledge levels.
Conclusion
Escape rooms are an increasingly popular, innovative teaching modality in health care education. This study lays the groundwork for the OT profession that collaborative and intraprofessional active learning experiences, such as escape rooms, can help build teamwork among OT and OTA students and enhance their knowledge levels.
Footnotes
Acknowledgments
Chia-Wei Fan expresses sincere gratitude to Dr. Jennifer Radloff, OTD, OTR/L, CDRS, for her inspiration and mentorship in initiating and developing active learning strategies. We also extend our appreciation to the following occupational therapy students for their valuable assistance in creating the learning puzzles: Tatiana King, Olivia Kralik, Destiny Hart, Vanessa Sanders, Reghan Massie, Hailey Stufflet, Emily Suarez, and Kyle Longhofer. This research was supported by AdventHealth University Graduate Student Research Grants OT5421, OT9822, and OT13723.