
Abstract
This study evaluated the activities of daily living independence and dependence of people with Parkinson’s disease based on each person’s disease stage.
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by motor symptoms (e.g., bradykinesia, rigidity, resting tremor, postural instability) and nonmotor symptoms (e.g., olfactory loss, sleep dysfunction, autonomic dysfunction, psychiatric disturbance, cognitive impairment; Armstrong & Okun, 2020). Disease progression tends to gradually affect activities of daily living (ADLs; Hoehn & Yahr, 1967; Sperens et al., 2020). Decreased independence in ADLs is associated with decreased quality of life (Muslimović et al., 2008) and increased caregiver distress (Karlstedt et al., 2020). Thus, addressing the improvement and maintenance of independence in ADLs is crucial in supporting patients with PD.
ADLs typically include self-care tasks, such as bathing, dressing, eating, grooming, toileting, and mobility. Levels of dependency in these ADL domains have been associated with a patient’s PD severity (Shulman et al., 2008). This information can help guide occupational therapists in offering the appropriate support levels needed to promote occupational performance. It can also make it possible to identify the appropriate measures needed to delay activity limitations by implementing early interventions and proposing compensation strategies for activities that are difficult at the advanced stages of PD. Additionally, it enables patients and caregivers to predict the progression of difficulties in ADLs and helps them to prepare for the future.
Several studies have established a causal relationship between ADLs and PD severity. However, most previous studies have focused either on only the relationship between disease severity and some ADL items, such as bladder symptoms (Iacovelli et al., 2010) and functional mobility (Mollà-Casanova et al., 2022), or on disease severity and total scores on ADL assessments (Hobson et al., 2001; Skorvanek et al., 2017). To our knowledge, there is only one study of the relationship between disease severity and individual ADL items (Shulman et al., 2008). Shulman et al. (2008) evaluated the disease severity of PD using the Hoehn and Yahr (H-Y) stages and ADL disability with the Older Americans Resources and Services (OARS) Disability subscale (Duke University Center for the Study of Aging and Human Development, 1978). They found that loss of independent function in PD is associated with disease severity, and patients with PD initially reported difficulty with walking, followed by problems with several gait-dependent activities. However, the OARS is a self-report questionnaire. Considering the discrepancy among patients with PD between subjective self-reports and objective performance ratings of ADLs (Shulman et al., 2006), further study using an ADL assessment conducted by a third person can help clarify the disabilities that occur in patients’ lives at each disease stage. Therefore, in this study, we sought to evaluate the ADL functional capacity profiles of patients with PD as assessed by occupational therapists in comparison with their H-Y stages.
Method
Study Design
A retrospective observational study was conducted in compliance with the guidelines of the Declaration of Helsinki to examine the association between disease severity and ADL performance. All patient information was anonymized and stored as unlinked data before analysis to prevent the disclosure of personal information. This study was approved by the Ethics Committee of Sendai Nishitaga National Hospital.
Participants and Data Collection
Data were obtained from the medical records of patients admitted to the hospital for rehabilitation between 2017 and 2020. Patients diagnosed with PD according to the U.K. Brain Bank Criteria (Gibb & Lees, 1988) were included. Conversely, patients who had undergone deep brain stimulation, those who presented with a medical history of diseases of the central nervous system other than PD (e.g., stroke, head injury, and epilepsy), and those who had ADL limitations caused by orthopedic disease were excluded.
Demographic and Clinical Characteristics of Patients
Data on age, sex, disease duration, and levodopa daily equivalent dose were collected from patient records. Global cognitive functioning was assessed using the Mini-Mental State Examination (MMSE; Folstein et al., 1975). The MMSE is a valid and reliable instrument that is widely used to screen for cognitive impairment among older adults (Tombaugh & McIntyre, 1992), and it is also commonly used in PD studies. For example, studies with people with PD using the MMSE have showed a progression in cognitive decline (Roheger et al., 2018), a relationship between cognitive decline and pathological stage (Braak et al., 2006), and a relationship between cognitive decline and brain atrophy (Garcia-Diaz et al., 2014; Zarei et al., 2013).
Outcome Measures
Patients’ H-Y stage (Hoehn & Yahr, 1967), which was assessed by experienced neurologists at admission, was used to determine PD severity. The H-Y scale is a clinical rating scale widely used with patients with PD (Goetz et al., 2004); it categorizes motor function into the following five stages: 1, unilateral involvement only, usually with minimal or no functional impairment; 2, bilateral or midline involvement, without impairment of balance; 3, first sign of impaired righting reflexes; 4, fully developed, severely disabling disease; and 5, confinement to bed or wheelchair unless aided (Hoehn & Yahr, 1967).
The Barthel Index (BI; Mahoney & Barthel, 1965), which occupational therapists used to assess patients at admission, was used to measure independence in performing ADLs. The BI is a valid and reliable outcome measure that can be used to assess level of disability among patients with PD (Taghizadeh et al., 2020). The BI consists of 10 items: feeding, bathing, grooming, dressing, bowel control, bladder control, toilet use, transfers, mobility, and stairs. The scores allotted to each item are as follows: ▪ for bathing and grooming, 0 points (dependent or needs help) or 5 points (independent) per item; ▪ for feeding, dressing, toilet use, and stairs, 0 points (unable or dependent), 5 points (needs help), or 10 points (independent) per item; ▪ for bowel control and bladder control, 0 points (incontinent), 5 points (occasional accident), or 10 points (continent) per item; and ▪ for transfers and mobility, 0 points (unable or immobile), 5 points (major help or wheelchair independent), 10 points (minor help or walk with help), or 15 points (independent) per item.
The total score for each item ranges from 0 to 100, with higher scores indicating greater independence (McDowell, 2006).
Statistical Analysis
We used IBM SPSS Statistics (Version 27) for all analyses, with p < .05 considered significant. Because very few patients were in the H-Y Stage 1 group (n = 5), they were excluded from our analysis. The clinical and demographic data of patients in the other four groups (H-Y Stages 2, 3, 4, and 5) were compared using one-way analyses of variance (ANOVAs) or a χ2 test with post hoc Bonferroni correction. ADL dependency among the four groups was compared using the Kruskal–Wallis H test with post hoc Dunn’s test and Bonferroni correction because of ordered, nonparametric data (Ostertagová et al., 2014).
Results
Demographic and Clinical Characteristics of the Patients
In total, 209 patients with PD (75 men, 134 women) with a mean age of 73.3 yr (SD = 7.7) were included. The demographic and disease-specific features of patients in each group are shown in Table 1. There were 55, 98, 40, and 16 patients in the H-Y Stages 2, 3, 4, and 5 groups, respectively. A one-way ANOVA revealed significant differences in the MMSE scores among the four groups, F(1, 58) = 15.9, p < .001. Post hoc comparisons indicated that MMSE scores were significantly worse in the H-Y Stage 4 and Stage 5 groups than in the H-Y Stage 2 (p <. 001) and H-Y Stage 3 (p <. 001) groups.
Demographical and Clinical Characteristics of the Participants
Note. Post hoc Bonferroni correction: H-Y 2, 3 > 4, 5. LEDD = levodopa daily equivalent dose; H-Y = Hoehn and Yahr; MMSE = Mini-Mental State Examination.
aOne-way analyses of variance or χ2 test.
Comparison of ADL Limitations Across the Four H-Y Groups
Figure 1 shows the prevalence of independence in the ADL subdomains at each stage of PD. The prevalence of independence in the H-Y Stage 2 group was high for feeding (98.2%), grooming (98.2%), bowel control (92.7%), bladder control (94.5%), toilet use (87.3%), and dressing (83.6%) and low for mobility (58.2%) and stairs (58.2%). In the H-Y Stage 3 group, more than half of the patients with PD had limitations in bathing (39.8%), mobility (38.8%), and stairs (26.5%), although most patients remained independent in the other ADLs. In the H-Y Stage 4 group, more than half of the patients required assistance with most ADLs, except feeding and bowel control. In the H-Y Stage 5 group, the prevalence of independence was relatively higher for feeding (43.8%), grooming (37.5%), bowel control (31.3%), and bladder control (25.0%) than for other ADL items, such as bathing (0.0%), dressing (12.5%), toilet use (0.0%), transfers (6.3%), mobility (0.0%), and stairs (0.0%). Details on the frequency of the BI subdomain scores across the four H-Y stages are available in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
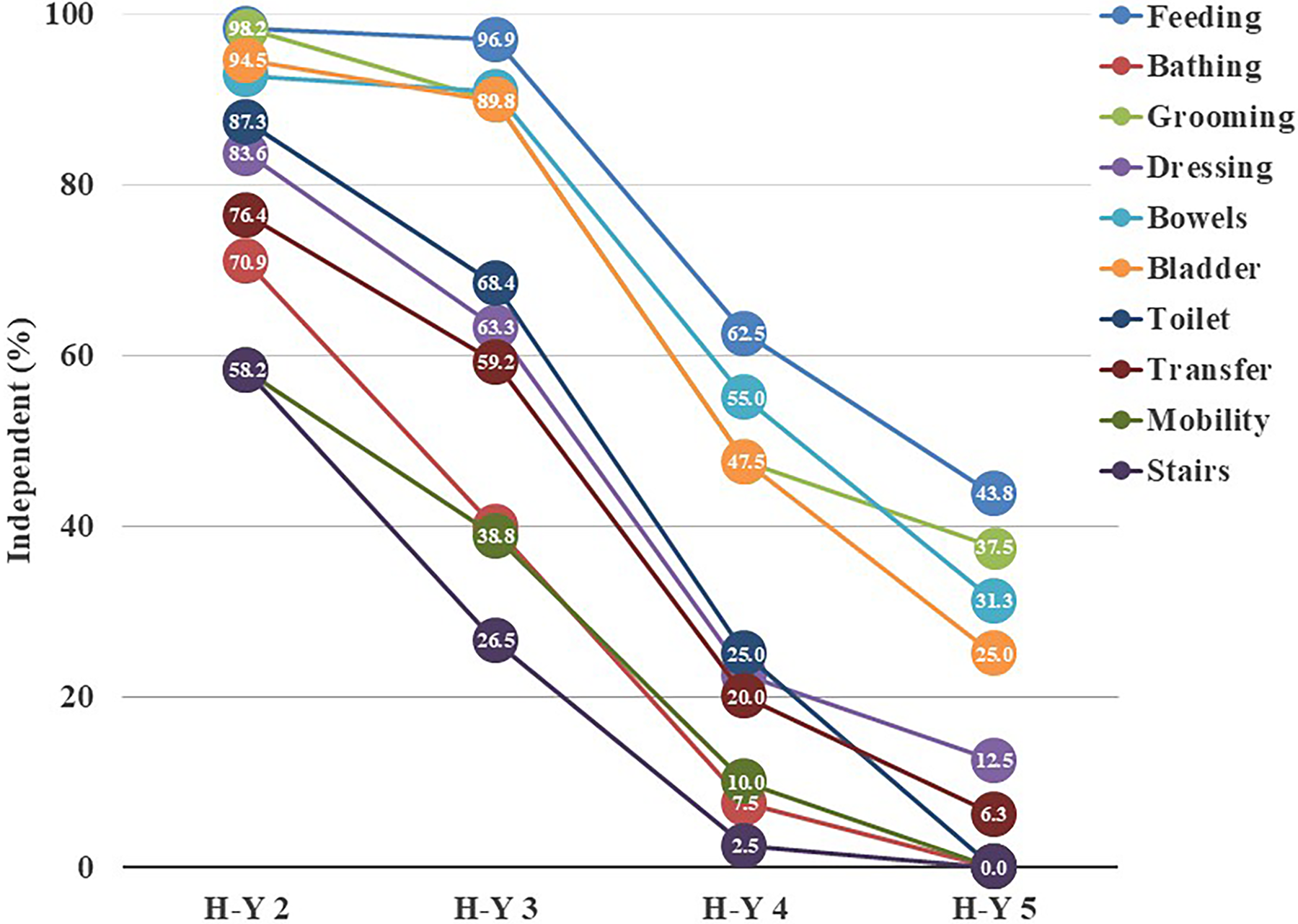
Functional independence in ADL subdomains among patients with PD across H-Y stages.
The Kruskal–Wallis H test revealed significant differences in the total BI score and all BI subdomain scores among the four groups (p < .001 for all comparisons; Table 2). Post hoc analysis showed that the total BI scores were significantly worse in the H-Y Stage 3 group than in the H-Y Stage 2 group (p = .002; Table 2). Similarly, the total BI scores were significantly worse in the H-Y Stage 4 and Stage 5 groups than in the H-Y Stage 2 and Stage 3 groups (p < .001). Feeding, grooming, dressing, bowel control, bladder control, toilet use, transfers, and mobility scores were significantly worse in the H-Y Stage 4 and Stage 5 groups than in the H-Y Stage 2 and Stage 3 groups (p < .001 for all comparisons). Bathing and stairs scores were significantly worse in the H-Y Stage 3 group than in the H-Y Stage 2 group (p < .001 and p = .001, respectively), and they were significantly worse in the H-Y Stage 4 and Stage 5 groups than in the H-Y Stage 2 and Stage 3 groups (p <. 001 for all comparisons; Table 2).
BI Scores Across H-Y Stage
Note. BI = Barthel Index; H-Y = Hoehn and Yahr.
aKruskal–Wallis H test.
bDunn’s test with Bonferroni correction.
Discussion
In this study, we investigated the profiles of ADL functional capacity for patients at each stage of PD. Our findings showed that BI scores decreased as patients progressed to the more severe H-Y stages. This implies that the greater the severity of PD was, the lower the functional capacity of patients. This finding is consistent with previous findings indicating that progression of PD severity was accompanied by increased ADL impairment (Hoehn & Yahr, 1967; Shulman et al., 2008).
This study demonstrated that more than 80% of patients in H-Y Stage 2 remained independent in many ADLs (feeding, grooming, dressing, bowel control, bladder control, and toilet use). Conversely, fewer than 60% of patients with PD in H-Y Stage 2 were independent in walking and stairs. A similar finding was reported by Hariz and Forsgren (2011), who demonstrated that problems with numerous gait-dependent activities, such as “walking in neighborhood,” “transfer to bed,” and “climbing stairs” are exhibited at an early stage of disease. Shulman et al. (2008) also highlighted that gait-dependent ADL disabilities tend to start earlier in the course of PD. Mobility, particularly gait and postural control, is affected in the early stages of PD (Morris et al., 1994); thus, it is not surprising that the rate of independence in walking and stairs was lower than that in the other ADL items in this study. Many previous studies on rehabilitation for patients with PD have focused on improving these abilities (Alves Da Rocha et al., 2015; Keus et al., 2007); thus, gait-dependent activities are the primary target for rehabilitation intervention at earlier stages of the disease.
More than half of the patients with PD in H-Y Stage 3 had limitations in bathing, mobility, and stairs, although most patients remained independent in other ADLs. Notably, the independence in bathing and stairs was significantly lower in the H-Y Stage 3 group than in the H-Y Stage 2 group. The H-Y stages, especially Stages 3 to 5, are weighted toward postural instability, suggesting that the progression of postural instability may limit these activities. In addition to improving postural instability and gait among patients at H-Y Stage 3, appropriate care can include making adaptations in the environment to support postural stability in activities, such as installing grab bars or tub rails for bathing and installing a handrail or a chair lift for stairs (Clapcich et al., 2008).
The frequency of independence in all ADL items was significantly lower among patients in H-Y Stage 4 than among those in H-Y Stage 3, and more than half of the patients in H-Y Stage 4 required assistance for most ADLs, except feeding and bowel control. Iwasa et al. (2021) revealed that the number of patients living in nursing homes significantly increased from Stage 4 onward. A significant deterioration in overall ADL performance may lead patients or their families to consider nursing home admission. In our study, the H-Y Stage 4 group also showed significantly worse performance on the MMSE than the H-Y Stage 3 group. Although the epidemiology of cognitive impairment among people with PD remains unclear, the risk of dementia increases with disease progression (Braak et al., 2006). Rosenthal et al. (2010) revealed that both physical impairment and cognitive function affect some ADL items among patients with PD. Thus, among patients with PD, both cognitive and motor dysfunctions might accelerate the deterioration in ADLs at H-Y Stage 4. Although most intervention studies relevant to occupational therapy and PD have addressed physical performance skills (Foster et al., 2014), consideration of cognitive issues and physical functions in ADL performance is necessary to develop effective rehabilitation programs for patients in H-Y Stage 4.
Fewer than 10% of patients in H-Y Stage 5 were independent in most activities. However, approximately 40% patients with PD remain independent in feeding and grooming, even during the severe stages of the disease. This result indicates that non-gait-dependent activities were relatively preserved, in line with the findings of a previous study that involved patients with PD in a nursing home (Chekani et al., 2016). Previous studies on rehabilitation at an advanced stage have usually focused on motor impairment (Capato et al., 2020). However, the management of PD should not be limited to functional impairments. Non-gait-dependent activities, such as feeding and grooming, as well as patients with PD at an advanced stage, require targeted rehabilitation approaches. Indeed, independence in ADLs has been identified as a determinant of patient satisfaction with overall care (Rosqvist et al., 2019).
Strengths and Limitations
A major strength of this study is that we were able to obtain and review a relatively large dataset that included patients with various severities of PD and associated functional loss. However, this study has several limitations. First, because the study design was cross-sectional, it was not possible to demonstrate the changes in ADL independence over time. Second, the enrolled participants were admitted to a hospital for rehabilitation. Therefore, the sample may have been biased toward people experiencing more severe ADL limitations. Third, although the primary target for rehabilitation intervention at each stage of PD severity was revealed, further research is needed to understand the factors associated with ADL limitations and to design detailed rehabilitation programs. Last, because of the small number of patients in H-Y Stage 5, there could be random variation in the results for this group, which may limit generalizability to the broader population. Future research should reconfirm these findings by conducting a larger scale study.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ Many patients with mild to moderate PD have limitations in stair climbing, mobility, and bathing. These ADLs should be carefully reviewed for patients with mild to moderate PD. ▪ Occupational therapists should consider the effect of not only physical dysfunction but also cognitive function on ADLs among patients in the moderate to advanced PD stages. ▪ Although patients with severe PD have limitations in most ADLs, their independence in feeding and grooming is relatively preserved. These ADLs require a rehabilitation approach that preserves these functions among patients with advanced-stage PD.
Conclusions
This study described profiles of ADL functional capacity among patients with PD based on disease stage. Independence and dependence in ADL items differed according to disease stage.
Supplemental Material
Supplementary material for Profile of Independence in Activities of Daily Living Among Patients With Parkinson’s Disease: A Retrospective Observational Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050882.pdf for Profile of Independence in Activities of Daily Living Among Patients With Parkinson’s Disease: A Retrospective Observational Study by Kayoko Yokoi, Iori Kawasaki, Atsushi Takeda, Aaron M. Eakman and Kazumi Hirayama in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
The positionality of Kayoko Yokoi is that of a Japanese researcher. This study was supported by Japan Society for the Promotion of Science KAKENHI (Grant No. JP20K19416).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.