
Abstract
This review examined the current state of gender-affirming care in occupational therapy and identifies areas for improvement.
Over the past decade, estimates of the number of transgender adults have significantly increased (Meerwijk & Sevelius, 2017). In the United States, 1.6 million people report identifying as a part of the trans community (Herman et al., 2022). Researchers expect this number to grow because of increasing social acceptance and awareness of transgender and gender-diverse (TGD) identities (Rajkovic et al., 2022). Given this increase, it is becoming more likely that occupational therapy practitioners will have clients who identify as TGD. As such, the occupational therapy profession must be prepared to support TGD individuals.
Sex and gender play important roles in influencing health and overall well-being (American Heart Association, 2020; World Health Organization, n.d.). Sex pertains to a set of biological characteristics that are associated with physical and physiological features, including chromosomes, gene expression, hormonal function, and reproductive anatomy (Canadian Institutes of Health Research, Institute of Gender and Health, 2012). Often, the sex assigned at birth, or what is recorded on an individual’s birth certificate, is determined by medical professionals on the basis of biological attributes. Conversely, gender refers to the socially constructed roles, behaviors, and identities attributed to men, women, and gender-diverse people (Canadian Institutes of Health Research, Institute of Gender and Health, 2012). There are subgroups in understanding gender, and these are identity and expression. Gender identity is how someone associates themselves inwardly, and gender expression is how someone presents or performs their gender externally (American Occupational Therapy Association [AOTA], 2023); there are a wide variety of both identities and expressions, and they may change across an individual’s lifespan. Gender expression and identity influence how individuals perceive themselves and others, how they interact with their surroundings, and the distribution of societal power and resources. In many cultures, gender is often incorrectly conceptualized as a binary (male–female), when in reality gender exists on a spectrum (Heidari et al., 2016). TGD people have a gender identity that differs from their sex assigned at birth (University of California, San Francisco, 2016); cisgender is a term used to describe those whose gender identity aligns with their sex assigned at birth (Boston Medical Center, 2024). Language regarding this population has recently changed to reflect terms chosen by the community. Because of this focus on language use, there are a variety of different accepted, respectful descriptors and names for TGD populations (AOTA, 2023).
Conversely, many descriptors have been removed from popular vernacular because they arose from discrimination, bias, or hate (Bouman et al., 2017). As such, it is important to consider that language regarding the TGD community will continue to change over time, and best practices should be continually checked and updated. Here, we use the term TGD because of its recent emergence as a respectful term encompassing a wide range of gender identities (Thorne et al., 2019). Some identities represented under TGD include trans masc (person assigned female at birth whose gender identity leans toward the masculine side of the spectrum; University of California, San Francisco, 2016), trans femme (person assigned male at birth whose identity leans toward the feminine side of the spectrum; University of California, San Francisco, 2016), and nonbinary (someone whose gender is a combination of, or beyond, the traditional binary; AOTA, 2023), among many others. AOTA (2023) summarized terminology for the TGD community in its glossary of gender-affirming language, highlighting the importance of knowledge of language use related to this community.
Although recent years have brought a shift in attention toward providing positive TGD care, this community still disproportionately experiences adverse environmental barriers to occupational engagement, such as extreme poverty, unemployment, housing insecurity, and violence (Grant et al., 2011). Additionally, the TGD community experiences elevated rates of HIV (Grant et al., 2011), and 41% of TGD survey respondents reported at least one suicide attempt (Grant et al., 2011). TGD individuals with intersecting minoritized identities are at even higher risk for health disparities and violence; 84% of TGD victims lost in 2023 were people of color, and 50% were Black transgender women (Human Rights Campaign, 2023). TGD individuals are even underrepresented in health monitoring surveys because of demographics and data collection practices (Bauer et al., 2009), which may increase the health care gap. High rates of depression, suicidality, violence, and substance abuse are also present among youth in the TGD community (Newcomb et al., 2020). One way to help improve health care outcomes for TGD individuals is to begin bridging the gap by creating comfortable environments across professions for individuals to receive health care. In fact, 28% of TGD individuals postponed medical care because of discrimination (Grant et al., 2011). Opportunities exist for occupational therapy practitioners to improve TGD care, support client-centered interactions, and increase holistic care. Addressing the care gap for TGD individuals is the responsibility of all health care professionals, especially occupational therapy practitioners because of occupational therapy’s profession-wide commitment to client-centered care and advocacy (AOTA, 2020).
One way to improve health outcomes and quality of life for TGD individuals is through gender-affirming care (GAC; Bhatt et al., 2022). The World Health Organization (WHO; 2023) defines GAC as interventions aimed at supporting and endorsing an individual’s gender identity that can include many different mediums across settings. GAC can be a lifesaving measure (Inwards-Breland et al., 2022). Any intervention intentionally designed to support and validate an individual’s gender identity is GAC (WHO, 2023). Gender-affirming medical interventions (puberty blockers and hormones) have resulted in significant improvements in depression and suicidality over a 12-mo period and longer (Inwards-Breland et al., 2022). Medical intervention can include hormonal or surgical intervention; however, GAC also encompasses a range of social, psychological, and behavioral interventions. Given the variety of ways to affirm someone’s gender, any practitioner can provide this care. In fact, any practitioner who engages in interpersonal gender-inclusive practices such as listing their own pronouns, using gender-neutral language, and validating TGD clients can have a positive impact on client health outcomes and quality of life (Bhatt et al., 2022). There are also many different ways to validate a TGD individual, including normalizing ways to share or update pronouns, asking a client for their chosen name, and putting inclusive gender options on all paperwork (Jarvis, 2022). Four types of gender affirmation that occupational therapy practitioners could practice are social (e.g., name, pronoun), psychological (e.g., internal, felt self), medical (e.g., hormones, surgery, safe binding practices, and other body modification), and legal (e.g., changing legal gender markers or name; Reisner et al., 2016). On the basis of these classifications, occupational therapy practitioners have the capacity to use GAC in their typical practice or to begin practicing in areas specific to TGD clients.
Although occupational therapy practitioners have the potential to provide GAC, and it is considered high-quality care, it is not being adequately taught in health care professional curricula, and a high prevalence of transphobia remains (Acker, 2017; AOTA, 2021). Contact with TGD people has a statistically significant negative relationship with transphobia, but only 7% of surveyed students reported having contact with TGD people (Acker, 2017). Similarly, exposure to educational content related to transgender issues has shown a correlation with decreased levels of transphobia (Acker, 2017). The need for occupational therapy practitioners’ knowledge about GAC and TGD health factors is juxtaposed with the limited available research on GAC in health professions. The process of transitioning encompasses both mental and physical health, yet the field of occupational therapy lacks substantial discourse on transgender health care (Beagan et al., 2013). Almost one-half of individuals in helping professions presented moderate to high levels of transphobia (Acker, 2017). In fact, occupational therapy students reported significantly higher levels of transphobia compared with social work students (Acker, 2017). Throughout history and until the present time, TGD clients have been subjected to microaggressions, misgendering, and harassment from health care professionals and other clients (Bhatt et al., 2022). Although transphobia in the medical setting is often unintentional, it is one of many barriers to health faced by TGD people, because it shapes their health care interactions (Heng et al., 2018).
Occupational therapy practitioners have the potential to make a positive impact in the TGD community, serving as supports for everyday living and transitions. TGD individuals report facing occupational losses, adaptation, and gaining of new meaningful occupations at different points in gender transition (Beagan et al., 2012; Schneider et al., 2019). Gender identity and occupation have a transactional relationship: Participants’ gender identities shape their occupational engagement, and they use occupations to convey their gender identity (Beagan et al., 2012). These relationships between occupation and gender identity affect overall well-being, health, and occupational participation. Again, this is reflected in AOTA (2021) policy, which states that gender-diverse individuals participate in occupations in distinct and meaningful ways. Occupational therapy practitioners would have a larger scope of practice and a more positive impact on health outcomes in any setting if they were knowledgeable about and confident in administering care that is gender inclusive and considers how TGD individuals create their identity through occupation.
Occupational therapy practitioners are positioned to include affirming gender-diverse clients as part of providing ethical care, yet there is a lack of training, knowledge, and consistency in conceptualizing what GAC entails in practice. Without sufficient training and education on GAC in occupational therapy, practitioners are left questioning how to implement GAC and what best practices are. A first step to revealing and enhancing occupational therapy practitioners’ potential roles is to explore the professional literature to see how and to what extent GAC has been evoked. Our objective in this scoping review is to summarize the existing literature related to GAC in occupational therapy, identify gaps, and offer recommendations for integrating GAC knowledge into occupational therapy practice. Our aims were to (1) describe the current published perspectives on GAC in occupational therapy, (2) summarize language use related to GAC and how it has changed over time, and (3) describe gaps in peer-reviewed published literature related to GAC.
Method
Protocol and Registration
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018) and the JBI Scoping Review Network (Peters et al., 2022). The final protocol was registered on the Open Science Framework on August 31, 2023, and is accessible at https://osf.io/jgz93/.
Eligibility Criteria
Studies were included if they (1) included the term gender-affirming care, (2) included language relating to the TGD community (e.g., gender diverse, gender fluid, nonbinary, transgender, or any noncisgender identity), and (3) mentioned occupational therapy. Articles published between the date of database inception and September 2023 were included. Studies included qualitative, quantitative, and mixed-methods research. Articles were excluded if they were not peer-reviewed (e.g., magazine articles, dissertations, book chapters), did not include intervention, or were theory-based articles.
Information Sources and Search
A detailed systematic biomedical literature search was executed by an experienced medical librarian (Kim L. Lipsey) using a combination of standardized subject terms, keywords, and wildcard searching for relevant concepts, including but not limited to androgyny, gender-affirming care, gender dysphoria, gender expression, gender identity, gender nonbinary, gender reassignment, gender transition, hormone therapy, LGBTQ, occupational justice, occupational therapy, occupational transitions, sexual and gender minorities, transgender, transgender persons, and Two-Spirit. Six databases—PubMed/MEDLINE, EMBASE, Scopus, PsycINFO, CINAHL, and Web of Science—were searched from their date of inception (1946, 1947, 1823, 1800, and 1937, respectively) through September 19, 2023 (date of search). All results were exported to EndNote (Clarivate). The medical librarian (Lipsey) used the duplicate finder in EndNote, and 222 duplicates were assumed to be accurately identified using the methodology outlined by the Better Duplicate Detection For Systematic Reviewers: Evaluation of Systematic Review Assistant-Deduplication Module (Rathbone et al., 2015). Identified duplicates were then removed, for a total of 614 unique citations. The complete search strategy is available in Appendix A of the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Selection of Sources of Evidence
The research team met before each review round to ensure consistency and discuss criteria for inclusion and best practices for the review. First, all four team members (Laurel K. Stugart, Sophia C. Larson, Grayson Owens, Catherine R. Hoyt) independently reviewed titles and abstracts (two team members per article) for inclusion through the Covidence systematic review management system (Veritas Health Innovation, Melbourne, Victoria, Australia), and two similar votes indicated the decision for that title. All four team members discussed differences regarding study inclusion until a consensus was reached. After abstract appraisal, all authors (two for each article) reviewed the full text and determined final article selection.
Data Charting Process and Data Items
Stugart, Larson, Owens, and Hoyt met to determine extraction elements. Three reviewers independently extracted data (Stugart, Larson, and Owens), and two reviewers completed extraction for each individual text; the data extraction form was updated throughout the process. Consensus for each data extraction point was agreed upon by three reviewers (Stugart, Larson, and Owens). The following data were extracted from all final studies: country in which the study was conducted, original language, aim of the study, setting, practice domain, definition of GAC, population description, type of GAC, inclusion and exclusion criteria, participant age, total number of participants, stage of transition, design of the study, funding, participant recruitment method, conclusions, and author-identified next steps. Categories for the type of GAC were based on those outlined by Reisner et al. (2016). Data were summarized and can be found in Table A.1 in the Supplemental Material.
After data collection and review completion, three community reviewers assessed the review for (1) language use regarding the TGD community, (2) interpretation of results, and (3) methodology. Community reviewers were selected on the basis of background and expertise in one or more of these criteria.
Synthesis of Results
The full data extraction chart, with each study listed alphabetically by author, is available in the Supplemental Material (see Table A.1). We analyzed the following characteristics of each reported study: country in which the study was conducted; aim of the study; theory, model, or framework; definition of GAC; language used regarding the TGD community; setting; practice domain; design of the study; population description; inclusion and exclusion criteria; participant age; total number of participants; stage of transition; participant recruitment method; intervention description; outcome measures; conclusions; and author-identified next steps. Data on language used in the study regarding GAC and TGD people, country of origin, and original language (when translated) were collected and are provided alphabetically by study author in Table A.2. Data charts reflect the terminology and language use regarding TGD populations of the original article.
Results
Selection of Sources of Evidence
Database searches returned 614 unique citations, which were uploaded to the Covidence systematic review management system and screened at the title and abstract level. During the screening process, 566 articles were removed because they did not meet inclusion criteria (n = 549) or were duplicates (n = 17). After title and abstract screening, 48 articles remained for full-text review. We removed 31 articles during full-text assessment for (1) lack of focus on GAC (n = 12), (2) focus on the queer population without specific inclusion of TGD language (n = 8), (3) lack of peer-reviewed status (n = 6), (4) identification as a review article (n = 3), and (5) not including occupational therapy (n = 2). A total of 17 studies were included (Figure 1).
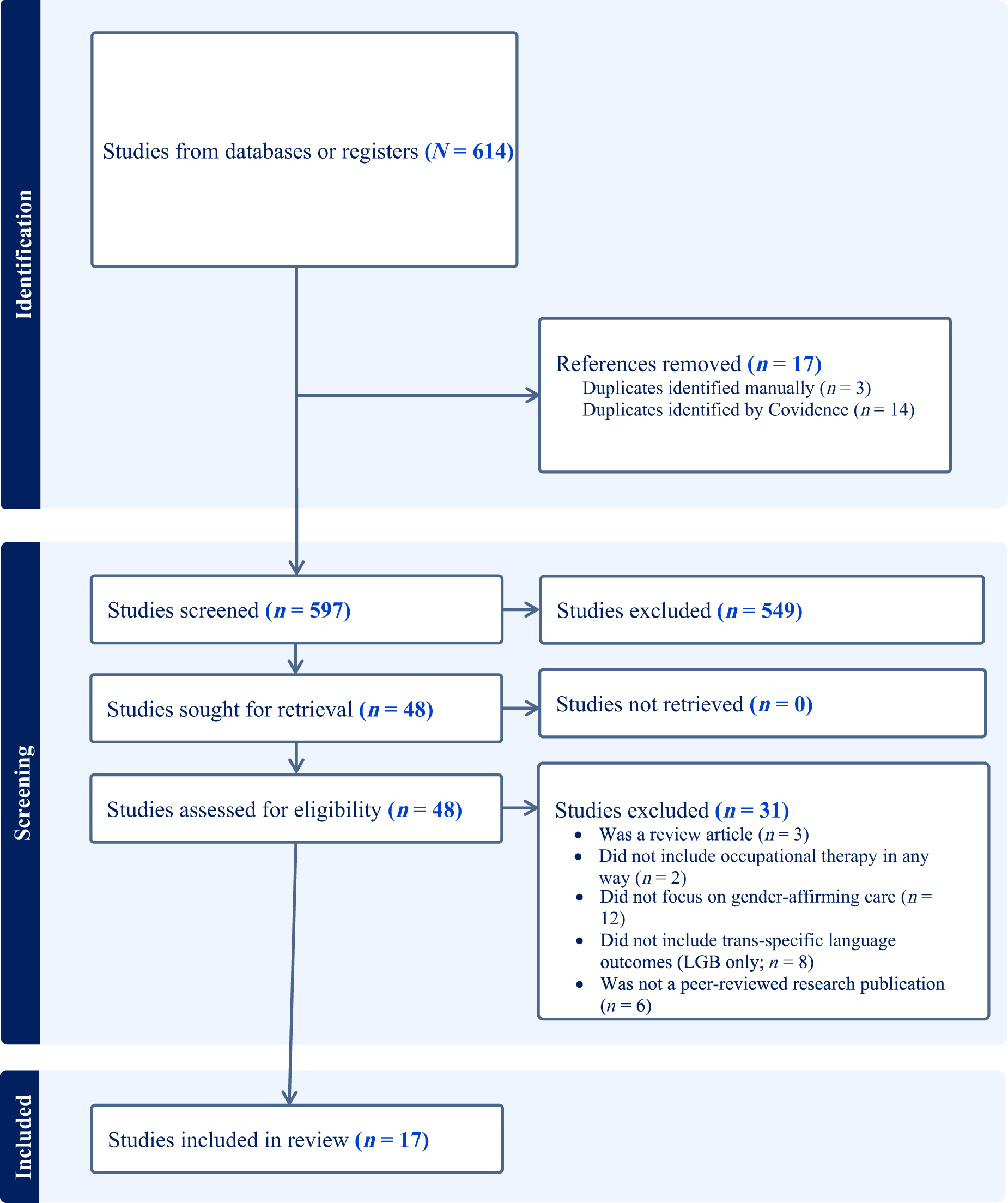
Flow diagram of search procedures.
Characteristics of Sources of Evidence
Publication characteristics are summarized in Table 1. All but 1 study were published between 2000 and 2023, with the majority (n = 9) published between 2021 and 2023. Canada had the most studies published (n = 8; Bar et al., 2016; Beagan et al., 2012, 2013; Hanafy et al., 2022; Lindsay & Kolne, 2020, 2022; Lindsay et al., 2021, 2022). Study designs were mostly qualitative (n = 9; Beagan et al., 2012, 2013; Gómez-Antilef et al., 2020; Hanafy et al., 2022; Lindsay & Kolne, 2020, 2022; Lindsay et al., 2021, 2022; McCarthy et al., 2022; Swenson et al., 2022). Further details on study characteristics and data extracted can be found in Table A.1.
Study Characteristics (N = 17)
General Trends
More than 70% of the included studies on GAC in occupational therapy practice were published by U.S. and Canadian authors. Almost one-half of the articles focused on the clinician perspective (n = 8; 47%); three indicated that clinicians want more training on GAC (Hanafy et al., 2022; Lindsay & Kolne, 2020; Lindsay et al., 2022). Additionally, six articles pointed to a need for more training on GAC for occupational therapy practitioners (Hanafy et al., 2022; Lindsay & Kolne, 2020, 2022; Lindsay et al., 2022; Steuer & Walker, 2023; Swenson et al., 2022). Studies uncovered that occupational therapy practitioners feel a lack of knowledge about and confidence in working with TGD clients, and they desire more training across delivery modalities. Qualitative research was the most common type of research for this topic and accounted for more than half (n = 9; 53%) of the included studies (Beagan et al., 2012, 2013; Gómez-Antilef et al., 2020; Hanafy et al., 2022; Lindsay & Kolne, 2020, 2022; Lindsay et al., 2021, 2022; McCarthy et al., 2022; Swenson et al., 2022). Cultivation of supportive environments, furthering provider education, and taking on advocacy roles were described as opportunities.
The assessment of these global trends allows us to identify current gaps in knowledge. The inclusion of more evidence centered on client perspectives could make research more holistic. As clinicians, it is important to assess research articles from other countries and cultures not only to understand clients with perspectives other than one’s own but also to potentially learn from others when it comes to best practices. Thus, that the research originated primarily in Western countries constitutes a gap in the literature and decreased generalizability. The lack of research on specific interventions further complicates occupational therapy care for the TGD population; only four articles detailed such an intervention (Hanafy et al., 2022; Jessop, 1993; Steuer & Walker, 2023; Wasmuth et al., 2021). Of the four interventions described, one focused on people with traumatic brain injury (Hanafy et al., 2022), another was on vaginoplasty (Steuer & Walker, 2023), one addressed community and stigma issues (Wasmuth et al., 2021), and only one consisted of individualized occupational therapy services (Jessop, 1993). Of the included articles, about 41% (n = 7) pinpointed actual actionable items to incorporate into practice, providing a limited view of how to change current practice (Bar et al., 2016; Beagan et al., 2013; Gómez-Antilef et al., 2020; Jessop, 1993; Lindsay & Kolne, 2020, 2022; Steuer & Walker, 2023). Furthermore, the suggestions made in those seven articles included advocacy and creating supportive environments but contained little specifics on how to accomplish these changes (Bar et al., 2016; Beagan et al., 2013; Gómez-Antilef et al., 2020; Jessop, 1993; Lindsay & Kolne, 2020, 2022; Steuer & Walker, 2023). The literature suggested that additional research (n = 10; 59%) is an important next step (Beagan et al., 2012; Beagan et al., 2013; Bolding et al., 2022; Hanafy et al., 2022; Lindsay & Kolne, 2020; Lindsay et al., 2021, 2022; McCarthy et al., 2022; Schneider et al., 2019; Swenson et al., 2022). Additionally, research (n = 9; 53%) pointed to either a current lack of practitioner knowledge or a need for further occupational therapy practitioner training (Beagan et al., 2013; Bolding et al., 2022; Hanafy et al., 2022; Lindsay & Kolne, 2020, 2022; Lindsay et al., 2021, 2022; Steuer & Walker, 2023; Swenson et al., 2022).
Synthesis of Result
Most of the existing literature used a qualitative or narrative approach to deepen the field’s understanding of how identifying as transgender shapes daily occupations (e.g., Beagan et al., 2012; Schneider et al., 2019; Swenson et al., 2022). However, the field lacks interventions specifically designed to promote GAC.
On the basis of this review, we determined that the existing literature encompasses two main categories: clinician-reported comfort and knowledge working with TGD individuals and TGD individuals’ reported experiences. The first category encompasses training and education sessions that focus on cultivating a gender-inclusive environment. Provider education aims to enhance clinicians’ comfort with and competence in caring for TGD clients (Beagan et al., 2013; Bolding et al., 2022; Lindsay & Kolne, 2020, 2022; Lindsay et al., 2021, 2022). This review revealed a lack of confidence among health care providers in delivering inclusive and sensitive care to TGD individuals, emphasizing the need for further tailored training and education to enhance awareness and competence in providing gender affirming care. Occupational therapy interventions in the literature focus primarily on activities of daily living (Steuer & Walker, 2023), instrumental activities of daily living, and occupations involved in identity expression, such as clothing management, social outings, hair care, and skin care (Jessop, 1993). Addressing postoperative education and care, including mental health considerations (Steuer & Walker, 2023), has emerged as a crucial component of GAC for occupational therapy practitioners working with TGD clients undergoing a surgical procedure.
Collectively, the available research advocates for occupational therapy practitioners to address three main factors in GAC: (1) gender-inclusive language and practices, (2) cultivation of a supportive environment, and (3) further education. The current body of literature positions the field as a pivotal player in advancing social justice, equality, and authentic gender expression for TGD individuals across diverse life stages and health care settings. The existing literature posits that occupational therapy practitioners should take on advocacy roles for the TGD community.
Discussion
In this study, we explored the trends in the current occupational therapy literature regarding GAC. We identified 17 primary studies addressing GAC in occupational therapy practice. Findings indicated a paucity of overall research on this topic; specifically, the number of studies considered quantitative or high-level evidence was low. Most articles originated in the United States or Canada, which provides a primarily Western perspective and renders findings nongeneralizable. We also found an overall lack of evidence for a specific intervention or practice related to GAC. Articles predominantly discussed a need for more training and education for occupational therapy practitioners but did not include a perspective on how this should be implemented.
Limitations of this review include the low number of scoping reviews on this topic, which led us to include studies published in any year, such that not all included studies were current. However, this shows a large range of language and knowledge on topics surrounding gender and how these have changed over time. Another limitation to the study process is that data extraction points for the full-text review were inherently determined before reading the included articles. For this reason, some articles did not align with the categories we selected. Although this posed a challenge for the current study, it was telling that research did not encompass categories we thought would be addressed in the literature, further emphasizing the gaps in occupational therapy research around GAC.
Future research should include more high-quality research on more specific practices and interventions to determine best practices with this population and to help guide occupational therapy practitioners in deciding how to deliver GAC. Occupational therapy practitioners could benefit from research on how to change practices in their current settings and interventions (e.g., language use), as well as how they can work within specific GAC interventions (e.g., post–gender-affirming top or bottom surgery care, help with gender change in legal documentation). Further research on one-on-one sessions as well as group therapy sessions could benefit occupational therapy practitioners. Because published research on GAC in occupational therapy is limited, practitioners should also consider non–peer-reviewed literature to guide practice and inform future studies. Some practitioners are beginning to explore and create innovative ways to integrate these concepts into practice. One of the best ways to gain knowledge on these subjects is connecting with related panels and speaking to those currently providing GAC.
Implications for Occupational Therapy Practice
The current state of research on GAC in occupational therapy practice limits the amount and clarity of direct implications for practice that can be gleaned from this work. However, the following implications for occupational therapy are extremely important, as evidenced by their reiteration throughout the evidence: ▪ Practice guidelines for GAC in occupational therapy need to be created. ▪ More training is needed, specifically in language use and the unique occupational engagement of TGD populations. Trainings should also consider culture and the role of intersectionality in gender identity and expression. ▪ Trainings on GAC should be integrated into both practice and education across multiple mediums (online, in clinics, etc.) These trainings can stand alone or be integrated seamlessly into current curricula. Such integration into current teaching is especially relevant in academia to accommodate the time constraints of occupational therapy education.
Conclusion
The lack of evidence on GAC in occupational therapy practice poses a challenge for occupational therapy practitioners, especially when juxtaposed with the ethical obligation to provide occupational therapy intervention that applies principles of GAC. Specifically, the lack of intervention and implementation studies further increases the uncertainty that occupational therapy practitioners feel in administering GAC. There were insufficient data to conduct a systematic review or meta-analysis; thus, the aim of this scoping review was to assess what evidence currently exists on GAC in occupational therapy practice and to identify any gaps in the literature. We found that although GAC is important in all stages, it is especially prevalent in gender transition periods (i.e., when a person is beginning to ask people to use new pronouns, going through a name change, or generally adjusting so that their daily life aligns more closely with their gender identity (Planned Parenthood Federation of America, 2024). As such, next steps should involve special consideration of gender transition periods and the creation of interventions tailored to assisting in occupation change.
Next steps should include further training of occupational therapy practitioners in how to deliver GAC, and training should be provided over many different platforms (e.g., in person, online). Education is a funnel for practice, and learners from three health professions including occupational therapy who identified with historically marginalized groups have reported experiencing isolation, normative curricula, and marginalization by classmates and instructors (Pride et al., 2024). For this reason, training in GAC and TGD health should also be provided in occupational therapy education and academic settings. Further evidence could help shape practice guidelines and training for occupational therapy practitioners. Health care professions can learn from one another; thus, evidence from other health care fields should be assessed (Beagan et al., 2013).
Supplemental Material
Supplementary material for Gender-Affirming Care Is Not Standard Care in Occupational Therapy: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050883.pdf for Gender-Affirming Care Is Not Standard Care in Occupational Therapy: A Scoping Review by Laurel K. Stugart, Sophia C. Larson, Kim L. Lipsey, Grayson Owens and Catherine R. Hoyt in The American Journal of Occupational Therapy
Footnotes
*Indicates studies included in the scoping review.
Acknowledgments
Thank you to the community reviewers: Steve Taff, PhD, OTR/L, FNAP, FAOTA; Bri Guillory, OTD; and Cody R. Meyer, MA, LPC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.