
Abstract
This project identified challenges and supports for Black American families of autistic children regarding access to and engagement in occupational therapy services.
Autism spectrum disorder is the most prevalent neurodevelopmental disorder, affecting 1 in 36 children (Maenner et al., 2023), inclusive of minority groups, but despite this fact, research for standardizing assessments and interventions has used a majority White sample (DuBay et al., 2018; Maenner et al., 2023). Minority representation in health care research is often lacking, which affects providers’ recognition of autism symptoms and presentation in children from minority groups, delaying diagnosis and referrals. These delays are exacerbated by health care professionals’ limited knowledge about relevant resources and tools for children and families from diverse groups, such as population-validated evaluations (Stahmer et al., 2019).
Various cultural biases and logistical factors also affect access to autism services. Parents and caregivers from minority groups, including Black American families, report negative health care experiences, such as being dismissed by health care staff who normalize parental concerns and fail to make referrals for needed therapies. These factors can contribute to patient–provider mistrust, perpetuated by stigma within diverse communities and bias from health care providers (DuBay et al., 2018; Stahmer et al., 2019).
These disparities in access to and utilization of services extend to occupational therapy services for autistic children. Occupational therapy is one of the most used and requested services by the families of autistic children to support participation in daily life and routines and to address the sensory factors that often affect their participation (Shepherd et al., 2018). In a recent study, 68.2% of Black American autistic children were reported to have sensory features (Kirby et al., 2022). Sensory features are part of the diagnostic criteria for autism and are linked to challenges with sleeping, eating, adaptive behaviors, emotional regulation, and motor development, which can affect daily life and routines (Kirby et al., 2022). Occupational therapy using Ayres Sensory Integration® (OT–ASI; Ayres, 1979; Schaaf & Mailloux, 2015) is an evidence-based intervention that focuses on improving participation in tasks, activities, and occupations through individually tailored, sensory–motor activities, contextualized in play at the just-right challenge (Steinbrenner et al., 2020). However, there are no cultural adaptations of this intervention for Black American autistic children. Because therapeutic goals and parental concerns differ on the basis of culture and identity, interventions such as OT–ASI may require extensive adaptation to ensure cultural responsiveness (DuBay et al., 2018).
Thus, in this project, we aimed to adapt the OT–ASI intervention to be culturally responsive for Black American families of autistic children to improve its utilization and acceptability. The specific aims were to identify cultural barriers and facilitators of occupational therapy service utilization and access for Black American families of autistic children and to use these findings to adapt the existing OT–ASI intervention to be culturally responsive for Black American families of autistic children.
Method
This qualitative study referenced the Cultural Adaptation Process (CAP; Bernal et al., 2009; Domenech Rodríguez et al., 2011), a systematic process to culturally tailor an intervention according to diverse populations, to guide the adaptation of OT–ASI. The CAP involves three phases: researching and collaborating with persons from the relevant population and assessing needs, adapting the intervention, and reviewing and revising adaptations to prepare for testing (Domenech Rodríguez et al., 2011). The CAP aligns with the scope of occupational therapy in being client centered and addressing factors that could affect participation, such as attitudes held by others outside of the clients, the need for supportive relationships, and services not meeting clients’ needs (American Occupational Therapy Association, 2020).
This article details the research team’s process through the first two phases of CAP. Phase 1 included reviewing relevant research and conducting online focus groups and interviews, and Phase 2 included adapting the OT–ASI intervention on the basis of literature and findings from the focus groups and interviews. All study procedures received approval through the Thomas Jefferson University Institutional Review Board. All included participants consented to this project and were assigned a randomly generated three-digit number for anonymity.
Recruitment and Participants
Convenience sampling was completed through the research team’s professional networks and at local community organizations and fairs. The research team reviewed project details with interested participants and completed eligibility screening. Participants included cultural experts, Black American parents or caregivers of autistic children, and occupational therapy practitioners to discuss barriers and supports to occupational therapy services. Inclusion criteria were as follows: ▪ For cultural experts, having a job that supports Black American culture. ▪ For parents and caregivers, self-identifying as Black American and having a child with an autism diagnosis. ▪ For clinicians, being an occupational therapy practitioner and actively providing services to Black American autistic children.
Eligible participants completed informed consent and received an e-mail with the date, time, and Zoom link for the focus group or interview, access to an online document for writing thoughts during and after the online discussions, and the research team’s contact information.
Data Collection
Focus groups were coordinated according to participants’ schedules. When participants could not attend a focus group because of scheduling changes or emergencies, individual interviews were conducted. The focus group or interview questions queried participants about the cultural barriers to occupational therapy service access and utilization (e.g., “What problems have you experienced with accessing occupational therapy services for your child?”), facilitators to utilizing services (e.g., “Can you tell us about any efforts by your occupational therapy practitioner working to address any of these needs?”), ways to design therapy sessions for optimal support and engagement (e.g., timing, frequency, format), and efforts or training to develop trustworthy provider–caregiver relationships. The questions were focused on occupational therapy services in general and did not ask specifically about OT–ASI so that a broader understanding of experiences and barriers could be identified. Each focus group and interview began with introductions, session rules, and an icebreaker. The questions were shared verbally and shown on the shared Zoom screen. Two focus groups (one for all practitioners and another for parents and caregivers), two cultural expert interviews, and two parent interviews occurred between April 2022 and June 2022.
Data Processing and Analysis
Recordings were transcribed using Otter.ai, an online transcription program (https://otter.ai/). Three research team members compared transcripts with the recordings to ensure accuracy. Finalized deidentified transcripts were imported to NVivo, a qualitative analysis software (https://help-nv.qsrinternational.com/12/win/v12.1.115-d3ea61/Content/welcome.htm). Thematic analysis adhered to recommended procedures (Castleberry & Nolen, 2018; Saldaña, 2016). Three research team members independently completed initial and inductive coding, reviewed the codes, and recoded as needed. Each member reviewed the data at least three times before triangulation meetings for each transcript. During triangulation meetings, the team engaged in open discussions, allowing members to share their rationales and reach a consensus on themes. After determining each group’s overall themes, we developed a thematic map to represent the findings.
Trustworthiness Procedures
Credibility was implemented through researcher triangulation involving three research team members who reviewed transcriptions, completed independent coding, participated in team meetings, and discussed the coding and themes. We sent member-checking surveys to the participant groups to gain feedback and ensure a valid interpretation of the results. Reflexivity was implemented through team members’ documenting reflections of their personal views to reduce bias. Transferability was achieved through descriptions of the collected data and themes. Dependability was demonstrated through an audit trail (i.e., recordings of the focus groups and interviews, logs of transcripts, codebooks, thematic rationales and decisions, study coordination, and reflexivity throughout the study; Nowell et al., 2017).
Results
CAP Phase 1: Focus Group and Interview Findings
Of the 20 prospective participants who responded with interest, 4 did not respond for eligibility screening, 1 was ineligible during screening, and 3 completed screening but had scheduling conflicts. Twelve adults completed eligibility screening, provided consent, and participated. Characteristic information for the included participants is available in Table 1.
Participant Characteristics
Themes about challenges, supports, and parent or caregiver roles emerged. Each participant quote is followed by their random participant number in parentheses. Five themes emerged from the participants about challenges in accessing and utilizing services (Figure 1).
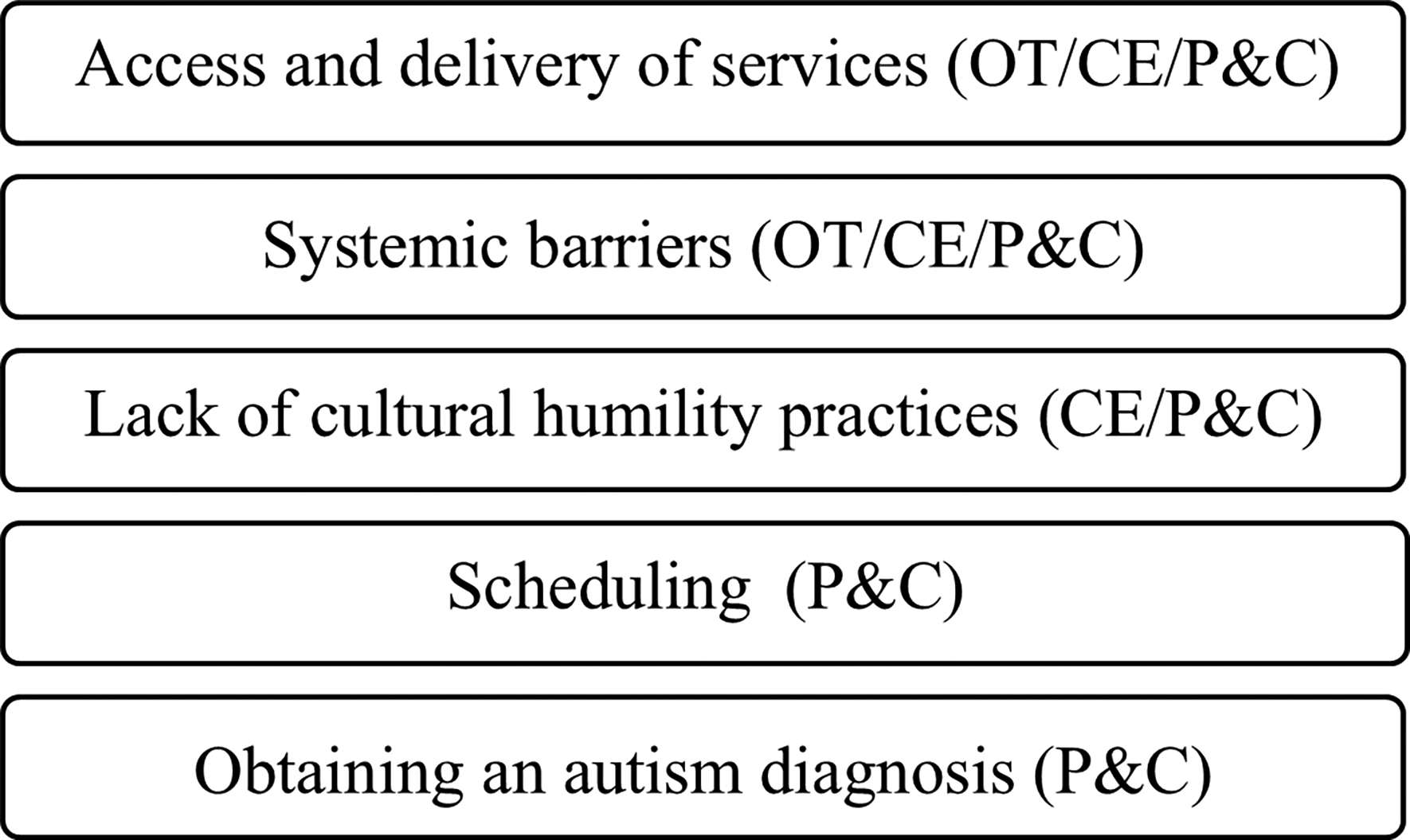
Barriers and challenges identified by all participant groups.
Access to and Delivery of Services
All participant groups discussed challenges to access and delivery of services. Parents and caregivers identified a lack of inclusion of family traditions and values, poor communication, provider bias, and being dismissed because of their race as impediments to accessing services. A parent explained, And I’ll say as a mom and a Black woman.… It’s really crazy because, as a Black woman, I already experienced it, but raising a Black boy on the spectrum, it’s like it’s a constant, “No, you need to listen to what I’m saying” and then people trying to tell me kind of what they think. (No. 185)
Practitioners identified similar challenges regarding communication: Families may be unfamiliar with occupational therapy, which inhibits trust and parent–practitioner relationships. Also, practitioners noted that many assessments did not incorporate cultural diversity or information on cultural relevance.
Cultural experts identified challenges with the complexity of special education systems, the use of jargon, and the lack of communication about benefits and services for families. Experts noted that some Black American families are hesitant to have early intervention because of practitioners who are predominantly White coming to their homes and because of cultural differences such as multigenerational households, parenting methods, and traditions related to self-care.
Systemic Barriers
All participants detailed barriers embedded throughout the health care system that affect Black American families’ access to services. Parents and caregivers reported an unequal geographic distribution of therapy services, with most outpatient therapy centers being in urban or higher income areas, requiring reliable transportation, time, and financial resources. Limited public transportation makes traveling difficult for some families with children with greater needs, and parking in cities is costly.
All parents and caregivers agreed that waitlists were a significant barrier to services, and some directly referenced the impact of racial profiling on access to services. A parent spoke about an incident during which, after health care staff misnamed her, she clarified her real name, then next minute, they’re like, asking me questions like “Oh, well, is that the father of all your kids?” Or it’s just like some crazy stuff when I’m sitting here trying to get services. And I’m not like, none of that should even matter…. Different things that they’re asking me that I know that they’re like racially profiling me. If I can put it that way, and it’s very sad, it’s hurtful. And I feel just because of that, I feel like I’m put on waiting lists. (No. 107)
Lack of Cultural Humility Practices
Parents, caregivers, and experts shared how biases from practitioners and disregarding cultural values and preferences create barriers to optimal care. An expert noted, “If someone feels like you’re not honoring their family situation, you’re looking down upon it because it’s different, then that creates an initial feeling of, you’re not going to give me the best care” (No. 155). Parents, caregivers, and cultural experts also identified a paucity of male practitioners and representation in health care. One parent expanded on the impact for Black American autistic children, “When they see somebody that looks like them can make a big difference. And when they see that it’s a male, especially for boys that might not have a male, that’s very helpful” (No. 141).
Scheduling Challenges
Parents and caregivers identified challenges in scheduling therapy services and the need for flexibility in therapy delivery, including services after school, during regular business hours, and on weekends. When considering the format of therapy delivery, parents and caregivers expressed wanting flexibility with in-person and remote therapy options according to individual needs and preferences.
Challenges of Obtaining an Autism Diagnosis
Parents and caregivers expressed frustration with the effort and time needed to get an autism diagnosis and how pediatricians and other providers often dismissed their concerns. Sometimes, they were told to wait and “watch,” referring to the child’s development. Furthermore, parents identified the lack of available resources and information on autism and ineffective autism screening during medical visits as challenges.
Eight themes emerged from the participants about supports that improve access to and delivery of occupational therapy services (Figure 2).
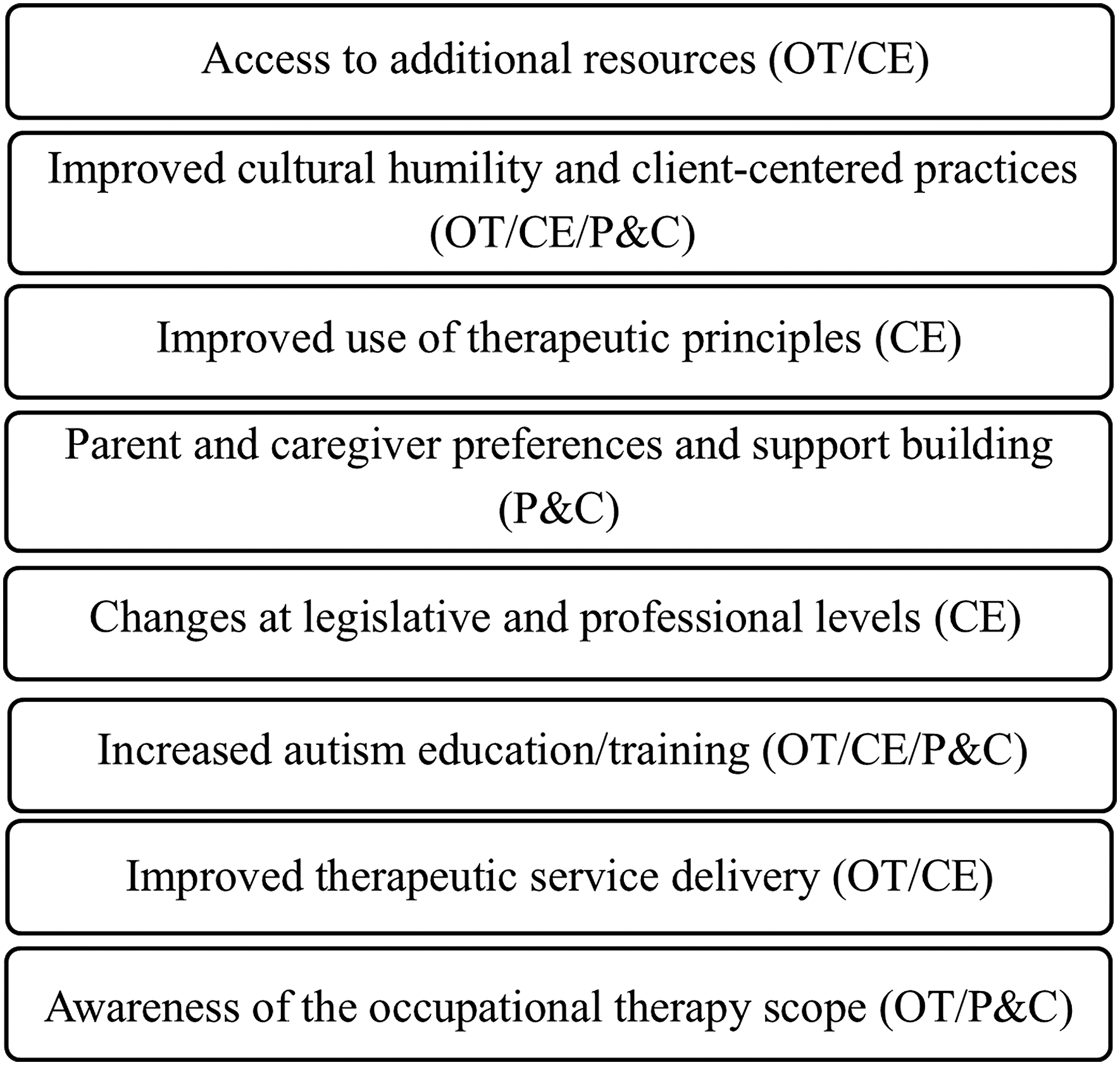
Supports identified by all participant groups.
Access to Additional Resources
Practitioners and experts identified the importance of community outreach, resources distributed to communities, and shared transportation systems to alleviate the travel burdens to therapy sites. Peer support networks between Black American families also increased awareness of available services. One expert shared, We had other parents who are at different stages in the diagnosis be in the same room so that they could talk to each other about, “Okay, I know this now, but when I was where you are, I didn’t know that then.” So they were able to talk to each other. (No. 180)
Improved Cultural Humility and Client-Centered Practices
All participants noted practitioners’ use of culturally responsive practices as a support. Parents and caregivers discussed how relationships and respect from practitioners helped them to benefit more from services. Practitioners reinforced using culturally sensitive materials and learning about families’ cultural backgrounds. A practitioner said, “I do try to dig a little bit deeper during the parent interview portion of the evaluations to identify things that are of cultural importance to the families, like religious importance” (No. 158).
Improved Use of Therapeutic Principles
Cultural experts discussed improved use of therapeutic service principles, including increased collaboration between providers and parents, parental engagement, and the use of lay language. A cultural expert said, “If we connect implicit bias and cultural humility to our code of ethics, to therapeutic use of self, it becomes embedded into all of the things we emphasize in our profession” (No. 155). Education and training for providers, parents, and caregivers were recommended to improve engagement and recognition of the signs and symptoms of autism in diverse populations.
Parent and Caregiver Preferences and Support Building
Parents and caregivers identified the importance of including service delivery preference (e.g., the setting, time, and frequency of services) and establishing practitioner–client partnerships through trust and collaboration to build support. A parent shared that “having the parent’s number and having a relationship where they can text each other to me is a must. Because I text mine almost every day or every other day or some sort of point of contact” (No. 185).
Changes at a Legislative and Professional Level
Experts shared that legislative and professional changes also need to be made. At the legislative level, increased funding and outreach for underserved communities were identified as ways to be inclusive of Black American families. At the professional level, experts reinforced the need for provider training on cultural humility while increasing initiatives to make the occupational therapy profession more diverse.
Increased Autism Education and Training
All participants agreed that families benefit from increased education about occupational therapy (e.g., the areas addressed, the strategies and interventions used, and how they differ from other professions). Practitioners noted the importance of education about different professions and services that can work together to support children’s outcomes.
Improved Therapeutic Service Delivery
Practitioners and experts identified strategies to improve service delivery, including building a collaborative team involving the family, effectively communicating, and empowering parents and caregivers to be active leaders throughout the therapeutic process. An expert noted, I do think that taking the approach of the parent as a member of the team, and the child as a member of the team, and yeah, just taking that approach, so that, yeah, we might be the experts in terms of occupational therapy, but the parent and the child are the experts of the child that we’re working with and what that looks like for that parent. (No. 180)
Awareness of the Scope of Occupational Therapy
Parents and caregivers discussed how services would be used more if there was increased awareness of the role of occupational therapy. Strategies to accomplish this included outreach to the larger community and more parent and caregiver resources about occupational therapy and other services. Practitioners reported that increasing health care providers’ awareness can provide more appropriate referrals for occupational therapy services.
Two themes emerged from parents and caregivers about the importance of their experiences and roles in the therapeutic process (Figure 3).
Parent and caregiver experiences and roles related to therapy.
Successful Strategies
Parents and caregivers shared that they found meaning in their role on the treatment team. They recommended establishing a good relationship with practitioners and ongoing communication and collaboration to achieve goals, adopt new routines, and participate in new activities and services. One parent spoke about a practitioner who “was very quick in returning e-mails and offering other therapies or things to try; she would tell me what skills she is trying to work on and things at home that would reinforce that” (No. 139).
Advocacy Efforts
Parents and caregivers shared that they had to take on a new role in navigating the health system and advocating for their child to obtain a diagnosis and high-quality services. Advocating included creating parent support networks, peer networks to identify providers, and petitions to increase school access to autism-related services. One parent stated, “One thing I’m proud of is becoming an advocate for my daughter” (No. 139). Parents and caregivers also reinforced advocating for more cultural humility and responsiveness.
CAP Phase 2: Intervention Adaptation
After the thematic analysis, specific adaptations for the OT–ASI intervention were incorporated into the manual on the basis of the insight and expertise of participants and from relevant literature.
Cultural Humility Information and Resources
These adaptations included information for practitioners about cultural humility, the intersection between occupational therapy and cultural humility, and training and self-assessment resources. The research team also provided cultural humility training links and podcasts for guided resources, research articles, and organizational and webinar discussion links. Cultural humility resources included methods for ongoing self-reflection throughout the therapeutic process and intervention sessions through cultural humility scales and reflection forms.
Important Cultural Considerations During the OT–ASI Process
The adapted manual included cultural consideration prompts throughout the therapeutic process. Cultural interview questions were provided to explore and incorporate family traditions, religion, values, and interests. Adaptations included guidance in a family-centered approach to the exploration of cultural considerations and the meaningfulness of daily occupations and intervention goals. Reminders were embedded to reinforce the use of culturally appropriate and diverse materials (e.g., toys, printed items, visuals) during intervention sessions. Handouts were developed with lay language about occupational therapy, OT–ASI, and how to access services. Additional resources detailed the therapeutic process and the assessments (i.e., the purpose, what it measures, and what the interpretations indicate), as well as local and national resources and support groups.
Family Considerations
Adaptations in the OT–ASI manual included reinforcement of respecting each family member’s preferred name and correct pronunciation, as well as guidance on utilizing the families’ preferred communication methods (e.g., calls, text, and e-mail). Additional guidance included collaborating with scheduling and the session format, with remote or hybrid sessions provided as needed to support families’ preferences, busy schedules, or emergencies. Prompts were embedded throughout the manual to reinforce the importance of collaborating with parents and caregivers who are the experts regarding their children.
Discussion
This study referenced the CAP to guide cultural adaptations of the OT–ASI intervention for Black American autistic children. While the use of convenience sampling limits the generalization of findings, it contributed to the inclusion of people invested in the research topic and built on established relationships, resulting in engaged focus group/interview discussions. The themes from the focus group and interview discussions correspond with current research on challenges of and facilitators to accessing services for culturally diverse populations (Onovbiona et al., 2024; Pearson et al., 2020; Rivera-Figueroa et al., 2022; Smith et al., 2020).
Systemic barriers that impede access to services, such as lack of transportation options and location of clinics, were evident in our data and have been noted in other studies as well (Onovbiona et al., 2024; Stahmer et al., 2019) and necessitate the inclusion of alternate delivery models to ensure accessibility. We incorporated flexible formats of therapy delivery, including remote options, to assist in bridging service gaps. OT–ASI is primarily provided in clinics, but it has been recently translated into a remote delivery format (Schiano et al., 2024). Families have reported remote delivery as a convenient method and supported collaboration (Wallisch et al., 2019). However, because not all parents and caregivers will prefer remote delivery (Ferguson et al., 2022), it is crucial to collaborate on the preferred therapy delivery formats that best match the needs of the families.
Participants identified a need for improved cultural humility practices and considering the family's cultural values and preferences, which is supported by literature reporting that practitioners demonstrating poor cultural responsiveness can negatively affect the parent–practitioner relationship (Smith et al., 2020). Research supports the inclusion of cultural humility for improved quality of life, effective treatments, increased client-centered practice, and increased feelings of being heard and treated with compassion and respect (Agner, 2020; Foronda et al., 2016).
Parents and caregivers also identified that advocacy for their child’s needs was essential for increasing service quality and improving practitioners’ awareness of the need for culturally responsive services. These findings are consistent with current research about the importance of building parent–practitioner relationships for dual advocacy to facilitate access to services for autistic children and their families (Rivera-Figueroa et al., 2022; Stahmer et al., 2019). Thus, it was essential to create and synthesize resources to empower parents and caregivers in their knowledge of occupational therapy, OT–ASI, and resources; and to develop practitioners’ cultural humility skills for culturally sensitive services.
Limitations
Having a small number of participants through convenience sampling and having an occupational therapy practitioner group that consisted of only White women may affect the generalizability of our findings. It would have been beneficial to seek Black American practitioners who work with autistic children to learn from their lived experiences. Because most parents and caregivers were from an urban region, engaging suburban and rural communities could reveal additional considerations and needs. Given that the parents’ and caregivers’ children had a wide age range (4–16 yr), it is difficult to determine whether our findings are applicable to specific age groups. Furthermore, because of their schedules and emergency conflicts, several participants engaged in interviews instead of focus groups, which could have affected their comfort and exploration of topics.
Implications for Occupational Therapy Practice
Culturally adapted evidence-based interventions ensure that service provision is culturally responsive and aligns with parents’ and caregivers’ needs and expectations. This study has the following implications for occupational therapy practice: ▪ Occupational therapy practitioners should advocate for and provide lay language information to health care providers, parents, and caregivers about autism and occupational therapy to increase their awareness of available services and how children can be supported. ▪ Collaboration and respect for families’ cultures, structures, and schedules are important in improving therapeutic service delivery. ▪ Occupational therapy practitioners should engage in cultural humility training; collaborate to incorporate the families’ traditions, values, and interests; and self-reflect throughout the therapeutic process.
Conclusion
Culturally adapting occupational therapy interventions is an essential step toward equitable and inclusive practice in supporting children and families from diverse cultural and ethnic backgrounds. This article details the cultural adaptation of an occupational therapy intervention that is based on input from Black American parents and caregivers, practitioners, and cultural experts. Future studies will evaluate the adapted intervention’s acceptability and feasibility.
Footnotes
Acknowledgments
This project was supported by the Jefferson College of Rehabilitation Sciences Dean’s Award and the Nancy Talbot Postdoctoral Research Fellowship funded by the American Occupational Therapy Foundation.