
Abstract
This study assessed cognitive self-efficacy and its clinical significance among individuals with fibromyalgia syndrome.
Fibromyalgia syndrome (FMS), a type of chronic widespread pain, affects 0.4% to 8.8% of the global population, with a mean prevalence of 2.7% (Sarzi-Puttini et al., 2020). FMS is characterized by pain in at least four of five body regions and is associated with multiple symptoms, such as sleep disorders, cognitive dysfunction, somatic symptoms, functional disability (Nicholas et al., 2019; Sarzi-Puttini et al., 2020), lower perceived health (Hoffman & Dukes, 2008), and multisensory overresponsiveness (Harte et al., 2018). The mechanism underlying FMS is derived from central sensitization processes in which innocuous or normally painful stimuli are perceived as painful or elicit more intense pain, respectively (Pinto et al., 2023). The cognitive difficulties in FMS, manifested in attention, working memory, and information-processing impairments (Bell et al., 2018), are thought to derive from constant pain, which acts as a prominent distractor that drains attentional resources (Teodoro et al., 2018). More important, cognitive factors can also modulate and affect the intensity of subjective pain (Sarzi-Puttini et al., 2020).
One of these cognitive factors that influence the pain experience is self-efficacy, defined as people’s belief about their abilities to generate effects (Bandura & Wessels, 1997). It is an “operative competence” (Bandura, 1982, p. 122) requiring emotional and cognitive skills to manage and face obstacles or aversive experiences. Self-efficacy is key in enhancing chronic pain treatment outcomes (Raman & Sharma, 2022), reducing functional impairment and emotional distress (Jackson et al., 2014), enhancing physical activity adherence (Raman & Sharma, 2022), and contributing to overall resilience (Cheng et al., 2018). However, patients with FMS demonstrated lower self-efficacy compared with patients with rheumatoid arthritis, which negatively correlated with disease severity, depression, perceived health, fatigue, and pain intensity (Moyano et al., 2019).
Cognitive self-efficacy (CSE) is a specific type of self-efficacy and is defined as the belief in one’s own capacity to cope with cognitive challenges and to effectively use cognitive skills in various situations (Toglia et al., 2020). For nonclinical populations over the life course, CSE was found to affect goal setting, task persistence, and strategy use throughout an activity (Berry & West, 1993), highlighting its role in occupational performance. Thus, the relationship between CSE and occupational performance may expand the understanding of a patient’s functional barriers (Gage & Polatajko, 1994), especially among patients with FMS, characterized by cognitive difficulties (Bell et al., 2018; Glass, 2008). Thus, assessment and monitoring of CSE may add to the intervention process and improve occupational therapy outcomes (Gage & Polatajko, 1994). However, to the best of our knowledge, an empirical study testing CSE and its relation to FMS has not yet been reported. Given the clinical heterogeneity reported among FMS patients whereby physical, social, and psychological profiles differ (Gianlorenço et al., 2024; Yim et al., 2017), a similar heterogeneity in CSE is expected. Therefore, this study’s goals were to (1) explore the CSE levels of individuals with FMS compared with healthy population norms; (2) reveal the FMS heterogeneity using CSE as a classifier variable; and (3) test the clinical significance of CSE in relation to FMS symptom severity, pain-related function, sensory responsiveness, and perceived health.
Method
Study Design
After Tel Aviv University Institutional Ethics Review Board approval (0002991-1), this cross-sectional study used an online survey through Qualtrics. Anonymous participants were required to indicate their consent before responding to survey items.
Participants
This study included men and women with a diagnosis of FMS. The sample was purposive, and participants were recruited online via a link to the study survey, published on social media and FMS online communities. Study inclusion criteria were Hebrew speaking, older than age 18 yr, and a specific date of a formal FMS diagnosis.
Measures
Sociodemographic and Health Information Form
This self-report form, developed for the study, consisted of sociodemographic and health information and was used to verify the inclusion criteria.
Cognitive Self-Efficacy Questionnaire II
The Cognitive Self-Efficacy Questionnaire II (CSEQ; Toglia & Johnston, 2017) assesses people’s beliefs regarding their ability to recognize, monitor, and manage cognitive symptoms (e.g., cognitive fatigue, slow processing speed, difficulty organizing information) and everyday challenging cognitive activities (e.g., coordinating schedules, following a group conversation). In addition, this measure examines people’s ability to identify and apply strategies to everyday problem situations that involve cognitive skills (Toglia & Johnston, 2017). Although the CSEQ includes four parts, we used Parts I and II for this study. Part I includes 16 items that assess a person’s self-confidence in recognizing cognitive symptoms during an activity. Part II includes 19 items examining the person’s level of certainty in managing the cognitive symptoms when they occur. The items in all subscales are rated on a 10-point scale, with 0 indicating no sense of self-efficacy and 10 indicating the highest sense of self-efficacy (Jethani et al., 2023). Established norms for the test, based on healthy participants (N = 200, ages 18–64), were published in Toglia et al. (2020).
Fibromyalgia Impact Questionnaire
The Fibromyalgia Impact Questionnaire (FIQ) is a self-report questionnaire designed to assess patients’ current health status and the influence of FMS symptoms on their daily life (Bennett, 2005; Burckhardt et al., 1991). The FIQ contains 10 questions regarding the ability to perform gross motor everyday tasks in the past week (e.g., shopping, cooking, driving), number of days absent from work because of FMS symptoms during the past week, and a symptom severity scale (e.g., depression, fatigue, pain). Higher scores indicate a greater impact of FMS on function (Bennett, 2005; Iversen, 2003). In this study, we used both the total FIQ and Item 3 (“How many days did you miss work last week?”) scores.
Brief Pain Inventory
The Brief Pain Inventory (BPI; Cleeland & Ryan, 1991) was developed to provide a quick and easy self-administered tool to measure pain intensity and the extent of its interference in the lives of patients with various pain conditions (Tan et al., 2004). Respondents rate their worst, least, and average pain level in the past 24 hr, current pain intensity, and degree to which pain interferes with seven domains of functioning on a scale of 0 (no interference) to 10 (interferes completely). Scores are calculated on two scales, Pain Intensity and Pain Interference, with higher scores indicating greater pain and its functional impact.
Sensory Responsiveness Questionnaire
The Sensory Responsiveness Questionnaire (SRQ; Bar-Shalita et al., 2009) consists of 58 items assessing responses to daily sensory scenarios, including auditory, visual, gustatory, olfactory, vestibular, and somatosensory stimuli, excluding pain. The SRQ is used to identify sensory over- and underresponsiveness. Items are stated in a manner that attributes a hedonic or aversive disposition to the situation. By using a 5-point scale of 1 (not at all) to 5 (very much), the SRQ yields two scores, SRQ–Aversive and SRQ–Hedonic, providing two cutoffs for over- and underresponsiveness, respectively. Higher scores indicate greater overresponsiveness or underresponsiveness (Bar-Shalita et al., 2015).
Self-Rated Health
We assessed self-rated health (SRH; Martikainen et al., 1999) with a single-item self-report of perceived health by asking, “Generally speaking, how would you rate your health?” Responses range from 1 (excellent) to 5 (poor). Poor SRH was found to be associated with chronic pain states, including FMS (Mäntyselkä et al., 2003).
Procedure
Participants were requested to complete an online survey and were given the option to leave items unanswered or cease answering at any point. The survey took an average of 45 min to complete.
Statistical Analysis
We used IBM SPSS Statistics (Version 26) to perform all statistical analysis. Descriptive statistics for continuous variables were summarized by means and standard deviations, and nominal variables were summarized and categorized by frequencies. The statistical significance was set at p ≤ .05.
First, we performed a two-step cluster analysis to identify subgroups in the dataset based on CSE mean scores. We assessed the cluster model fit by using Schwarz’s Bayesian information criterion (Schwarz, 1978) and calculated the quality of the cluster model by using the silhouette score method. A value near +1 indicates a good model fit, a value around 0 suggests the data point could belong to another cluster, and a value near –1 indicates the data point is likely in the wrong cluster (Shahapure & Nicholas, 2020).
We tested the cluster association with sociodemographic variables by using chi-square and t tests. Then, we performed a multivariate analysis of variance (MANOVA) to test the differences in the study measures by cluster groups, revealing the external validity of the cluster model (Benassi et al., 2020). The effect size for testing group differences was calculated via partial η with cutoff for small (η2 = 0.01), medium (η2 = 0.06), and large (η2 = 0.14) effects (Schelly & Ohl, 2019). Because participants were allowed to leave questions unanswered, the MANOVA procedure included participants who completed all survey items without missing data (N = 100).
Results
Participants
Data were collected between April and August 2021 (N = 118 responders). The sample consisted of 109 women (92.4%; age, M = 42.64 yr, SD = 13.12; disease duration, M = 5.94 yr, SD = 6.03) and 9 men (7.6%; age, M = 38.22 yr, SD = 9.23; disease duration, M = 3.37 yr, SD = 2.72). Using the SRQ we identified 92% with multisensory overresponsiveness. When we divided the sample by sex, using the Mann–Whitney U test, groups did not differ in age (z = –1.05, p = .29) and in disease duration (z = –0.96, p = .334). The sample demographic characteristics are presented in Table 1.
Demographic Characteristics of Participants With Fibromyalgia Syndrome (N = 118)
Data are missing for occupational status (n = 4).
CSEQ Scores (Parts I and II): Relation to Published Norms
The mean scores of CSEQ Parts I (M = 7.05, SD = 1.99) and II (M = 6.69, SD = 1.9) for the FMS participants were lower than those for healthy participants (M = 8.2, SD = 1.2 and M = 8.1, SD = 1.3, respectively). The FMS sample scores fell within the 10th to 20th percentile of the population distribution (Toglia et al., 2020).
Cluster Analysis Model
The cluster model included the CSE total score as the classifier variable. The derived model yielded two cluster groups with a good cluster quality reflected by a silhouette index of 0.7 (Supandi et al., 2021). The two cluster groups were low CSE (M = 5.81, SD = 1.3) and high CSE (M = 8.65, SD = 0.83), yielding significant mean differences between groups, t(115) = 14.48, p < .001.
Sociodemographic Characteristics of the Cluster Groups
The χ2 analysis showed nonsignificant associations between the cluster and gender (Φ = –0.90, p = .331), marital status (Φ = 2.42, p = .658), education (Φ = .097, p = .574), and occupational status (Φ = .096, p = .306). Although not statistically significant (Φ = 5.54, p = .063), a higher percentage of participants in the low-CSE cluster group reported a below-average income (79%) than the high-CSE group (59.5%). Conversely, more participants in the high-CSE cluster group reported above-average income (23.8%) than those in the low-CSE group (10.1%). Based on the data derived from the third question of the FIQ, the low-CSE cluster group had significantly more work absences in the past week (M = 3.13, SD = 2.33) compared with the high-CSE cluster group (M = 2.20, SD = 2.04), p = .042. There was no significant difference in disease duration between the groups, t(115) = 1.76, p = .077.
CSE Clusters: Clinical Significance
Table 2 presents the differences between the two cluster groups for the study measures. The high-CSE cluster group showed significantly higher SRH (p = .049) and lower scores for the FIQ and BPI–Interference (p < .001), the latter with a large effect size (Figure 1). The differences in the SRQ (both Hedonic and Aversive scales) and BPI–Severity scores were not statistically significant.
Differences in Study Measures Based on the CSE Cluster Groups
Note. The measurement scores were based on their total score. CSE = cognitive self-efficacy; FIQ = Fibromyalgia Impact Questionnaire (possible scores range from 0 to 10, with higher scores indicating greater impact of fibromyalgia syndrome on function); BPI = Brief Pain Inventory (possible scores range from 0 to 10, with higher scores indicating greater pain and its functional impact); SRQ = Sensory Responsiveness Questionnaire (possible scores range from 1 to 5, with higher scores indicating greater over- or underresponsiveness); SRH = self-rated health (possible scores for this single item range from 1 to 5, with higher scores indicating poorer health and more chronic pain).
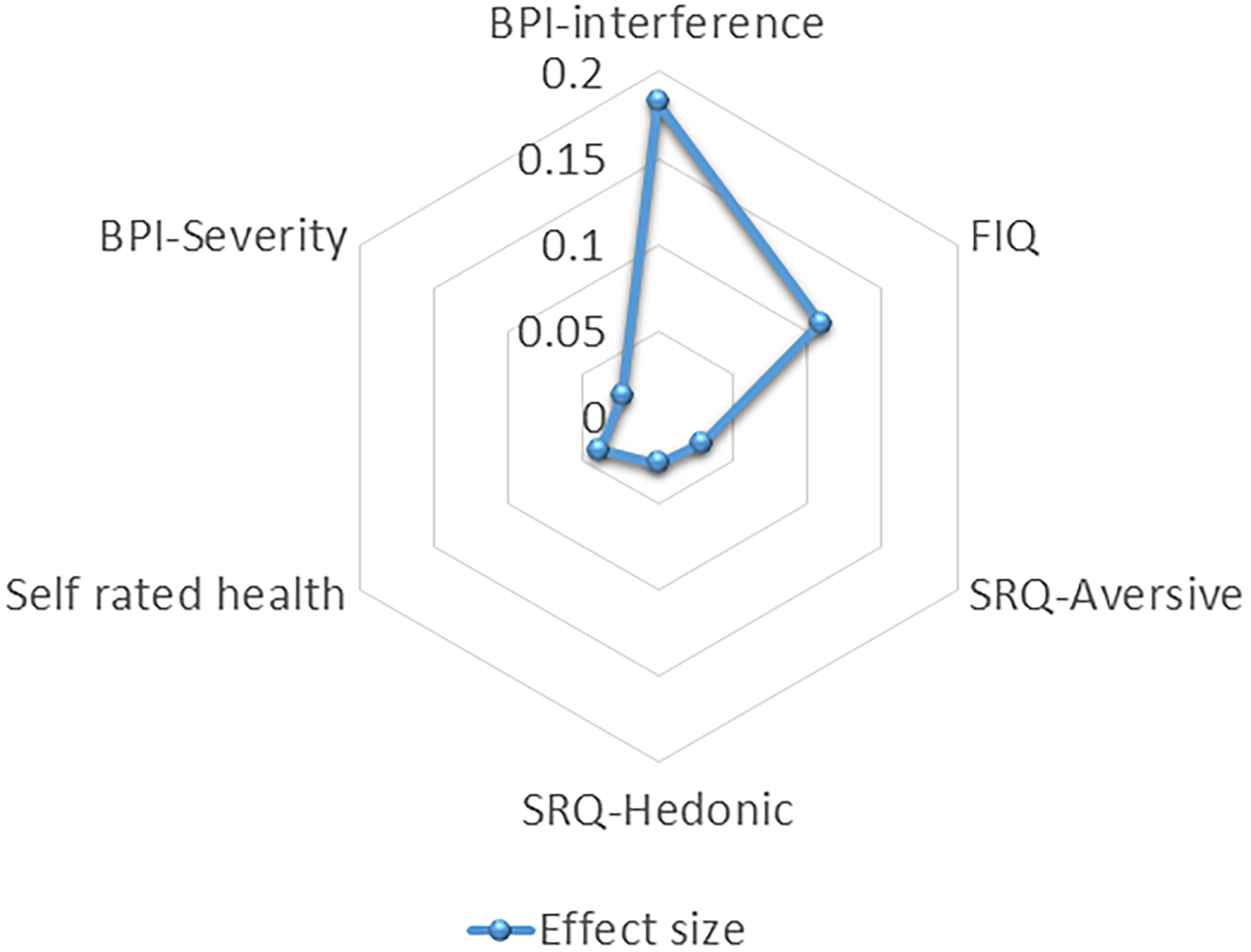
Effect sizes of study measures by cluster membership.
Discussion
The study aimed to assess the CSE levels and their clinical significance in a sample of participants with FMS. Findings revealed that the CSEQ scores of the FMS participants were lower than the healthy population norms. Participants were categorized into high- and low-CSE groups using the CSEQ as a defining variable. The high-CSE cluster group showed significantly fewer absent days from work, lower fibromyalgia severity and pain interference, and higher perceived health. However, the groups did not differ in sensory responsiveness and pain severity scores.
CSE of Participants With FMS
Attention and memory difficulties are woven into FMS symptomatology (Bell et al., 2018). Thus, it is not surprising that FMS participants had lower CSE than the healthy population, which may reflect lower confidence in their ability to recognize cognitive symptoms within an activity or use cognitive skills effectively in various situations (Jethani et al., 2023). Moreover, the chronicity of physical and emotional symptoms and perceiving their vulnerability as validating their poor performance can lead to negative self-judgment, affecting their self-efficacy (Bandura & Wessels, 1997). Self-efficacy and cognitive appraisal are theoretically (Gist & Mitchell, 1992) and empirically (Diotaiuti et al., 2023) associated. Cognitive appraisal refers to the way people assess a particular situation and choose actions to mitigate risks or enhance potential benefits (Folkman et al., 1986). Threat anticipates future harm or loss, whereas challenged appraisal foresees the potential for gain even in demanding situations (Folkman et al., 1986). Specifically, an association was suggested between negative appraisal and lower CSE (Putwain et al., 2015). A recently developed model (Pinto et al., 2023) implied that FMS is derived from an overactive threat response and an underactive soothing–affiliative system. The model suggests that a predominance of harm and threat appraisals might play a significant role in FMS pathomechanisms, which may be associated with lower personal resources such as reduced resilience and self-efficacy (Pinto et al., 2023).
Clinical Relevance of CSE Classification in FMS
In the context of chronic pain, patients with high CSE may approach pain as a challenge to overcome and actively seek ways to manage its impact; consequently, they may be less prone to rumination and feeling overwhelmed by pain (Cheng et al., 2018). Furthermore, self-efficacy in FMS emerged as a significant positive predictor of reduced pain behaviors and higher physical activity (Buckelew et al., 1994; Culos‐Reed & Brawley, 2003) as well as for better functional, psychological, and ill adjustment (Sahar et al., 2016). Our findings indicate that the high-CSE group showed lower FIQ and pain interference scores and higher perceived health. More important, the differences in the FIQ and pain interference are considered clinically meaningful (Bennett et al., 2009; Cheng et al., 2018). These findings imply that targeting self-efficacy during assessment and treatment may improve functional outcomes (Gage & Polatajko, 1994). Indeed, an occupational therapy pain program that focuses on building mastery over significant activities despite pain was shown to contribute to higher self-efficacy, which had a significant positive impact on occupational performance (Thomas et al., 2021).
The high- and low-CSE cluster groups differed in pain interference but not in pain intensity. The association between pain severity and pain interference is complex. Although some studies found mutual associations (Jensen et al., 2017), others reconfirmed that pain severity and pain interference present distinct factors of pain dimensions (Fayers et al., 2011), specifically in musculoskeletal types of pain such as FMS (Jumbo et al., 2021). Furthermore, the cluster groups did not differ in sensory responsiveness; both groups demonstrated sensory overresponsiveness, a condition characterized by allodynia, hyperalgesia, and after-sensation (Bar-Shalita et al., 2019; Weissman‐Fogel et al., 2018), indicating central sensitization (D’Mello & Dickenson, 2008; Woolf & Max, 2001; Woolf & Salter, 2000). Indeed, the pain matrix processes both noxious and non-noxious sensory stimuli, shaping the interrelationship between pain intensity and sensory responsiveness (Mouraux et al., 2011; Senkowski et al., 2014). Of note, this is the first study to quantify sensory overresponsiveness, indicating very high incidence. Given that pain and sensory amplification are both core FMS clinical and nociplastic pain constituents (Harte et al., 2018; Nicholas et al., 2019) and thus fundamental in FMS development, they may be less influenced by CSE in FMS, which explains our findings.
Analyzing the differences between the high- and low-CSE cluster groups indicated that the fibromyalgia impact and pain interference showed the highest effect size. More important, the high-CSE cluster group participants had less absence from work, and a higher percentage reported above-average income levels. These findings indicate that CSE could be regarded as functionally oriented, emphasizing cognitive engagement and using cognitive strategies such as self-regulation, goal setting, motivation, and self-management, all of which are crucial for daily functioning (Jethani et al., 2023). These strategies may also promote better disease management, contributing to higher perceived health and further supporting our results.
Identifying two distinct groups of CSE—high and low—validates the sample’s heterogeneity and supports previous findings that active coping strategies are associated with better FMS adjustment (Braun et al., 2020; Raak et al., 2003; Rubio Fidel et al., 2022). Self-efficacy serves as a source of active, positive coping (Sahar et al., 2016), which the occupational therapy practice framework identifies as one of the psychological assets that internally influence function and disability (American Occupational Therapy Association, 2020).
The findings support targeting CSE in occupational therapy practice as a valuable personal factor that may affect FMS and pain-related function. Future research should explore the specific effects of CSE in FMS compared with other self-efficacy domains and develop CSE-enhancing therapeutic intervention to assess their effectiveness.
Study Limitations
This study had several limitations that may affect the generalizability of findings. FMS diagnosis was based on self-report, though participants provided the date of formal diagnosis. Although our sample was consistent with other FMS research, most participants were women and were highly educated. Furthermore, this research relied on self-reported measures and did not include clinical tests or functional observations. Finally, 15% of participants did not complete the FIQ, although the groups did not differ in other study measures.
Implications for Occupational Therapy Practice
The findings of this study confirm the importance of recognizing coping and self-belief factors as reflecting cognitive and emotional mechanisms that may guide precision therapeutic intervention of patients with FMS. CSE is a new measure not commonly encountered in occupational therapy practice. Therefore, this study has the following implications for occupational therapy practice: ▪ The findings highlight the importance of assessing and targeting CSE of individuals with FMS during occupational therapy intervention, particularly those with cognitive symptoms, significant functional limitations, and nonadaptive behaviors, to improve disease management and pain-related function. ▪ The findings suggest that CSE can serve as a clinical marker of functional abilities and coping strategies, explaining gaps between functional abilities and actual performance of individuals with FMS.
Conclusion
This study aimed to reveal CSE heterogeneity and its clinical significance among FMS participants. Findings show that CSE influences pain-related function, symptom severity, and subjective health but not pain severity or sensory responsiveness, suggesting its role in cognitive–emotional domains of coping and functioning of individuals with FMS.
Footnotes
Acknowledgments
We thank the participants for their time and effort. Hana Karpin and Ronnie Deutsch contributed equally to this study.