
Abstract
Focusing on Latino families affected by cancer, this study showed that familismo, which prioritizes family needs over individual needs, is a cultural value that plays out in many ways.
In 2024, an estimated 195,300 Latinos in the United States were diagnosed with cancer (American Cancer Society, 2024) and joined the growing cancer survivor community (Miller et al., 2021). Latinos experience cancer disparities in large part because of the social determinants of health—such as limited access to health insurance and financial resources—that affect health care access (Kronenfeld et al., 2021). For example, cancer is the leading cause of death among Latinos because they are also more likely to be diagnosed at a later stage than non-Hispanic Whites (Miller et al., 2021). Latino/a cancer survivors (LCSs) report worse psychological, physical, and social well-being compared to other racial/ethnic groups (Samuel et al., 2020). Consequently, there is increased attention to the occupational injustices of LCSs. LCSs experience occupational deprivation because they not only face the common challenges encountered by the broader cancer survivor community (e.g., functional deficits, treatment side effects) but also navigate unique contexts (e.g., low socioeconomic status, political climates, language barriers) that hinder participation (Ramirez et al., 2022; Sleight, 2017). Despite these disparities, Latino representation in broader oncology research is lacking (Kronenfeld et al., 2021). Similarly, occupational therapy cancer research is largely silent on issues of race/ethnicity (Buwana et al., 2023; Newman et al., 2024). As the occupational therapy profession continues to expand its reach to diverse populations, there are opportunities to further learn about the Latino community’s culture to best serve them within the context of cancer care.
Culturally tailored interventions show great promise to improve the health and participation of Latino communities affected by cancer (Baquero & Parra-Medina, 2020). Although Latino culture is heterogeneous, there are salient cultural values that are important to understand when developing culturally tailored interventions. One prominent Latino cultural value is familismo, which prioritizes close immediate and extended family relationships with loyalty, respect, obligation, and support (Sabogal et al., 1987). Grounded in interdependence and reciprocity, familismo prioritizes family needs over individual ones (Adames & Chavez-Dueñas, 2017). The literature has documented the various impacts of familismo on LCSs. Familismo can serve as a protective factor against depression and facilitate social support throughout the cancer care continuum (Marín-Chollom & Revenson, 2022; Torres-Blasco et al., 2022). When cultural expectations related to familismo are not met, LCSs report experiencing social isolation (Barden et al., 2016). Given familismo’s emphasis on family needs over individual ones, LCSs may minimize their personal needs to avoid burdening their families (Lopez-Class et al., 2011). Given the many ways this cultural value can play out, familismo should be considered when developing culturally tailored interventions for LCSs (Graves et al., 2012). Despite the relevance of familismo to LCSs, no occupational therapy–informed studies have focused primarily on the role of familismo among Latino families experiencing cancer.
The purpose of this study is to describe familismo’s role among Latino families affected by cancer from the perspectives of LCSs living in survivorship, family caregivers (FCs) of LCSs, and cancer care providers. Aligned with cultural humility, this study aims to learn from various stakeholders, uncover knowledge gaps, and provide suggestions for the profession to develop culturally tailored interventions (Agner, 2020). The study was conducted as part of a broader analysis of the experiences of LCSs (Ramirez et al., 2022).
Method
Design
We used a generic, cross-sectional qualitative design (Percy et al., 2015) with six-step reflexive thematic analysis (Braun & Clarke, 2022) informed by a social constructivist lens (Carter & Little, 2007). Generic qualitative research is a widely used approach to understand people’s subjective reflections on their experiences (Percy et al., 2015) and is thus ideally suited for understanding how familismo affects LCSs and their families. The University of Illinois at Chicago Institutional Review Board approved this study.
Participants
We recruited a purposive sample of diverse interest holders in long-term survivorship among Latino families, including LCSs, FCs, and cancer care providers. The purposeful inclusion of these diverse groups provided an opportunity to gain a more holistic understanding of cancer survivorship at the individual and family levels. Moreover, cancer care providers further broaden perspectives on the basis of the knowledge they have accrued from serving multiple individuals and families (Magasi et al., 2012). Including these three participant groups also provided the opportunity to triangulate perspectives across interest holders. All participants were at least age 18 yr. Latino/a was defined as a person having a Latin American background. Eligible cancer survivors self-identified as a LCS who had completed primary cancer treatment and received support from family during survivorship. FCs were eligible if they identified as a caregiver to a LCS. Providers were eligible if they had at least 1 yr experience working with LCSs. Individuals were excluded if they were unable to participate in a 2-hr data collection session.
Data Collection
Measures and Instruments
Interview guide.
Interview guides, informed by the Model of Human Occupation (Taylor et al., 2024) and conceptual and first-person understandings of Latino culture, were developed in English and Spanish. Spanish interview guides were pilot tested with a LCS and their FC, resulting in minor edits (see Tables A.1, A.2, and A.3 in the Supplemental Material for the interview guides, available online with this article at https://research.aota.org/ajot).
Short Acculturation Scale for Hispanics.
The Short Acculturation Scale for Hispanics (SASH) is a self-report measure of acculturation validated among Latina breast cancer survivors (Hamilton et al., 2009; Marín et al., 1987). Measured by the SASH, acculturation is the extent to which Latino/a participants adopt American cultural norms and practices. Acculturation has a complex relationship to health and health behaviors in Latino communities (Lara et al., 2005; Van Wieren et al., 2011). For example, higher levels of acculturation are associated with improved access to care, use of preventive health services, and self-perceived health, as well as with an erosion of health behaviors related to substance use and healthy eating (Lara et al., 2005). The SASH was administered as part of the demographic survey. SASH scores for each LCS and FC are reported descriptively with the intention of providing a thick description to characterize the sample (Ponterotto, 2015). Following recommendations by Marín et al. (1987), a mean SASH score of >2.99 was used as the cut-off score to represent high levels of acculturation. Understanding participants’ levels of acculturation can help contextualize their discussions of familismo.
Data collection sessions.
The first author, Ricardo D. Ramirez, gathered all data in person (except for one telephone-based provider interview) between January and March 2020. After providing informed consent, participants completed a demographic questionnaire. Individual semistructured interviews were conducted in the participant’s preferred language. Survivor and provider interviews lasted approximately 1 hr, and caregiver interviews lasted about 40 min. Survivors and caregivers received $25 for their contributions to the research. Interviews were audio-recorded and transcribed verbatim with identifiers removed, and Ramirez translated the Spanish interviews into English. Transcripts were uploaded to Atlas.ti for data management and analysis. Ramirez wrote field notes after each data collection session and maintained an audit trail to further promote dependability (Creswell & Miller, 2000).
Data Analysis
Data collection and analysis occurred in tandem. A six-phase reflexive thematic analysis process was used (Braun & Clarke, 2022). Interviews were transcribed manually by Ramirez, which afforded him the opportunity to become deeply familiar with the data. An iterative coding dictionary with clear working definitions of codes was developed, and data were then coded in Atlas.ti. Ramirez coded all data, and Susan Magasi coded a subset of the data (Creswell & Miller, 2000). A total of 71 codes and subcodes were initially identified. Emergent themes were tracked and quantified after each interview.
Consistent with Guest et al.’s (2020) method for monitoring saturation in the thematic analysis studies, we evaluated the continued emergence of new themes over time with the addition of new data collection sessions. On the basis of these processes, we determined that an acceptable saturation threshold was achieved after 18 interviews (8 LCSs, 5 FCs, and 5 cancer care providers). This exhaustive code list was refined by generating themes that synthesized the data into three substantive themes. Themes were reviewed and refined through nine iterative rounds of analysis. To enhance credibility, we engaged a social worker and an occupational therapist in a peer debriefing process; these providers were not participants in the study and had extensive experience in cancer care (Creswell & Miller, 2000). These experts confirmed the salience of the key findings and offered insights into their implications. A final set of salient themes was identified. Analytic decisions were meticulously documented in the iterative coding dictionary in which codes and themes were named and defined.
In the final stage of the thematic analysis process, we used Weaver-Hightower’s (2019) setup–quote–comment method for writing qualitative research. To comply with the COnsolidated criteria for REporting Qualitative research (Tong et al., 2007) in writing up the findings, we include descriptions of each theme along with illustrative quotations and discuss the study’s implications for cancer care and occupational therapy practice.
Results
Eighteen individuals participated in this study: 8 LCSs, 5 FCs, and 5 cancer care providers (see Tables 1–3, respectively). LCSs’ ages ranged from 29 to 58 yr, and time in survivorship ranged from 3 mo to 48 yr. Of the 8 LCSs, 7 were women with history of breast cancer. Six LCSs lived with their FC, and only 1 reported receiving occupational therapy services in acute care. FCs’ ages ranged from 28 to 73 yr. Of the 5 FCs, 3 were male. Five LCSs and 2 FCs identified as Mexican immigrants. Per their SASH scores, only 1 LCS and 1 FC had higher levels of acculturation, and all but three interviews were conducted in Spanish. Moreover, 2 occupational therapists and 3 social workers participated in the study, with the most seasoned provider having 10 yr of clinical experience working with LCSs.
Latino/a Cancer Survivor Demographics
Note. SASH = Short Acculturation Scale for Hispanics.
Family Caregiver Demographics
Note. SASH = Short Acculturation Scale for Hispanics.
Provider Demographics
Note. LCSs = Latino/a cancer survivors.
LCS, FC, and cancer care provider perspectives on familismo were captured in three themes: (1) multilevel support, (2) present yet distant, and (3) unmet expectations.
Multilevel Support
Using familismo as a guiding cultural value, all participants emphasized the culture of interdependence that was crafted by not only immediate family members but also extended family and community members.
Immediate Family
All LCSs experienced long-term effects of cancer and its treatment, and FCs problem-solved ways to support their occupational needs, especially activities of daily living (ADLs). Survivors deeply appreciated the support they received. For example, Rosa, a breast cancer survivor, described when decreased upper extremity range of motion and lymphedema made ADLs challenging: My shirts are too tight and he [husband] helps me lift my arm and helps me put on my shirt. My daughter helped me put lotion on my back. . . . I thank God that I have a daughter that has helped me out significantly.
Most caregivers willingly adopted new responsibilities, especially instrumental activities of daily living (IADLs), when survivors were unable to meet role demands. Caregivers embraced the opportunity to contribute to their family’s well-being: “Because of her cancer situation, she can’t lift stuff. Washing and doing chores around the house that she can’t do, that kind of stepping up . . . it doesn’t really bother me because I’m doing it for a good cause” (Gabriela, Rosa’s daughter).
Caregivers were attuned to survivors’ mental health. Recognizing the importance of everyday participation, FCs encouraged survivors to engage in meaningful occupations, such as volunteering and community exploration: My husband always says, “You can do it. Don’t say that you can’t because you can . . . My son [says,] “Let’s go out to the streets to not be here!” He is the one who is my chauffeur. I always say that my Uber has arrived! [laughs] . . . They try to uplift my spirit in going out, in making me laugh. (Maria, breast cancer survivor)
Survivors were not passive recipients of supports. Rather, they valued contributing to the family unit. These synergies were inherent in caregiving relationships: “If they [parents] have to go grocery shopping . . . I have to go with them because they can’t be carrying stuff because they’re a bit older. . . . It’s a combination of us helping each other” (Carmen, breast cancer survivor).
Extended Family
Extended family (such as cousins, aunts, uncles, in-laws) and social relations (such as compadres and family friends) supported survivors and caregivers. Survivors were pleasantly surprised by the diversity of support they received during treatment, especially because many LCSs were the first in their immediate family to be diagnosed with cancer. Dormant relationships were reignited: After finishing treatment, [my comadre] helped me out so much. . . . A lot of people talked to me that I hadn’t talked to in years . . . anytime that I had a question, she was there to answer. [She was] huge in my healing process. (Jessica, lymphoma survivor)
Small gestures incorporating psychosocial support often meant a great deal: “When family and friends come over and talk to us . . . that helps tremendously—that support that they provide to me” (Jesus, Jessica’s father).
Providers expressed confidence in Latino immediate and extended families’ ability to meet the challenges required to manage a cancer diagnosis: I rarely see one of our Latinx patients come alone. They’re often with a loved one, a family member, with a friend or with multiple people. . . . The celebration of family is so beautiful to me . . . it’s very different from my own culture. (SW2)
Although providers acknowledged the support people received from extended family as a result of familismo, they did not fully grasp how integral these extended support networks were for LCSs.
Community
The importance of familismo was also evident as community members—such as neighbors and support group members—provided support ranging from small acts such as daily check-ins to larger actions such as ADL and IADL assistance. These acts of kindness were meaningful to LCSs. Survivors recognized that their upbringing instilled in them a dedication to community because familismo emphasizes reciprocity: “For any little thing, my neighbors help me out . . . that’s what my parents taught me: if someone helps you of free will, then you should also return the favor to other people” (Silvia, breast cancer survivor).
With firsthand knowledge and experience with familismo, Latina providers also shared their experiences with rapport building in their encounters with LCSs and recognized it as a way to build trust. For example, SW1 said that “people connect as if I’m a family member. . . . It allows them to be more open and honest. . . . Instead of talking to a professional, they’re talking to a family member.” Acknowledging the role of reciprocity in familismo, providers would selectively disclose personal information about themselves to foster a sense of connection with LCSs.
Present Yet Distant
Although all participants considered familismo a strength, LCSs and FCs emphasized that their family dynamics had unspoken complexities. When the cultural expectations of dedication, respect, and support were not met, families experienced distress and relationship strain. Thus, although familismo united Latino families, it also simultaneously caused some to feel disconnected and disappointed.
Unknowingly Unsupportive
LCSs expressed that their families did not fully recognize how cancer altered their daily life. This lack of recognition was interpreted as being unsupportive and inconsiderate. For example, Jessica expressed frustration that her family did not understand her cancer-related fatigue. Survivors were burdened with the responsibility of advocating to their family members about their symptoms. This distressed survivors and divided tight family units: “My parents didn’t understand what happens after chemo. . . . There have been times where I’ve told them [family] that I’m really tired and they’re like, ‘I just did a 10-hr shift, I’m tired.’ They belittle me!” (Jessica, lymphoma survivor).
In contrast, FCs believed they were being attentive to their loved one’s needs, especially when survivors resumed many of their precancer roles. Jessica’s father reflected on his daughter’s functioning: “Even though she went through this difficult treatment, she never stopped working . . . she always put forth her best effort. . . . She hasn’t told us that she has felt bad” (Jesus, Jessica’s father).
Prioritizing Family Needs
Survivors recognized the toll that their cancer had on their family members. Consequently, survivors tried to prioritize their family’s needs as they selectively withheld portions of their cancer experiences, forcing them to deal with this adjustment alone. “My husband calls me from work, ‘How are you doing?’ ‘I’m okay’ . . . He says, ‘What’s wrong?’ . . . I don’t want them to worry about other stuff that they don’t need to be worried about” (Beatriz, breast cancer survivor).
LCSs upheld the collectivistic essence of familismo, often resulting in a variety of psychosocial concerns. Indeed, this complex interaction among familismo, functional impairments, and role participation was discussed by many of the participants and is succinctly described in the following quotation: When someone is pronounced “cured,” then [the] expectation is that everything goes on the way it was before and you shouldn’t have any more issues. [Survivors think that] as a mother, there are cultural expectations. The family was more than happy to step in during treatment, but now that you are cured and done with treatment, why are you not resuming that role as it looked before? I think the cultural expectations can be suspended during the treatment itself but then they return without sort of accounting for what has changed, both physically, emotionally, mentally afterwards. . . . It weighs very heavily on them. I think they feel a lot of guilt. They’re dealing with their own sadness, anxiety about having had cancer but then they feel guilty. . . . Their family did help them and now they want to return the favor. . . . I think they place huge expectations on themselves that not everyone does in other cultures to repay what the family did to support them during that time. (SW3)
Survivors also worried about their caregiver’s mental health and did not feel comfortable asking them about their own well-being. Survivors worried this would exacerbate an already fraught situation: “She [niece] comes out of working here with me and then goes to work. . . . I notice in her face that she is worried about me. . . . I don’t have the courage to ask her” (Eduardo, melanoma survivor).
Similarly, caregivers prioritized their loved one’s needs over their own and often masked their emotions: “It does make me feel down. . . . I shouldn’t show that to her. I should show her a positive attitude. . . . It is heartbreaking to see her . . . knowing that she was so active before” (Gabriela, Rosa’s daughter).
Unmet Expectations
Although family dynamics varied across participants, families expressed disappointment when expectations of connectedness and interdependence from familismo were not met.
Survivor Perspectives
Given familismo’s emphasis on mutual support, survivors were shocked when their relationships were not as reciprocal as they thought they were. Years into survivorship, survivors continued to feel devalued: They [brothers] would rather not come because they don’t want to see me helpless. If they see me sitting down and see that I’m aching about something, they will rather get up and go, because they don’t want to ask me, “Are you okay?” (Carmen, breast cancer survivor)
Survivors who were immigrants also experienced the absence of extended family members who lived in their home country. Some survivors experienced heightened social isolation: “[I feel] sad that it’s just me that is here. My parents are in Mexico. . . . Everyone is busy. My mother too; I would call but she would end the conversation and she would tell me she was very busy” (Silvia, breast cancer survivor).
Caregiver Perspectives
FCs also experienced disappointment when their extended family members did not assemble to provide support. Instead of dwelling on this absence, they concentrated on their immediate families’ support. Many caregivers found strength during treatment in their own families’ capacity to support one another. Juan, Maria’s husband, mentioned, “No one [supported us during my wife’s cancer treatment] . . . like support from [extended] family, no. Better us [immediate family] . . . we were there for her.”
Whether found in expansive networks or tight family units or mourned in its absence, familismo was a core value that shaped the experiences of LCSs and their families.
Discussion
This study examined the role of familismo for Latino families affected by cancer, adding to the emerging occupational therapy literature centered on this group. With recognition of how cultural values contribute to cancer outcomes for Latinos (Yanez et al., 2016), this study sheds light on the nuanced ways in which familismo affects LCSs and their FCs. As the profession moves toward upholding cultural humility and amplifying the voices of people from racially minoritized backgrounds (Agner, 2020; Johnson et al., 2024), it is imperative to recognize how the heterogeneous experiences of LCSs and their families are shaped by multifaceted cultural values such as familismo.
Overall, we found that whether familismo was found in expansive networks or tight family units or mourned in its absence, it was a core value that shaped the experiences of LCSs and their families. Familismo embraces family loyalty and support while emphasizing interdependence among biological and chosen family. In this study, this was evident because reciprocal caregiving relationships were the foundation of immediate family units; the support strengthened the family and people collaborated for individual and collective benefit. Moreover, all LCSs and FCs underscored the broad levels of physical and emotional support they received throughout their cancer journey. This finding corroborates existing literature about familismo as a protective factor among Latino families affected by cancer (Ashing-Giwa et al., 2006; Carrion et al., 2017). Given the significant role familismo may play, Western occupational therapy practice—which often prioritizes independence—should consider facilitating interdependence among their Latino/a clients (Collins, 2017).
In this study, all providers identified familismo as a strength. Higher provider cultural sensitivity plays a pivotal role in patient satisfaction among Latinos (Roncoroni et al., 2022). Because cultural humility acknowledges that all humans have implicit biases, it is important to recognize that non-Latino health care providers may view cultural values such as familismo as barriers to treatment (Moreno et al., 2023). With 4.5% of occupational therapy practitioners being Latino (American Occupational Therapy Association, 2024), it is important for the profession to not only learn more about Latino cultural values but to also diversify the workforce with more Latinos in service of promoting health equity in oncology practice (Kronenfeld et al., 2021).
Given the prioritization and importance of the tight family unit, it is also necessary to understand familismo’s complexities because both survivors and FCs often dealt with psychosocial challenges related to cancer by themselves. Several LCSs felt unsupported when their family did not understand the impact cancer had on them during survivorship. Yet, survivors’ reticence to trouble their caregivers with the realities of their experiences may have unintentionally kept their loved ones in the dark, thereby creating a vicious cycle of unexpressed needs and inadequate support. Conversely, when their own mental health was affected, FCs masked their emotions (Cordova-Marks et al., 2023). The irony of the desire to prioritize the other’s needs is that neither party feels fully heard or supported. Therefore, frank discussions and open communication among families are needed to help identify unmet needs (Yu & Sherman, 2015).
Familismo is also grounded in feelings of loyalty, mutual respect, and obligation. Participants expressed disappointment when their families’ actions did not reflect the level of reciprocity they associated with familismo. By applying cultural humility, occupational therapy practitioners should thus avoid making assumptions regarding family dynamics among Latino families and instead carefully evaluate the social environment when working with this group.
As a prerequisite to implementing these findings in practice, survivors must have access to occupational therapy services. Only 1 LCS reported receiving occupational therapy services. Occupational therapy has great potential to work with underserved cancer survivors such as LCSs, but access to services is paramount. Ongoing efforts to address the social determinants of health in cancer rehabilitation are needed (Gupta et al., 2023).
Limitations
This study has several limitations. The primary limitation is that most participants were female breast cancer survivors. Moreover, data collection occurred during a time of amplified anti-immigrant rhetoric, potentially resulting in undocumented individuals being less likely to participate. Although acculturation data were collected, most survivors and caregivers had lower levels of acculturation. Future studies should strive for a more diverse sample of LCSs based on cancer type, immigration statuses, and acculturation levels.
Implications for Occupational Therapy Practice
As occupational therapy continues to embed itself into routine cancer care (Braveman & Newman, 2020), occupational therapy practitioners can facilitate strengths-based practices for Latinos affected by cancer through the provision of culturally tailored care (Figure 1). Findings from this study have the following implications for occupational therapy practice with LCSs: ▪ Acknowledging the heterogeneous experiences of Latino families affected by cancer, practitioners should embrace cultural humility to avoid making assumptions, understand family dynamics, and learn about Latino cultural values such as familismo. ▪ Framing familismo as a strength, practitioners can actively include biological and chosen family members throughout the occupational therapy process to ensure families have the necessary information to support one another. Given the unspoken complexities of family dynamics, open and honest communication among the whole family should be emphasized throughout the cancer care continuum, especially survivorship. ▪ Using their holistic scope of practice, practitioners can screen and address mental health concerns among both survivors and family caregivers. ▪ Recognizing the influence of familismo, practitioners should adapt existing evidence-based occupational therapy interventions for LCSs that infuse cultural values (Costas-Muniz et al., 2023), and occupational therapy researchers can develop novel ones that are rooted in Latino cultural values (Casillas et al., 2021). ▪ To further understanding of Latino cultural values, the profession can increase its involvement with the Latino community by recruiting Latino practitioners and partnering with community-based organizations to cocreate culturally tailored services (Kronenfeld et al., 2021).
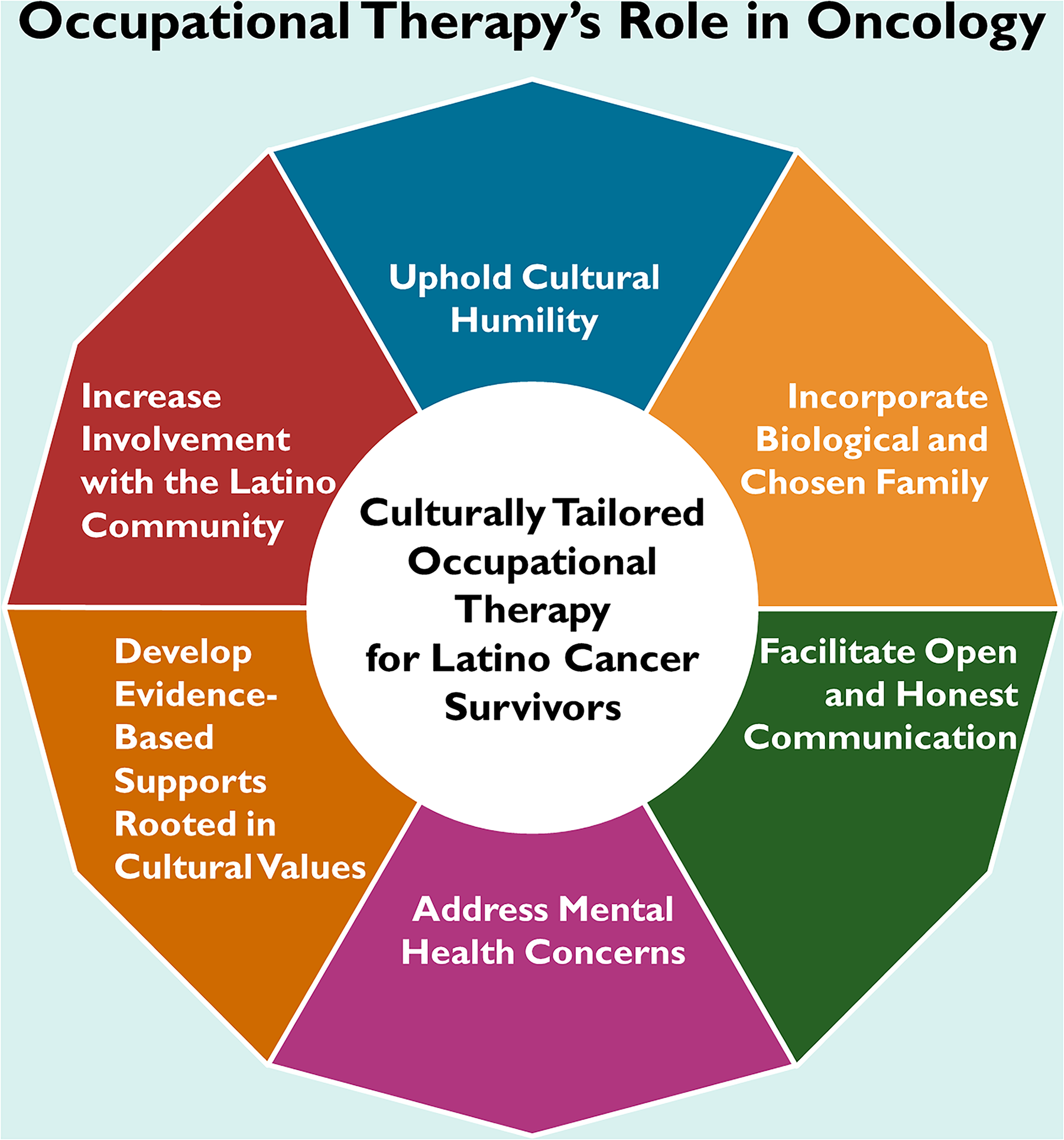
Schematic depicting recommendations for culturally tailored occupational therapy for LCSs within the context of occupational therapy’s role in oncology
Conclusion
Familismo influences Latino families affected by cancer in myriad ways. This study calls for familismo and other cultural values to be carefully examined throughout the occupational therapy process and the cancer care continuum. To thoughtfully do this and work toward remediating cancer health disparities, it is essential to implement culturally tailored care for Latino families affected by cancer that acknowledges the impact of familismo. This work must be at the forefront as occupational therapy continues to communicate its distinct value to diverse communities and within oncology practice. As the profession continues advancing diversity, equity, and inclusion, it must continuously seek to understand the cultural values held by diverse communities so that they can be leveraged as strengths.
Supplemental Material
Supplementary material for Role of Familismo in Latino Families Affected by Cancer: Implications for Culturally Tailored Occupational Therapy Services
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050937.pdf for Role of Familismo in Latino Families Affected by Cancer: Implications for Culturally Tailored Occupational Therapy Services by Ricardo D. Ramirez and Susan Magasi in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We sincerely thank all of our participants—with special appreciation to the Latino families—for sharing their invaluable knowledge and experiences with us.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.