
Abstract
This review summarizes 43 articles on the effectiveness of occupational therapy telehealth interventions for all ages and populations from 2019 to 2022.
The delivery of telehealth (i.e., telemedicine) services has expanded exponentially in recent years (World Health Organization [WHO], 2022). Because of advances in technology and innovation that stemmed from the COVID-19 pandemic, occupational therapy practitioners are using telehealth today more than ever before. The American Occupational Therapy Association (AOTA; 2018) has determined that the delivery of telehealth occupational therapy services is appropriate and effective when mutually agreed upon by both client and provider. Furthermore, telehealth may improve access to services. Evidence of telehealth interventions’ effectiveness within the scope of occupational therapy practice has emerged (Feldhacker et al., 2022).
The AOTA (2018) position paper “Telehealth in Occupational Therapy” referred to telehealth as an “emerging model of health care delivery” (p. 1). In 2018, telehealth was a developing tool, available to practitioners seeking a means to deliver occupational therapy services at a distance from the care recipient. Since 2018, the use of telehealth has expanded dramatically, and although no longer considered innovative, its use has improved how practitioners are accessing and providing services to individuals, groups, and populations.
Despite increased knowledge of benefits and new telehealth approaches, variations remain between state regulations, payer sources, and health systems regarding how telehealth is used in occupational therapy practice. AOTA has published resources, including a telehealth decision guide (AOTA, 2020c) that advises practitioners to review guidelines in both their practice state and their client’s state, evaluate facility policies, and identify requirements set by the payer. Because of these factors, uncertainty remains regarding the delivery of and reimbursement for occupational therapy delivered via telehealth. Hence, additional research demonstrating the outcomes of telehealth services is urgently needed. Because telehealth increases client satisfaction, assists in the reduction of health care costs, and increases the availability of services to clients in rural and medically underserved areas (Cottrell et al., 2021; Harkey et al., 2020), research exploring occupational therapy telehealth outcomes can help lead to important changes in policies and practice.
A systematic review by Feldhacker et al. (2022) reported that interventions provided via telehealth for clients with neurological and pain conditions resulted in strong strength of evidence. However, based on low strength of evidence, interventions for clients with developmental disorders or other medical conditions were only supported on a case-by-case basis. In addition, although there was some literature available exploring telehealth with children receiving occupational therapy in a school system, the articles that were included described barriers affecting the quality of these interventions.
Because Feldhacker et al.’s (2022) review included a wide variety of outcomes, based on the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; AOTA, 2014), some outcomes were more supported in the literature than others. Furthermore, the fourth edition of the OTPF has been released (OTPF-4; AOTA, 2020b). As such, it was determined that more research was warranted specifically focusing on occupation-centered outcomes using telehealth. Finally, the 2022 review was conducted on a review of available evidence from 2009 to 2019. Given an influx in telehealth intervention and research that has occurred because of the COVID-19 pandemic, it was determined that an updated systematic review, spanning articles published during the 2019–2022 timeframe, was warranted. For example, the U.S. Government Accountability Office (2022) reported that Medicare telehealth services rose dramatically from 5 million in April to December 2019 to 53 million in the same period in 2020. For these reasons, we conducted a systematic review to examine the research question, “What is the effectiveness of occupational therapy interventions, when provided using telehealth as the mode of service delivery, for occupation-centered outcomes?”
Method
Search Strategy
The Cochrane methodology (Higgins et al., 2016) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews (Page et al., 2021) provided a framework for the present review. A health science librarian and Whitney Lucas Molitor, Diana Feldhacker, Zhaoying Li, and Vanessa Jewell developed the search terms (Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot) through an iterative process using the OTPF–4 (AOTA, 2020b) to identify and describe the occupational therapy scope of practice. The databases searched were PubMed, CINAHL, PsycINFO, and Cochrane Database of Systematic Reviews. This review was not registered.
Eligibility Criteria
The review included articles that met the following criteria: written in English, peer-reviewed, published from 2019 to 2022, and classified as evidence Level 1b, 2b, or 3b. Research needed to include interventions delivered via telehealth by an occupational therapy practitioner, either as part of an interprofessional team or as a sole provider, and outcomes that were within the occupational therapy scope of practice. We defined occupation-centered outcomes as those outlined in the OTPF–4 (AOTA, 2020b). The Oxford Centre for Evidence-Based Medicine (2009) guidelines provided the evidence hierarchy used to determine the level of evidence. Systematic reviews or meta-analyses (Levels 1a, 2a, and 3a) were kept for hand-searching purposes only and were excluded from the review to avoid duplication of data and errors that may occur from multiple secondary interpretations. Exclusion criteria included conference proceedings, presentations, abstracts, non-peer-reviewed articles, levels of evidence 4 or 5, dissertations, white papers, psychometric studies, and articles that were included in a previous systematic review (Feldhacker et al., 2022) to prevent duplication. Further definitions of the criteria are in Table A.2 in the Supplemental Material.
Procedure and Data Extraction
Li, Jewell, and a health science librarian completed the database searches, organized the search results, and conducted hand searching of systematic reviews and prominent authors publishing on telehealth in applicable journals. Selected articles from hand searching were added to the database search results and screened using the same process. Covidence (https://www.covidence.org) was used to manage and organize the search results as well as to easily identify and remove duplicative articles. We developed a checklist to assist with article screening that outlined review criteria (see Table A.2 in the Supplemental Material). Two authors were assigned to independently screen each article by title and abstract. Each author independently categorized articles as “yes,” “no,” or “maybe” in Covidence, and comparisons of agreement between reviewers were made within the web-based software tool. As a team, we reviewed any articles not agreed upon by the two reviewers and determined inclusion based on group consensus.
Li uploaded the full text of articles categorized as “yes” and “maybe” into Covidence for a full-text review. This full-text review step mirrored the title and abstract screening process, in which two authors were randomly assigned to independently review and determine whether the article met the inclusion criteria (see Figure 1 for the flow diagram). Articles that met inclusion were then divided among four authors for data extraction into an evidence table (see Table A.3 in the Supplemental Material). We used an online shared file that allowed us to track the progress of the team and review for consistency. We evaluated the risk of bias based on the research design of the studies (Tables A.4 and A.5; Higgins et al., 2016; National Heart, Lung, and Blood Institute, 2014). All studies were assessed for risk of bias by one author and reviewed for accuracy by a second author to reach a final determination, with all authors participating in this assessment.
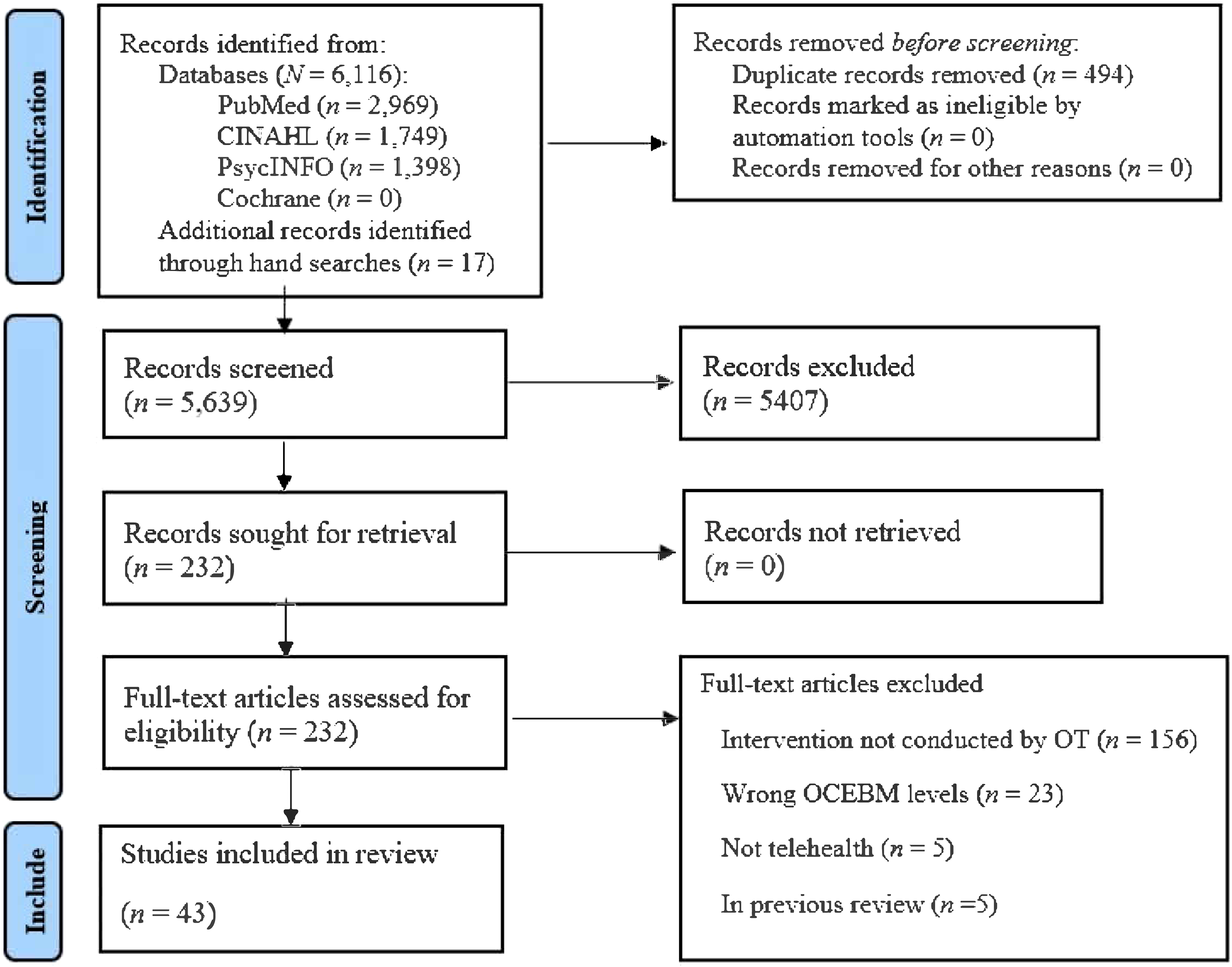
Flow of article inclusion and exclusion for the systematic review.
If the risk of bias level was uncertain between Level 1b or Level 2b, we looked for justification for the sample size (e.g., a priori power analysis or similar) to inform our decision. Where relevant, client-factor outcomes related to the occupation-centered outcomes were also reported. For example, Hesseldal et al. (2022) investigated occupation-centered outcomes for quality of life, and related psychosocial function outcomes were also collected.
Once data extraction and assessment for bias were completed, we analyzed the data based on the populations receiving telehealth intervention, the type of intervention, delivery setting, and outcomes. We sorted and grouped the articles into themes agreed upon by all authors during a team meeting.
Analysis
We used guidelines recommended by AOTA (2020a) and based on the U.S. Preventive Services Task Force (2018) to analyze each theme for the strength of evidence by using information from the study design, research findings, and risk of bias to make determinations. The strength of evidence was rated according to the following criteria: ▪ Strong: Two or more Level 1a or 1b studies reporting consistent results. The studies are well designed and conducted, so their results are not likely to be questioned by future research. ▪ Moderate: A minimum of one high-quality Level 1a or 1b study or several studies (Level 2a or 2b, Level 3a or 3b) that are moderate quality. The evidence is sufficient to determine health outcomes, although studies may include concerns with the number, size, or quality or there may be inconsistency in the findings. ▪ Low: A small number of low-level research resulting in insufficient evidence to assess effects on health outcomes. There may be a limited number of studies identified, flaws in the design or methods, or inconsistent findings.
Results
The initial database searches yielded 9,417 results. Application of filters for reviews, systematic reviews, and meta-analyses yielded 6,116 abstracts. We used Endnote and Covidence to remove duplicates, resulting in 5,639 abstracts. After screening, 43 articles met the criteria to be included in this review (see Figure 1) and were summarized by theme and level of evidence (see Table A.3 in the Supplemental Material). The evidence table (Table A.3) was sorted into themes based on health conditions and includes study design, risk of bias, participants, study setting, intervention and control groups, outcome measures, and study findings. Interventions included both interprofessional approaches and those delivered solely by occupational therapy practitioners. The risk-of-bias tables for controlled and noncontrolled trials are in Tables A.4 and A.5 in the Supplemental Material. Table A.6 highlights the distinctions by theme and level of evidence.
Chronic Conditions
Eleven studies explored telehealth interventions for individuals with chronic conditions. Articles were further categorized into four subthemes based on the type of intervention: lifestyle and nutrition (n = 4), chronic pain management (n = 3), care partner involvement (n = 3), and cancer-related cognitive interventions (n = 1).
Lifestyle and Nutrition Interventions
Four articles (Hesseldal et al., 2022; K. Lim et al., 2021; Lozano-Lozano et al., 2020; Schepens Niemiec et al., 2021) described telehealth interventions focused on lifestyle and nutrition for participants diagnosed with obesity, diabetes mellitus, or cancer. These articles were classified as Level 1b evidence (Hesseldal et al., 2022; K. Lim et al., 2021; Lozano-Lozano et al., 2020) and Level 3b evidence (Schepens Niemiec et al., 2021).
Three studies (Hesseldal et al., 2022; K. Lim et al., 2021; Schepens Niemiec et al., 2021) described interprofessional team interventions, with occupational therapy practitioners supporting lifestyle changes during initial sessions and 4- to 6-mo follow-up sessions. Occupational therapists, nurses, dieticians, and physiotherapists, trained in digital health coaching and with 2 yr of experience, delivered interprofessional digital lifestyle coaching focused on lifestyle and habits (Hesseldal et al., 2022). K. Lim et al. (2021) studied occupational therapists, dieticians, and physiotherapists health coaching interactions and monitoring of participant-logged data on daily habits related to nutrition, weight, and physical activity, collected via electronic applications. Finally, occupational therapists partnered with community health workers and provided healthy eating and health navigation education via telehealth (Schepens Niemiec et al., 2021). One study described an occupational therapy intervention as the sole provider for an 8-wk lifestyle intervention in which the occupational therapists provided the intervention in a group format using an electronic application for recording lifestyle habits (Lozano-Lozano et al., 2020).
Outcomes across studies included quality of life, occupational performance and satisfaction, and psychosocial function. Several of the studies measured a variety of health indicators, which we included as health management outcomes (e.g., weight, glycated hemoglobin [HbA1c], blood pressure) that practitioners may focus on as part of health management intervention, in addition to occupational performance measures. We determined that outcomes related to laboratory values, weight, or body composition were relevant to health management interventions, but we only included studies that paired these outcomes with functional findings related to occupation.
Results from the four studies showed that telehealth interventions provided by occupational therapy practitioners improved lifestyle and nutrition outcomes for participants with chronic conditions. Three of the four study designs included a control group, and these studies found statistically significant improvements to support the use of telehealth compared with usual or standard care. K. Lim et al. (2021) reported statistically significant improvements in outcomes of health management (i.e., nutritional intake, self-efficacy) for telehealth interventions, as compared with the control group. Hesseldal et al. (2022) also reported a statistically significant reduction in health management outcomes (i.e., weight, HbA1c). Although both groups showed improvement, the telehealth group had more significant gains in the study outcomes than did participants in the control group who received usual care without telehealth-delivered lifestyle coaching. Lozano-Lozano et al. (2020) conducted research in which both groups received telehealth as an augment to rehabilitation or usual care interventions, and they found improved outcomes for both groups. However, the mHealth and rehabilitation group had statistically significant improvements compared with the mHealth and usual care group for global quality of life, global health, upper extremity function, and active range of motion. The rehabilitation group reported statistically significant improvements over the control group, although both groups received telehealth.
There is strong strength of evidence to support telehealth interventions for individuals with chronic conditions for nutrition-focused health behaviors (Hesseldal et al., 2022; K. Lim et al., 2021). There is moderate strength of evidence to support lifestyle-based telehealth-delivered intervention for upper extremity function (Lozano-Lozano et al., 2020) and improvements in health outcomes including blood pressure (Hesseldal et al., 2022; Schepens Niemiec et al., 2021). Because of mixed results or study design, there is low strength of evidence to support outcomes of health indicators (i.e., weight, BMI, HbA1c), sleep, and psychosocial function.
Chronic Pain Management Interventions
Three articles focused on chronic pain management through the implementation of Reboot, a multidisciplinary, 16-wk internet-delivered cognitive–behavioral therapy, and physical activity intervention (D. Z. Lim et al., 2021, Level 3b; Shiner et al., 2022, Level 3b; Smith et al., 2019, Level 2b). Two studies used a retrospective cohort design (Shiner et al., 2022; Smith et al., 2019), and one study used a randomized controlled trial (RCT) design (Smith et al., 2019). All studies had a low risk of bias. The occupational therapy–specific component included an expert educational video on using activity for pain management.
The telehealth intervention significantly reduced pain across all studies. In addition, Smith et al. (2019) found that the intervention significantly increased pain self-efficacy compared with usual care, with benefits lasting at the 3-mo follow-up. Evidence from one Level 2b and two Level 3b studies with low risk of bias suggests moderate strength of evidence for the use of telehealth for interprofessional interventions for chronic pain management, including the integration of occupational therapy services.
Care Partner Involvement Interventions
Three articles included care partners of individuals living with dementia (Laver et al., 2020, Level 1b), juvenile idiopathic arthritis (Mulligan et al., 2022, Level 1b), and unspecified adult general chronic conditions (Serwe & Walmsley, 2020, Level 3b). Telehealth interventions included synchronous videoconferencing with an occupational therapist, focusing on problem- solving, education, and skills building (Laver et al., 2020; Serwe & Walmsley, 2020) and an interprofessional educational website codeveloped with an occupational therapist (Mulligan et al., 2022). Control groups received usual on-site clinical care (Mulligan et al., 2022) or in-home therapy (Laver et al., 2020).
In Laver et al.’s (2020) study, both groups reported significant improvements in perceived change in caregiver well-being, indicating the telehealth delivery of the occupational therapy intervention was comparable with traditional face-to-face delivery. Likewise, Mulligan et al. (2022) reported significant improvements in parenting stress compared with usual care for an interprofessional telehealth intervention. This is inconsistent with the results of Serwe and Walmsley (2020), which indicated improvement in depression but not in caregiver well-being for an interprofessional intervention. Overall, although there is some inconsistency, the higher quality studies indicated moderate strength of evidence to support the use of telehealth interventions through 1:1 sessions or an educational website for outcomes of caregiver well-being.
Cancer-Related Cognitive Interventions
Maeir et al. (2021, Level 3b) studied individuals experiencing mild cognitive decline secondary to cancer or cancer-related treatment. In this feasibility study, occupational therapy interventions were delivered via telehealth to six participants in a single-group, nonrandomized design. The authors used computerized training (BrainHQ) via remote sessions using an occupation-based approach to address cognition, quality of life, and occupational performance. Findings indicated statistically significant improvements in occupational performance and satisfaction and in social quality of life. Because of the study design, there is insufficient evidence for the use of occupational therapy–delivered telehealth intervention for the outcomes of cognition and occupational performance for individuals with cancer-related cognitive decline.
Effects of COVID-19 Isolation
Two Level 2b studies with low risk of bias (Belhan Çelik et al., 2022; Pekçetin & Günal, 2021) studied telehealth interventions with adolescents and young adults. Belhan Çelik et al. (2022) conducted an RCT examining the effects of online group occupational therapy during the COVID-19 lockdown on occupational balance, well-being, and quality of life. Similarly, Pekçetin and Günal (2021) studied the effects of a web-based, occupational therapist–designed telehealth intervention focused on time use on occupational balance during the pandemic. Both studies supported the use of telehealth intervention to promote occupational balance and quality of life. Whereas the control group in the Pekçetin and Günal (2021) study improved on some quality-of-life measures, the intervention groups from both studies resulted in statistically significant improvements compared with the controls. There is moderate strength of evidence for the use of occupational therapy telehealth interventions for adolescents and young adults experiencing changes in routine, as was the case during COVID-19 lockdowns, to address time use and occupational balance.
Developmental Disorders
Two studies included participants with a developmental disorder, including one Level 2b (Jamali et al., 2022) and one Level 1b (Parsons et al., 2019) study, both with a moderate risk of bias. Jamali et al. (2022) delivered occupational performance coaching twice a week via videoconference to caregiver–child dyads to promote occupational performance, quality of life, and health management. Parsons et al. (2019) used tablets to supplement existing therapy for children and caregivers, addressing visual–motor skills, socialization, social interaction, and play provided by psychologists and occupational therapists. Although both studies indicated positive effects of telehealth interventions compared with the control groups, the control groups also showed positive outcomes for some measures. For example, although improvement in performance and satisfaction scores of the Canadian Occupational Performance Measure were statistically significant for telehealth intervention participants, quality of life and health management outcomes did not differ between groups (Jamali et al., 2022). Similarly, Parsons et al. (2019) reported that cognitive outcomes were significantly improved for those in the telehealth intervention, whereas other outcomes were similar between groups. Therefore, there is moderate strength of evidence to support telehealth when delivered to child–caregiver dyads with developmental disorders for the outcomes of occupational performance and satisfaction and of cognition (expressive language).
Musculoskeletal Conditions
Ten studies examining telehealth interventions for musculoskeletal conditions were included in this review, nine with adults and one with children. These studies were further categorized on the basis of whether the musculoskeletal condition affected upper or lower body function.
Musculoskeletal Conditions Affecting Upper Body Function
Five studies included participants with musculoskeletal conditions affecting upper body function (Blanquero et al., 2019, Level 2b; Blanquero et al., 2020, Level 2b; Gagnon et al., 2021, Level 3b; İnal & Tunçer, 2022, Level 2b; Murphy et al., 2021, Level 2b). These conditions included carpal tunnel syndrome; bone and soft tissue injuries of the wrist, hand, or fingers; multiple congenital contractures; and lateral epicondylitis.
Significant findings were related to upper extremity function, return to work, grip and pinch strength, and pain. In two studies, app or web-based exercise programs, developed by an interprofessional team that included occupational therapists, were compared with paper-based exercise programs (Blanquero et al., 2019, 2020). Findings showed that the telehealth delivery expedited return to work and enhanced short-term functional recovery and pinch strength for individuals with wrist, hand, or finger bone and soft-tissue injuries. In addition, İnal and Tunçer (2022) found that occupational therapy–led telephone-based follow-ups for individuals with lateral epicondylitis were more effective in reducing pain and increasing upper extremity function and joint protection than home-based methods. Telehealth interventions were more effective than typical or control interventions in all but one study. Gagnon et al. (2021) used a telehealth home exercise program delivered by occupational and physical therapists for congenital contractures but did not find significant improvements in pain or occupational performance. There is moderate strength of evidence to support upper extremity function outcomes and insufficient strength of evidence for pain for musculoskeletal telehealth interventions.
Musculoskeletal Conditions Affecting Lower Body Function
Five studies included participants with musculoskeletal conditions that affected their lower body function (C. T. Li et al., 2022, Level 2b; Ortiz-Piña et al., 2021, Level 1b; Tao et al., 2022, Level 1b; Torpil & Kaya, 2022a, Level 2b; Torpil & Kaya 2022b, Level 2b). Participants receiving telehealth intervention included those diagnosed with hip fracture, lower limb amputation, and total knee replacement.
Ortiz-Piña et al. (2021) found that interprofessional telehealth, including occupational therapy, resulted in significant improvements in self-care scores for older adults with hip fracture compared with home-based usual postoperative care. Similarly, C. T. Li et al. (2022) found significant improvements in instrumental activity of daily living (IADL) performance with occupational therapy telehealth. Torpil and Kaya (2022a, 2022b) found comparable improvements in quality of life and occupational performance and satisfaction following occupational therapy telehealth interventions after total knee arthroplasty. Ortiz-Piña et al. (2021) and Tao et al. (2022) used interprofessional telehealth interventions and found improvements in functional mobility and balance. Similarly, C. T. Li et al. (2022) and Torpil and Kaya (2022b) found significant improvements in functional mobility, ADL or IADL performance, health management, occupational performance, and quality of life when comparing telehealth intervention groups with control groups.
There is moderate strength of evidence for telehealth occupational therapy interventions provided to people with musculoskeletal conditions affecting lower body function for the outcomes of ADL performance, quality of life, and perceived occupational performance and satisfaction, although one study noted improvements for participants from both telehealth and nontelehealth interventions (Torpil & Kaya, 2022a). There is low strength of evidence for outcomes of IADL performance and balance confidence because of the small number of studies.
Neurological Conditions
Seventeen studies included individuals with neurological conditions. Subthemes included progressive neurological conditions (n = 5), spinal cord injury (n = 2), and brain injury (n = 10).
Progressive Neurological Conditions
Five studies included adult and older adult participants with progressive neurological conditions, including Parkinson’s disease (Anghelescu, 2022, Level 3b; Hashemi et al., 2022, Level 1b; Kim et al., 2021, Level 3b; Voola & Hema, 2020, Level 2b) and multiple sclerosis (Plow et al., 2019, Level 1b). Telehealth approaches included remote monitoring, live videoconferencing, and telephone conferencing either with an occupational therapy practitioner as the sole provider or with occupational and physical therapy practitioners. The interventions were varied and are outlined in Table A.3 in the Supplemental Material.
Telehealth intervention groups showed significant improvements in social well-being, occupational performance, fatigue management, and leisure-time exercise. Four studies reported statistically significant improvements in at least one outcome for individuals with Parkinson’s disease in the telehealth intervention groups. Hashemi et al. (2022) found statistically significant improvements for both face-to-face and remote-monitored virtual reality interventions for outcomes of sensory function and upper extremity movement functions. Voola and Hema (2020) reported improvements in functional movement and quality of life. Anghelescu (2022) and Kim et al. (2021) found significant improvements in functional mobility and balance. Kim et al. (2021) also noted significant improvements in quality of life and psychosocial function.
Overall, moderate strength of evidence supports the use of occupational therapy telehealth interventions for people with progressive neurological conditions for functional mobility and fatigue management. Because of the quality of studies, sample sizes, and findings between control and intervention groups, insufficient evidence supports occupational therapy telehealth interventions for this population for the outcomes of psychosocial function, upper extremity function, quality of life, and occupational performance and satisfaction.
Spinal Cord Injury
Two studies of adults with spinal cord injury (SCI) were included in the review (Dorstyn et al., 2019, Level 2b; Liu et al., 2021, Level 1b). Interventions addressed employment skills through online modules and remote health assessment and education via an app. Both studies incorporated telehealth-delivered interventions in which occupational therapy practitioners were members of the interprofessional team. Outcomes included psychosocial function, quality of life, and work. Telehealth was effective in significantly improving psychosocial outcomes for optimism (Dorstyn et al., 2019, moderate bias) and self-efficacy (Liu et al., 2021, low bias). Significant improvements were also reported in quality of life (Liu et al., 2021). There were no significant results for employment outcomes. Given one high-quality study with low bias, there is moderate strength of evidence to support telehealth intervention for adults with SCI, especially for outcomes of self-efficacy and quality of life.
Brain Injury
Ten studies were included in the brain injury subtheme. All but one of the studies included participants with a history of stroke. One study (Andreassen et al., 2022) included participants with stroke, traumatic brain injury (TBI), and aneurysm. Although this study also had participants with Parkinson’s disease and multiple sclerosis, we included the article in the brain injury subtheme because most of the participants experienced stroke or TBI. Levels of evidence of these studies were Level 1b (Asano et al., 2021; Borstad et al., 2022), Level 2b (Andreassen et al., 2022; Hung et al., 2021; L. Li et al., 2020; Zhang et al., 2022), and Level 3b (Burdea et al., 2020; Cramer et al., 2021; Fusari et al., 2022; Rozevink et al., 2021). Telehealth interventions provided by occupational therapy practitioners focused on upper body function related to hemiparesis, condition management, transition across delivery settings, ADLs and IADLs, functional mobility, cognition, caregiving, and quality of life.
Upper extremity training was conducted using various game-based approaches, electronic applications, or robot-assisted devices. Through several upper extremity outcome measures, findings showed improvement in upper body function among participants receiving telehealth (Borstad et al., 2022; Burdea et al., 2020; Cramer et al., 2021; Fusari et al., 2022; Rozevink et al., 2021; Zhang et al., 2022).
Burdea et al. (2020) described the need for stroke rehabilitation interventions to be intensive and engaging to align with neuroscientists’ knowledge of brain plasticity principles. According to Rozevink et al. (2021), keeping clients motivated is of high importance for adherence and can be achieved through game-based interventions. Four of the studies included game-based telehealth interventions (Borstad et al., 2022; Burdea et al., 2020; Hung et al., 2021; Rozevink et al., 2021). Two studies included motivational interviewing or coaching-based components delivered by online apps (Fusari et al., 2022; Zhang et al., 2022). Asano et al. (2021) and Cramer et al. (2021) delivered home-based telerehabilitation interventions that consisted of occupational therapy and physiotherapy or occupational therapy and physical therapy, respectively. Occupational therapy was also delivered via telehealth using the RemindMe application to promote the use of digital calendars and mobile phone use to address cognitive deficits secondary to a neurological condition (Andreassen et al., 2022).
Telehealth was not found to be superior to usual rehabilitation delivered by occupational therapists and physical therapists (Asano et al., 2021). Eight studies found statistical significance in decreasing tactile sensitivity (Borstad et al., 2022), upper extremity function (Burdea et al., 2020; Fusari et al., 2022; Hung et al., 2021; Rozevink et al., 2021), grip strength, depression, attention (Burdea et al., 2020), occupational performance (Andreassen et al., 2022; Cramer et al., 2021), quality of life (Fusari et al., 2022), the ADL of feeding, caregiver confidence (L. Li et al., 2020), IADLs, functional mobility, and caregiving (Zhang et al., 2022).
Although statistically significant findings were reported for upper extremity function outcomes, these findings primarily resulted from studies with small sample sizes. On the basis of the study findings, sample sizes, risk of bias, and study designs, a moderate strength of evidence supported the use of telerehabilitation for individuals with brain injury for upper extremity function. There is low strength of evidence for telehealth interventions provided for the outcomes of occupational performance, cognition, quality of life, and psychosocial factors.
Visual Impairment
One study included individuals with visual impairment (Bittner et al., 2022, Level 2b). This study was an RCT with low risk of bias that explored the use of telehealth for remote instruction on magnifier use for individuals with visual impairment delivered in 1-hr telehealth sessions. There were statistically significant improvements in the use of assistive technology (i.e., magnifier use) indicating the telehealth intervention was superior to the control condition. There is insufficient evidence for telehealth interventions used to promote magnifier use.
Discussion
The purpose of this systematic review was to analyze updated evidence exploring occupational therapy telehealth interventions for clients over the life course to improve occupation-centered outcomes. This study provides an extension from a prior systematic review on the same topic and demonstrates the growth in telehealth-delivered interventions following the COVID-19 pandemic. Feldhacker et al. (2022) identified 780 eligible articles from 2009 to 2019, ultimately including 20 in their systematic review. In the 3 yr of our review (2019–2022), the amount of research has increased substantially. We identified 6,116 eligible articles and ultimately included 43 that met the criteria and studied the use of telehealth-delivered intervention for the treatment of chronic conditions, the effects of COVID-19 lockdown, developmental disorders, musculoskeletal conditions, neurological conditions, and visual impairment for individuals over the life course. Many of the included studies did not prioritize direct comparisons between a group receiving telehealth intervention and a control group that did not receive telehealth intervention. Instead, the purpose was to evaluate the effectiveness of telehealth interventions on occupational therapy outcomes. Sometimes, but not always, this was compared with traditional or face-to-face interventions.
This review adds important practice recommendations regarding the use of telehealth for the delivery of interventions with clients experiencing chronic conditions. Feldhacker et al.’s (2022) review found low strength of evidence for the use of telehealth in the treatment of chronic conditions, whereas this review included 11 studies under this theme and reported strong and moderate strength of evidence across the outcomes studied. Chronic conditions require long-term health management and often, yet not exclusively, require interventions focusing on lifestyle (Centers for Disease Control and Prevention, 2024). As such, occupational therapy practitioners possess the qualifications to provide interventions addressing chronic disease management (Berger et al., 2018; Rouch et al., 2021; Smallfield et al., 2021). It is promising that outcomes of the studies addressing chronic conditions included in this review focused on quality of life, health management, and occupational performance and satisfaction through a variety of interventions, including lifestyle and nutrition coaching.
Evidence supporting occupational therapy interventions for the treatment of chronic pain, the effects of cancer and cancer treatment, and the inclusion of care partners is emerging, highlighting the valued role of occupational therapy in affecting outcomes for those with a chronic condition. Our study found moderate strength of evidence to support the use of telehealth interventions with occupational therapy expertise, through 1:1 sessions or an educational website, for outcomes of caregiver well-being. This adds important evidence for practitioners to consider, because a previous review was inconclusive concerning the effectiveness of interventions for caregivers of people with chronic conditions (Rouch et al., 2021). Additional research on the dosage and intensity of telehealth interventions for chronic conditions is needed, and future research should continue to address the results of app and game-based interventions to provide additional evidence to support their use.
The two articles included under the theme of effects of COVID-19 isolation (Belhan Çelik et al., 2022; Pekçetin & Günal, 2021) studied the impact of COVID-19 lockdown on well-being, quality of life, and occupational balance caused by the disruption experienced in daily routines. It was promising to see research addressing these factors. Prior research demonstrated that the COVID-19 pandemic did affect life routines, yet most of the research was conducted to address the impact on work disruptions (Alfano et al., 2023; Caringal-Go et al., 2022). Alfano et al. (2023) surveyed workers affected by the COVID-19 pandemic and reported changes in work– life balance by gender. Similarly, Caringal-Go et al. (2022) researched work–life balance among workers in the Philippines who telecommuted to determine strategies to promote balance. The findings of this study showed that balance in areas outside of work (e.g., relationships, self-care, physical activity) promoted greater work–life balance. The articles we included in this review had participants who were adolescents and young adults. We see this as a promising step for occupational therapy practitioners to provide interventions to these populations.
More research is needed to provide stronger strength of evidence for telehealth interventions delivered to individuals with a developmental disorder. Various interventions within the scope of occupational therapy practice are recommended when working with individuals with a developmental disorder in a health care facility (Bathje et al., 2021). Telehealth may be effective in providing continuity of care postdischarge. Although the two studies we included (Jamali et al., 2022; Parsons et al., 2019) showed promising findings for telehealth interventions, the study designs and sample sizes resulted in moderate risk of bias. Therefore, research designed with higher levels of evidence and less risk of bias is warranted to draw stronger recommendations for practice.
The findings of this review indicate moderate strength of evidence supporting the efficacy of telehealth occupational therapy intervention for those who have musculoskeletal conditions that affect upper and lower body function for a variety of outcomes. Partly because of the rising aging population, musculoskeletal conditions are affecting more people than ever before. A 2019 Global Burden of Disease study conducted by the Cleveland Clinic (2022) reports that 1 out of every 3 adults, or over 127 million people, are affected by musculoskeletal conditions. The review by Feldhacker et al. (2022) did not report findings specific to musculoskeletal conditions, making the recommendations reported in this review a critical update for occupational therapy practitioners. Despite variability in research protocols, outcomes, and populations, the aggregated results suggest that telehealth has the potential to match or surpass the effectiveness of traditional in-person approaches. Furthermore, telehealth should be considered as a viable alternative to conventional occupational therapy when clients experience barriers to attending in-person appointments, such as living in rural or remote regions or when financial, transportation, or time constraints exist, to facilitate greater access to occupational therapy services (Ortiz-Piña et al., 2021; Torpil & Kaya, 2022a, 2022b). In addition, as more clients age in place, telehealth occupational therapy can support them in their home environment (C. T. Li et al., 2022).
Clients with neurological conditions were also a focus of this review. Neurological conditions affect over 3.4 billion individuals globally (Institute for Health Metrics and Evaluation, 2024). Therefore, occupational therapy interventions are critically needed to assist in promoting occupational engagement and participation for clients with various neurological disorders. Welsby et al. (2019) drew a key takeaway that home-based therapies focusing on meaningful occupations were the most promising for optimizing occupational performance. Our added evidence demonstrates promise for the ability to advance home-based therapy services using telehealth. Furthermore, exercise including walking, stretching, and strengthening was incorporated in several studies to promote functional mobility and to reduce fatigue. Participants used goal setting and environmental cues along with care partner support to promote telehealth intervention success. We found these telehealth interventions were similar to non- telehealth-delivered interventions that also provide evidence for clients with conditions such as Parkinson’s disease and multiple sclerosis (Wood et al., 2022). For individuals with neurological conditions, there is a need for research evidence that explores telehealth to support nonmotor symptoms including quality of life and psychosocial function.
In this review, two studies were included that provided remote health assessment and education through online modules and an app for individuals with SCI (Dorstyn et al., 2019; Liu et al., 2021). With moderate strength of evidence, findings supported telehealth intervention for adults with SCI for outcomes of self-efficacy and quality of life. Although this is promising for supporting psychosocial functions, evidence is lacking for several areas of need as identified through an international scoping review. These areas include physical health, functional abilities, performing daily activities, and cost-effective adaptive equipment (Alve & Bontje, 2019). Alve and Bontje (2019) also emphasized the need to enhance participation in daily activities for people with SCI, particularly in low-resource conditions. Additional research on telehealth in these areas could help address gaps for those in such conditions. Furthermore, ongoing education for practitioners to improve comfort and competence in delivering telehealth interventions for individuals with SCI is warranted (Goel et al., 2022), given the strength of the findings in this review.
For individuals with brain injury, telehealth interventions were similar to those found in the 2022 review. For example, interventions focused on game-based approaches for addressing upper extremity function using tablets, electronic applications, and robot-assisted devices, along with home exercise programs delivered with electronic applications, activity tracking, and postdischarge follow-up. Researchers used telehealth to aid in communication with participants. In some instances, telehealth was as effective as other treatment methods (Asano et al., 2021; Borstad et al., 2022; Cramer et al., 2021). This provides evidence that telehealth may be useful as a modality for intervention and may benefit individuals even when combined with other approaches to intervention. It is promising that we identified research on game-based interventions to address upper extremity function. Nevertheless, there remains a need for additional research evidence to support this intervention method (Hildebrand et al., 2023).
The theme of visual impairment yielded one article related to interventions focusing on vision. Our findings are consistent with prior research showing telehealth for clients with visual impairment can be an effective treatment modality but is not superior to other approaches, including face-to-face intervention (Bittner et al., 2023). A prior review found no articles related to low vision (Bittner et al., 2020), so the inclusion of one study in our review is a promising finding. Clients with low vision may require specific training or modifications to successfully use telehealth (U.S. Department of Health and Human Services, 2022).
Limitations
This review was limited to articles in which practitioners conducted interventions using telehealth and articles that included occupation-centered outcomes. For this reason, articles may have been excluded if they did not include outcomes within the scope of the review criteria or did not specifically call out occupational therapy practitioners as study interventionists. The articles related to COVID-19 addressed interventions not related to the physical implications of COVID; instead, they focused on life balance and quality of life. Future research on the long-term implications of COVID-19 using interventions delivered via telehealth is needed. Even as we concluded this review, we noted the amount of new literature on telehealth. Because of the vast amount of literature on this topic (i.e., over 9,000 articles identified in our initial search), we anticipate the need for an updated review on this topic every 5 yr, or sooner. We recognize articles published since the search was conducted were not captured in this search.
Implications for Occupational Therapy Practice
The COVID-19 pandemic led to policy changes, allowing occupational therapy telehealth practitioners to provide telehealth services. This study has the following implications for occupational therapy practice: ▪ Telehealth is a viable delivery model for occupational therapy practitioners to provide care for a variety of clients across the life course, especially for those diagnosed with chronic conditions, using a lifestyle-based intervention approach. ▪ Promising new evidence supports telehealth services to potentially improve occupational performance for those affected by isolation secondary to COVID-19, developmental disorders, neurological conditions, and musculoskeletal conditions. ▪ Occupational therapy practitioners are producing research related to telehealth outcomes as the sole practitioner and as members of interprofessional teams. For this reason, occupational therapy practitioners may consider models of delivery that include single professional or collaborative intervention to best meet desired outcomes.
Conclusion
This review provides an updated synthesis of the effectiveness of occupational interventions over the life course delivered through a telehealth delivery model from 2019 to 2022. Feldhacker et al.’s (2022) review resulted in 780 articles through database searches, whereas this current review yielded 6,116 abstracts by applying similar search strings. The increasing number of studies indicated the explosive growth of telehealth occupational therapy intervention from 2019 to 2022, echoing that occupational therapy practitioners adopted telehealth as one of the main strategies to maintain therapy for clients during the COVID-19 pandemic.
Occupational therapy practitioners who use telehealth interventions should consider implementing telehealth for clients diagnosed with a chronic condition. The strongest available evidence was found in lifestyle-based interventions targeting nutrition and health behaviors. Occupational therapy practitioners should consider routinely providing this type of intervention when telehealth is considered appropriate. Various interventions delivered to a range of populations were supported by moderate evidence. Insufficient strength of evidence was found for interventions focusing on cancer-related cognitive decline, pain interventions for upper body function, visual impairment, and psychosocial function and quality of life for those with progressive neurological impairments. More research and larger participant samples are needed to enhance the strength of evidence in these areas before these interventions can be broadly implemented.
Supplemental Material
Supplementary material for Occupational Therapy Telehealth Interventions Across Populations From 2019 to 2022: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050939.pdf for Occupational Therapy Telehealth Interventions Across Populations From 2019 to 2022: A Systematic Review by Whitney Lucas Molitor, Diana R. Feldhacker, Zhaoying Li, Nicole Kuhl and Vanessa D. Jewell in The American Journal of Occupational Therapy
Footnotes
*Indicates articles included in this systematic review.
Acknowledgments
This review received financial support from the University of North Carolina at Chapel Hill Department of Health Sciences. We acknowledge Barbara Renner for her critical assistance with completing the database searches and Marit Watson for her review of an early version of the evidence table.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.