
Abstract
This study analyzed outcomes data from a U.K. clinical service that provides vocational rehabilitation to people with an acquired brain injury.
An estimated 75% of people with acquired brain injuries (ABIs) are of working age (Foy, 2014). However, long-term changes to physical, cognitive, emotional, and behavioral abilities are prevalent (Goldman et al., 2022) and constitute a substantial barrier to returning to work (Brasure et al., 2013; Foy, 2014; Hooson et al., 2013). Nevertheless, returning to work is one of the most important rehabilitation goals for many ABI survivors (Lundqvist & Samuelsson, 2012), and successful employment is a key predictor of quality of life after ABI (Arwert et al., 2017; Fride et al., 2015; Passier et al., 2011). This outcome may be because employment provides social connection, financial independence, and a sense of purpose to those with ABI (Tyerman, 2012).
Therefore, U.K. policy and clinical guidelines emphasize the importance of providing vocational rehabilitation (VR) to support ABI survivors to return to work (British Society of Rehabilitation Medicine, 2009, 2010; Department for Work and Pensions, 2013). Substantial evidence supports both the clinical and cost-effectiveness of VR for ABI survivors (Abrams et al., 1993; Donker-Cools, Daams, et al., 2016; Kendall et al., 2006). However, further high-quality randomized controlled trials are required to determine the optimal model of VR for ABI survivors (Tyerman, 2012). With regard to the clinical benefit, a quantitative synthesis of 26 studies showed that ABI survivors return to employment more quickly after injury when VR is provided (Kendall et al., 2006). Although cost-effectiveness varies depending on the specific VR model and intervention components, previous research has shown that the ratio of taxpayer benefit to operational cost may be as high as 2:1 (Abrams et al., 1993).
Although VR often plays an important role in supporting ABI survivors return to a familiar work role (i.e., their preinjury role), many ABI survivors encounter barriers to returning to previous roles, including condition-related, patient-related, and work-related factors (Donker-Cools et al., 2018). Therefore, supporting ABI survivors to find new vocational roles is often crucial (Tate et al., 2015), with studies suggesting that up to 40% of successful employment outcomes are achieved through this pathway (Fleming et al., 1999; Grauwmeijer et al., 2012). Supported employment models of VR may be particularly appropriate for helping ABI survivors find and retain new vocational roles, given their emphasis on the use of individualized assessments, job coaches, tailored job training, and ongoing support (Shames et al., 2007; Vornholt et al., 2018; Wehman, 2023).
Although the supported employment model of VR has been relatively widely implemented and well researched (Pogoda et al., 2022; Wehman, 2023), most of the existing evidence has originated from the United States, with far less research considering the extent to which this approach translates effectively to other countries with different health care systems and employment environments (Murray et al., 2022). In the United Kingdom, health care services that support ABI survivors to return to work are relatively rare, and services offering support to identify and retain new vocational roles are even more rare. Therefore, and because of the lack of U.K.-based research in this area, the extent to which the supported employment model of VR translates effectively to ABI survivors in the United Kingdom remains unclear. Moreover, in previous studies, researchers have tended to characterize VR outcomes using relatively coarse metrics, and exploration has been limited regarding the specific characteristics of new vocational roles obtained by ABI survivors.
Recognizing these gaps in the literature, the aim of this exploratory research was twofold. First, we gauged the extent to which a supported employment approach to VR may be effective in the United Kingdom by quantifying the number of ABI survivors who accessed the Working Out program between 2005 and 2023 and were successful in obtaining a new vocational role using routinely collected clinical data. The Working Out program is a rare example of a specialist U.K.-based health care service that provides rehabilitation plus supported employment to ABI survivors based in and around the Buckinghamshire region of the United Kingdom (Tyerman et al., 2008). Second, we characterized the new vocational roles obtained in terms of their type (paid vs. voluntary), status (full-time vs. part-time), and the employment sector. Characterizing roles obtained may be helpful for understanding the employment sectors that may be, on average, more or less feasible for ABI survivors.
Method
In this brief report, we present the first stage of a service improvement project. It was registered as an audit with Buckinghamshire Healthcare National Health Service (NHS) Trust Research and Innovation, who confirmed that it did not need a specific ethical committee review. Reporting is in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist.
Working Out Program
The Working Out program, run by the Community Head Injury Service in Buckinghamshire Healthcare NHS Trust, provides specialist rehabilitation, including VR for ABI survivors. It operates over the long term to support ABI survivors to return to previous work roles, find new work roles, and successfully maintain work roles. The program is tailored to an individual person but usually involves work-directed interventions, skills training, education, and coaching. Referral to the Working Out program may be through primary care services, secondary care services, or specialist voluntary organizations. Inclusion criteria for the Working Out program were age ≥16 yr, confirmed diagnosis of ABI (i.e., traumatic or other forms of acquired nonprogressive brain injury of any severity and at any stage postinjury), living in and around Buckinghamshire or neighboring counties, and clinically identified vocational assessment or rehabilitation need. Exclusion criteria were medically unstable and severe behavioral problems that were unmanageable in the community.
The Working Out program is delivered by a multidisciplinary team with input from occupational therapy practitioners, clinical psychologists, speech-language therapist, rehabilitation assistants, and a placement consultant. The placement consultant plays a pivotal role in supporting ABI survivors to find new vocational roles by offering individualized assessments to understand the ABI survivor’s strengths, skills, interests, and support needs. This assessment may inform a personalized employment plan, which, in turn, directs job searching and applications. Oftentimes, the placement consultant assists in job searching, application processes, and interviews. To support job retention, the placement consultant may also offer hands-on training or coaching to help the person learn tasks and adapt to their responsibilities. Throughout the process, the placement consultant acts as a key advocate for ABI survivors to ensure that their needs are met and that their rights are protected while also building relationships with employers to create or identify job opportunities. Further detail on the Working Out program can be found in previous publications (Tyerman et al., 2008) and online (https://www.buckshealthcare.nhs.uk/pifs/community-head-injury-service-information-for-clients-referred-to-the-working-out-team-vocational-rehabilitation/).
Data Collection and Analysis
In this study, we retrospectively analyzed routinely collected clinical data from 278 ABI survivors who accessed the Working Out program between 2005 and 2023 and who started a new vocational role during this period. A new vocational role was defined as “any paid, voluntary, or educational role that the person did not occupy prior to their referral to the Working Out program.” Data characterizing new vocational roles were collected by the placement consultant (Martin Hillier) as part of standard practice. The following variables were recorded for every new vocational role: ABI survivor starting role, year starting role, role type (paid, voluntary, education or training), role status (full time: ≥35 hr per week, part time: <35 hr per week), hours per week (at beginning of vocational role), and industry (Standard Industrial Classification [SIC] code). The following demographic and clinical data were retrieved retrospectively from clinical records to characterize the sample: date of birth, gender, ethnicity, date of ABI, ABI type, and date of first contact with Working Out team. Descriptive statistics were calculated to characterize the sample and new vocational roles obtained. R-Studio (Version 4.3.1) was used to facilitate data analysis and visualization.
Results
Sample Characteristics
A total of 278 people with ABI who accessed the Working Out program started a new vocational role. Of these people, 69 (24.82%) were female, and 212 (76.26%) were White–British. The most common type of ABI was traumatic brain injury (n = 99), followed by stroke (n = 98), brain tumor (n = 15), subarachnoid hemorrhage (n = 12), hypoxic brain injury (n = 9), and mild head injury (n = 7). The mean age at injury was 38.04 yr (SD = 15.31, range = 0.51–68.49), and the mean age at the point of first contact with Working Out was 41.75 yr (SD = 13.09, range = 16.64–68.78). The mean time between injury and first contact with Working Out was 4.06 yr (SD = 7.60, range = 0.12–53.32). The mean time between first contact with Working Out and starting an initial new vocational role was 1.98 yr (SD = 2.35, range = 0–14). Demographic and clinical data are summarized in Table 1.
Demographic and Clinical Characteristics of ABI Survivors Who Accessed the Working Out Program and Started a New Vocational Role Between 2005 and 2023 (N = 278)
Note. ABI = acquired brain injury.
New Vocational Roles
A total of 777 new vocational roles were obtained by the 278 included ABI survivors. Data on role type (paid, voluntary, education or training) were available for 767 (98.71%) of the vocational roles. Of these vocational roles, 332 (43.29%) were paid roles, 386 (50.33%) were voluntary roles, and 49 (6.39%) were education or training roles. The number of new vocational roles obtained per year is shown in Figure 1. Annual data showed that the number of new vocational roles of any type peaked in 2021, with a total of 56 new vocational roles obtained. The number of new voluntary roles peaked in 2009 (n = 33), whereas the number of paid roles peaked in 2023 (n = 35). The number of education or training roles peaked in 2021 (n = 8) but remained consistently lower than paid and voluntary roles.
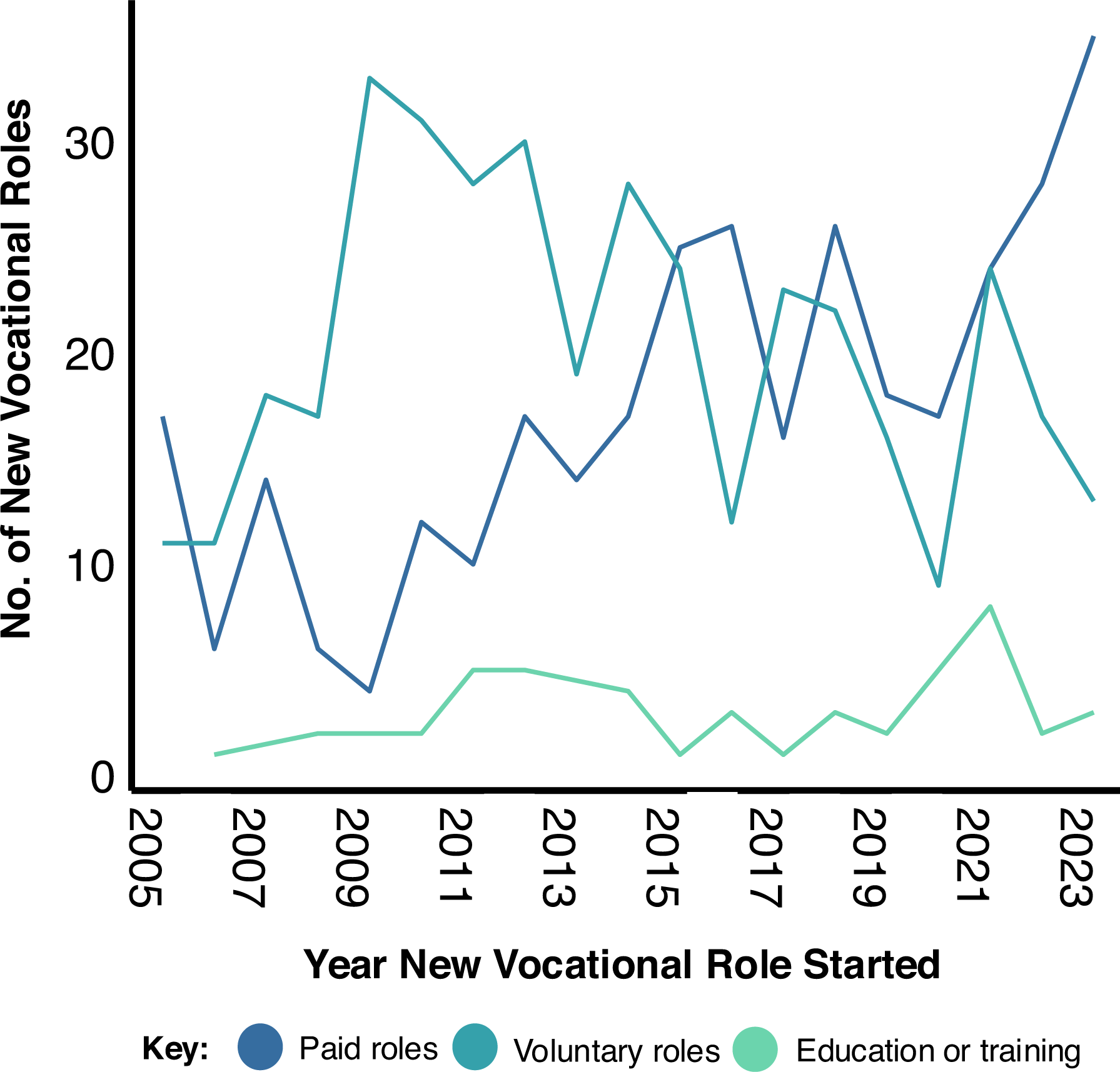
New vocational roles obtained by acquired brain injury survivors who accessed the Working Out Program between 2005 and 2023 plotted by year and role type.
ABI survivors obtained an average (mean) of 2.79 new vocational roles each (SD = 2.13, range = 1–15). Among the 278 ABI survivors, 181 (65.11%) obtained at least one paid role. Of these people with ABI, 74 (40.88%) obtained a voluntary role before obtaining a paid role. The number of ABI survivors who appeared to use a “stepping-stone” approach—in which they moved from placements of one type to another, with many ABI survivors progressing from voluntary roles to paid roles—is illustrated in Figure 2.
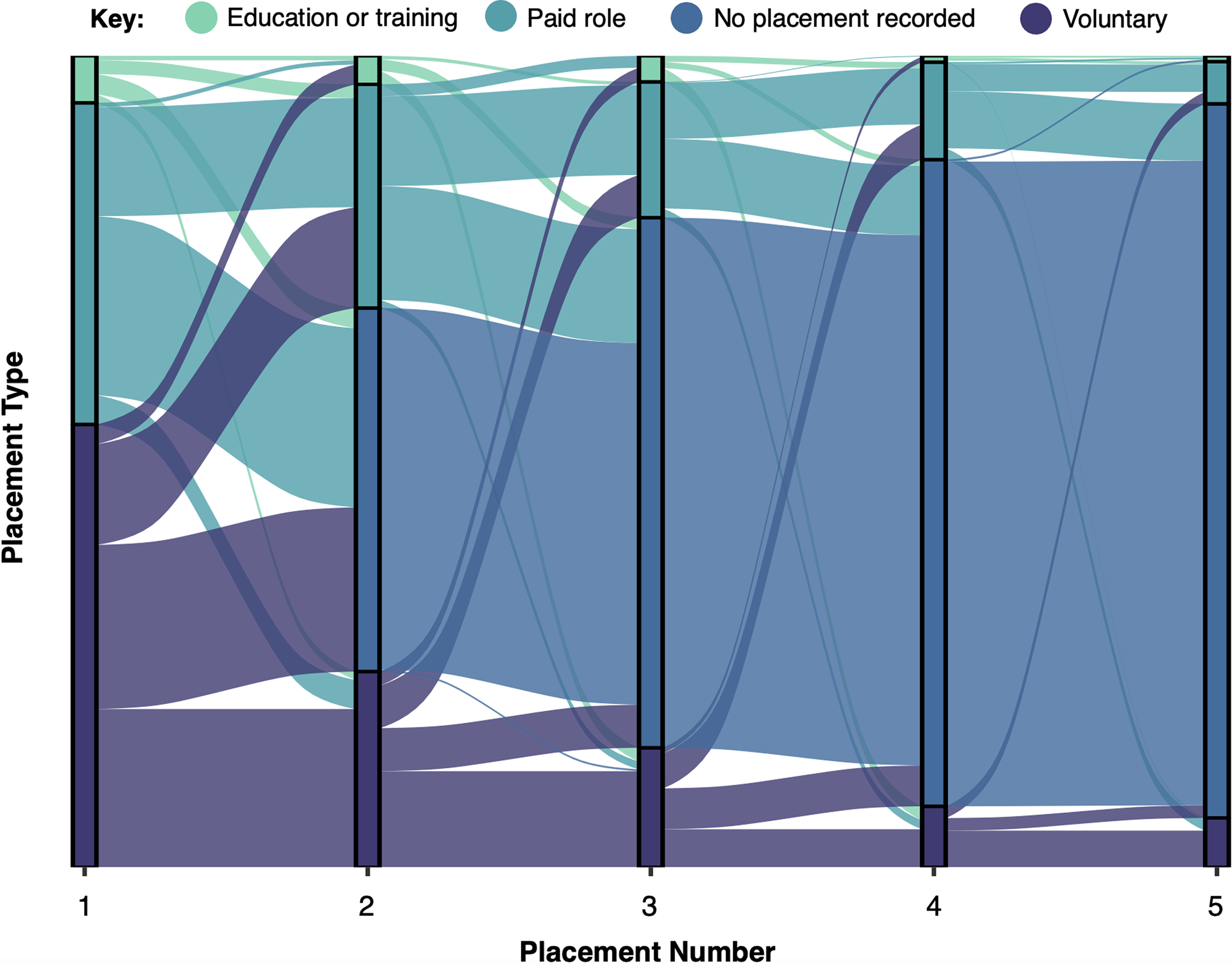
Sankey diagram showing how acquired brain injury (ABI) survivors who obtained multiple vocational roles often used a stepping-stone approach in which they progressed from one vocational role type to another over subsequent placements.
Data on full-time versus part-time role status were available for 581 (74.77%) vocational roles. Of these vocational roles, 441 (75.90%) were part time, and 140 (24.10%) were full time, in which full time was considered at least 35 hr working per week. For part-time roles, the mean number of hours worked per week was 9.53 (SD = 7.24, range = 0.50–32.00).
The industries in which new vocational roles were obtained are shown in Figure 3. Note that SIC classifications are provided as Supplemental Material (available online with this article at https://research.aota.org/ajot). The most frequent industry in which a new vocational role was obtained was administrative and support service activities (Section N: n = 172, 22.14%), followed by wholesale and retail trade; repair of motor vehicles and motorcycles (Section G: n = 126, 16.22%), and human health and social work activities (Section Q: n = 85, 10.94%).
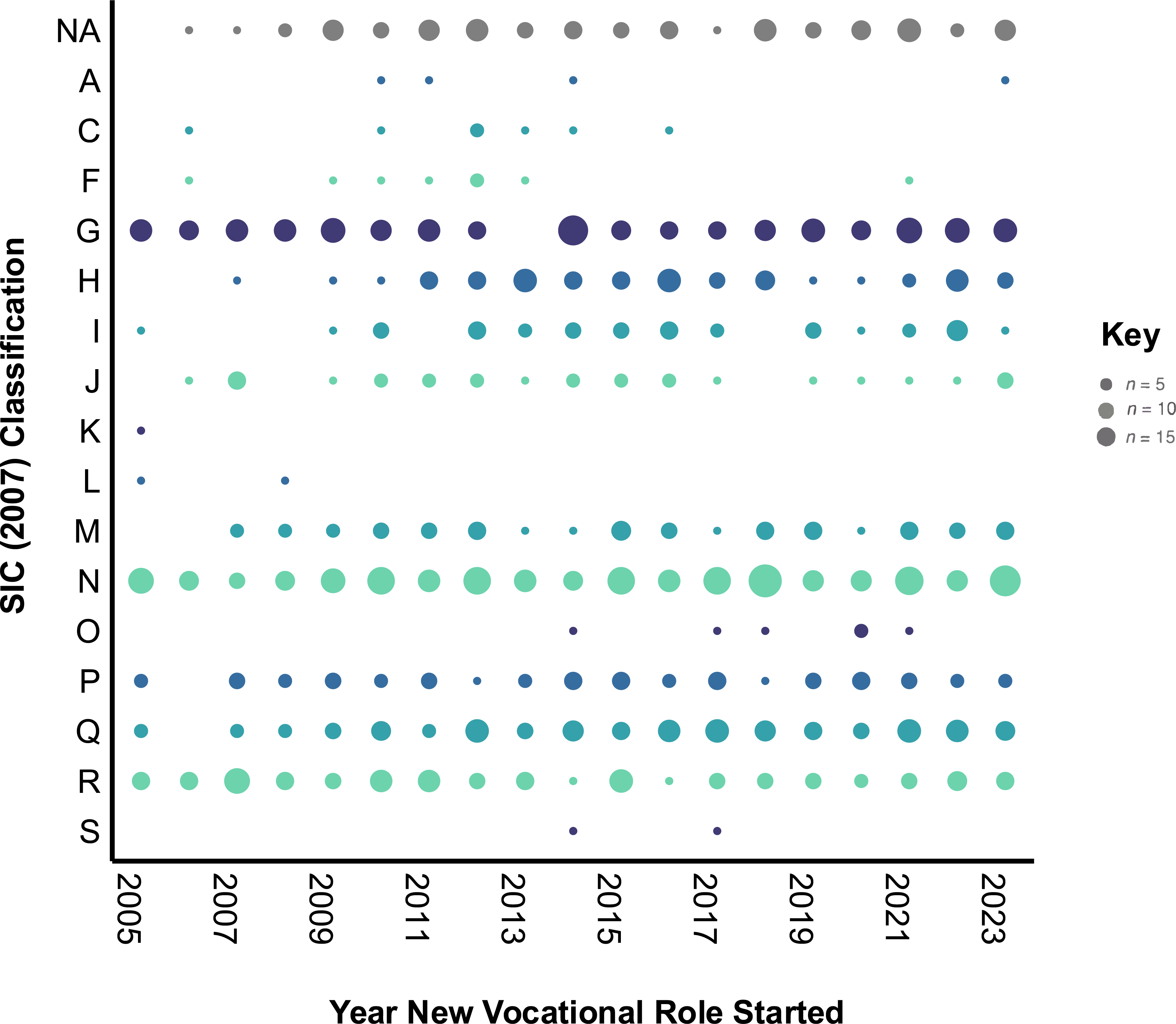
New vocational roles obtained by acquired brain injury (ABI) survivors who accessed the Working Out program between 2005 and 2023 plotted by year (x axis) and Standard Industrial Classification (SIC) code (y axis).
Discussion
By retrospectively analyzing routinely collected clinical data from a U.K. health care service providing rehabilitation and supported employment for ABI survivors, we showed that many ABI survivors successfully obtained new vocational roles, with approximately half of these new roles constituting paid positions. ABI survivors in this study began the Working Out program on average 4 yr after their injury, and it took on average 2 yr of VR intervention to find a new vocational role. It appeared that many ABI survivors used a stepping-stone approach, whereby multiple vocational roles were obtained, with voluntary roles often preceding a paid role. Overall, these results offer encouraging evidence that ABI survivors in the United Kingdom may be supported to find new vocational roles. However, rehabilitation plus supported employment interventions may be required for an extended period of time, given the complexity of ABI as a chronic health condition and challenges associated with finding new vocational roles.
Although in previous studies researchers have claimed that changes in vocational outcome after the first 2 yr postinjury are relatively rare (Groswasser et al., 1999; Johnson, 1998; Odgaard et al., 2017), our results suggest that—with appropriate specialist intervention—returning to employment remains a possibility for many ABI survivors in the years after brain injury. Nevertheless, finding a new vocational role took a substantial amount of time in many cases, with the 2-yr average reported here broadly aligning with previous estimates (Bloom et al., 2018; Iverson et al., 2012; Man et al., 2004; Simpson et al., 2020; Thor et al., 2021). However, it should be noted that past estimates have varied substantially because of differences in study populations and the way return to work has been operationalized.
Crucially, in previous studies, researchers who reported return to work time averaging less than 2 yr considered ABI survivors returning to previous roles only (Bruckner & Randle, 1972; Iverson et al., 2012). However, a multicenter observational study of patients with severe traumatic brain injuries demonstrated that finding a new vocational role after ABI took significantly longer than returning to a previous role (Simpson et al., 2020). Finding a new vocational role indeed requires additional highly specialist clinical input, potentially involving liaison with new employers and support to build new skills (Tyerman, 2012). The amount of time required to find new vocational roles in this study may reflect not only the complexity of the VR process but also the complexity of ABI as a chronic health condition with potential sequalae spanning cognitive, psychological, physical, sensory, and behavioral domains (Goldman et al., 2022). Finding a new vocational role requires these sequalae to be effectively managed (van Velzen et al., 2011), but developing strategies to compensate for post-ABI impairments takes substantial time and expertise.
The data showed temporal trends in the number of new vocational roles obtained. Although these trends should be interpreted with caution given the retrospective and exploratory nature of the study, they were observed to mirror significant global economic events, potentially indicating that VR outcomes may be influenced by contextual and individual factors that have already been thoroughly researched (Donker-Cools et al., 2016; Greenspan et al., 1996). For example, annual data showed substantial reductions in paid vocational roles obtained in 2008 and 2009, which followed a substantial global economic downturn. In addition, paid vocational roles obtained in 2023 dramatically increased after economic stimulation designed to counteract the impact of the coronavirus disease (COVID-19) pandemic. It may be important for VR practitioners to remain mindful of the context in which new vocational roles are being sought and to consider identifying voluntary positions for people with ABI to use as a stepping stone into paid employment, particularly during challenging economic periods.
Limitations
This study has several limitations. We were not able to establish the proportion of Working Out program clients who found new vocational roles versus those who were unsuccessful in obtaining new employment. We also were not able to identify factors associated with successful VR outcomes. Nevertheless, previous research speaks to these questions (Donker-Cools, Wind, & Frings-Dresen, 2016; van Velzen et al., 2009a, 2009b), and future research is planned to investigate prognostic factors specific to the Working Out program. Moreover, although our observation that it took on average 2 yr to find a new vocational role suggests that substantial clinical input was required, the specific VR intervention components accessed were not recorded. Thus, it was not possible to determine the amount of clinical input received by ABI survivors who found new vocational roles or the cost-effectiveness of the Working Out program. Finally, because no data were recorded on role retention, it is not possible to determine the success with which vocational roles were retained by ABI survivors.
Conclusion
In conclusion, this brief report extends the existing literature on supported employment after ABI by showing that a rehabilitation plus supported employment approach to VR is likely to provide some benefit to ABI survivors in the United Kingdom. Although the study objectives of quantifying and characterizing the vocational roles obtained were met, further research is required to provide more conclusive and definitive evidence of clinical effectiveness.
Supplemental Material
Supplementary material for Vocational Rehabilitation Outcomes From the U.K. Working Out Program: Characterizing the New Vocational Roles Obtained by People With Acquired Brain Injuries
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050957.pdf for Vocational Rehabilitation Outcomes From the U.K. Working Out Program: Characterizing the New Vocational Roles Obtained by People With Acquired Brain Injuries by Georgina Hobden, Martin Hillier, Ben Chetland and Amy Murphy in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank all staff involved in delivering the Working Out program between 2005 and 2023. We also thank all the people with acquired brain injuries who accessed the Working Out program over this period, without whom this research would not have been possible.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.