
Abstract
This study investigated the effects of using mirror therapy before augmented-reality therapy to improve motor and balance in stroke rehabilitation.
Upper extremity (UE) deficits after stroke may hinder performance of activities of daily living (ADLs; Lee et al., 2015). Stroke rehabilitation in the hospital allows patients to receive multidisciplinary services. Given the limited hospital length of stay, home-based practice is important to complement clinic-based stroke rehabilitation (Toh et al., 2022).
Home-based rehabilitation allows functional practice of ADLs that can be tailored to align with the level of stroke severity (Geller et al., 2022). Home-based interventions that implement UE functional practice, such as mirror therapy (MT; Geller et al., 2022; Hsieh et al., 2018) and telerehabilitation (Yang et al., 2022), have shown promising benefits.
MT uses the mirror reflection of the unaffected limb while symmetrical activities of both arms are performed to facilitate motor learning (Rossiter et al., 2015). MT provides sensory inputs and motor practice that reorganize the sensorimotor system of the brain for neurologic recovery (Ramachandran & Altschuler, 2009). MT may decrease sensorimotor impairments and enhance functional recovery (Lee et al., 2015) and ambulation in survivors of chronic stroke (Lin et al., 2014), and it may be used as a priming strategy to promote rehabilitation outcomes (Stoykov & Madhavan, 2015).
MT-primed interventions may enhance mobility and cognitive function (e.g., interactive gaming) to optimize treatment outcomes. Exergaming (Mubin et al., 2019) is relevant for motivating patient engagement in mobility and cognitive practice. Augmented reality (AR), a novel approach for gamified stroke rehabilitation, provides intensive, repetitive, and context-rich training (Gorman & Gustafsson, 2022). Recent research findings support the benefits of AR in stroke rehabilitation (Gorman & Gustafsson, 2022; Mubin et al., 2019).
Home-based practice of MT and AR may be set up and monitored with telerehabilitation to allow patient practice in a familiar environment and to reduce the cost of transportation between home and the clinic (Lloréns et al., 2015). Research on the comparative efficacy of clinic- and home-based rehabilitation is scarce; there is a need to evaluate the effects of practice setting. We hypothesized that MT preceding AR gaming in different treatment contexts may have differential effects. Clinic-based practice may improve motor and balance deficits more than home-based practice, given therapist guidance for clinical practice. Home-based practice may be advantageous for enhancing functional performance in daily life. The research may contribute to informing practice in clinic- and home-based stroke rehabilitation.
Method
Design
This study was an assessor-blinded, randomized crossover design (Lim & In, 2021). The 3-wk washout interval was determined from a previous study (Hsieh et al., 2018), with consideration to balance the potential dropout rate because of the prolonged treatment period in the crossover design. Outcome data were collected before and after two intervention phases and at the 3-mo follow-up. During each phase, participants underwent nine intervention sessions, consisting of 45 min of MT followed by 45 min of AR training, 3 days per wk, for 3 wk. The session count and total treatment duration were similar to those in previous crossover clinical trials (Carda et al., 2017; Hsieh et al., 2018). After a 3-wk washout period, the group that initially received home-based rehabilitation received clinic-based rehabilitation, and vice versa (Figure 1).
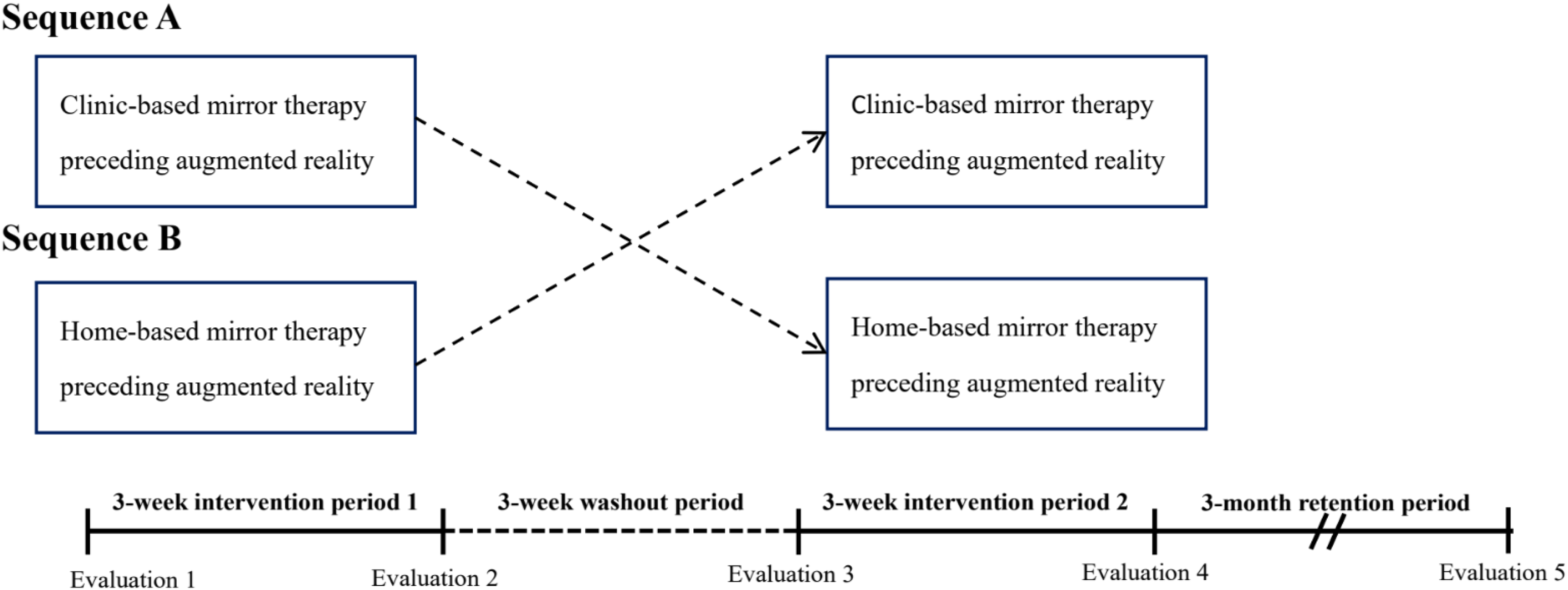
Crossover study design and procedure.
Participants were recruited from outpatient rehabilitation clinics with the approval of the respective ethics committees and provided informed consent. Eligible participants were randomly assigned to the group receiving either clinic-based or home-based MT before AR (Figure 2).
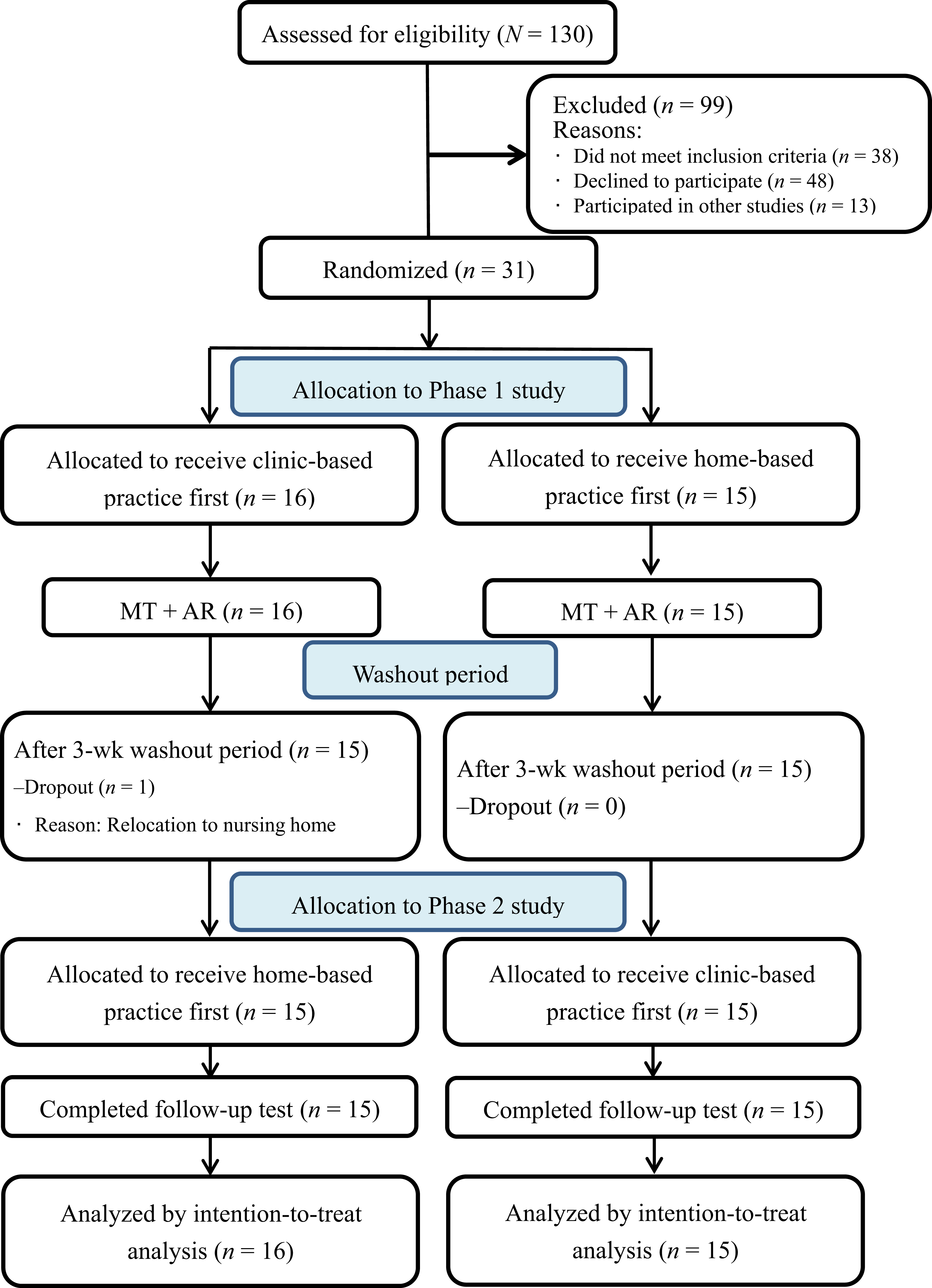
Study flowchart.
The assignment sequence was generated using a web-based randomization tool (https://www.randomizer.org/). A blinded research assistant provided the assigned sequence to the therapist and conducted outcome measurements. The same trained therapist administered the two intervention phases to all participants.
Participants
The inclusion criteria were as follows: ▪ age 20 to 80 yr, with a first-ever unilateral stroke lasting 3 mo or longer ▪ baseline score greater than 10 on the Fugl-Meyer Assessment Scale of Upper Extremity (FMA–UE; Fugl-Meyer et al., 1975) ▪ Modified Ashworth Scale (MAS) score less than 3 in all joints of the affected arm (Charalambous, 2014) ▪ ability to follow study instructions ▪ ability to maintain a step-standing position for at least 30 s (Lloréns et al., 2015) ▪ ability to walk a minimum of 10 m, with or without assistive devices (Park et al., 2017).
The exclusion criteria were a history of significant neurologic diseases or medical conditions, major visual deficits, and acute inflammation.
Intervention
Home-Based Rehabilitation
Participants received the intervention at their home. Research personnel trained the participants on the MT protocol (Lee et al., 2015) and on the setup and use of the AR system in the first session at each participant’s home (Figure 3). Research personnel monitored subsequent sessions remotely and in real time through Google Meet and provided real-time feedback. A wooden mirror box (41 × 50 × 30 cm3) was provided and placed in front of the participants in MT sessions. To enhance concentration on the mirror image, we used a small stool to conceal the unaffected arm from view (Hadoush et al., 2013; Lim et al., 2016). Following the MT practice of Geller et al. (2022), research personnel provided participants with objects used in daily routines (e.g., a mug, a rag, coins, etc.) and written guidelines. Each participant practiced unimanual MT and bimanual MT for a minimum of 150 repetitions (Bondoc et al., 2018) that consisted of movements of forearm pronation–supination, wrist flexion–extension, grasp and release, and in-hand manipulation.
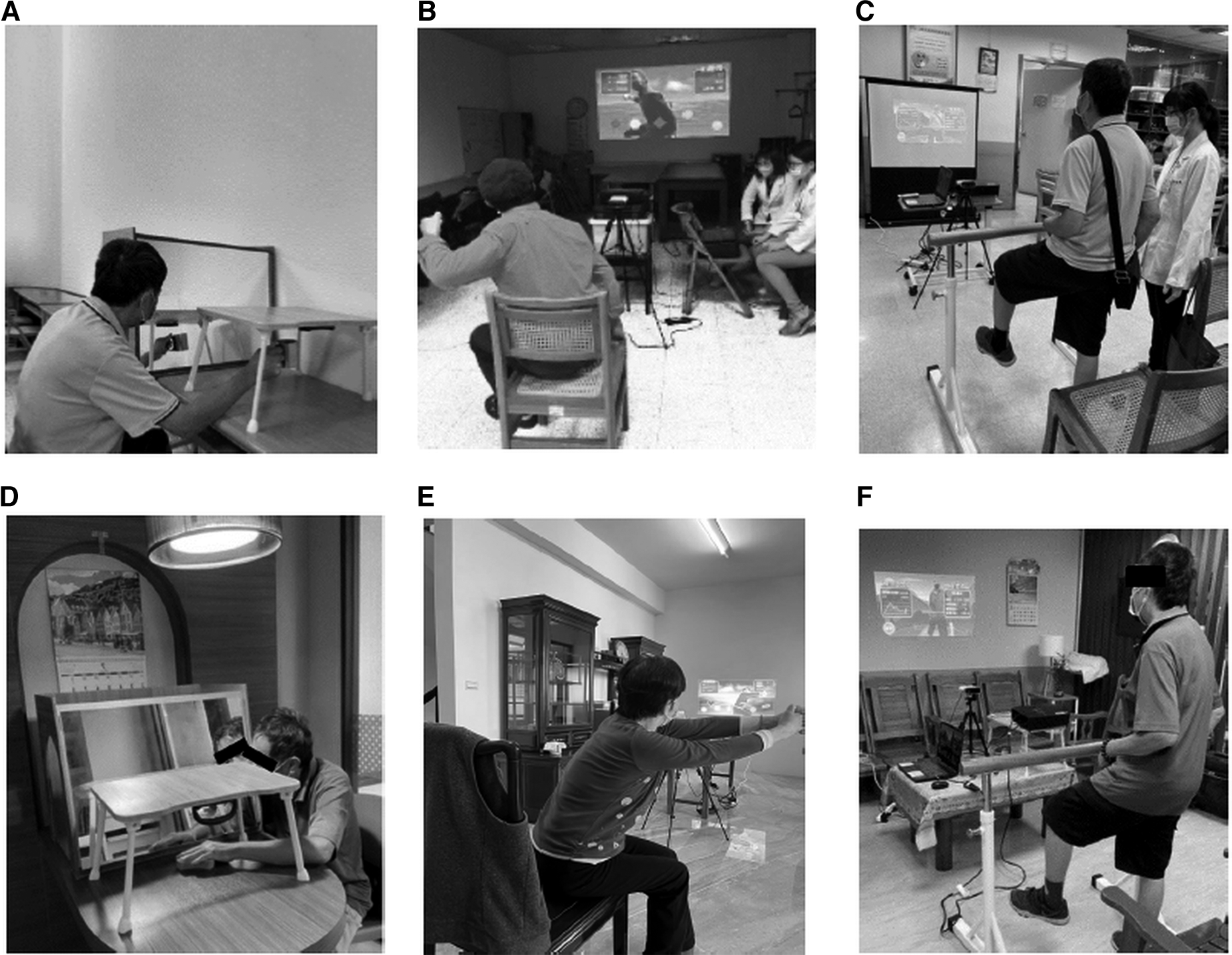
An illustration of clinic-based MT (A); clinic-based AR upper limb training (B); clinic-based AR lower limb, balance, and postural control training (C); home-based MT (D); home-based AR upper limb training (E); and home-based AR lower limb, balance, and postural control training (F).
The AR system consisted of a computer with a 50-in. screen positioned 3 m away from the participants, a Kinect sensor, a Kinect-based AR system program, and a projector (see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot).
Home-based practice sessions were videotaped using Google Meet and uploaded to the cloud drive for the therapist to review and discuss with the participant when needed. Participants recorded the frequency of home practice in a daily monitoring log and brought the activity log to the clinic for the therapist to review home program progression. The therapist also provided weekly phone calls for purposes of practice compliance.
Clinic-Based Rehabilitation
The participants underwent the MT and AR protocols under the supervision of a therapist in a clinical setting. The treatment principles of the clinic-based rehabilitation were the same as for the home-based group. The major difference was that the intervention took place in the clinical setting. The training tools that are used during MT practice in the clinic may not be as individualized as those in the home environment. Simulated equipment and modalities such as simulated cup-grabbing using a cone, simulated coin-flipping using a wooden chess piece, and simulated pen-taking using a cylinder peg were provided for functional practice. Similar to the home-based intervention, UE practice in the clinic involved forearm, wrist, and finger movements. The therapist provided feedback about movement strategy and performance quality.
Outcome Measures
Primary Outcome Measures
The FMA–UE is a 33-item scale that assesses motor impairment (Fugl-Meyer et al., 1975). The total score ranges from 0 to 66. The FMA–UE has good validity and responsiveness for survivors of stroke (Hsieh et al., 2009).
The Berg Balance Scale (BBS) uses 14 items to evaluate balance during static and functional movements within a specified time, with a maximum score of 56 (Blum & Korner-Bitensky, 2008). The BBS is reliable and valid for use with survivors of stroke (Kudlac et al., 2019).
Secondary Outcome Measures
The 13-item Chedoke Arm and Hand Activity Inventory (CAHAI) assesses bimanual activity performance after stroke and is rated on a 7-point scale ranging from 1 (total assistance) to 7 (complete independence). The reliability and validity of the CAHAI have been established in survivors of stroke (Barreca et al., 2005).
The Motor Activity Log (MAL) is a self-reported semistructured scale that evaluates the amount of use (AOU) and quality of movement (QOM) of the affected UE. It assesses 30 common daily tasks, and the score for each task ranges from 0 (never) to 5 (as prestroke). The reliability and validity have been validated (van der Lee et al., 2004).
The Stroke Impact Scale (SIS) measures health-related quality of life after stroke. The scale includes 59 items across eight subscales, each scored from 1 to 5, using one of the following anchors: strength (1 = no strength at all, 5 = a lot of strength), difficulty (1 = could not do at all, 5 = not difficult at all), or frequency (1 = all of the time, 5 = none of the time; Duncan et al., 2003). The global perception of stroke recovery, based on scores ranging from 0 (no recovery) to 100 (full recovery), represents the degree of recovery and quality of life. The metric properties of the SIS have been well established (Vellone et al., 2015).
Data Analysis
An effect size (f) of .42 for sample size estimation was based on previous studies (Hsieh et al., 2018; Yang et al., 2022). To reach a power of .80 with a level of significance set at .05, at least 15 pairs of participants per group were needed in this study.
The normality of data was studied on the basis of the value of skewness (±1). The baseline differences between the two groups were compared using the χ2 analysis for categorical data and a one-way analysis of variance for continuous data. The sequence effect was examined with an independent-samples Student’s t test immediately after the second phase of intervention. The carryover effect was examined with an independent t test to test for the differences between the groups (Wellek & Blettner, 2012). Pretest scores that were measured at the beginning of each phase were used for comparison. If the test did not yield significant results, suggesting a minimal carryover effect, the data from two phases were combined for further analysis. An intention-to-treat analysis, with the “last observation carried forward” method, was used to address missing data (Hamer & Simpson, 2009).
Changes in the outcome measures, where the data of the same treatment condition in the two sequences were combined, were evaluated using one-way analysis of variance immediately after the treatment and at the 3-mo follow-up. We calculated an effect size of partial η2 to measure the magnitude of differences between practice settings. The large, medium, and small partial η2s were .138, .059, and .01, respectively (Cohen, 2013). The level of statistical significance was set at .05. We performed the statistical analyses using IBM SPSS Statistics (Version 19.0) and G*Power software.
Results
Participants
The study recruited 31 participants. No dropouts occurred in Phase 1. During study Phase 2, one participant withdrew because of relocation to a nursing home. The baseline characteristics between the two groups were not significantly different (ps = .17–.93; Table 1). No significant injuries or adverse effects were reported. Data analysis showed no significant sequence effects (ps = .20–.80). The carryover effect was nonsignificant (ps = .14–.93).
Participant Baseline Characteristics
Note. Categorical data are presented as n (%), and continuous data are presented as M (SD). The p values were calculated according to χ2 analysis or one-way analysis of variance. BBS = Berg Balance Scale; FMA–UE = Fugl-Meyer Assessment Scale of Upper Extremity; NIHSS = National Institutes of Health Stroke Scale; SIS–Total = Stroke Impact Scale–Total.
Efficacy of UE Motor Function
Clinic-based practice improved significantly on the FMA–UE (η2 = .07, p = .04) (Table 2). This benefit extended to the 3-mo follow-up on the FMA–UE (η2 = .11, p = .01). In addition, clinic-based practice improved significantly better in BBS (η2 = .10, p = .01), relative to home-based practice. However, no significant difference was observed at the 3-mo follow-up assessment between the clinic-based practice and home-based practice.
Pretreatment, Posttreatment, and Follow-Up Assessment Between the Two Settings of Rehabilitation Practice on the Outcome Measures
Note. Scores for the MAL AOU and QOM range from 0 (never) to 5 (as pre-stroke). SIS domain scores range from 1 to 5, using one of the following anchors: strength (1 = no strength at all, 5 = a lot of strength), difficulty (1 = could not do at all, 5 = not difficult at all), or frequency (1 = all of the time, 5 = none of the time). The p values were calculated according to the analysis of variance. Effect size (partial η2) was calculated for magnitude of the difference between two practice settings. ADL = activities of daily living; AOU = amount of use; BBS = Berg Balance Scale; CAHAI = Chedoke Arm and Hand Activity Inventory; FMA–UE = Fugl-Meyer Assessment of Upper Extremity; IADL = instrumental activities of daily living; MAL = Motor Activity Log; NA = not applicable; QOM = quality of movement; SIS–Total = Stroke Impact Scale–Total.
*p < .05.
Efficacy of ADL
The home-based rehabilitation revealed a trend for better performance on the MAL AOU (η2 = .06, p = .06) and a small-to-moderate effect on the MAL QOM (η2 = .04, p = .11; Table 2). Although a significant time effect was noted between the pre- and posttreatment CAHAI results, no significant setting-specific effect was observed.
Efficacy of Participation in Life Situations
Clinic-based practice and home-based practice both showed a significant effect of time in SIS Total scores. Clinic-based practice resulted in significantly greater improvements in the SIS Mobility domain (η2 = .07, p = .05) immediately after the treatment and at 3 mo (η2 = .09, p = .02; Table 2). The clinic-based practice also maintained treatment gains at 3 mo in the SIS ADL–IADL (η2 = .11, p = .01) and Hand Function (η2 = .08, p = .03) domains.
Discussion
This single-blinded, randomized crossover study revealed that the clinic- and home-based practice of MT preceding AR yielded differential benefits in improving motor functions, ADL performance, and participation in stroke rehabilitation.
Practice that is based on the different treatment sequences may lead to diverse effects in stroke outcomes. The sequence effect was nonsignificant in the present study. Analysis was performed to investigate the differences between practice settings.
In support of the study hypothesis, clinic-based practice showed significantly better performance than home-based practice from pretest to posttest on UE motor function, balance, and functional participation reflected by the FMA–UE, the BBS, and the SIS Mobility domain, respectively. Except for the SIS Strength and SIS Mobility domains, the retention of therapeutic gains was observed within both practice settings at the 3-mo follow-up. From pretest to follow-up, the clinic-based practice was statistically significant compared with the home-based practice in the FMA–UE and the SIS domains of ADL–IADL, Mobility, and Hand Function. The effect of clinic-based practice was significantly better in the recovery of balance indicated by the BBS from pretest to posttest, but not from pretest to the follow-up assessment. The home-based rehabilitation condition caught up with the training progress and attained similar performance as the clinic-based rehabilitation condition at the 3-mo follow-up.
The improvement in UE motor function of the clinic-based practice was consistent with the findings of Bondoc et al. (2018), which revealed the clinically meaningful improvements of UE impairments reflected by the FMA–UE after MT was completed before task-oriented practice in the clinic. Survivors of stroke who receive one-on-one, in-clinic rehabilitation may have a higher sense of readiness to engage in the intervention, which may have possibly improved motor and functional deficits (Chi et al., 2020). Besides, the participants in the clinic received real-time feedback about their performance (Sharma, 2016). Given the instantaneous feedback provision, clinic-based practice may establish a better foundation for the acquisition and transfer of motor skills beyond practice context.
The clinic-based practice exhibited greater improvement in balance and postural control measured by the BBS from pretest to posttest. Traveling between home and the clinic may provide the participants with more opportunities to practice outdoor motor planning and execution skills, which may have possibly enhanced their motor abilities during the clinic–phase intervention. However, the home-based rehabilitation condition attained similar improvement at the 3-mo follow-up. On the one hand, one plausible explanation is that the clinic-based participants were treated more cautiously and conservatively for fall prevention during in-clinic training, which might have limited some exercises of lower limb movement and balance control. On the other hand, participants were familiar with their home environment, and they may have adapted some strategies to ambulate within the home environment, which may make them more confident and motivated to perform balance and postural control practices at home.
Clinic-based practice showed significantly better immediate treatment effect in both primary outcome measures, given the instantaneous feedback by the therapist, allowing participants to learn and adjust, which may facilitate subsequent training to build on the established foundation. Home-based practice may contribute to long-term benefits for balance and postural control with a well-structured home program and adequate monitoring through telerehabilitation.
Home-based rehabilitation has the advantage of promoting ADL performance (Geller et al., 2022; Hsieh et al., 2018). The home-based group in the present study showed a trend for improved outcomes in the MAL AOU. The findings are consistent with Hsieh et al. (2018), who reported that home-based MT and task-specific training enhanced the daily use of the stroke survivors’ affected UE measured by the MAL AOU compared with clinic-based practice. A review study showed that home-based UE interventions were more effective in improving affected UE function and satisfaction in using the affected arm for daily activities than clinic-based therapy, both after treatment and at follow-up assessments (Toh et al., 2022). The home environment offers a sense of familiarity and may promote transfer of learned skills to daily activities (Chi et al., 2020).
Participation results of the SIS demonstrated a significant effect from pretreatment to posttreatment for both practice settings, but differential setting-specific effects in some of the SIS subscales immediately after treatment and at the 3-mo follow-up. The clinic-based practice showed better retention of treatment gains in the SIS ADL–IADL, Mobility, and Hand Function domains. One possible explanation is that the clinic-based practice may involve participants commuting between home and clinic. During this process, the participants may have chances to visit a convenience store to purchase stuff (item in the SIS ADL–IADL domain), walk in the street and take transportation (items in the SIS Mobility domain), tie shoelaces, and pick up coins (items in the SIS Hand Function domain), which may lead to a better self-perceived ability and health state.
The rehabilitative program delivered in two practice settings demonstrated diverse effects in the outcomes of motor function, ADL, and participation in real-life situations. There is a trend for greater effect on self-reported outcome in ADL (i.e., MAL) in favor of home-based practice in this study. Home visits by the therapist for intervention may lead to stronger effects in daily life functioning. This possibly warrants study in further research. To provide more evidence on practice settings and treatment retention, further research is needed to validate the differential effects of clinic- and home-based rehabilitation. In addition, further research may investigate the effects of cross-setting practice compared with practice in single settings.
Limitations
First, the findings may not be generalized beyond the scope of the present study. Second, home-based practice was videotaped, and the participant received feedback on training completion. Further study may investigate the effects of synchronous and delayed feedback. Third, participants with limited digital skills may find it difficult to use electronic gadgets. Telerehabilitation may need to be implemented using user-friendly mobile applications.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ This study provides insights that participants for whom UE recovery is a priority may initially receive clinic practice to acquire better foundational skills; participants for whom attaining lower extremity recovery is a priority may keep practicing structured intervention protocols in their familiar home environment to achieve long-term benefits of balance and postural control. ▪ On-site or telerehabilitation-based feedback provided by occupational therapists was key in monitoring the participant’s training progress. Telerehabilitation devices with simple operation were recommended for participants with limited digital literacy. ▪ The differential effects of MT-primed AR practice across the clinic and home settings warrants further research on rehabilitation contexts. This research may inform the transition between hospital and home care in stroke rehabilitation.
Conclusion
This research indicated that clinic-based practice led to greater improvements in motor and balance deficits, whereas home-based practice may be advantageous for enhancing patient-reported use of the affected arm in real-life situations. The findings suggest the need to consider practice settings in stroke rehabilitation. Further study is needed to validate the findings.
Supplemental Material
Supplementary material for Clinic- and Home-Based Practice of Mirror Therapy Preceding Augmented Reality in Stroke Rehabilitation: A Crossover Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.050961.pdf for Clinic- and Home-Based Practice of Mirror Therapy Preceding Augmented Reality in Stroke Rehabilitation: A Crossover Study by Keh-chung Lin, Yi-chun Li, Yu-fang Lin, Hiu-ying Lau, Chih-chieh Kuo, Chia-jung Lin, Yi-hsuan Wu and Chih-yu Lin in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This study is registered through ClinicalTrials.gov (NCT05467813). The research was supported in part by the National Science and Technology Council (Grants MOST-111-2314-B-002-168-MY3, NSTC 112-2811-B-002-028, NSTC 112-2811-B-002-088, and NSTC 113-2811-B-022-075) and by the National Health Research Institutes (Grant NHRI-EX113-11333PI) in Taiwan. We are grateful to Dr. Anuchart Kaunnil and Dr. Sopida Apichai at Chiang Mai University in Thailand for their intellectual contribution to data interpretation and comments on the practical implications of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.