
Abstract
This study emphasizes the essential role of occupational therapy in developing equitable, client-centered interventions that address environmental barriers for older adults in low-income households.
The U.S. Census Bureau reports that just 10% of American homes are aging ready, suggesting that the home environment poses a significant barrier to older adults (i.e., those age 65 yr or older) who want to age in place (Vespa et al., 2020). Aging in place refers to the concept of older adults living in their own homes and communities safely and comfortably regardless of age, income, or ability level. The goal of aging in place is to support older adults’ health, well-being, and quality of life by providing the necessary community-based resources and home modifications to support their living spaces (Gustavson et al., 2023).
As the aging population continues to increase, there is a need to develop home modification programs designed to be inclusive and incorporate the unique needs and preferences of older adults who are living in lower-economic-status communities and who are racially and ethnically diverse (Gilmore-Bykovskyi et al., 2022; Robinson-Lane et al., 2023; Stark et al., 2017; Szanton et al., 2016, 2019). The number of U.S. older adults who identify as a member of a racial/ethnic population increased from 9.0 million (21%) in 2012 to 14.5 million (25%) in 2022 (Administration for Community Living [ACL], 2024), meaning that 1 in 4 older adults identified as such. Within racial/ethnic groups, 17.6% of Black American, 12.9% of Asian American, and 16.9% of Hispanic older adults lived below the poverty level, in comparison with 8.2% of non-Hispanic White older adults (ACL, 2024).
Overall, challenges commonly faced by older adults who reside in low-income households are limited access to health care services, housing instability, poor environmental conditions, financial insecurity, social isolation, and limited access to community support services (Bailey et al., 2017; Gilmore-Bykovskyi et al., 2022; Robinson-Lane et al., 2023; Wehner-Hewson et al., 2022). These population statistics highlight the increasing demand for inclusive and equitable home- and community-based services to address these disparities effectively.
In response to the growing need for inclusive aging-in-place initiatives and home modification programs for older adults, the Older Adult Home Modification Program (OAHMP) was established in 2021. This federally funded program, administered by the U.S. Department of Housing and Urban Development (HUD), aims to improve the safety, accessibility, and functionality of home environments for older adults. The program is designed to support aging in place by reducing fall risks and enhancing quality of life for adults age 62 yr and older who qualify on the basis of low-income status. Although the OAHMP does not enforce a uniform income threshold for eligibility, it targets older adults who meet low-income criteria established by federal or state guidelines. According to HUD (2023), individuals earning no more than 80% of the area’s median income are generally considered low income. For instance, in a region in which the median income is $51,200, a one-person household would qualify with an annual income of $44,800 or less.
The 2023 income-based qualifications for the OAHMP directly include individuals from all racial and ethnic groups who are affected by systemic economic disparities (HUD, 2023; National Equity Atlas, 2021). The OAHMP site for this specific study is based in the City of St. Louis, where the intersection of race and poverty is prominent; 18.9% of Black residents age 65 yr and older live below the federal poverty line compared with just 6.9% of their White counterparts (City of St. Louis, 2019). This disparity underscores the socioeconomic challenges that disproportionately affect older adults who live in low-income households. Historical disinvestment, housing discrimination, and limited access to resources has created systemic barriers that place older adults in vulnerable financial and housing situations (City of St. Louis, 2019; University of Missouri–St. Louis, 2023). The OAHMP has committed to fostering inclusivity by addressing these inequities through low-cost, high-impact home modifications; it aims to reduce fall risks, improve safety, increase accessibility, and enable older adults to age in place effectively.
The OAHMP seeks to address the following objectives: to (1) support underserved communities by promoting equity and community development, (2) advance housing justice by addressing the needs of vulnerable populations, (3) foster sustainable communities by linking home environments to health outcomes, and (4) strengthen environmental justice by reducing health risks and poor housing conditions in diverse, low-income communities (HUD, 2023). Delivered by an interprofessional team of occupational therapists, home repair professionals, and social workers, the program provides a holistic approach to enhancing safety and functionality (HUD, 2023).
The evidence for intervention models used to enact equitable and inclusive home- and community-based services and their outcomes is limited (Gustavson et al., 2023; Shippee et al., 2022). Gustavson et al. (2023) recently developed the applied research logic model for the equitable implementation of advanced care planning to promote aging in place. This model uses the health equity implementation framework and the equitable implementation logic model (Woodward et al., 2019), which align with the OAHMP by providing multilevel approaches to identify and address systemic barriers, ensuring equitable access and outcomes for underserved older adults. They emphasize addressing social determinants of health, such as housing inequities, socioeconomic disparities, and financial barriers while prioritizing contextual factors and implementation determinants (e.g., accessibility, funding) to promote safe, accessible living environments. However, additional inclusive aging research is needed that includes communities of diverse older adults, based on race, ethnicity, and income status, and incorporates aging-in-place supports and home modifications to establish evidence-based intervention, practices, and outcomes (Robinson-Lane et al., 2023).
The purpose of this study was to examine a specific OAHMP site and describe how an interprofessional team implemented the program in an urban community, focusing on the integration of occupational therapy, home repair services, and social work to address the safety, accessibility, and functional needs of older adults who live in low-income households. Our primary research questions were the following: “How does the OAHMP influence functional outcomes, and is it inclusive of older adults in low-income households?” On the basis of recent literature and the OAHMP’s goals, we hypothesized that the program would (1) result in an increase in independence in activities of daily living (ADLs) and instrumental activities of daily living (IADLs) and in environmental home safety postimplementation; (2) reveal a significant relationship between the functional outcomes of self-care ADLs, IADLs, fall risk, and home safety; and (3) enact equitable and inclusive practices to sustain home safety and the accessibility of community-based services.
Method
An evaluation of the older adult participants before and after OAHMP services was conducted. This analysis highlights the team’s collaborative efforts to deliver tailored interventions and modifications that promote aging in place. We received approval from the Saint Louis University institutional review board as an exempt program implementation evaluation.
Recruitment
Recruitment for this program consisted of outreach by the lead nonprofit organization, Mission St. Louis, through referrals from community partnerships, which included a regional Area Agency on Aging, neighbors, community members, and family members. We analyzed the outcomes collected between August 2022 and May 2023. The inclusion criteria included home ownership, an adult age 62 yr or older, and lower-income status (i.e., a family income ≤80% of local area median income).
Intervention
The intervention team included an occupational therapist (Emma Edwards) from an academic institution; a nonprofit community organization consisting of intake specialists, program managers, and home repair specialists; and social work professionals from a community senior services agency. The intervention involved an initial intake over the phone and a minimum of three in-home visits from the intervention team. At intake, the home assessment intake specialist called the client to collect demographic information and administer the screening measures.
At the first visit, the occupational therapist (Edwards) obtained consent for program participation from the client, evaluated the client’s ADL and IADL status and fall efficacy, and assessed the safety of the home environment. The client and the occupational therapist collaboratively developed client-directed functional goals focused on enhancing functional mobility and ADLs in the client’s home environment. The goal areas were categorized as functional mobility (e.g., transfers, stairs, indoor–outdoor tasks), ADLs (e.g., dressing, toileting, bathing), IADLs (e.g., medication management, household tasks, meal preparation), and other (e.g., over-the-counter items to address pain). After Visit 1, the occupational therapist (Edwards) referred the client to the social work team member if areas of concern in the community or living area were identified (e.g., utility bill management, health literacy consultation, meal services).
The home environment assessment was initiated at the second visit, and the client partnered with the occupational therapist (Edwards) and home repair coordinator to assess the home for environmental and safety modifications (e.g., lighting; flooring, steps, and railings; fall risk hazards) to improve functional use and safety. After Visit 2, the home modification contractor and the occupational therapist implemented modifications, the occupational therapist delivered durable medical equipment, and, if applicable, the social worker addressed community and living expenses with the client.
After the home repairs, the occupational therapist administered the Westmead Home Safety Assessment (WeHSA; Clemson et al., 1999) at Visit 3 to reevaluate the home environment; review the modifications made; follow up with the client to address any further home modifications, repairs, and/or social services; and continue to educate the client as needed on the use of durable medical equipment or assistive equipment to support the client’s established goals. The goals established at Visit 1 were evaluated as having been met (successfully using modifications with improved safety and confidence in task completion), partially met (achieving some desired function or implementing some modifications), or not met (unimplemented modifications or ongoing difficulties and safety concerns). The occupational therapist (Edwards) provided written documentation and goal progression using the REDCap data management system (https://project-redcap.org/).
In the 6-mo postimplementation period, the occupational therapist (Edwards) completed a follow-up interview via telephone and reassessed fall efficacy, mobility, and ADL and IADL function.
Data Collection and Measures
The demographic information collected included age, gender, health, disability, and income status. The home assessment intake specialist screened potential clients using the Stopping Elderly Accidents, Death, and Injury (STEADI) fall risk assessment tool (Stevens, 2013) developed by the Centers for Disease Control and Prevention. The STEADI is used to screen older adults for fall risk and assess modifiable factors, and it provides evidence-based resources to reduce fall risk. A score of four or more indicates an increased risk of falling.
The OAHMP–Activities of Daily Living Determination scale (OAHMP–ADLD; HUD, 2023) and the Lawton IADL scale (Lawton & Brody, 1969) were used to assess self-care ADLs and IADLs. The OAHMP–ADLD scale is an adaptation of the Katz et al. (1963) ADL scale, which assesses difficulty with grooming; dressing the upper and lower body; and bathing, functional mobility, eating, and transfers (HUD, 2023). Scores were based on clients’ responses to eight questions, with a score of 1 = No, I do not have difficulty, and I do not need help (independent), 2 = Yes, I have difficulty, but I do not need help (moderately independent), and 3 = I need help regardless of difficulty (minimal to moderate assistance). The client-reported Lawton IADL scale was used to assess clients’ perceived independence in daily living tasks, including meal preparation, medication management, money management, and community mobility (Lawton & Brody, 1969). Scoring on the Lawton IADL scale ranges from 0 (low function, dependent) to 8 (high function, independent).
Clients’ fear of falling and perception of stability during ADLs were assessed with the Falls Efficacy Scale–International (FES–I) Outcome Assessment (Tinetti et al., 1990; Yardley et al., 2005). This 16-item questionnaire asks clients to score their fear of falling while performing a specific activity on a 4-point Likert scale (ranging from 1 = not concerned at all to 4 = very concerned). The scores are summed, and higher scores indicate higher concern for falls, with scores of 20 to 27 indicating a moderate concern about falling, and scores of 28–64 indicating a high concern about falling.
The WeHSA (Clemson et al., 1999), an evidence-based home hazard assessment, was used to evaluate vital components of the home environment. The WeHSA is used to assess external traffic ways (e.g., steps, doorways), internal traffic ways (e.g., hallways, space), bathrooms, bedrooms, kitchen, general indoor spaces (e.g., lighting, seating), medication management, and safety call systems (e.g., fire alarm, CO2 detector). The WeHSA identifies hazards in each environment as “hazard present” or “hazard not present.” Twelve or more identified hazards indicate a home environment safety risk (Clemson et al., 1999).
Data Analysis
We conducted a descriptive analysis of older adult participants to understand their demographics, health, and housing needs, followed by a preimplementation–postimplementation analysis to evaluate changes in ADL and IADL independence, fall risk, and home safety. The descriptive analysis was used to evaluate sociodemographic profiles, postimplementation data, home repairs or modifications, and the distribution of durable medical equipment and over-the-counter items. Paired-samples t tests were used to evaluate participants’ scores across ADL status, IADL status, FES–I fear of falling, and the WeHSA home hazard and safety assessment. A Pearson correlational analysis explored relationships between assessments and services provided, identifying factors linked to successful outcomes. These methods sought to provide a comprehensive evaluation of the OAHMP’s impact on enhancing safety, functionality, and quality of life for older adults aging in place. Cohen’s d was calculated to measure effect size, with 0.20 indicating a small effect, 0.50 a medium effect, and 0.80 a large effect. Pearson’s r was used to assess relationships between program measures, with .10 indicating a small effect size, .30 a medium effect size, and .50 a large effect size. All analyses were performed using IBM SPSS Statistics (Version 28).
Results
The descriptive analysis included 65 (76.5%) of the 85 participants who enrolled in the OAHMP. Of the 85, 13 (15.3%) unenrolled before completion of the program, 5 (5.8%) declined program participation, 1 (1.2%) moved out of their home before the start of the program, and 1 (1.2%) died.
The 65 participants who completed the OAHMP had an average age of 72 yr (SD = 7.3; Table 1). Participants were predominantly female (95.4%) and Black or African American (87.7%). They primarily lived alone (81.5%), with another person (17%), or with two other people (1.5%). Regarding mobility, 83.1% indicated that they did not use a mobility device at home. However, STEADI scores indicated a self-reported fall risk factor. The average STEADI score was 6.6 (SD = 2.4). Twenty-nine participants indicated an average of 2.4 (SD = 2.6) falls over 12 mo. Overall, most participants self-reported their health status as very good (21.5%), good (43.1%), or fair (30.8%); the remainder reported excellent (3.1%) or poor (1.5%) health status. Participants had lived in their homes for an average 32.8 yr, mainly in a single-family detached structure (86.2%). The OAHMP offered a range of services, including installing indoor lighting and grab bars and outdoor modifications such as stair railings and ramps. The cost for these modifications and repairs, including labor and materials, ranged from $482.31 to $1,727.28, with an average expense of $1,135.45 (SD = $238.48; Table 1).
Demographic Characteristics of the OAHMP Participants (N = 65)
Note. OAHMP = Older Adult Home Modification Program.
Scores on the OAHMP–ADLD differed significantly from before (M = 9.68, SD = 1.87) to after (M = 8.77, SD = 2.16) participation in the program, t(64) = 3.429, p < .001, and the number of documented safety hazards identified with the WeHSA decreased (before, M = 25.42, SD = 3.92; after, M = 18.35, SD = 4.91), t(64) = 2.356, p < .001. The increase in self-care ADL level of independence (d = 0.425) and the decrease in home hazards (d = –0.292) demonstrated medium effect sizes postimplementation. There were no significant differences on the other outcome measures after participation in the program; scores on the Lawton IADL and FES–I were not significantly different before and after participation (Table 2).
Results of Paired-Samples t Test for OAHMP Pre- and Posttest Scores (N = 65)
Note. OAHMP–ADLD = Older Adult Home Modification Program–Activities of Daily Living Determination; Lawton IADL = Lawton Instrumental Activities of Daily Living scale; FES–I = Falls Efficacy Scale–International; WeHSA = Westmead Home Safety Assessment.
*p < .01.
The WeHSA (Figure 1) identified that the most prevalent modifications and equipment (N = 316) were related to functional mobility and safety modifications (n = 83; e.g., flooring, steps, or railings), lighting in internal and external spaces of the home (n = 66), and self-care ADL adaptive equipment (n = 61). Examples of adaptive equipment included reachers, shower chairs, motion sensor nightlights, and long-handled bathing equipment. The data indicated that the areas of hazard reduction in the home environment were as follows: lighting hazards 64.0% (preimplementation n = 150, postimplementation n = 54), kitchen hazards 37.0% (preimplementation n = 28, postimplementation n = 17), bathroom hazards 35.6% (preimplementation n = 390, postimplementation n = 251), step/stair hazards 21.8% (preimplementation n = 101, postimplementation n = 79), and total hazard reduction 40.1% (preimplementation n = 669, postimplementation n = 401; Figure 3).
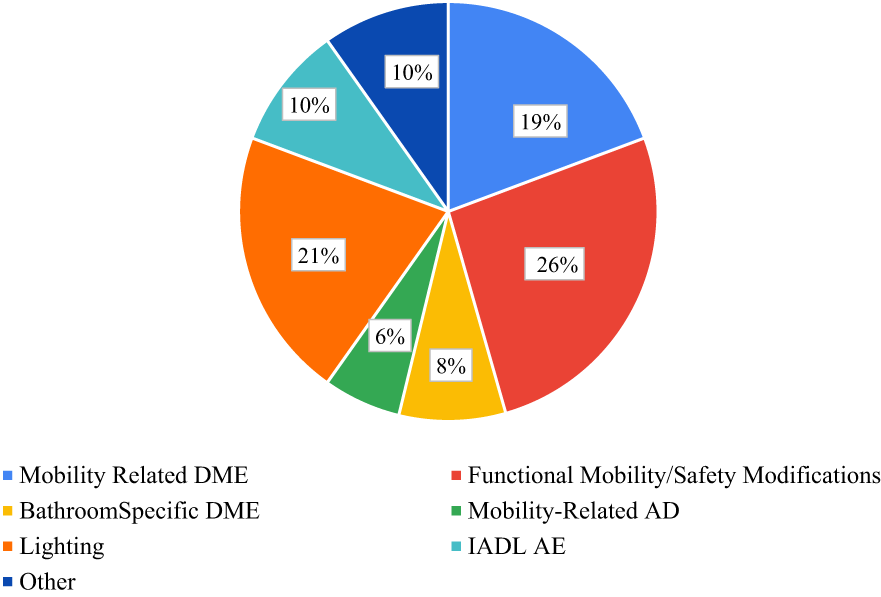
DME, AE, and over-the-counter items provided.
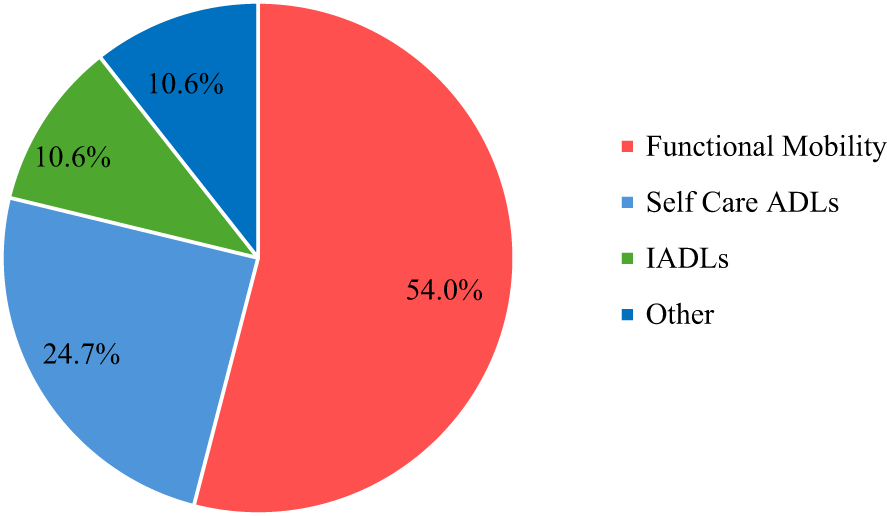
Client-directed functional goals.
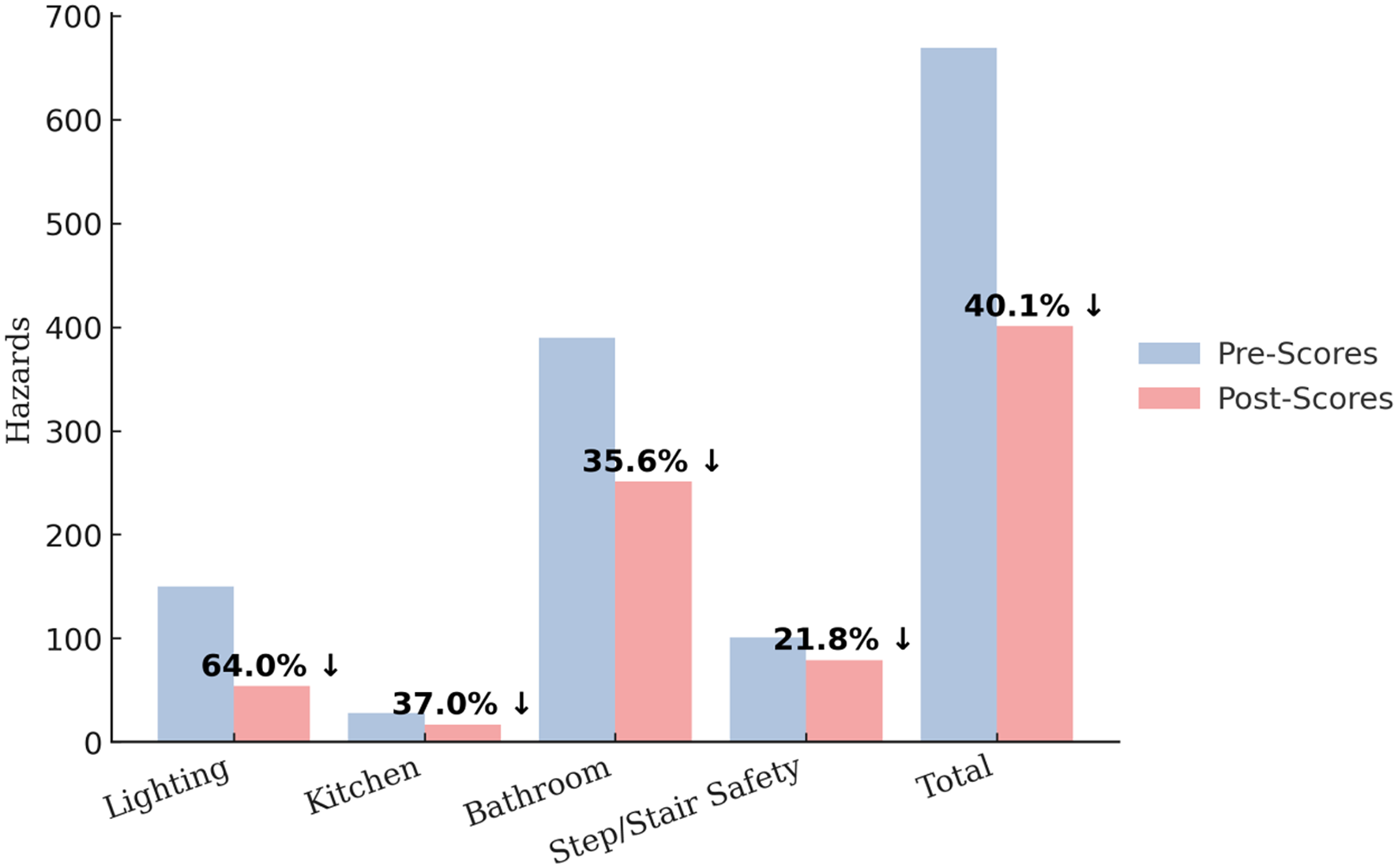
Home hazards assessed by the WeSHA.
In collaboration with the participants, client-directed functional goals (N = 198; Figure 2) addressed identified hazards (Figure 1) in the areas of functional mobility and safety modifications and ADLs (i.e., self-care and home management). The goal areas reported were related to functional mobility and safety (54.0%; n = 107), self-care ADLs (24.7%; n = 49), IADLs (10.6%; n = 21), and other (over-the-counter items; 10.6%; n = 21). Of the 198 goals, the outcomes were as follows:
▪ For functional mobility and safety goals (n = 107), 53.3% (n = 57) were met, 41.1% (n = 44) were partially met, and 5.6% (n = 6) were not met.
▪ For self-care ADL goals (n = 49), 40.8% (n = 20) were met, 30.6% (n = 15) were partially met, and 28.6% (n = 14) were not met.
▪ For IADL goals (n = 21), 33.3 % (n = 7) were met, 47.6% (n = 10) were partially met, and 19.1% (n = 4) were not met.
▪ For other goals, most related to over-the-counter items (n = 31), 45.1% (n = 14) were met, 19.4% (n = 6) were partially met, and 35.5% (n = 11) were not met.
The Pearson correlation analysis examined the relationship between all post assessment outcomes. The results demonstrated significant positive relationships between self-care ADL function, IADLs, health status, and perceived fear of falling after the program (Table 3). In addition, the program’s functional outcomes were analyzed for significance on the basis of age, gender, or income; however, no other relationships were found between these sociodemographic factors and the functional outcomes.
Selected Correlations of Functional Measurements Postimplementation of OAHMP
Note. OAHMP–ADLD = Older Adult Home Modification Program-Activities of Daily Living Determination; Lawton IADL = Lawton Instrumental Activities of Daily Living scale; FES–I = Falls Efficacy Scale International; WeHSA = Westmead Home Safety Assessment.
*p < .01.
Discussion
We began this study by posing the following questions: How does the OAHMP influence functional outcomes, and is it inclusive of older adults in low-income households? The OAHMP clients demonstrated a successful functional goal completion rate, with 91% of 198 goals being met or partially met. The findings of this study align with the initial hypothesis that implementation of the OAHMP would result in increased independence in ADLs and IADLs, as well as enhanced environmental home safety, for this population. The results demonstrate that targeted interventions and tailored home modifications effectively improved functional ability and reduced environmental risks, promoting client independence and safety. Furthermore, not only did these changes create a safer living environment by reducing fall risks, but they also established significant positive relationships between functional outcomes, including self-care ADLs, IADLs, and fall efficacy. These outcomes underscore the importance of individualized approaches to home modifications and their role in fostering functional independence and safety among older adults living in low-income households.
This OAHMP site addressed equitable and inclusive practices to sustain home safety and accessibility by advancing housing justice (HUD, 2023) and advancing sustainability, which recognizes the critical link between the home and community environment and health.
For this specific group of OAHMP clients, the typical home repair project cost averaged $1,135.45 (SD = $238.48), including labor and materials. This is significantly lower than the average for home improvement costs in the United States, where older adult homeowners in lower-economic-status communities incur the highest average repair costs among all demographic groups, at $4,187 per household (Wallace et al., 2019). These costs might be considerably understated because these homeowners may need further home modifications, as identified by this analysis, to ensure a safe living environment (ACL, 2024; Wallace et al., 2019). The OAHMP site effectively implemented equitable and inclusive practices that not only advanced housing justice but also provided cost- effective home modifications, demonstrating its critical role in enhancing home safety and accessibility for older adults in low-income households.
In the past 20 yr, the number of community-dwelling older adults in traditional housing has increased. In 2023, 28% (16.2 million) of all older adults lived alone (ACL, 2024). Although the number of those living in nursing homes has declined, in 2022, 25% (1.3 million) of adults older than age 65 were nursing home residents (ACL, 2024). In 2023, the annual estimated cost of a shared room in a nursing home was $64,000, with a Medicare reimbursement rate of 76% or less, which leaves a potential out-of-pocket cost of $15,000 or more annually (Medicaid and CHIP Payment and Access Commission, 2023; Missouri Department of Health and Senior Services, n.d.). The participants in this study had an average annual income of $21,905 (SD = $10,607) and could potentially face significant economic challenges if institutional settings, such as nursing homes or assisted living facilities, were their only option for care. Given the high costs associated with long-term care—averaging more than $67,000 annually for a shared nursing home room—these expenses would far exceed the participants’ financial capacity, leading to considerable out-of-pocket burdens, financial insecurity, or reliance on limited public assistance programs. This study demonstrated that the OAHMP is a cost-effective solution that effectively promotes functional independence and enhanced environmental safety, and it supports equitable (through client-directed goals) and sustainable intervention for older adults in low-income households, ultimately fostering community stabilization, reducing economic burdens, and offering a potential sustainable alternative to costly long-term-care settings.
Strengths and Limitations
The strengths of this study include the use of an inclusive model established by the HUD development team that has environmental justice aspects and the client-centered interprofessional collaboration among the occupational therapist, home modification specialist, and social worker who implemented this program. This collaboration was bolstered by actively listening to and respecting the participants’ needs. The limitations of this evaluation include the use of self-reported ADL and IADL measures administered by the occupational therapist, which may have introduced response bias and affected the accuracy of the outcomes, and the small sample size (N = 65) and a short implementation period of 10 mo, which restricts the ability to generalize outcomes to larger communities and to generate longitudinal evidence. However, this OAHMP site is currently enrolling participants and is projected to reach more than 300 homes by 2027.
Implications for Occupational Therapy Practice
With only 10% of U.S. homes considered aging ready, many older adults, particularly those from low-income and diverse backgrounds, face barriers to aging safely at home. The OAHMP addresses these challenges through affordable home modifications that improve safety, accessibility, and independence. This study highlights how occupational therapy–led interventions, in partnership with other professions, can enhance autonomy and promote aging in place among older adults. This study has the following implications for occupational therapy practice: ▪ Tailored home modifications, such as grab bars, improved lighting, and adaptive equipment, help older adults safely perform daily activities and promote occupational engagement. ▪ Home-based interventions provide a cost-effective alternative to institutional care, promoting autonomy and quality of life and supporting aging in place. ▪ Working alongside social workers and home repair professionals ensures holistic care that addresses both health and environmental needs and fosters interprofessional collaboration.
Looking Ahead to Clinical Practice
The findings highlight the importance of integrating home modification programs such as OAHMP into routine occupational therapy practice, especially for clients in low-income communities. Occupational therapists should advocate for policies that fund aging-in-place initiatives and develop client-centered intervention plans that reflect individual needs and preferences. As the OAHMP continues to expand, future research should explore its long-term outcomes and scalability, providing further evidence for its inclusion in standard care models. By addressing environmental barriers and promoting occupational engagement, occupational therapy practitioners play a vital role in helping older adults age in place safely.
Conclusion
The findings presented in this study highlight the urgent need for inclusive and equitable aging-in-place initiatives to address the barriers posed by non- aging-ready homes, particularly for older adults in low-income households and inclusive of racially and ethnically diverse communities. Programs such as the OAHMP demonstrate how tailored interventions, including home modifications and interprofessional collaboration, can effectively enhance safety, accessibility, and functional independence among older adults. The results of this analysis show that targeted modifications reduce home hazards, increase ADL and IADL independence, and improve home safety while addressing systemic disparities.
The OAHMP’s commitment to fostering equity is reflected in its prioritization of underserved populations who face higher rates of poverty and housing instability. The program contributes to broader community stabilization and well-being by reducing financial burdens and promoting sustainable homeownership. Additionally, its cost-effective approach to home repairs and modifications provides an economically viable alternative to institutional care, helping older adults maintain autonomy and quality of life.
Despite limitations such as the reliance on self-reported measures and a small sample size, the study demonstrates the significant potential of programs such as the OAHMP to enact meaningful change. As the program continues to expand, further research is needed to evaluate long-term outcomes and refine intervention models that incorporate diverse perspectives and needs. Overall, this study reinforces the critical importance of inclusive home modification programs as a cornerstone of supporting aging in place and advancing health equity in aging populations.
Footnotes
Acknowledgments
We extend our gratitude to Dr. Susy Stark and the Participation, Environment and Performance Lab in the Program of Occupational Therapy at Washington University School of Medicine in St. Louis for their guidance and consultation on the manuscript of this article. This study was sponsored by the U.S. Department of Housing and Urban Development, Office of Lead Hazard Control and Healthy Homes’ Older Adult Home Modification Grant Program. We have no known conflict of interest to disclose.