
Abstract
This study provides support for using the Measure Yourself Medical Outcome Profile® (MYMOP–LAS) with Spanish-speaking Latino communities in the United States.
In the United States, 39 million people speak Spanish at home (Statistical Atlas, 2018). Members of the Spanish-speaking community, particularly those with limited English proficiency, frequently experience difficulty navigating the U.S. health care system partly because of language barriers (Escobedo et al., 2023), hindering access to services (Himmelstein et al., 2021). This reduced access presents a major public health challenge given that the aging Latino population has disproportionate disability that often goes untreated (Garcia et al., 2017).
The Measure Yourself Medical Outcomes Profile® (MYMOP) is a validated measure of health-related symptomatology in which respondents rate the severity and impact of their self-identified health issues of greatest personal concern (Paterson, 1996; Paterson & Britten, 2000). The MYMOP is able to detect clinical change over time from a range of therapeutic interventions, including occupational therapy (Schepens Niemiec et al., 2018), across a wide variety of practice settings, such as primary care (Paterson, 1996) and palliative care (Monnery et al., 2018). The MYMOP is an ideal tool for occupational therapists because it (1) emphasizes symptom non-specificity and therefore dovetails with personalized treatment goals, (2) contains items that directly assess the impact of reported symptoms on activity, and (3) allows practitioners to link MYMOP responses to treatment goals. A licensed, validated Spanish-language version for the Latino community is not yet available. Therefore, this study’s purpose was to develop and validate a culturally appropriate, linguistically accessible, and readable Latin-American Spanish translation of the MYMOP.
Method
Instrument
The MYMOP, originally produced in British English (Paterson, 1996; Paterson & Britten, 2000), assesses one’s self-reported overall symptom well-being in the past week. As part of a brief consultation with a health care practitioner before therapeutic intervention, the client identifies a health problem and, on 7-point Likert scales, rates the severity of the one or two most important associated symptoms, the impact of their health problem on activities of daily living, and their general feeling of well-being. At subsequent treatment visits (or through independent self-report), the individual rerates the same information, with an option to rate a third new symptom. The tool yields an overall profile score along with four subscales: Symptom 1 and Symptom 2 severity, health problem impact on activities of daily living, and well-being. The MYMOP has successfully detected change in response to a variety of interventions, including occupational therapy (Schepens Niemiec et al., 2018) and interdisciplinary primary care (Paterson, 1996).
Translation and Cultural Adaptation Procedures
As detailed in Figure 1, we followed the Translation and Cultural Adaptation of Patient-Reported Outcomes Measures—Principles of Good Practice process (Wild et al., 2005) to adapt the original MYMOP for use in the United States for Spanish-speaking communities. This overall procedure was designed to enhance the cultural appropriateness and scientific meaning of the translation and was approved by the University of Southern California Institutional Review Board on July 11, 2023 (Study ID UP-23–00559). It entailed 10 steps that included key components such as use of Spanish and English translation teams, forward translation, back translation, harmonization, assessment of validity equivalence, research team review, proofreading, and production of a final report. Selected tasks were performed by a professional translation company (LA Translation, Los Angeles, CA) and four Spanish–English bilingual study team members from the University of Southern California Mrs. T. H. Chan Division of Occupational Science and Occupational Therapy. Participant respondents (N = 40) met the following inclusion criteria: were age 45 yr or older, lived in the United States, identified as Latino/Hispanic, spoke and read Spanish, and reported one or more chronic health conditions. Those who self-reported a cognitive disorder were excluded. Enrollees provided verbal informed consent to participate following review of an information sheet.
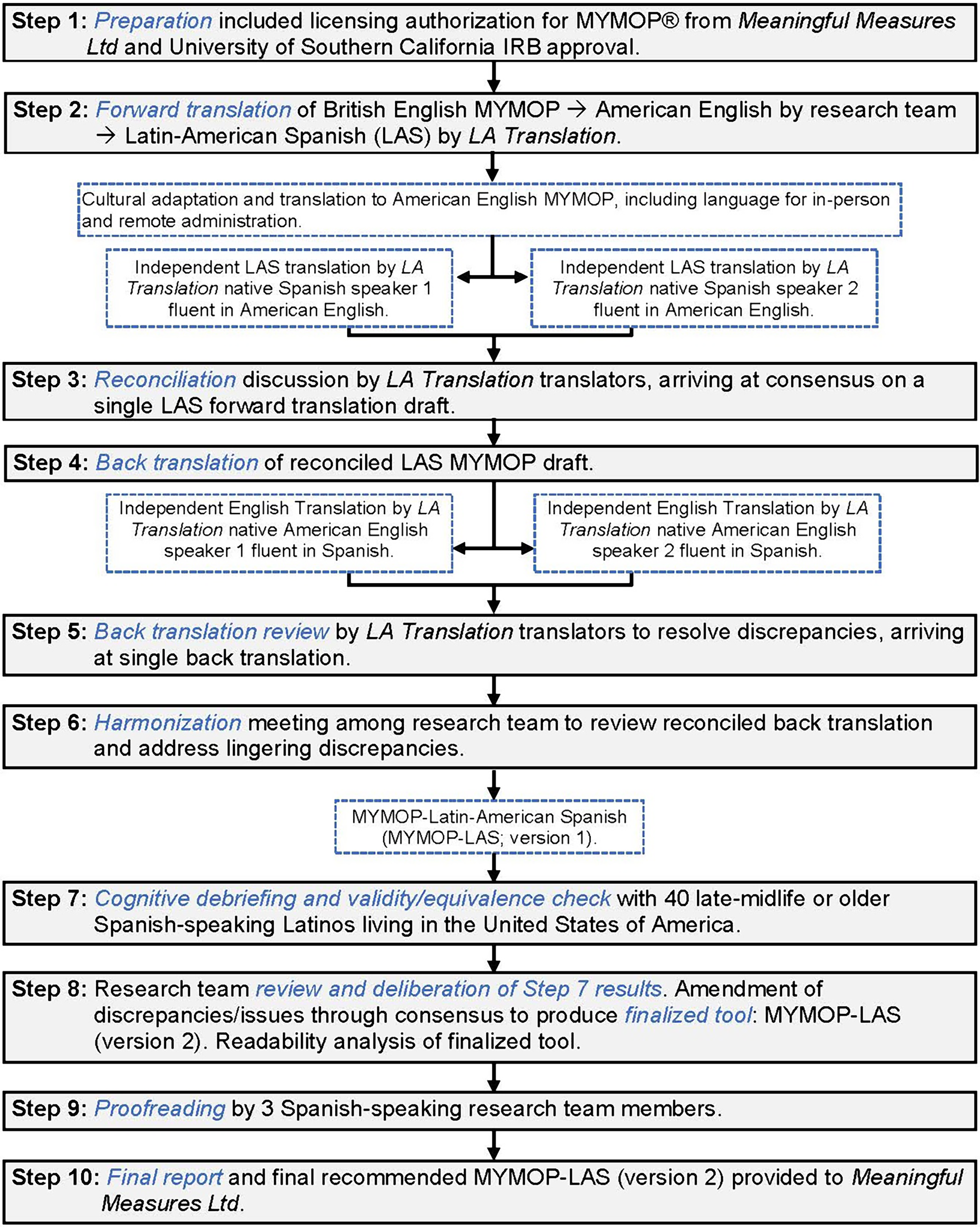
Adaptation process for the MYMOP–LAS according to the Translation and Cultural Adaptation of Patient-Reported Outcomes Measures—Principles of Good Practice (Wild et al., 2005)
We evaluated the construct validity of the MYMOP–LAS (Version 1; using the first form to gauge baseline results only) by comparing it with the Spanish-language EuroQol Five-Dimension Five-Level (EQ–5D–5L; Herdman et al., 2011) tool, which participants self-administered using an online survey before cognitive debriefing. The EQ–5D–5L is a valid and reliable generic measure of health status (Feng et al., 2021) that addresses five dimensions of perceived health (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) at five levels of impairment within a domain (problems: ranging from no to extreme). Cognitive debriefing (Step 7 in Figure 1) required participants to describe their understanding of items on the MYMOP–LAS as they were asked and to make recommendations for changes as relevant.
We measured participants’ demographic characteristics by using a face-valid, study-specific questionnaire and assessed acculturation with the General Acculturation Index–Spanish (Balcazar et al., 1995). We explored the equivalence of administration context by comparing the MYMOP–LAS first-form scores between remote (by telephone or video call; n = 28) and in-person (n = 12) administration.
Readability of the MYMOP–LAS (Version 2) was assessed using three established tools (https://legible.es) specific for analysis of Spanish text: Fernández Huerta, Szigriszt-Pazos, and INFLESZ tests. We compared the results with the American English version’s readability as assessed by the Flesch Reading Ease, Flesch–Kincaid Grade Level, and New Dale–Chall Readability Formula algorithms (https://readabilityformulas.com). Although a fifth- to sixth-grade level is recommended to ensure readability for most of the population, a third- to fifth-grade level is ideal for respondents at risk for limited literacy (Weiss, 2003).
Statistical Analysis
We used descriptive statistics to summarize participant characteristics and first-form responses to the MYMOP–LAS (Version 1) and EQ–5D–5L. We examined the MYMOP–LAS’s construct validity by calculating Pearson correlation coefficients between the MYMOP–LAS profile and its four subscales with the EQ–5D–5L index-based utility scores generated from application of the U.S. value set (Pickard et al., 2019) and with the visual analog scale (EQ–VAS) health rating. Correlations (absolute r values) were interpreted as strong (≥ .7), moderate (.3 to < .7), or weak (< .3). We hypothesized moderate-strength negative correlations among the variables given that the instruments measure similar, but not identical, health-related constructs in oppositely scored directions. Equivalence of remote and in-person administration was evaluated by using independent t tests that compared MYMOP–LAS first-form scores.
Results
Participant Characteristics
Forty adult Latino/Hispanic participants were recruited through flyers placed in the community (in California) and word-of-mouth. Although having a chronic health condition was necessary for study inclusion, respondents were neither from a specific client population nor attending clinics for a particular intervention. The mean age of participants was 61.8 yr (SD = 8.4), and most were female (72.5%), had a high school education or less (55%), identified race as either White (48%) or other (38% qualifying “other” as Mexicano/a), and had lived in the United States for more than 20 yr (82.5%). Participants’ mean acculturation status score was low (M = 1.9, SD = 0.7). Hypertension, diabetes, and arthritis were the most prevalent health conditions reported. Table 1 presents basic descriptive statistics for the MYMOP–LAS and EQ–5D–5L. Table A.1 in the Supplemental Material provides further detail of participant characteristics (available online with this article at https://research.aota.org/ajot).
Means and Standard Deviations for MYMOP–LAS and EQ–5D–5L Scales (N = 40)
Note. EQ–5D–5L = EuroQol Five-Dimension Five-Level; MYMOP–LAS = Latin-American Spanish translation of the Measure Yourself Medical Outcomes Profile.
aScale range from 0 to 6, with lower MYMOP–LAS and higher EQ–5D–5L scores indicating better health and functioning.
b n = 26 identified a second symptom.
Cognitive Debriefing
On the basis of participants’ feedback from cognitive debriefing, we replaced words and phrases that several participants identified as too formal or difficult with more common, everyday terms (e.g., indíqueme [indicate] → dígame [tell me]). Furthermore, the rating scale anchors were simplified from as good as it could be and as bad as it could be to muy bien (very good) and muy mal (very bad). Confusion about what “your problem” was referring to regarding impact on activity was clarified by expanding the phrase to problema de salud (health problem).
Construct Validity
As shown in Table 2, the MYMOP–LAS profile score and three of four subscales were significantly negatively moderately correlated with the Spanish EQ–5D–5L utility index score (r = –.473 to –.519, ps ≤ .013), with the MYMOP–LAS activity impact subscale correlation trending in the hypothesized direction (r = –.282, p = .078). Similar correlations were observed between the MYMOP–LAS profile and same three subscales and the EQ–VAS score (r = –.354 to –.536, all ps ≤ .025).
Pearson Correlations Between MYMOP–LAS (First Form) and EQ–5D–5L Scores (N = 40)
Note. EQ–5D–5L = EuroQol Five-Dimension Five-Level; EQ–VAS = EuroQol visual analog scale; MYMOP–LAS = Latin-American Spanish translation of the Measure Yourself Medical Outcomes Profile.
a n = 26 identified a second symptom.
*p < .05. **p < .01. ***p < .001.
Operational Equivalence
No significant differences were detected between participants who were administered the questionnaire remotely (n = 28) or in person (n = 12) on the MYMOP–LAS profile or any subscales (all ps > .5, mean d effect size ≈ 0.10), supporting operational equivalence.
Readability
Results from the readability analysis demonstrated that the MYMOP–LAS (Version 2) produced acceptable readability outcomes. Across the three Spanish readability algorithms, the MYMOP–LAS had on average a fifth-grade readability level, which is comparable with the American English MYMOP (see Table A.2 for details).
Discussion
This study aimed to develop and culturally adapt a Latin-American Spanish translation of the MYMOP for Spanish-speaking people living in the United States. The resulting MYMOP–LAS demonstrated construct validity, readability, and operational equivalence across remote and in-person administration.
On the basis of cognitive debriefing and subsequent synthesis of participant critiques and suggested refinements, the first version of the MYMOP–LAS was generally comprehensible to participants but benefited from integration of more colloquial language and terminology used by Spanish-speaking Latinos to make it more accessible to the community. A significant proportion of our study sample had less than a high school education and low acculturation to American culture, both factors associated with low health literacy (Calvo, 2016; De Alba et al., 2019). This underscores the importance of prioritizing feedback about clarity.
The revisions made to the first version of the MYMOP–LAS, such as simplifying wording, illustrated our responsivity to issues of accessibility. Participants also remarked that asking individuals to assign a positive response to a seemingly negative symptom was not logical (e.g., rating pain “as good as it could be” insinuates that pain is good at some level). Although replacing the anchors with simplified language addressed the former critique, we could not resolve the latter issue because of the requirements for operational equivalence by Meaningful Measures Ltd. (Bristol, England). A team in Brazil that had translated a pre-licensed MYMOP into Brazilian Portuguese encountered similar issues with the scale anchors (Barbosa Lima et al., 2016). To improve understandability and alignment with rating problematic symptoms (or their absence), unconstrained by a licensure agreement, the team adapted the anchors to 0 = none and 1 = bearable through 6 = unbearable. Future research may want to consider a comparable adaptation for the MYMOP–LAS to be fully responsive to the U.S. Spanish-speaking community. Nevertheless, the final recommended MYMOP–LAS (Version 2) features familiar terminology and demonstrates acceptable readability, which will make the tool accessible even to those with limited literacy (Weiss, 2003).
The construct validity of the initial MYMOP–LAS form was supported with moderately strong, significant negative correlations with the EQ–5D–5L quality of life questionnaire, in which good health is noted by low scores on the MYMOP–LAS and high scores on the EQ–5D–5L. One subscale of the MYMOP–LAS, the activity impact score, resulted in a weak, nonsignificant correlation, although trending in the hypothesized direction. Our findings track with other validation studies. Brazilian Portuguese–adapted and German-adapted MYMOP tools demonstrated moderately strong negative correlations with the EQ-5D (Barbosa Lima et al., 2016; Hermann et al., 2014). Along similar lines, a study of the original MYMOP (Paterson, 1996) and a Chinese-adapted version (Chung et al., 2010) showed comparable associations with the 36-item Short Form Health Survey of well-being at baseline.
Finally, preliminary investigation comparing MYMOP–LAS profile and subscale scores of participants who completed the questionnaire remotely and those completing it in person yielded no significant difference between groups. To our knowledge, this is the first study showing preliminary support for the operational equivalence of survey administration methods for the MYMOP. Although further study is needed because of statistical power considerations, having flexibility to administer the MYMOP–LAS remotely is timely given trends in telehealth expansion (Ndwabe et al., 2024).
Limitations
This study had several limitations. First, the sample was nonrandom and relatively small, which potentially restricts generalization of the findings to ethnic subgroups, such as Puerto Ricans or individuals living on the U.S. East Coast. Despite this drawback, the results underscore the essential validity of the MYMOP–LAS as demonstrated by a consistent pattern of large, statistically significant correlations with an alternate, well-accepted health status measure. Second, cognitive debriefing questions were inserted between questionnaire items, which may have altered participants’ responses to and critique of the instrument. Third, data were collected cross-sectionally rather than repeatedly as intended for standard administration during an intervention study. Although we could not test sensitivity to change, it should be noted that the MYMOP follow-up form, which we also successfully translated, is nearly identical to the MYMOP baseline form, and it is therefore highly likely that the translated follow-up form has similar construct validity. Last, the finalized version of the MYMOP–LAS was not tested, although we anticipate that the finalized tool will likely have slightly superior psychometric properties.
Conclusion
Translation and cultural adaptation of the original MYMOP according to Wild et al.’s (2005) principles of good practice resulted in a valid, readable, and operationally equivalent Latin-American Spanish tool—the MYMOP–LAS—ready for use with the U.S. Spanish-speaking Latino population. Given that the patient-centered MYMOP–LAS is condition agnostic with a focus on well-being, occupational therapy practitioners may find this tool useful for Spanish-speaking clients in settings such as primary care or to demonstrate change following health- and wellness-focused intervention. Further studies on the final recommended instrument’s measurement properties are warranted, including studies with larger sample sizes that involve clients who are assessed both before and after receiving services within varied health care settings.
Supplemental Material
Supplementary material for Developing and Validating the Latin-American Spanish Version of the Measure Yourself Medical Outcome Profile® (MYMOP–LAS)
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051021.pdf for Developing and Validating the Latin-American Spanish Version of the Measure Yourself Medical Outcome Profile® (MYMOP–LAS) by Stacey L. Schepens Niemiec, Jesús Díaz, Celso Delgado, Mike Carlson and Jocelyn Arteaga in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
MYMOP® has been copyrighted and licensed by Meaningful Measures Ltd since 2020. Anyone wishing to use MYMOP must contact ![]() for a license and the updated MYMOP version. This study was supported by the USC Chan Division of Occupational Science and Occupational Therapy—Summer Funding for Innovative Research Projects. We thank Laura Guzmán, Lorena Alvarado, and Dayannara Campos Medina for their assistance with recruitment and data collection for this study.
for a license and the updated MYMOP version. This study was supported by the USC Chan Division of Occupational Science and Occupational Therapy—Summer Funding for Innovative Research Projects. We thank Laura Guzmán, Lorena Alvarado, and Dayannara Campos Medina for their assistance with recruitment and data collection for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.