
Abstract
To address concerns regarding previous reviews that used varied and inconsistent definitions of ASI interventions and arrived at mixed conclusions, this review focused exclusively on high-level studies of ASI that adhered to the ASI Fidelity Measure.
Sensory integration is the neurological process through which sensory information is organized in the central nervous system (CNS), enabling the interpretation of the surrounding environment and understanding of the body within that environment (Ayres, 1972). Ayres proposed that sensory integration difficulties can affect the academic development and motor gains of children with learning impairments (Ayres, 1972, 1976) and autistic children (Ayres & Tickle, 1980). Her theory explains how differences in sensory processing, in the absence of peripheral or CNS damage or cognitive deficits, can affect occupational performance (Bundy & Lane, 2020).
Sensory integrative difficulties (Bundy & Lane, 2020), also known as sensory processing disorders (Miller, Anzalone, et al., 2007), are difficulties with sensory perception, sensory–motor integration, and sensory reactivity. These challenges have a prevalence of 5% to 10% among children without disabilities (Ahn et al., 2004) and are particularly common among autistic children, with a prevalence of 45% to 96% (Ben-Sasson et al., 2009; Lane et al., 2010; Schaaf et al., 2014).
Ayres developed a sensory integration intervention to address the sensory and motor factors that affect the ability to participate fully in activities, tasks, and occupations (Ayres, 1972, 1976; Ayres & Tickle, 1980). This intervention is based on a systematic process that includes assessment of the sensory and motor factors affecting the child’s postural control, self-regulation, motor coordination, bilateral integration, and praxis, with a particular emphasis on tactile, vestibular, and proprioceptive processing (Bundy & Lane, 2020; Fisher & Murray, 1991; Schaaf & Mailloux, 2015). Although this approach has mainly been studied with autistic children (Schaaf et al., 2018; Schoen et al., 2019), studies have also been conducted with children who have experienced trauma (Joseph et al., 2021), children with cerebral palsy (Cemali et al., 2022; Kantor et al., 2022), children with Down syndrome (Uyanik et al., 2003), and children born prematurely (Lecuona et al., 2017; Pekçetin et al., 2016).
It is important to note the distinction between the intervention developed by Ayres and other sensory-based interventions, which is not always made clear in the literature (Watling & Hauer, 2015). Sensory-based intervention is an overarching term for approaches and strategies that address sensory aspects (Kantor et al., 2022). However, Ayres Sensory Integration® (ASI) intervention differs from other sensory-based approaches because it involves active, individually tailored, sensory–motor activities, contextualized in play at the just-right challenge to improve adaptive responses as a basis for participation in activities, tasks, and occupations (Parham et al., 2007; Schaaf & Mailloux, 2015). Overlooking this distinction can lead to confusion when interpreting research results (Watling & Hauer, 2015). Therefore, the term ASI was trademarked to distinguish the intervention that adheres to Ayres’s theoretical framework and differentiate it from sensory-based interventions in general (Smith Roley et al., 2007). Moreover, the ASI Fidelity Measure™ (ASIFM; May-Benson et al., 2014; Parham et al., 2007, 2011) identifies the structural and process elements of ASI and measures adherence to them in research and practice. The structural elements establish requirements for clinician training and mentoring, room and equipment characteristics, and communication with stakeholders. Ten identified process elements guide the delivery of ASI intervention: (1) ensuring physical safety; (2) presenting sensory opportunities; (3) helping to maintain appropriate levels of alertness; (4) challenging postural, ocular, oral, or bilateral motor control; (5) challenging praxis and organization of behavior; (6) collaborating in activity choice; (7) tailoring activity to present just-right challenges; (8) ensuring that activities are successful; (9) supporting the child’s intrinsic motivation to play; and (10) establishing a therapeutic alliance.
Despite registering the term ASI as a trademark, and the introduction of the ASIFM, the ASI approach has continued to be inconsistently defined in the literature (Bundy & Lane, 2020). In an editorial discussion published in the Australian Occupational Therapy Journal, Rodger et al. (2012) cautioned that using sensory approaches (including ASI) that lacked robust evidence would be a disservice to the occupational therapy profession. To that editorial, Bundy et al. (2013) replied that therapists criticizing ASI were using incorrect definitions, leading to inaccurate conclusions regarding its effectiveness. These differing views highlight the debate about whether ASI is effective.
In recent years, several reviews assessing ASI’s effectiveness with children have been conducted (e.g., Case-Smith et al., 2015; Lang et al., 2012; May-Benson & Koomar, 2010; Novak & Honan, 2019; Schaaf et al., 2018; Schoen et al., 2019). Conclusions have been mixed, in part because of inconsistent definitions of sensory integration, mixed methodologies, and varied methodological quality. Some of the previous systematic reviews claiming to assess the effects of ASI have also included studies investigating sensory-based approaches that do not meet fidelity for ASI. For example, in Lang et al.’s (2012) systematic review of sensory integration with autistic children, more than half of the studies included in the review investigated the effect of weighted vests, therapy ball chairs, massage, or brushing procedures. The authors of the reviewed studies did not claim to be using ASI, and their interventions could be better described as sensory stimulation or sensory-enriched programs. Although these approaches may complement ASI, they do not represent the intervention proposed by Ayres and, by themselves, should not be used to judge the efficacy of ASI (Bundy & Lane, 2020). Nevertheless, Lang et al. (2012) concluded that the evidence does not support the implementation of ASI with autistic children.
Similarly, Novak and Honan’s (2019) systematic review of occupational therapy interventions with children concluded that therapists should avoid using ASI with autistic children. However, similar to Lang et al. (2012), they defined sensory integration as “sensory diets, swinging, brushing, therapy balls, weighted vests, and body socks” (p. 261). Once again, these are sensory-based interventions, but they are not representative of ASI.
In contrast, Schaaf et al.’s (2018) systematic review suggested that ASI can benefit autistic children’s achievement of individualized goals related to function and participation. Similarly, Schoen et al.’s (2019) systematic review concluded that ASI meets the criteria for an evidence-based practice for autistic children. Notably, both these reviews only included studies that adhered to the ASIFM.
Because of the inconsistencies highlighted in the available literature, this systematic review evaluates the efficacy of ASI with children ages 0 to 12 yr based on the outcomes reported from randomized controlled trials (RCTs) adhering to fidelity and comparing ASI with treatment as usual, other treatments, or no treatment.
Method
This systematic review, registered in PROSPERO (CRD42022346191), followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). The final search, completed in June 2024, encompassed the Cochrane Central Register of Controlled Trials, MEDLINE, CINAHL, PsycINFO, and Embase. Additionally, a manual search was conducted by scanning the reference lists of all included studies and relevant systematic reviews. The search strategy, developed in consultation with a librarian and adapted for each database, is available in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Selection Criteria
Studies included were RCTs published in the peer-reviewed scientific literature from the inception of each database until June 2024; were reported in English; established and maintained fidelity to the Ayres theoretical framework, including those interventions delivered along with other frameworks; and were conducted with children ages 0 to 12 yr.
Fidelity Assessment
We screened RCTs from the inception date of each database. Therefore, some screened studies were published before the ASIFM was first available in 2007.
To assess whether studies published before 2007 adhered to Ayres’s theoretical framework, we considered the core principles of ASI published by Parham et al. (2007) as the minimum required to describe ASI, because they were the first fidelity tool and the best available research to define ASI in the early literature. We used a checklist of the 10 core principles of ASI following Parham et al. (2007), and studies published before 2007 were excluded if they did not mention all 10 principles when describing the intervention. Notably, the initial version (Parham et al., 2007), in contrast to the most recent one (Parham et al., 2011), does not include the item “challenging postural, ocular, and bilateral development” (p. 136).
Studies published after 2007 were only included in this review if they explicitly stated adherence to the ASIFM (Parham et al., 2007, 2011), regardless of whether they provided details on how adherence to fidelity was assessed.
Data Extraction and Synthesis
Search citations were imported to Covidence software, and duplicates were automatically eliminated. Two authors, Carolina Acuña (occupational therapist, certified in ASI with 10 yr experience) and Jacqui Barfoot (occupational therapist with more than 20 yr experience working with children but no experience in ASI), independently conducted the screening by title, abstract, and full text. Jessica Hill (occupational therapist with 11 yr experience working with children but no experience in ASI) resolved disagreements. Acuña and Sebastian Gallegos-Berrios (occupational therapists with 14 yr experience and introductory training in ASI) independently conducted data extraction guided by the Template for Intervention Description and Replication (TIDieR) Checklist (Hoffmann et al., 2014).
Analysis
Each study was assessed for risk of bias using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2; Sterne et al., 2019). The assessment was conducted independently by Acuña and Gallegos-Berrios, and interrater reliability (Cohen’s κ) was calculated using an R statistical environment (R Core Team, 2022). When necessary, Hill resolved disagreements. Levels of evidence were assigned based on standards developed by the Oxford Centre for Evidence-Based Medicine (OCEBM Levels of Evidence Working Group, 2009). RCTs were rated as Level 1b (well-designed individual RCT) or 2b (low-quality RCT, such as a pilot or feasibility study with a small sample size). The strength of evidence (level of certainty) was determined on the basis of U.S. Preventive Services Task Force (2012) guidelines.
Results
Data Extraction
Figure 1 presents the PRISMA flow diagram. A total of 174 articles were screened, and 50 studies underwent full-text review. During this review, the eligibility of the RCTs, based on their adherence to ASI fidelity, was evaluated last, after studies were excluded for other criteria. Of 22 RCTs that otherwise met the inclusion criteria, 13 were excluded because of uncertainty about their adherence to ASI fidelity; six RCTs published before 2007 (Densem et al., 1989; Humphries et al., 1990, 1992, 1993; Wilson et al., 1992; Ziviani et al., 1982) and seven studies published after 2007 (Faramarzi et al., 2016; Ganapathy Sankar, 2015; Ganapathy Sankar et al., 2020; Ning & Wang, 2021; Shamsoddini, 2010; Shamsoddini & Holisaz, 2009; Wójtowicz et al., 2021). Additionally, searches run in June 2024 identified another two RCTs that were excluded because of uncertainty about their adherence to the ASIFM (Baharian et al., 2023; Lv et al., 2023). Ultimately, nine RCTs were included in the review.
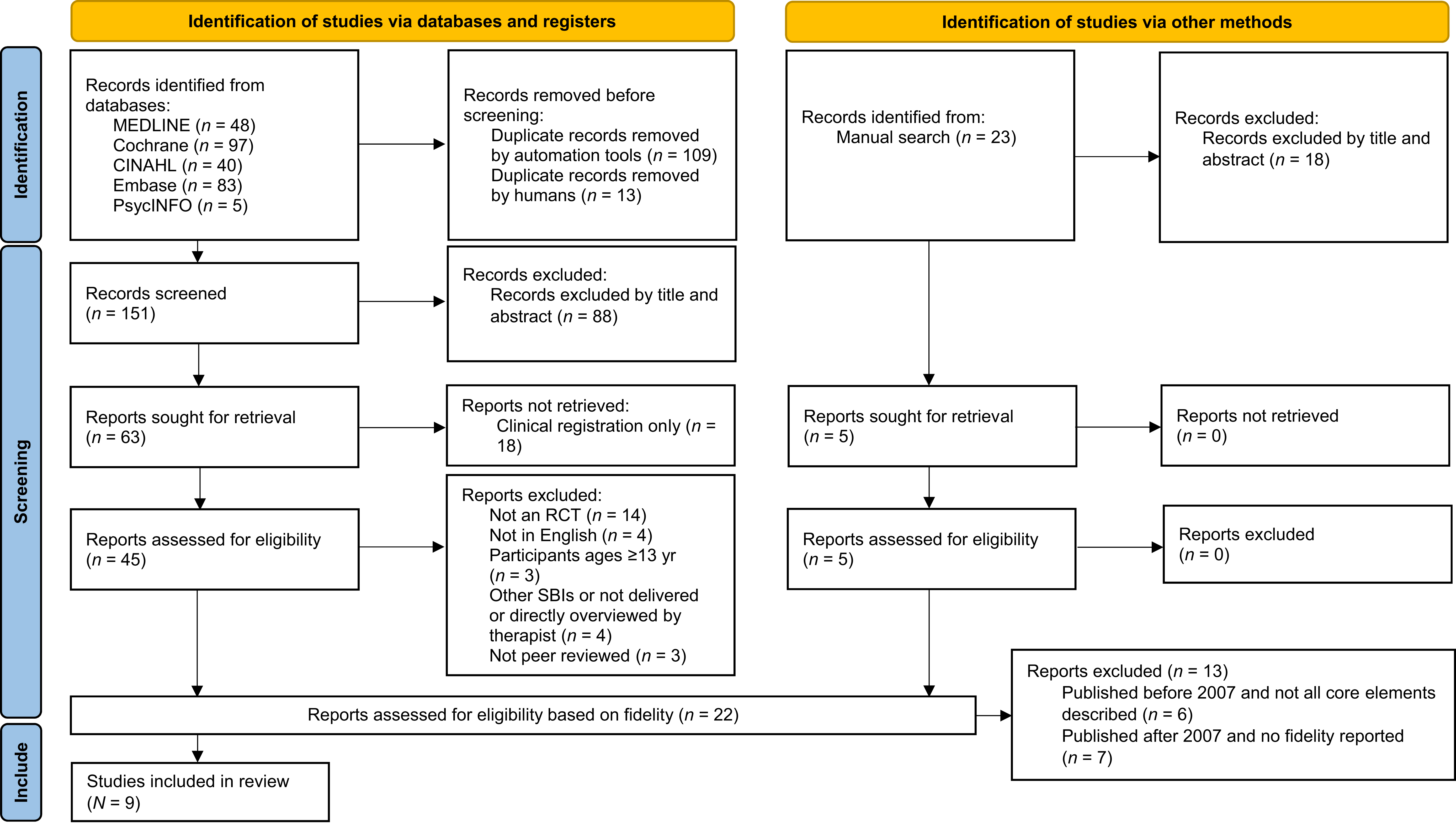
Flow of RCTs included in and excluded from this systematic review.
Study Characteristics
The nine included RCTs were published between 2007 and 2022 and represented a total of 344 participants. Six studies were conducted with autistic children, mostly male, between 3.9 and 12.0 yr (Dunbar et al., 2012; Kashefimehr et al., 2018; Omairi et al., 2022; Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014). The remaining three studies were performed with children with sensory modulation disorder (Miller, Coll, & Schoen, 2007), prematurity (Lecuona et al., 2017), or cerebral palsy and cortical vision impairment (Cemali et al., 2022).
In terms of the intervention’s characteristics, all ASI sessions were individualized and performed by occupational therapists face to face in therapy rooms. The length of sessions ranged between 45 and 60 min, and the frequency varied from one to three sessions per week. Most studies reported interventions conducted over a 10- to 12-wk period. However, two studies provided shorter interventions. All included studies claimed to follow ASIFM, but not all specified how they ensured this; those reporting mean fidelity ratings demonstrated high credibility for ASI (Lecuona et al., 2017; Omairi et al., 2022; Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014). Overall participant and study characteristics are included in Table A.2 in the Supplemental Material. A detailed description of ASI interventions in the included RCTs guided by the TIDieR Checklist is available in Table A.3.
Outcomes
Outcomes are presented separately for (1) studies relating to autistic children and (2) studies reporting on other child populations. A summary of the evidence is presented in Table A.2.
Findings for Autistic Children
Four studies were RCTs (Level 1b; Kashefimehr et al., 2018; Omairi et al., 2022; Randell et al., 2022; Schaaf et al., 2014), and the other two were pilot RCTs (Level 2b; Dunbar et al., 2012; Pfeiffer et al., 2011). All studies aimed to evaluate the effectiveness of occupational therapy using ASI compared with usual care (Omairi et al., 2022; Randell et al., 2022; Schaaf et al., 2014), routine school occupational therapy (Kashefimehr et al., 2018), sensory–motor activities in the classroom (Dunbar et al., 2012), and fine motor intervention (Pfeiffer et al., 2011). In addition to ASI’s clinical effect, Randell et al. (2022) intended to evaluate ASI’s cost effectiveness. The outcomes assessed included individualized goals related to occupational performance, function, and participation; outcomes related to behaviors of concern; and outcomes related to functional and developmental skills, along with assistance needed for the child to participate fully and career stress and quality of life.
Individualized goals.
Five studies (Kashefimehr et al., 2018; Omairi et al., 2022; Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014) reported statistically significant gains in individualized goals related to occupational performance, function, and participation. Omairi et al. (2022), Pfeiffer et al. (2011), and Schaaf et al. (2014) found that the ASI group scored statistically significantly higher than the control groups on goal attainment scaling (GAS; Kiresuk & Sherman, 1968; Kiresuk et al., 1994; Ruble et al., 2012). In these studies, the GAS goals represented a wide range of outcome areas such as sensory processing and regulation, social–emotional function (Pfeiffer et al., 2011), self-care, sitting, daily routine, meal preparation, community participation, communication, self-stimulatory behaviors, emotional regulation, gross motor and praxis, safety, sleep (Schaaf et al., 2014), dressing, bathing, feeding, school participation, sports participation (Omairi et al., 2022), fine motor skills (Pfeiffer et al., 2011; Schaaf et al., 2014), and play (Omairi et al., 2022; Schaaf et al., 2014). As a result of the diversity of the goal areas across the studies when using GAS, it was not possible to establish further comparisons. Kashefimehr et al. (2018) measured individualized goals using the Short Child Occupational Profile (SCOPE; Bowyer et al., 2008). This study indicated statistically significantly greater improvement among the ASI group than among the group receiving routine school occupational therapy on all domains of the SCOPE. These goals were mainly related to communication, interaction, and process skills. Similarly, Randell et al. (2022) reported that the ASI group showed a statistically significant increase in carer-rated and child-rated performance and satisfaction scores from pre- to posttest on the Canadian Occupational Performance Measure (Law et al., 1990). These goals were related to occupational performance and participation problems identified by carers and children.
Behaviors of concern.
Three studies (Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014) reported on outcomes related to behaviors of concern, such as resistance to change, arousal regulation issues, irritability, hyperactivity, social withdrawal, noncompliance, and inappropriate speech. Randell et al. (2022) used the Aberrant Behavior Checklist (Aman & Singh, 1986), and Schaaf et al. (2014) used the Pervasive Developmental Disorders Behavior Inventory (Cohen et al., 2003); both reported no statistically significant differences between ASI and usual care. Similarly, Pfeiffer et al. (2011) reported nonsignificant changes between ASI and alternative intervention groups on the Social Responsiveness Scale (SRS; Constantino & Gruber, 2005), with the exception that the ASI group exhibited significantly fewer autistic mannerisms on a subscale of the test.
Functional and developmental skills.
All studies assessed outcomes related to specific functional and developmental skills. Outcomes and tools to measure them varied across the studies. These outcomes were related to self-care skills, communication abilities, social functioning, play, motor skills, and sensory processing function, along with caregiver assistance and modifications needed for the child to participate fully, caregivers’ stress, and quality of life.
Three studies (Kashefimehr et al., 2018; Omairi et al., 2022; Pfeiffer et al., 2011) measured outcomes related to sensory processing function. Omairi et al. (2022) found a statistically significant change (improvement) for the ASI group on some of the Sensory Integration and Praxis Tests (Ayres, 1989). The same study (Omairi et al., 2022) reported a statistically significant decrease in sensory processing difficulties for the ASI group on the Sensory Processing Measure (SPM; Parham & Ecker, 2007), whereas for the control group, challenges slightly increased or remained unchanged. Similarly, Kashefimehr et al. (2018) reported that the ASI group showed a statistically significantly greater change than the control group on most Sensory Profile (SP; Dunn, 1999) domains except for Emotional Reactions and Emotional/Social Responses. However, Pfeiffer et al. (2011) found statistically nonsignificant differences between groups for sensory processing standardized scores on the SPM.
Two studies (Omairi et al., 2022; Schaaf et al., 2014) used the Pediatric Evaluation of Disability Inventory (PEDI; Haley et al., 1992) and reported statistically significantly greater improvement for the ASI group than the usual-care group on self-care caregiver assistance and social function caregiver assistance (Schaaf et al., 2014) and on self-care and social function (Omairi et al., 2022).
Dunbar et al. (2012) used the Revised Knox Play Scale (Knox, 1997) and reported improvements in play skills for both the ASI group and a group receiving sensory–motor activities in the classroom. However, the statistical significance was not calculated.
Additionally, studies found statistically nonsignificant differences between ASI and control groups on various outcome measures. Pfeiffer et al. (2011) found nonsignificant differences in motor skills using the Quick Neurological Screening Test (Mutti et al., 1998), and Randell et al. (2022) found nonsignificant change in quality of life and carers’ stress as assessed with the EuroQol–5 Dimensions (Herdman et al., 2011), Carer Quality of Life (Brouwer et al., 2006), and Autism Parenting Stress Index (APSI; Silva & Schalock, 2012). Moreover, two studies (Randell et al., 2022; Schaaf et al., 2014) found no differences between groups on the Vineland Adaptive Behavior Scales, Second Edition (VABS2; Sparrow et al., 1996, 2005), which measure communication, daily living, and socialization composites. The exception was that Randell et al. (2022) found a decline in scores in the Communication domain for the ASI group at 12 mo; however, they also noted inaccuracies in the assessment’s implementation.
As shown in Table A.4, five RCTs (Kashefimehr et al., 2018; Omairi et al., 2022; Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014), four of them Level 1b, found that ASI resulted in autistic children’s improvements on individualized goals, indicating strong strength of evidence for this approach. In contrast, three RCTs (Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014), two of them Level 1b, indicated no statistically meaningful changes in outcomes related to behaviors of concern (except for an SRS subscale), resulting in moderate strength of evidence, suggesting the ASI approach’s lack of effect for outcomes such as resistance to change or irritability. In terms of specific functional and developmental skills, evidence is mixed. Although two RCTs (Omairi et al., 2022; Schaaf et al., 2014) reported improvements on the Self-Care and Socialization domains measured with the PEDI, two RCTs (Randell et al., 2022; Schaaf et al., 2014) indicated no statistical change in VABS2 scores. Moreover, other nonsignificant findings were reported by individual studies, including motor skills (Pfeiffer et al., 2011), career stress, and quality of life (Randell et al., 2022). Additionally, two RCTs (Kashefimehr et al., 2018; Omairi et al., 2022) reported significant improvements in sensory processing function, but one RCT (Pfeiffer et al., 2011) found nonsignificant change. Conflicting effects among individual studies result in low strength of evidence for functional and developmental skills. Table A.4 shows the strength of evidence for ASI’s effect on autistic children’s outcomes.
Findings for Other Child Populations
Miller, Coll, and Schoen (2007) conducted a pilot RCT (Level 2b) with children with sensory modulation disorder, comparing the ASI group with an activity protocol group and a no-treatment group. They reported statistically significantly greater gains for the ASI group than the other two groups on GAS (Kiresuk et al., 1994). Additionally, they reported that the ASI group significantly increased scores on the Attention and Cognitive/Social subscales compared with the children in the other groups as measured with the Leiter International Performance Scale–Revised (Roid & Miller, 1997). Change scores were not significant for the Short SP (McIntosh et al., 1999a), the Child Behavior Checklist (Achenbach, 1991), and the Vineland Adaptive Behavior Scales Socialization subtest (Sparrow et al., 1984). A tendency toward reduced hyperreactivity was observed for the ASI group on the Electrodermal Reactivity Test (Mangeot et al., 2001; McIntosh et al., 1999b; Miller et al., 1999), but the changes were not significant, and missing data were reported for this test.
Lecuona et al. (2017) conducted an RCT (Level 1b) with premature infants, comparing the ASI and no-treatment groups. They reported statistically significant differences favoring the ASI group’s receptive communication and fine motor skills using the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley, 2006). Sensory processing outcomes were measured with the Infant/Toddler SP (Dunn, 2002) and the Test of Sensory Functions in Infants (TSFI; DeGangi & Greenspan, 1993). Although sensory processing improvements were reported in the ASI group, statistical significance was not presented.
Cemali et al. (2022) conducted an RCT (Level 1b) with infants with cerebral palsy and cortical vision impairment. The experimental group received ASI and physiotherapy, and the control group received physiotherapy only. They reported statistically significant changes in both groups. The ASI group showed a statistically significantly greater improvement on the TSFI in sensory processing than the control group, except for oculomotor skills (Aracikül, 2014; DeGangi & Greenspan, 1989). Nonsignificant differences were found for motor gains between groups on the Alberta Infant Motor Scale (Piper et al., 1992).
Risk-of-Bias Assessment
The risk of bias for each study was assessed using RoB 2 with an interrater reliability (Cohen’s κ) of .84. The quality appraisal of the studies is presented in Table A.5. In summary, six studies presented some bias concerns (Lecuona et al., 2017; Miller, Coll, & Schoen, 2007; Omairi et al., 2022; Pfeiffer et al., 2011; Randell et al., 2022; Schaaf et al., 2014), and three other RCTs presented a high risk of bias (Cemali et al., 2022; Dunbar et al., 2012; Kashefimehr et al., 2018). Among studies, the following challenges were commonly found to introduce a risk of bias: (1) difficulties blinding carers when using caregiver-reported outcome measures; (2) lack of evidence that the allocation was concealed until children were allocated to experimental or control groups; and (3) unavailability of researchers’ prespecified intentions, such as published research protocols, resulting in a lack of evidence that planned outcome measurements and analysis intentions preceded the availability of unblinded outcome data to the trial researchers.
Discussion
The ongoing debate about the use of ASI treatment in occupational therapy and the mixed conclusions of previous systematic reviews underscores the need to evaluate the efficacy of ASI, conducted with fidelity and reported from RCTs, for autistic children and broader populations. Overall, strong evidence indicates that ASI supports achievement and is therefore recommended to address individualized goals related to occupational performance, function, and participation for autistic children with sensory processing differences. This result is unlikely to be challenged by further research. In contrast, moderate evidence suggests that ASI has no effect and is therefore not recommended to address outcomes related to behaviors of concern, such as resistance to change and irritability. This finding might be challenged or strengthened by further research. Although some benefits were reported for self-care, socialization, and sensory processing function for autistic children, the evidence for specific functional and developmental skill outcomes is conflicting, and more research is needed to be confident about the observed results.
Remarkably, to determine the effect of the intervention, all studies with autistic children compared ASI with usual care or other treatments rather than no treatment. Therefore, the observed effects are more likely attributable to the specific impact of ASI. However, although most studies conducted with autistic children concluded that evidence supported benefits for this population when implementing ASI, Randell et al. (2022) expressed uncertainty regarding whether changes were observed in addition to usual care. More important, Randell et al.’s (2022) primary outcome was related to behaviors of concern (irritability and agitation), and the lack of improvement in these behaviors may have influenced their conclusions. Moreover, Randell et al. (2022) did not measure individualized occupational performance outcomes for the control group, limiting the possibility of comparing changes between groups.
Notably, in studies with autistic children, the reported gains were obtained with a therapy frequency of two to three weekly sessions. This frequency should be considered to support similar outcomes in clinical practice. Interestingly, although two studies (Kashefimehr et al., 2018; Omairi et al., 2022) reported that ASI resulted in significant improvements in sensory processing function over a 10- to 12-wk period, a shorter intervention (6 wk; Pfeiffer et al., 2011) did not lead to significant changes in sensory processing outcomes, suggesting that 6 wk may not be sufficient to see improvements in sensory processing.
In keeping with the recommendations of the American Occupational Therapy Association (AOTA; Gillen et al., 2019), all studies with autistic children identified and documented participants’ sensory processing differences and tailored the intervention to each child’s specific needs. Because of the individualized nature of ASI intervention when adhering to fidelity, outcome measures focused on individual goals may be better suited to capturing progress and detecting changes. Therefore, an information-gathering process that identifies the child’s and caregiver’s concerns, and develops and addresses individualized goals driven by client priorities, seems important for clinical practice.
Additionally, most of the studies performed with autistic children (except Dunbar et al., 2012) included measures related to specific developmental skills, as well as individualized goals related to occupational performance, function, and participation outcomes. Measuring the effect of the intervention at proximal (performance components) and distal (occupational performance) levels seems important not only to better understand the effect of the intervention but also because distal outcomes are generally caregiver-reported measures. When conducting research, blinding caregivers to their child’s intervention condition is not feasible. This knowledge could influence caregiver-reported outcomes, introducing risk of bias.
Unlike previous systematic reviews, this review did not limit participants’ inclusion solely to autistic children. Even so, we found only three single RCTs conducted with other child populations (Cemali et al., 2022; Lecuona et al., 2017; Miller, Coll, & Schoen, 2007). Although these studies reported benefits in underlying skill development for their population of interest, more research is needed to support observed outcomes and confidently extend the use of this approach beyond autistic children.
It is important to note that two of the three studies conducted with other child populations (Cemali et al., 2022; Lecuona et al., 2017) did not specify sensory processing differences as an inclusion criterion. Although they assessed sensory processing, it was unclear whether all participants exhibited such differences. Following AOTA’s Choosing Wisely® recommendations, it is necessary to assess and document clients’ specific patterns of dysfunction because treatments that do not target these individualized patterns may lead to ineffective outcomes (Gillen et al., 2019). Therefore, in future studies and clinical practice, individuals’ specific sensory processing differences should be identified before ASI is provided. Additionally, the same two studies (Cemali et al., 2022; Lecuona et al., 2017) focused their evaluations solely on specific developmental skills, such as motor skills and sensory processing. Measuring only specific developmental skills poses limitations, because it does not measure changes in overall occupational performance, leaving the functional benefits of the intervention uncertain. In contrast, in the other study with other child populations, Miller, Coll, and Schoen (2007) characterized participants’ sensory processing differences and assessed individualized goals and skill development. Interestingly, similar to the group of studies with autistic children, Miller, Coll, and Schoen (2007) reported that children with sensory modulation disorders who received ASI made significant gains in individualized goals measured with GAS.
On the basis of the results of this systematic review, future research and practice should use a precise definition of ASI and adhere to fidelity; consider ASI only for children presenting with sensory processing differences that interfere with occupational performance, function, and participation; clearly characterize patterns of sensory processing differences to ensure that intervention addresses client-specific needs; and continue to use individualized goals along with other measures to assess the effect of the intervention.
Limitations
The fidelity assessment used in study selection severely limited the number of studies included. This was expected, because the ASIFM was introduced in 2007, so earlier studies were not likely to meet fidelity criteria. Although all included studies stated that they followed the ASIFM, four studies did not report mean rating values of fidelity adherence, making it impossible to assess those studies’ adherence to ASI. The restriction to studies published in English also means that publications in other languages may have been overlooked. The heterogeneity among studies prevented meta-analysis, imposing methodological limitations. Additionally, bias concerns persisted for most of the included studies, warranting caution in interpreting the results.
Implications for Occupational Therapy Research and Practice
This study has the following implications for occupational therapy research and practice: ▪ ASI may support the achievement of individualized goals related to occupational performance, function, and participation for autistic children who present with sensory processing differences. ▪ ASI is not recommended for addressing outcomes related to autistic children’s behaviors of concern, such as irritability. ▪ ASI appears to have benefits for functional and developmental skills for autistic children and other child populations; further research is needed to be confident in the observed outcomes.
Conclusion
When assessing the effects of ASI by conducting studies or systematic reviews, it is imperative that the intervention performed truly aligns with ASI and does not inadvertently involve concepts that fall short of fidelity criteria. Failure to maintain fidelity in defining and implementing ASI can result in inaccurate interpretations. Overall, when performed with fidelity, strong evidence suggests that ASI enhances autistic children’s individualized goals related to occupational performance, function, and participation. However, the current state of evidence does not support its use to address behaviors of concern, such as resistance to change or irritability. Additionally, emerging research shows some specific functional and developmental benefits of ASI for autistic children and broader child populations; further research is needed to be confident in the observed outcomes.
Supplemental Material
Supplementary material for Ayres Sensory Integration® With Children Ages 0 to 12: A Systematic Review of Randomized Controlled Trials
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051023.pdf for Ayres Sensory Integration® With Children Ages 0 to 12: A Systematic Review of Randomized Controlled Trials by Carolina Acuña, Sebastian Gallegos-Berrios, Jacqui Barfoot, Pamela Meredith and Jessica Hill in The American Journal of Occupational Therapy
Footnotes
*
Indicates articles included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.