
Abstract
This review examines different interventions used by occupational therapists to minimize the impact of cognitive decline.
Mild cognitive decline is a deterioration in a person’s cognitive function that cannot be attributed to another mental disorder (e.g., delirium, major depressive disorder, or schizophrenia; American Psychiatric Association, 2013). Mild cognitive decline falls under the broader umbrella of cognitive decline, which spans from mild to moderate to severe cognitive decline. However, the current literature varies on how severities of cognitive decline are defined or identified (Petersen et al., 2014). For example, some studies use subjective or self-reports of decline (Bhome et al., 2018; Roheger et al., 2021), others use standardized assessments such as the Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (Chiang et al., 2024; Dorris et al., 2021), and others do not specify how mild cognitive decline is defined (Bai et al., 2022; Lin et al., 2023; Wu et al., 2021). Consequently, the current literature is ambiguous, often blurring the lines between mild cognitive decline and what is considered part of the normal aging process (Moreira et al., 2019). However, Alzheimer’s Association (2022) reports that mild cognitive decline affects approximately 12% to 18% of older adults, of whom 10% to 15% progress to develop dementia each year. Although mild cognitive decline does not always equate with aging, its prevalence is likely to increase as the global population ages (Pais et al., 2020), making the ambiguity in the literature concerning.
For older adults experiencing mild cognitive decline, maintaining independence and sustaining participation in daily activities are crucial to preserving quality of life (National Institute on Aging, 2023). This means that people experiencing mild cognitive decline will require greater effort, support, or adaptive strategies to maintain independence, putting an increased load on health care systems (Pais et al., 2020). Occupational therapists can play a role in delivering these interventions to enhance or sustain a person’s participation in meaningful activities. Occupational therapists are specialists in assessing functional cognition (Wolf et al., 2019), which combines the concept of using cognitive skills in the context of everyday occupations and performance. Occupational therapists focus on the assessment of functional cognition at the participation level rather than relying on impairment-based measures of cognition (Wolf et al., 2019). This approach allows occupational therapists to understand and predict the amount of time and support an older adult would need to manage their daily activities. Notably, the diversity of the impact of cognitive decline requires a person-centered and evidence-based approach to occupational therapy interventions (Wolf et al., 2019).
Previous systematic reviews (Duan et al., 2018; Ham et al., 2021; Hui et al., 2021; Lee et al., 2022) have explored occupational therapy interventions used with people experiencing more severe cognitive decline, such as Alzheimer’s disease or dementia. These reviews found that occupational therapy interventions, including reminiscence therapy (Hui et al., 2021), cognitive stimulation (Duan et al., 2018), and mindfulness (Duan et al., 2018) have a positive effect on cognitive performance of older adults with a dementia or Alzheimer’s diagnosis or a more severe cognitive impairment that affects their daily activities. Many of these previous systematic reviews (Chow et al., 2021; Duan et al., 2018; Ham et al., 2021; Hui et al., 2021; Lee et al., 2022; Wu et al., 2021) have focused on measuring older adults’ cognitive performance, or memory and executive function, rather than their participation in daily tasks. Most found a statistically significant improvement in participants’ cognitive performance (Ham et al., 2021; Hui et al., 2021; Lee et al., 2022; Wu et al., 2021). However, the interventions described in these systematic reviews are not relevant to people experiencing mild cognitive decline because interventions for more severe cognitive decline typically focus on managing, compensating, or adapting the environment to accommodate for problem behaviors and cognitive decline (Hui et al., 2021; Lee et al., 2022; Wu et al., 2021). In contrast, when working with individuals experiencing mild cognitive decline, there is a greater opportunity for early intervention and the use of remediation approaches aimed at improving or maintaining cognitive function (Hui et al., 2021). Both approaches have value, and their application should be tailored to the individual’s level of impairment and specific needs (American Occupational Therapy Association [AOTA], 2020).
The evidence on the types of occupational therapy interventions provided for adults who experience mild cognitive decline is limited; thus, the evidence to support occupational therapists in replicating clinical trial interventions in a clinical setting is limited. Therefore, this review examined occupational therapy interventions used with older adults experiencing mild cognitive decline and determined the effect of these interventions on participation in daily activities. The research questions for this systematic review were as follows: What occupational therapy interventions are used with older adults experiencing mild cognitive decline? What is the impact of these interventions on participation in daily activities?
Method
This systematic review of randomized or quasi-randomized controlled trials used methods recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2023) and is reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). This review was registered with the International Register of Systematic Reviews (PROSPERO; CRD42023388102) before it commenced and was updated after completion of the final searches.
Search Strategy
Systematic searches were completed of the Embase, CINAHL, and MEDLINE databases. Searches were completed in March 2023 and updated in August 2024. Search terms were adapted for each database and included words related to older adults, mild cognitive decline, and occupational therapy interventions. An academic librarian supported the systematic search and keyword selection. The full search strategy is presented in Table A.1 in Supplemental Appendix A (available online with this article at https://research.aota.org/ajot). Two authors (Emma Ward and Emma J. Schneider) conducted an initial review of article titles to remove duplicates.
Eligibility Criteria
Types of Studies
Studies were considered for inclusion if they were designed to investigate the effect of at least one occupational therapy intervention targeting mild cognitive decline against one comparator. The comparator group could be active (different doses of the same interventions) or passive (standard treatment or no treatment). Only randomized or quasi-randomized trials, the highest level of evidence (Levels 1b and 2b), were considered for inclusion, as defined by the OCEBM Levels of Evidence Working Group (2011). Systematic reviews, study protocols, conference proceedings, editorials, and commentary papers were excluded. Studies were also excluded if the full text was unavailable or not published in English.
Participants
The population included participants with a mean age of 65 yr or older with mild cognitive decline. For this review, we defined mild cognitive decline as subjective self- or caregiver-reported cognitive decline or objective mild cognitive impairment on a standardized assessment, for example the MMSE (Folstein et al., 1975). Studies were excluded during the screening process if participants had other comorbidities that likely affected their cognition, including a diagnosis of dementia, Alzheimer’s or Parkinson’s disease, or alcohol or drug use.
Interventions
Interventions were included if they were within the scope of occupational therapy practice and facilitated by an occupational therapist or by a research assistant or occupational therapy assistant led by an occupational therapist. Interventions could be delivered in a hospital or community setting to capture all possible intervention strategies. The Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; AOTA, 2020, Table 13) was used to describe the approaches to intervention as either remediation (to restore a skill or ability that has been impaired) or compensation (to adapt or modify to support task performance) and whether an education intervention was provided (AOTA, 2020, Table 12).
Outcomes
To answer the first research question, studies that reported any patient or hospital outcomes were included in this review. To answer the second research question regarding the impact of these interventions on participation in daily activities, any outcomes that directly measured participation in daily activities, as outlined by Wolf et al. (2019), were included in the meta-analysis. For example, outcome measures such as the Lawton Instrumental Activities of Daily Living (IADL) Scale (Graf, 2008) and the Bayer Activities of Daily Living (ADL) Scale (Choi et al., 2003) were included.
Study Selection
All retrieved studies were stored in an EndNote library and uploaded to Covidence software (https://www.covidence.org). After removal of duplicates, two authors (Ward, Laura Jolliffe, Caitlin Casson, Alyssa Turcott, Jodi Ferrer, or Schneider) independently screened titles and abstracts to identify eligibility against predetermined selection criteria. Full-text copies of potentially relevant studies were retrieved and independently screened by two authors (Ward, Jolliffe, Julia Schmidt, Turcott, Ferrer, or Schneider) for inclusion. A third author (Ward, Kylie Wales, Natasha A. Lannin, or Schneider) resolved disagreements. The proportion of reviews with agreement between authors and Cohen’s κ statistic for interrater reliability were calculated in Covidence.
Data Extraction
Data from studies that met the inclusion criteria were extracted into a predetermined Excel spreadsheet by Ward and reviewed by Schneider. Characteristics of each study (authors, year, study design), participants (mean age, sex, setting), intervention (characterized by the Template for Intervention Description and Replication [TIDieR] checklist; Hoffmann et al., 2014), and outcomes were extracted. Two authors (Ward and Lannin) checked extracted data from source documents when completing the meta-analysis.
Risk of Bias
We assessed the quality of the included studies using the Cochrane risk-of-bias online tool (ROB2) for randomized controlled trials (Higgins et al., 2011). The tool uses an algorithm to propose a risk-of-bias judgment of low risk, some concerns for risk, or high risk for each study on the basis of answers to the signaling questions. Ward completed quality assessment and data collection simultaneously and independently, and Schneider cross-checked them.
Data Analysis
To answer the first research question, we extracted data to describe the participants and study characteristics. We also completed a narrative synthesis using the TIDieR checklist (Hoffmann et al., 2014) to examine the occupational therapy interventions used with older adults with mild cognitive decline and identify commonalities between and differences in interventions.
To answer the second research question, Ward and Lannin analyzed postintervention scores to obtain a pooled estimate of the effect of the intervention on participation using Comprehensive Meta-Analysis software (Biostat, 2023). Data were converted when necessary using methods recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2023). Because different outcome measures were used to assess participation, the effect size for continuous data was reported as the standardized mean difference (SMD) with a 95% confidence interval (CI). We assessed the impact of heterogeneity on results using the I 2 statistic.
Results
Included Studies
The database searches identified a total of 14,058 studies. After removal of duplicates and title and abstract screening, 155 studies were identified as potentially meeting the inclusion criteria. After the full-text review, 11 articles reporting 10 studies met the inclusion criteria and were included. One article that met the inclusion criteria was a follow-up to a previous study (Gómez-Soria et al., 2022), so we combined it with the primary study (Gómez-Soria et al., 2020) for analysis. One article (Gómez-Soria et al., 2023) was a four-arm randomized controlled trial with groups stratified by level of cognitive decline (none to moderate); only the two groups that met the inclusion criteria (subjective cognitive impairment and level deterioration) were included in this review. Three of the included studies (Jeong et al., 2016; Law et al., 2019, 2022) had more than one intervention arm; only the groups that met the inclusion criteria are described in this review. Refer to Figure 1 for the PRISMA flowchart and Table B.1 in Supplemental Appendix B (available online with this article at https://research.aota.org/ajot) for a list of the excluded studies and reasons for exclusion. The proportion of author agreement ranged from 82% to 100% in the title and abstract screening phase and from 74% to 100% in the full-text review phase. Cohen’s κ results indicated that interrater reliability ranged from 0.39 (fair) to 0.41 (moderate) during the title and abstract screening and from 0.4 (moderate) to 1.0 (perfect) during the full-text review.
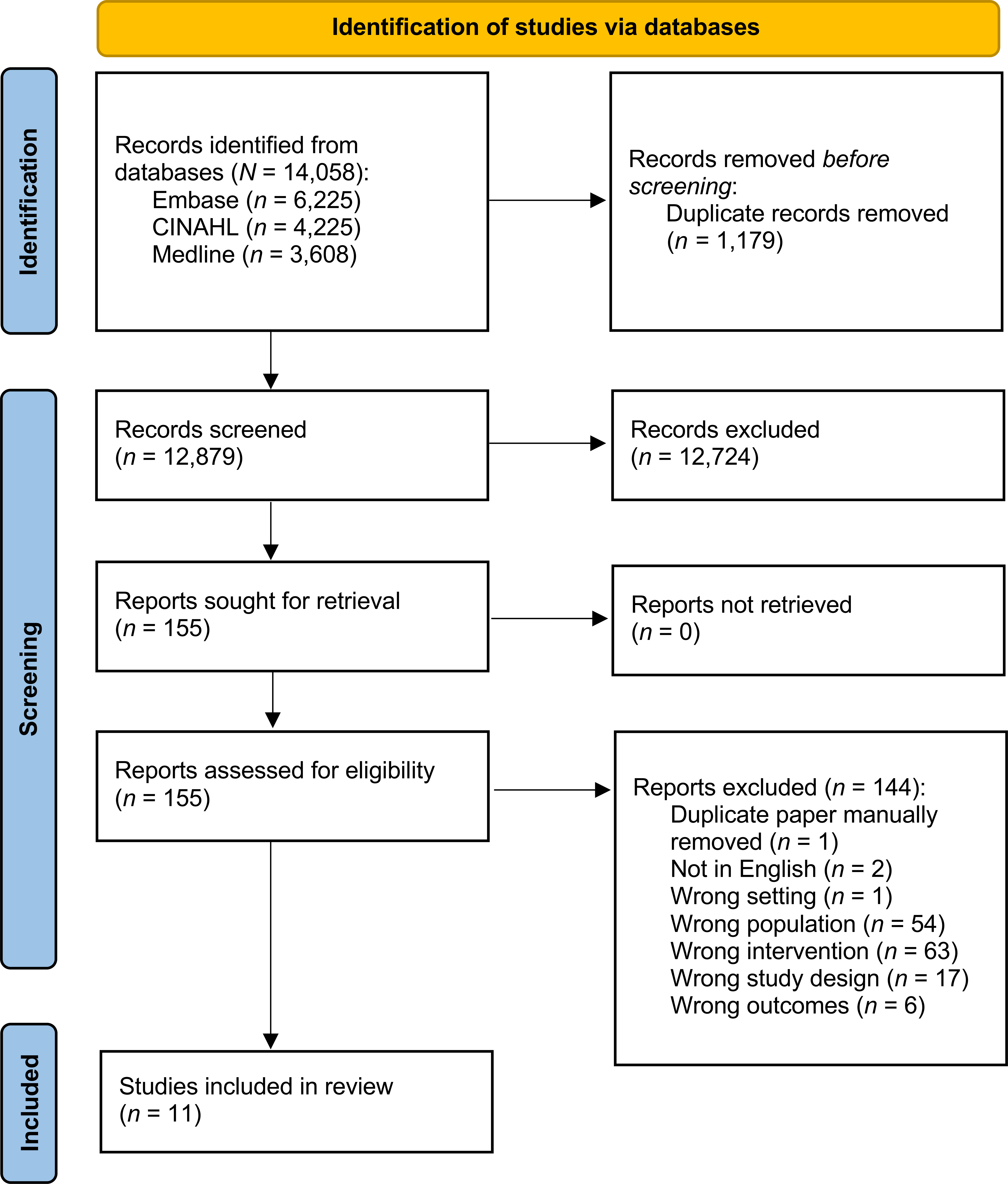
Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram.
Study Characteristics
Table A.2 describes the characteristics of the 10 included studies.
Settings
Most studies (n = 9; 90%) were completed in an outpatient setting and one (10%) in a long-term care facility. Three studies (30%) were conducted in Hong Kong, two (20%) in Spain, and one study each in Australia (10%), the United States (10%), Thailand (10%), South Korea (10%), and Taiwan (10%).
Participants
The included studies had a combined total of 1,307 participants, with the smallest study including 40 participants and the largest including 293 participants. Participants’ mean age ranged from 67.4 to 78.4 yr, and the majority (64%) were female. Refer to Table A.2 for full details.
Outcomes
Two (Griffiths et al., 2020; Kinsella et al., 2016) of the 10 included studies that did not measure participation were excluded from the meta-analysis. Of the eight studies that did measure participation, six (Gómez- Soria et al., 2022, 2023; Law et al., 2014, 2019, 2022; Yang et al., 2022) used the Lawton IADL Scale (Graf, 2008), one (Jeong et al., 2016) used the Bayer ADL Scale (Choi et al., 2003), and one (Greenaway et al., 2013) used the Everyday Cognition Memory subscale (Farias et al., 2008) and were included in the meta-analysis. All studies included a variety of outcomes designed to measure the impairment level according to the International Classification of Functioning, Disability and Health (World Health Organization, 2023).
Risk of Bias
The overall risk-of-bias analysis resulted in seven studies with low risk of bias, two with some concerns of risk of bias, and one study with high risk of bias. Table A.3 shows the full risk-of-bias evaluation, including ROB2 scores. In this review, none of the included studies reported harm or a risk of harm to participants or researchers.
Occupational Therapy Interventions Used With Older Adults Experiencing Mild Cognitive Decline
Eight interventions were used and described in the 10 included studies; three studies (Law et al., 2014, 2019, 2022) evaluated the same functional task exercise program. The intervention approaches were remediation (Gómez-Soria et al., 2022, 2023; Griffiths et al., 2020; Law et al., 2014, 2019, 2022; Yang et al., 2022), compensation (Greenaway et al., 2013), or a combination of both (Jeong et al., 2016; Kinsella et al., 2016).
Remediation was used in all but one included study (Greenaway et al., 2013), with the interventions designed to support a participant’s cognitive abilities through cognitive strategy training or education. Compensation was used in three studies (Greenaway et al., 2013; Jeong et al., 2016; Kinsella et al., 2016), with the interventions designed to train participants in the use of external memory aids such as calendars or memory books and how they can be used to compensate for mild cognitive decline during daily activities to improve performance. Greenaway et al. (2013) used a compensatory intervention approach alone that was designed to change the task demands through a memory support system (notebook). Only one study (Gómez-Soria et al., 2020) reported using the Model of Human Occupation (Kielhofner & Burke, 1980) and the OTPF–4 (AOTA, 2020) to form the conceptual framework for the study.
Education was part of the intervention protocol in three studies (Jeong et al., 2016; Kinsella et al., 2016; Yang et al., 2022), designed to target participants’ knowledge about health education, lifestyle and dementia prevention, memory and changes in memory associated with aging and lifestyle issues, or coping strategies. Exercise interventions were less common but included rhythmic aerobic movement to music (Griffiths et al., 2020) or simulated task exercises, including placing and collecting cups (Law et al., 2014, 2019, 2022). These studies theorized that stimulating the brain through exercise would improve older adults’ cognitive functioning. Five studies included simulation of tasks or activities as part of the intervention (Griffiths et al., 2020; Law et al., 2014, 2019, 2022; Yang et al., 2022). Four studies included homework between sessions as part of the intervention (Greenaway et al., 2013; Jeong et al., 2016; Kinsella et al., 2016; Yang et al., 2022). Only one study (Gómez-Soria et al., 2022) allowed participants to identify personal goals that guided the standardized intervention to target the participants’ main concerns and preferences. Only three studies allowed tailoring of exercises (Law et al., 2014, 2019, 2022), one personalization of activities (Gómez-Soria et al., 2023), and one modification of the homework’s level of difficulty (Jeong et al., 2016).
Occupational therapy interventions were primarily delivered face to face using group-based approaches. Groups contained four to 47 participants (M = 20, SD = 16) over an average of 17 sessions (SD = 16). The mean session length was 65 min (SD = 32), once to twice per week, for a mean of 10 wk (SD = 3) and followed a standardized treatment protocol. Two of the included studies (Greenaway et al., 2013; Kinsella et al., 2016) included a caregiver, friend, or family member as part of the intervention. Tables A.4 and A.5 describe the TIDieR checklist items for the eight interventions used in the included studies.
Effectiveness of These Interventions on Participation in Daily Activities
The immediate effect of occupational therapy interventions was determined by pooling postintervention data using a random effects model from seven comparisons that measured participation in daily activities immediately after the intervention period. These comparisons were from studies that had a combined 571 participants (Gómez-Soria et al., 2020, 2023; Greenaway et al., 2013; Jeong et al., 2016; Law et al., 2014, 2019; Yang et al., 2022). Occupational therapy interventions did improve participation in daily activities immediately after the intervention period (SMD = 0.504, 95% CI [0.194, 0.813]; Figure A.1a in the Supplemental Material). There was considerable heterogeneity (I 2 = 68%), indicating the variation between results of the trials was above the variation expected by chance (Deeks et al., 2023).
We also analyzed six comparisons that measured participation 6 mo after the intervention period for studies with a combined 447 participants (Gómez-Soria et al., 2020, 2023; Greenaway et al., 2013; Jeong et al., 2016; Law et al., 2014, 2022). Occupational therapy interventions did improve participation 6 mo after the intervention period (SMD = 0.271, 95% CI [−0.090, 0.631]; Figure A.1b). There was considerable heterogeneity (I 2 = 71%), indicating the variation between results of the trials was above that expected by chance (Deeks et al., 2023).
Discussion
The purpose of this systematic review was to examine the occupational therapy interventions for older adults experiencing mild cognitive decline and the effect of these interventions on participation in daily activities. The results show that both compensation and remediation approaches provide benefit, with solely compensation strategies used less commonly. Many of the interventions remediate cognitive abilities through skill acquisition, activity performance, or both, whereas the most common compensatory approaches were strategy use and education. Interventions were mostly completed in a face-to-face group environment, once or twice a week.
Our meta-analysis indicates that improvement in participation is maintained for up to 6 mo after the intervention concludes. This favorable result may indicate the long-lasting benefit of occupational therapy intervention, similar to results from previous research with community-dwelling older adults, which indicated that participation outcomes are maintained after occupational therapy interventions conclude (Smallfield & Molitor, 2018). Further research may clarify the components of the interventions that facilitate the maintenance of participation gains and methods to promote long-term improvement.
An interesting factor in older adults’ participation identified in our findings was the involvement of caregivers in the delivery of the occupational therapy intervention. Two of the studies included caregivers, and both demonstrated that the intervention alleviated caregiver burden (Greenaway et al., 2013; Kinsella et al., 2016). Previous occupational therapy research with the population with dementia also suggests the benefits of involving caregivers, with interventions leading to improved performance of ADLs and improved health outcomes for participants and their caregivers (Raj et al., 2021). It is also possible that caregivers may increase adherence to the intervention protocol, as reported in the review studies, improving outcomes overall. Future research could explore the impact, experience, and key features of involving caregivers in interventions for mild cognitive decline in older adults.
As previously mentioned, functional cognition is core to occupational therapy, and assessing participation in meaningful functional activities is the best way to measure the impact of occupational therapy intervention (Wolf et al., 2019). Most studies in our review focused on participation in daily activities as an outcome, for example, taking medication, using a telephone, preparing food, and using transportation. This is a positive indication that occupational therapy research is adopting a person-centered, functional lens. This approach aligns with the core of occupational therapy and functional cognition, providing a true measure of occupational therapy intervention outcomes. Studies that do not measure participation but instead focus on body structure and impairment level may overlook essential elements of a person, such as external environmental factors, routines, habits, social relationships, and past experiences. Previous literature has highlighted the importance of these elements in facilitating successful participation in activities (Pyatak et al., 2022). Careful consideration should be made to ensure that robust and appropriate outcome measures are used and that measures are consistent to ensure comparisons across studies.
This review had four main limitations. First, it is possible that relevant articles were missed in screening, which may lead to incorrect interpretation of findings. However, our search strategy received expert consultation, and our exclusion process was rigorous, with two authors independently reviewing articles. Second, we included only published studies (i.e., no gray literature) and those written in English, affecting the evidence’s generalizability. However, the review included studies conducted across seven countries, meaning that the findings may be applicable internationally. Third, moderate to considerable heterogeneity exists in the interventions used to mitigate mild cognitive decline in older adults. This may not be surprising given the breadth and scope of occupational therapy practice (Schell & Gillen, 2018) and the diverse issues that older adults with mild cognitive decline experience (Pais et al., 2020). It may also suggest that between-studies variation in the interventions used is too great, and we may not be able to determine the core features of the intervention given that variability. However, this heterogeneity highlights the versatility and person- centered approaches used in occupational therapy interventions. Fourth, the use of an American occupational therapy model may bias the analysis of interventions with predetermined categories that may not fully reflect the intent or mechanism of the intervention when delivered in diverse international settings.
Implications for Occupational Therapy Practice
The results of this systematic review have the following implications for occupational therapy practice: ▪ Occupational therapy interventions used with older adults experiencing mild cognitive decline can improve participation in daily activities for up to 6 mo. ▪ Occupational therapists should draw on remediation intervention approaches (e.g., cognitive stimulation, memory groups, functional task exercise), compensation intervention approaches (e.g., education, memory support system, coping strategies), or both, plus various procedures and materials to address activity participation in older adults with mild cognitive decline. ▪ When working with this population, occupational therapists should consider the range of interventions designed to target cognitive decline and the opportunity to tailor and personalize treatment plans.
Conclusion
Occupational therapy interventions result in small but significant improvements in participation in meaningful activities immediately after intervention and for up to 6 mo for older adults experiencing mild cognitive decline. When working with this population, occupational therapists should consider the range of interventions designed to target cognitive decline and the opportunity to tailor and personalize treatment plans. Future research could identify the impact of interventions, examine core features of the interventions, and understand longer-term outcomes.
Supplemental Materials
Supplementary material for Interventions Used to Increase Participation Among Older Adults Experiencing Mild Cognitive Decline: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051121.pdf for Interventions Used to Increase Participation Among Older Adults Experiencing Mild Cognitive Decline: A Systematic Review by Emma Ward, Kylie Wales, Laura Jolliffe, Julia Schmidt, Natasha A. Lannin, Caitlin Casson, Alyssa Turcott, Jodi Ferrer and Emma J. Schneider in The American Journal of Occupational Therapy
Supplementary material for Interventions Used to Increase Participation Among Older Adults Experiencing Mild Cognitive Decline: A Systematic Review
Supplementary material, sj-pdf-2-aot-10.5014_ajot.2025.051121.pdf for Interventions Used to Increase Participation Among Older Adults Experiencing Mild Cognitive Decline: A Systematic Review by Emma Ward, Kylie Wales, Laura Jolliffe, Julia Schmidt, Natasha A. Lannin, Caitlin Casson, Alyssa Turcott, Jodi Ferrer and Emma J. Schneider in The American Journal of Occupational Therapy
Footnotes
*Denotes articles include in the systematic review.
Acknowledgments
This research was not funded by any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. However, Natasha A. Lannin was supported by a Future Leader Fellowship from the Heart Foundation of Australia (GNT 106762).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.