
Abstract
The findings of this study suggest that virtual reality could be a valuable addition to therapeutic programs for children with developmental coordination disorder and help them achieve better outcomes.
Developmental coordination disorder (DCD) is a neurodevelopmental disorder characterized by significant difficulties in motor skills, as defined by the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM–5–TR; American Psychiatric Association, 2022). The diagnosis is based on four main criteria: (1) a marked impairment in motor coordination below the expected level for the child’s age; (2) significant interference of this impairment with daily activities, academic performance, and social interactions; (3) the exclusion of other medical conditions as the primary cause of motor difficulties; and (4) the confirmation that the condition is consistent with the child’s developmental stage (American Psychiatric Association, 2013).
DCD is a neurodevelopmental disorder that is commonly observed in elementary school-age children (Lingam et al., 2010; Tunçtürk et al., 2019). Children with DCD face a series of difficulties in various areas of life, such as executive function, sensory-perceptual function, and motor control of movements, thus limiting their academic, social, and physical abilities (Wilson et al., 2013). In addition, DCD not only affects a child’s physical capabilities but also contributes to emotional and psychological distress, affecting family dynamics (Zwicker et al., 2015).
The motor coordination of a child with DCD falls below age-appropriate expectations, and there may be delays in early motor skills such as walking and crawling. Children with DCD often experience problems with a range of motor tasks, such as running, dressing, and writing (Lino et al., 2021). Gross motor skill development and performance are negatively affected because of poor motor control, which is one of the main features of DCD. Gross motor skills, which are among the basic movement skills, are emphasized to be important in terms of development, because they form the basis of functional activities, play, and socialization and support the complex movement skills required for sports and competence in children (Lucas et al., 2016).
Studies have shown that executive dysfunctions are also common, as are motor disorders, that there is not enough work on this topic, and that more focus needs to be placed on it (Fogel et al., 2023; Wilson et al., 2013). In a systematic review, it was stated that it would be important for the occupational therapist to assess a child’s movement difficulties, as well as cognitive areas such as working memory, to consider the relationship between motor skills and executive functions and to establish relevant intervention targets (Fogel et al., 2023). Given the evidence of executive function impairments in DCD, negative effects are observed in movement control (Wilson et al., 2016).
The primary sensory systems associated with movement control are the visual, vestibular, and proprioceptive–kinesthesia systems (Piek et al., 2007). Problems in processing visual, proprioceptive, or tactile information (Ameratunga et al., 2004; Piek et al., 2007), as well as difficulties in visual–motor integration, are considered underlying causes of challenges in motor planning (Laufer et al., 2008). Children with DCD are often reported to have difficulties with organization and praxis (Wilmut & Byrne, 2014). It has been particularly noted that children with DCD exhibit significant delays in task planning and execution, organizing their bodies for the task, performing motor activities, interacting with peers during motor tasks, and responding to stimuli (Farmer et al., 2016). Failure to implement interventions in these areas can lead to social participation difficulties in children with DCD, which may continue to affect their lives throughout adolescence and adulthood (Sylvestre et al., 2013).
Sensorimotor coordination impairments in DCD affect children’s ability to perform daily living activities, which leads to difficulties in functional tasks such as dressing, riding a bicycle, and participating in leisure activities (Bonney et al., 2017). Because of difficulties with skill acquisition, it can also affect their ability to acquire and perform motor skills, to perform daily living activities, and to benefit from interventions (Poulsen et al., 2007). Children with DCD have been reported to experience activity limitations that are due to decreased participation in activities of daily living and physical activities (Batey et al., 2014).
It has been emphasized that using the International Classification of Functioning, Disability and Health (ICF) model to examine the impairments and activity limitations of a child with DCD in a meaningful context offers distinct advantages, compared with other approaches (Ferguson et al., 2014). The ICF framework reflects an ecological approach, because it considers the relationship between functional performance and contextual factors, making it a suitable model for understanding DCD (World Health Organization, 2007). Within the ICF framework, in terms of body structures and functions, DCD affects motor functions such as muscle tone, balance, and coordination, leading to significant motor skill difficulties (Keating et al., 2022). From the perspective of activity and participation, it also affects children’s participation in social and physical activities, limiting their social interactions, compared with typically developing peers (Steenbergen et al., 2020).
Regarding contextual factors, the effects of DCD are influenced by environmental and personal factors, with family and therapist support playing a crucial role in promoting participation (Ferguson et al., 2014). Interventions for DCD are generally categorized into two types: process and/or disorder focused and task oriented (Blank et al., 2019). Studies have shown that children with DCD benefit more from task-oriented approaches (Armstrong, 2012; Krajenbrink et al., 2022). Moreover, across all approaches, frequent practice in different environments and consistent feedback are essential elements for successful interventions in children with DCD (Smits-Engelsman et al., 2013).
Recently, digital technologies have gained prominence, offering innovative ways to engage children in therapy. These technologies provide adaptable intervention environments and experiences that are tailored to individual needs (Mentiplay et al., 2019). One such method, virtual reality (VR), is classified as both an activity-oriented and a participation-oriented approach. VR has emerged as a promising intervention tool for children with motor difficulties (Green & Wilson, 2012). Like task-oriented approaches, VR interventions incorporate key elements of motor learning, such as multiple movement repetitions, augmented feedback, and variability in practice (Ashkenazi et al., 2013). Studies have emphasized that VR can be effectively integrated into rehabilitation programs to enhance motor skills and functional performance through task-specific training (Nilsen et al., 2015; Scalona et al., 2019; Szturm et al., 2013). VR is considered a functional intervention in occupational therapy because it enhances motor skills, increases participation in daily activities, and provides sensory stimulation and motivation (Choi et al., 2021; Pérez-Marcos et al., 2017). VR interventions are increasingly supported by the embodied cognition theory, which suggests that executive functions are closely linked to sensory and motor experiences. By offering immersive, multimodal environments, VR has the potential to activate attention, working memory, inhibition, and cognitive flexibility—key components of executive functioning—through goal-directed tasks and real-time feedback mechanisms (Parsons et al., 2017).
One of the key advantages of VR-based rehabilitation is its ability to offer interactive and immersive environments that simulate real-life activities, providing children with immediate feedback and personalized challenges tailored to their level of ability. These immersive experiences significantly enhance motivation, attention, and adherence, which are crucial factors that positively affect therapeutic outcomes in pediatric populations (Utamayasa & Mardhika, 2024). The gamification of rehabilitation through VR not only increases engagement but also supports repetitive practice in a controlled environment, which is essential for skill acquisition (Liu et al., 2022). It allows individuals to practice real-life scenarios in a controlled environment, facilitating skill transfer and rehabilitation. Its customizable nature enables therapists to tailor interventions to individual needs, making therapy more effective and engaging (Rodríguez-Hernández et al., 2021). However, there is a need for larger, blinded, randomized controlled trials to better assess the benefits of VR interventions for children with coordination difficulties (Cavalcante Neto et al., 2019; Hammond et al., 2014).
The literature highlights the need for randomized controlled trials with large sample sizes to assess the effects of VR interventions for children with DCD. Additionally, studies have emphasized that research in this area should focus on all dimensions of the ICF framework (Ferguson et al., 2014; Hammond et al., 2014). No studies were found that comprehensively examine the effects of VR interventions on body structures and functions, as well as activity levels, in children with DCD. This research is based on the hypothesis that the VR intervention has no significant effect on motor skills, cognitive skills, sensory-perceptual skills, and activity in children with DCD. Therefore, from an ICF framework perspective, our study was designed to investigate the impact of VR interventions on motor, cognitive, and sensory-perceptual skills, as well as activity levels, in children with DCD.
Method
We conducted a single-blind randomized controlled trial to examine the effects of VR on motor, cognitive, praxis, and visual perception skills and activities in children with DCD. Ethical approval was obtained from the university ethics board (University of Health Sciences, Antalya Training and Research Hospital Clinical Research Ethics Committee), and written consent was secured from each participant’s legal guardian. This trial has been registered with ClinicalTrials.com (NCT06246318).
Participants
Because of the power analysis conducted with 80% power and a 5% error rate, we calculated the sample size as 46. A total of 65 children were initially assessed for eligibility, but 17 met the criteria for exclusion. Therefore, the final sample consisted of 48 children with DCD, ages 5–8 yr.
The inclusion criteria were the following: ▪ Diagnosis of DCD by a physician according to DSM–5–TR criteria. ▪ A diagnosis that was established on the basis of a comprehensive clinical evaluation, including developmental history, direct observation, and standardized motor assessments, in accordance with DSM–5–TR guidelines. ▪ Ages 5 to 8 yr. ▪ A score between 15 and 46 points on the Developmental Coordination Disorder Questionnaire (DCDQ) for children ages 5–7 yr. ▪ A score between 15 and 55 points on the DCDQ for children ages 8 yr. ▪ A score higher than 28 on the Mini-Mental State Examination adapted for children ages 5–8 yr.
Among the those who met the inclusion criteria, children who had the presence of a serious neurological disease, vision (other than glasses) or hearing impairments, and/or participation in any other therapy program during the study were excluded.
Procedure
Volunteers who met the inclusion criteria were informed about the study’s purpose and methodology, and we obtained informed consent from their legal guardians. Participants were randomly assigned to two groups: the study group (n = 24) or the control group (n = 24). The simple randomization method was used in the randomization of sample groups. The random assignment sequence was generated using a computer-based random number generator. The random assignment sequence was applied using preprepared, consecutively numbered, and sealed envelopes. We used sealed, opaque envelopes to ensure assignment confidentiality. Each envelope contained the assigned group assignment and was opened only after a participant was enrolled and consented to do so. Participants were enrolled by the second author (Koray Kara), who was unaware of the assignment sequence. The intervention assignment was performed by the same researcher who opened the sealed envelopes. The researcher who performed the pretest and posttest was blinded to the group assignment. All included in the study were evaluated by a single evaluator (Sedef Şahin, an associate professor and occupational therapist) at pretest and posttest. Interventions were carried out by a single researcher with sufficient experience and equipment in the field (Zeynep Kolit, an assistant professor and occupational therapist).
The study group received both conventional occupational therapy (COT) and additional VR intervention, whereas the control group received only the COT program. The VR intervention used Nintendo Wii Fit Plus as the VR tool. The COT program incorporated sensorimotor-based activities (see Appendix A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot).
Participants in the control group were offered the option to receive the VR intervention after the study was completed. The interventions took place twice a week, with each session lasting 45 to 60 min, over a total period of 8 wk. The study flowchart is presented in Figure 1.
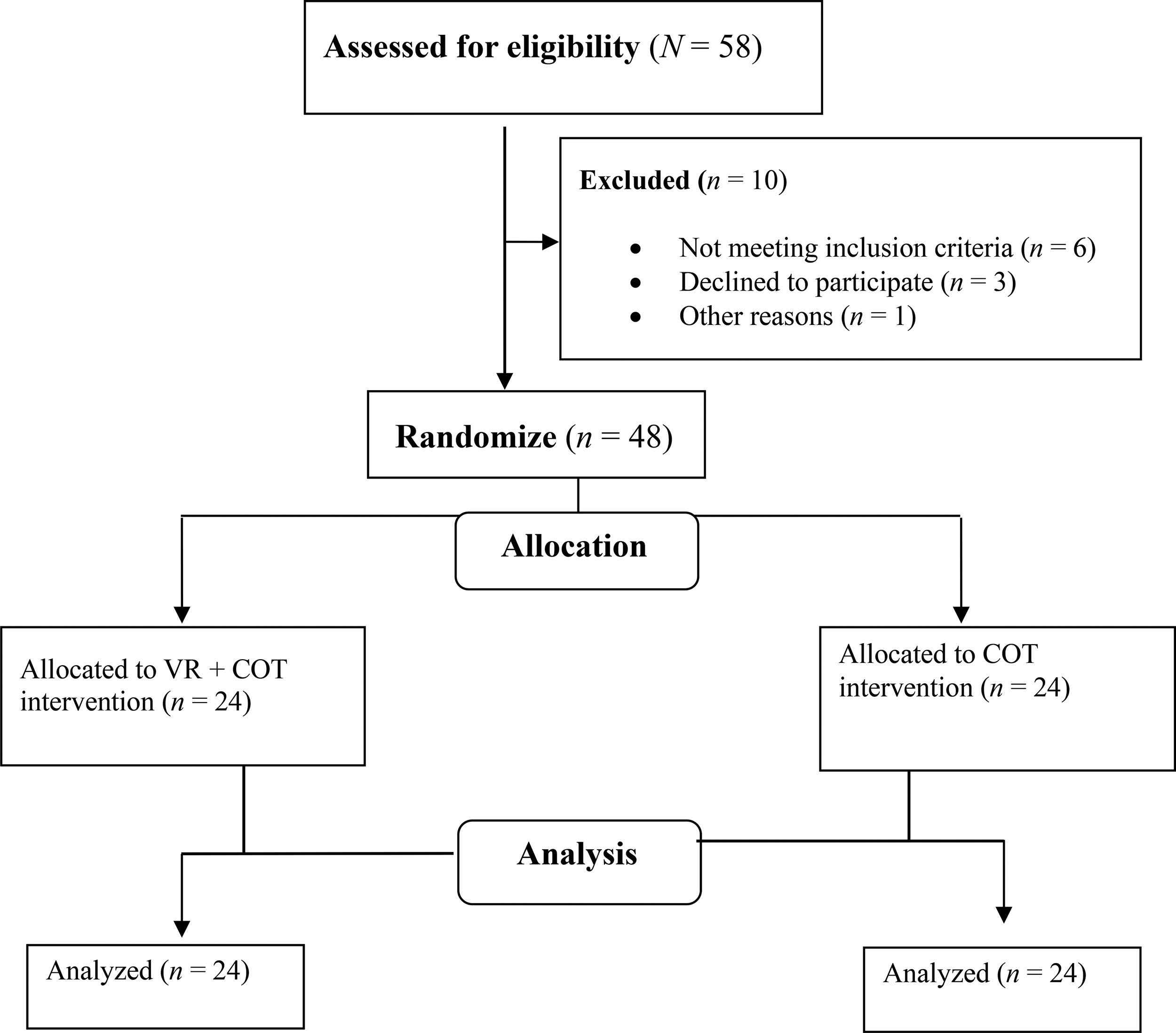
Study flow chart.
Measures
In this study, we used the following assessment methods: the Sociodemographic Information Form, the Test of Gross Motor Development (2nd ed.; TGMD–2) for gross motor skills; the Childhood Executive Functioning Inventory (CHEXI) for cognitive skills; the Sensory Integration and Praxis Test (SIPT) for sensory (praxis) skills; the Motor-Free Visual Perception Test–3 (3rd ed.; MVPT–3) for motor skill–independent visual perception skills; and the Functional Independence Measure for Children (WeeFIM) for activity (Figure 2). The effectiveness of the intervention was determined using pre- and postintervention assessment methods.
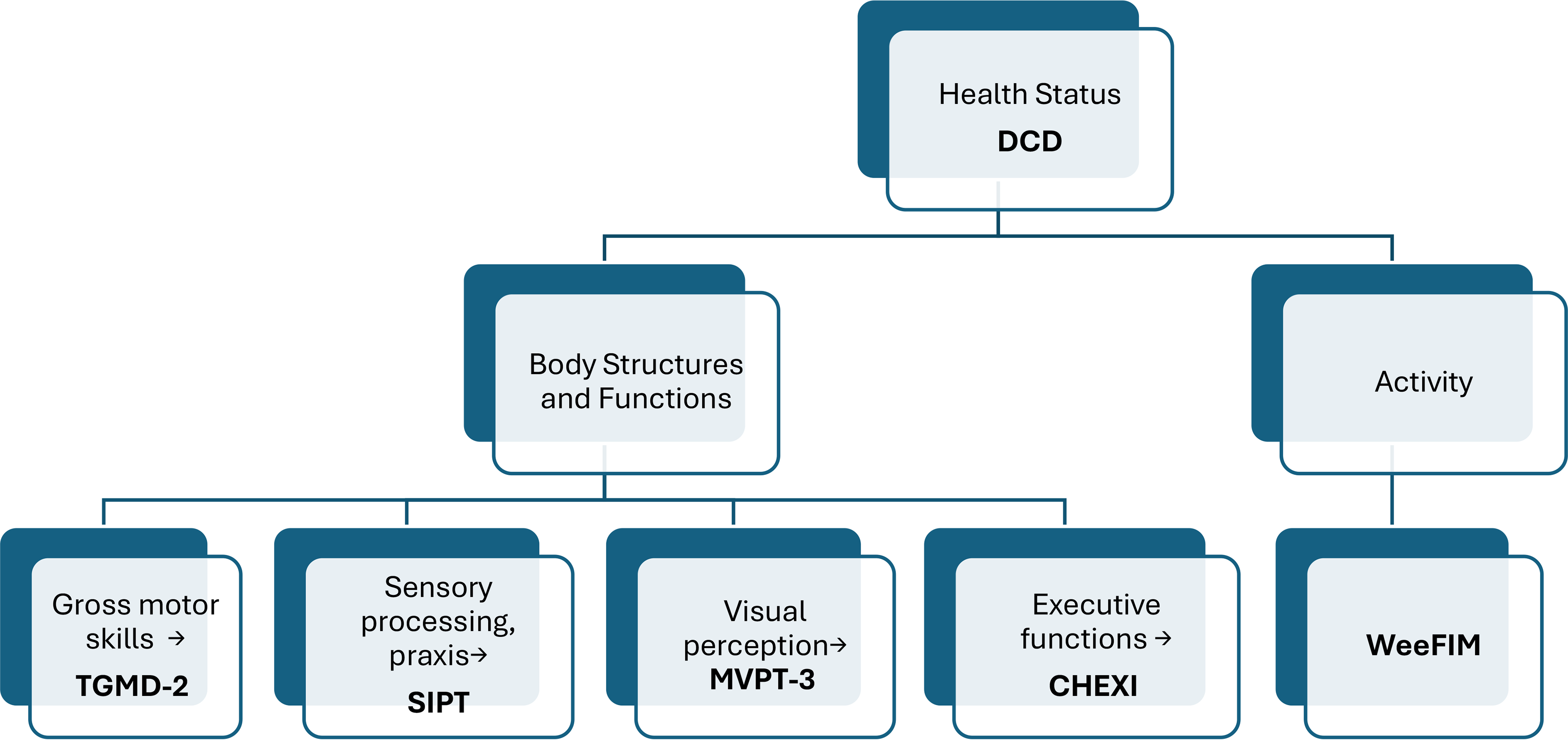
Assessments used from an ICF perspective.
Sociodemographic Information Form
We developed this form to collect the participants’ demographic information, such as age, gender, body mass index (BMI), education level, and dominant hand side.
TGMD–2
Developed by Ulrich (1985) to evaluate the motor skills of children between the ages of 3 and 10 yr and was revised as the TGMD–2 in 2000. The test contains 12 motor skills divided into two subtests: locomotor (run, leap, gallop, hop, jump, and slide) and object control (catch, strike, bounce, over- and underhand throw, and kick). The assessment can typically be completed within 20–30 min. The sum of the observed criteria for each subscale comprises the total raw score (0–48 points; Ulrich, 1985). The validity and reliability of the test in Turkish was established by Boz and Güngör Aytar (2012; Cronbach’s α = .87).
CHEXI
Developed by Thorell and Nyberg (2008) as a measurement tool focused on the executive functions of children ages 4–12 yr (Thorell & Nyberg, 2008), the CHEXI can be completed by parents or teachers. Consisting of 24 items, this 5-point Likert-type scale ranges from 1 (definitely not true) to 5 (definitely true). It has two subscales: working memory and inhibitory control. The scale takes 5–10 min to complete. Higher scores on the scale indicate that the child has more difficulties with executive functions (Thorell & Nyberg, 2008). The validity and reliability of the scale in Turkish were established by Arslan Çiftçi et al. (for inhibitory control, Cronbach’s α = .91; and for working memory, Cronbach’s α = .95; Arslan Çiftçi et al., 2020).
SIPT
The SIPT is a fundamental tool in the assessment of sensory processing and praxis in children, particularly those with sensory integration disorders. Developed by A. Jean Ayres, the SIPT consists of 17 standardized tests that are designed to evaluate various sensory integration functions, including visual and tactile perception, motor planning, and vestibular–proprioceptive functions (Ayres, 1996). The test has been validated and standardized on a large sample of children ages 4 yr to 8 yr, 11 mo demonstrating strong reliability and validity across diverse populations (Holmlund & Orban, 2021). To assess praxis skills, we used SIPT subtests that measured postural praxis, praxis on verbal command, oral praxis, sequencing praxis, and constructional praxis.
MVPT–3
Originally developed by Colarusso and Hammill (1972), it was revised in 2003 as 65 items for people between the ages of 4 and 95 yr (Colarusso & Hammill, 2003). The first 40 items in the test are applied to children between the ages of 4 and 10 yr, and the 51 items for people between the ages of 14 and 65 yr are applied to children ages 10 yr and older. The application takes approximately 15–20 min for each child. Each correct answer given is recorded on the score sheet as 1 point, and each wrong answer is recorded as 0 points. In scoring the test, the wrong answers are subtracted from the correct answers to obtain a raw score, and these scores are calculated as a percentage. The total score is equal to the number of correct answers given. Metin and Aral established the validity and reliability of the MVPT–3 in Turkish (Cronbach’s α = .85; Metin & Neriman, 2012).
WeeFIM
An 18-item and seven-level ordinal scale, WeeFIM measures a child’s incoherent performance in basic daily functional skills (Liu et al., 1998). It can be used for children with developmental disabilities, with subscales that measure self-care, sphincter control, movement, transfers, social cognition, and communication. We used a scale on which scores ranged between 1 (total assistance) and 7 (total independence). The maximum total score is 126, and the lowest total score is 18, whereas the maximum scores for self-care, mobility, and cognition are 56, 35, and 35, respectively (Liu et al., 1998). Tur et al. established the validity and reliability of the Turkish version of the WeeFIM in children, highlighting its effectiveness in clinical settings (Tur et al., 2009).
VR Intervention
The Nintendo Wii Fit Plus has emerged as a significant tool in rehabilitation and exercise, particularly in enhancing balance, strength, and overall physical function across various populations. This variety not only caters to different fitness levels but also maintains user engagement, which is crucial for adherence to exercise programs. The interactive nature of the Wii Fit Plus, which incorporates VR elements, has been highlighted as a motivating factor that encourages repetitive practice and motor learning, which are essential components in rehabilitation. The platform’s ability to provide real-time feedback and adjust difficulty levels makes it suitable for various rehabilitation settings (Kim et al., 2015; Mohammadi et al., 2023).
In this study, we used the Nintendo Wii Fit Plus, incorporating the Wii Balance Board and Wii remote controllers. This system allows players to participate in games that vary in difficulty while controlling their center of movement throughout activities. The Wii Fit Plus’s balance board provides real-time feedback, which is essential for users to correct their posture and movements. Wii Fit Plus offers over 40 activities, including yoga, strength training, aerobics, and balance games. For the intervention, the therapist categorized the Wii Fit Plus activities by difficulty level, progressing from easy to more challenging tasks. Each session included a variety of activities that were tailored to the participant’s progress and abilities (Meldrum et al., 2012). The VR games were selected on the basis of their alignment with specific therapeutic goals related to motor coordination (e.g., balance, bilateral coordination), cognitive engagement (e.g., decision-making, attention), and sensory-perceptual skills (e.g., visuospatial processing). For instance, Wii Fit balance games were used to target dynamic balance and proprioceptive feedback, whereas training games (e.g., Rhythm Kung Fu) were chosen for their emphasis on reaction time, bilateral upper limb coordination, and task-focused cognitive engagement. Activity progression followed a gradual increase in complexity, from basic movements (e.g., single-limb balance) to more dynamic, dual-task challenges requiring coordination, timing, and strategic thinking. This progression was tailored weekly according to each child’s performance, as evaluated by the therapist using preset performance criteria (e.g., ability to maintain posture, response accuracy, level of assistance required).
The specific Nintendo Wii Fit Plus activities used during the intervention are detailed in Table 1. At least two to three different activities were selected from each category in each session from the activities included in Nintendo Wii Fit. Thus, each child tried the activities in all categories (Appendix A.2). For example, in the first session, for yoga: Deep Breathing, Half Moon Pose, and Warrior Pose were selected; for strengthening: Torso Twist, Push-ups and Side Plank, and Single Leg Extension were selected; for aerobics: Hula Hoop, Step Training, and Running were selected; and for balance games; Soccer, Ski Slalom, and Ski Jumping were selected. To ensure an individualized therapeutic challenge, we systematically adjusted the difficulty level of Wii Fit Plus activities on a weekly basis according to each participant’s performance. Initial sessions were used to establish a functional baseline for balance, coordination, and attentional capacity. When a child demonstrated ≥80% success on a task, progression was implemented by increasing movement complexity or duration, adding cognitive load or reducing external cues. Task advancement followed a structured three-phase progression model: basic motor tasks in Wk 1–2, dynamic balance and bilateral coordination in Wk 3–5, and cognitively demanding dual-task activities in Wk 6–8. This progression was guided by motor learning principles and clinical observation, ensuring both safety and therapeutic efficacy.
Nintendo Wii Fit Plus Activities
COT Intervention
COT intervention encompasses approaches that are aimed at helping people overcome physical, cognitive, and emotional challenges to achieve independence in daily living activities. This intervention includes personalized activities, environmental modifications, and skill development tailored to the person’s specific needs. The goal is to enhance the person’s quality of life and promote functional independence by providing practical solutions (Tanner et al., 2020). The COT program used sensorimotor-based activity approaches designed to offer children diverse sensorimotor experiences. Within this approach, the principles of sensory integration and neuroplasticity were used to facilitate improvements in motor planning, coordination, and general functional abilities (Fu et al., 2022). Sensorimotor-based intervention activities were conducted within a standardized protocol framework (Schaaf & Mailloux, 2015) by an occupational therapist with training and licensure in this field. The sensorimotor-based activity approach encompasses various interventions and strategies that are designed to enhance motor skills and sensory processing through engaging, interactive activities. The COT intervention involved activities that stimulate the senses and motor skills—such as swinging, running, obstacle courses, crawling through tunnels, jumping on a trampoline, and playing with textured materials (Ouellet et al., 2021). The therapist designed personalized strategies to help children address their challenges, choosing activities that aligned with their unique needs and preferences. Additionally, children were motivated to actively participate by proposing their own activity ideas and creating individual action plans, which promoted both engagement and independence (Kantor et al., 2022).
Statistical Analysis
We performed statistical analysis using SPSS statistical software, Version 20 for Windows. Descriptive statistics, including participants' sociodemographic information, were reported as frequencies or means and standard deviations, depending on the variable type. The variables were investigated using visual (plots or histograms) and analytical (the Kolmogorov–Smirnov test) methods to determine whether they were normally distributed. The results indicated that the data did not conform to the assumption of normality; therefore, we used nonparametric statistical methods for subsequent analysis. For this, we used the Mann–Whitney U test and Wilcoxon test—which are known to provide robust analysis. A significance threshold of p < .05 was applied for all statistical tests. For within-group comparisons of pre- and postintervention measurements, we used the Wilcoxon signed-rank test. To compare outcomes between the two groups, we used the Mann-Whitney U test. Clinical significance was further assessed using the effect size index for independent groups and was categorized on the basis of effect size: small, <0.3; medium, 0.3–0.8; and large, ≥0.8 (Cohen, 1977).
Results
The demographic characteristics of the participants are summarized in Table 2. Both groups were statistically similar in terms of age, education level, BMI, gender, and dominant hand side (p > .05).
Demographic Characteristics of the Participants
Note. N = 24. BMI = body mass index.
Mann–Whitney U test statistics were used to compare two independent groups.
The χ2 test was used for categorical variables. Statistical significance was considered at p < .05.
Findings related to within-group changes in TGMD–2, CHEXI, SIPT (praxis), MVPT–3, and WeeFIM scores and effect sizes are presented in Table 3. In the study group, significant improvements were found in TGMD–2, CHEXI, SIPT (praxis), MVPT–3, and WeeFIM scores (p < .05). In the control group, statistically significant differences were observed in the SIPT (praxis), MVPT–3, and WeeFIM scores (p < .05), whereas no significant differences were noted in TGMD–2 and CHEXI scores (p > .05). Effect sizes indicated strong effects in the study group for TGMD–2, CHEXI, SIPT (praxis) and WeeFIM scores (d > 0.8). In the control group, a low level of effect (d < 0.3) was found in TGMD–2, CHEXI, and WeeFIM scores, and a moderate level of effect (0.3 < d < 0.7) was found in SIPT (praxis) scores. It was determined that there was a moderate effect on MVPT–3 scores in both groups (0.3 < d < 0.7).
Within-Group Changes in Motor, Cognitive, Praxis, and Visual-Perceptual Skills, as Well as Activity Levels
Note. For both the study and control groups, n = 24. The p values for within-group change were calculated using the Wilcoxon signed-rank test. Boldface indicates statistically significant values (p < .05). CHEXI = Childhood Executive Functioning Inventory; MVPT–3 = Motor-Free Visual Perception Test (3rd ed.); Post = postintervention; Pre = preintervention; TGMD–2 = Test of Gross Motor Development (2nd ed.); SIPT = Sensory Integration and Praxis Test; WeeFIM = Functional Independence Measure for Children.
Effect size >0.80.
Comparisons of pre- and postintervention scores on the TGMD–2, CHEXI, SIPT (praxis), MVPT–3, and WeeFIM between the groups are presented in Table 4. No significant differences were found between the groups in terms of preintervention values (p > .05). Postintervention comparisons revealed statistically significant differences between the groups in the TGMD–2 and SIPT (praxis; p < .05).
Comparisons of Pre- and Postintervention Motor, Cognitive, Praxis, and Visual Skills and Activity Levels Between Groups
Note. For both the study and control groups, n = 24. The p values for between-groups differences were calculated using the Mann-Whitney U test. Boldface indicates statistically significant values (p < .05). CHEXI = Childhood Executive Functioning Inventory; MVPT–3 = Motor-Free Visual Perception Test (3rd ed.); SIPT = Sensory Integration and Praxis Test; TGMD–2 = Test of Gross Motor Development (2nd ed.); WeeFIM = Functional Independence Measure for Children.
Discussion
Our aim in this study was to investigate the impact of adding VR to COT interventions on motor, cognitive, sensory (praxis), and perceptual (visual) skills and activity levels in children with DCD. The results demonstrated that adding VR to COT interventions was more effective in improving motor, cognitive, sensory (praxis), and perceptual (visual) skills, as well as in activity levels for children with DCD. When the relevant literature is examined, this study is the first, to our knowledge, to demonstrate the effects of VR interventions on motor, cognitive, sensory-perceptual skills, and activity levels in children with DCD from an ICF perspective.
Children with DCD typically experience delays in the development of motor coordination, particularly in gross motor skills (Gao et al., 2024). The Nintendo Wii-based VR intervention was found to be more effective than task-oriented training in improving motor skills in children with DCD (Cavalcante Neto et al., 2020; Neto et al., 2021). A study indicated that both Nintendo Wii Fit– and Xbox Kinect–based interventions led to similar improvements in motor performance in children with DCD, with the children showing progress in at least one motor task (Jelsma et al., 2023). A systematic review highlighted the need for further research to determine the effects of video game or VR interventions on motor outcomes in children with DCD (Mentiplay et al., 2019). Preintervention data being similar between the two groups is crucial for evaluating the intervention’s effectiveness. In our study, there were no significant differences in preintervention data between the two groups (Table 3). This demonstrates that the two groups were homogeneous in terms of their baseline assessments. In our study, the Nintendo-based VR intervention, in addition to the COT intervention, demonstrated superior effects on motor skills in children with DCD, aligning with the positive findings in the existing literature. The effect of VR intervention is consistent with the positive findings in the existing literature, and this effect is clinically meaningful. The large effect sizes suggest that these changes primarily enhance children’s motor skills. It is suggested that adding VR to COT interventions could help improve motor skill problems in children with DCD, and the inclusion of such interventions in rehabilitation programs is considered important.
In addition to motor impairments, issues with cognitive functions such as planning, attention, working memory, inhibition control, and cognitive flexibility are also known to be present in this population (Jelsma et al., 2021). In studies comparing executive function skills in typically developing children and children with DCD, it has been observed that children with DCD perform worse in visual-spatial perception, working memory, and inhibition control (Sartori et al., 2020; Wilson et al., 2020). Additionally, the necessity for interventions that support executive functions has been emphasized in the studies conducted (Rahimi-Golkhandan et al., 2016; Sartori et al., 2020). In a study that examined the effects of Wii Fit training on visual perception and executive functions in boys with DCD, positive effects on visual perception and executive functions were reported (Hashemi et al., 2022). It is noted that impairments in working memory, a critical component of executive functioning, relate to deficits in visual perception and retention of motor information in children with DCD (Ke et al., 2019). Deficiencies in executive functions may hinder the application of visual-perceptual skills in problem-solving contexts, leading to challenges in tasks that require both cognitive domains (Bernardi et al., 2018). Given the limited number of studies examining the impact of VR interventions on executive functions, this study offers valuable evidence by exploring the effects of VR interventions on executive functions in children with DCD. The findings suggest that incorporating VR into COT programs could be a promising approach for improving these functions. Notably, the large effect sizes observed in this study underscore the significant clinical improvements, reinforcing the potential of VR interventions in enhancing executive functioning in children with DCD.
In addition to motor difficulties and problems with executive functions in children with DCD, challenges in perceptual skills may also be observed, highlighting the importance of providing support in this area (Van Dyck et al., 2022). It has been reported that children with DCD experience difficulties in visual perception tasks, which consequently leads to challenges in praxis or motor planning, resulting in slower performance compared with their peers (Goyen et al., 2011; Li et al., 2015). Waal et al. pointed to a developmental immaturity in brain networks responsible for complex visual-spatial processing in children with DCD, suggesting that impairment in these cognitive domains may underlie their difficulty with motor skills (Waal et al., 2018). This highlights the potential overlap between visual processing deficits and praxis challenges, because motor planning requires efficient visual input to execute movements. Furthermore, studies have drawn attention to the oculomotor control deficits in children with DCD, which can hinder their ability to effectively direct visual attention and integrate visual information necessary for skilled motor actions (González et al., 2016; Sumner & Hill, 2024). In studies involving participants that include children with DCD, it has been frequently reported that they experience difficulties in praxis skills, particularly in postural praxis and verbal noncommand praxis tasks (Dewey et al., 2007; Sinani et al., 2011). One study identified positive effects of the VR intervention on visual perception (Hashemi et al., 2022). No other studies in the literature examine the effects of VR interventions on sensory and visual perceptual skills. In our study, improvements in sensory skills (praxis) were observed in both groups; however, the effects in the study group were more pronounced compared with those in the control group. Notably, the large effect size observed in praxis outcomes highlights the clinical relevance of these findings, suggesting that the VR intervention may effectively enhance body awareness, motor planning, and sensorimotor integration. These findings suggest that VR interventions could serve as a valuable complement to traditional therapy approaches, offering a structured yet engaging medium for targeting praxis deficits in children with DCD. In terms of visual perception skills, both groups exhibited similar effects, which, we think, is related to the role of sensorimotor-based interventions in supporting visual perception (Soref et al., 2023).
Processing difficulties related to sensory perceptual and visual systems can lead to challenges in daily living activities for children with DCD. Therefore, it is emphasized that incorporating sensory perceptual-based activities into rehabilitation programs is crucial for enhancing their independence (Elbasan et al., 2012). Studies have indicated that VR significantly augments the rehabilitation experience, presenting opportunities for repetitive practice of functional tasks in a motivating context, which could potentially lead to greater retention of skills and improved functional outcomes (Choi et al., 2021; Rodrigues et al., 2020). Studies conducted with children with cerebral palsy and Down syndrome have indicated that VR interventions help enhance the motor skills of these children, enabling them to move more independently and effectively in daily living activities (Boato et al., 2022; Khaledi et al., 2022). The need for further research to investigate the effectiveness of VR interventions on daily living activities in children with DCD has been emphasized (EbrahimiSani et al., 2020). Significant improvements in daily living activities were observed in both groups. However, it was found that the study group receiving VR exhibited more pronounced effects in terms of activity levels compared with the control group. The magnitude of improvement in daily living activities observed in the study group, reflected by a large effect size, highlights the substantial clinical relevance of the intervention beyond statistical significance. Such a large effect size may have important implications for clinical decision-making, suggesting that VR-enhanced interventions should be considered a priority when aiming to improve daily living performance in children with DCD. This finding suggests that the addition of VR to COT leads to a greater improvement in daily living activities and indicates that such interventions could be an effective rehabilitation method.
Despite the positive findings in our study, there is a limitation that could be addressed in future research: the lack of long-term follow-up. Long-term follow-up studies would be important for the generalizability of the findings. Given the importance of early intervention in children with DCD, our study focused on younger age groups. However, it would be valuable to investigate the effects of VR intervention within the ICF framework in adolescents with DCD as well. Additionally, the small sample size in our study is another limitation, and larger sample sizes would help strengthen the dissemination of the results. An important limitation of the present study is the lack of formal assessment of environmental facilitators and barriers, which are essential components of the ICF framework. Although the intervention setting was standardized to minimize environmental variability, future research should incorporate both quantitative and qualitative measures to capture the contextual influences on activity and participation outcomes more comprehensively. Another limitation is that comorbid conditions commonly associated with DCD, such as ADHD and learning disabilities, were not distinguished for in this study. The impact of these comorbid conditions could affect children’s performance in different ways, so it would be beneficial to consider these factors in future research. Although VR has shown promising results in therapeutic settings, the cost of equipment and software can be a significant barrier to widespread adoption, particularly in clinical environments with limited budgets. Future studies could benefit from a more explicit inclusion of environmental factors to enhance ecological validity. To overcome these challenges, future research and developments should focus not only on improving VR technologies but also on creating cost-effective solutions and providing accessible training programs for health care professionals.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: ▪ The study emphasizes that integrating VR with COT can significantly improve motor, sensory-perception, and cognitive skills and activity levels in children with DCD. ▪ This highlights the potential for VR to serve as a powerful adjunct to traditional therapy, offering an innovative approach to target motor coordination, sensory processing, and cognitive skills. ▪ Occupational therapists should consider incorporating VR into therapy plans to optimize treatment effectiveness, particularly for children facing motor planning and coordination difficulties.
Conclusion
This study demonstrates that the addition of VR intervention to COT enhances the motor, cognitive, and sensory-perceptual skills and the activity levels of children with DCD and that, especially, it is more effective than COT alone in improving gross motor skills, executive function, praxis skills, and functional independence in activities of daily living in children with DCD.
Supplemental Material
Supplementary material for Effects of Virtual Reality Among Children With Developmental Coordination Disorder: An ICF-Based Randomized Controlled Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051134.pdf for Effects of Virtual Reality Among Children With Developmental Coordination Disorder: An ICF-Based Randomized Controlled Study by Zeynep Kolit, Koray Kara and Sedef Şahin in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This article was registered with the ClinicalTrials.gov registry (NCT06246318). This study was supported by TÜBITAK.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.