
Abstract
This study aimed to enhance the assessment of activity participation for people with upper extremity nerve injuries.
Peripheral nerve injury (PNI) of the upper extremity can significantly disrupt sensorimotor function, often leading to long-term disability and reduced participation in work and leisure activities (Novak et al., 2010). Despite optimal surgical interventions and extended rehabilitation efforts, approximately 57% of patients with PNI report unsatisfactory outcomes (Lundborg & Rosén, 2007; Padovano et al., 2022). These persistent poor outcomes limit physical functioning, mental health, and social participation (Bailey et al., 2009; Miller et al., 2017). Unfortunately, there are limited activity-focused assessments available that allow therapists to effectively measure the impact of PNI on patients’ participation.
Participation is defined as engagement in meaningful activities that are important for the patient’s sense of identity and well-being (Law, 2002). Occupational therapy has the potential to facilitate activity engagement among patients after PNI (Bailey et al., 2009). However, it remains difficult to quantify how PNI impairments limit patients’ engagement in relevant daily activities.
PNI impairments have clear effects on many patients’ motor performance, but the relationship between impairment, performance, and participation remains complex and poorly understood. For instance, Kim et al. (2024) found that positive PNI patient outcomes were linked to both preserved function and utilization of the affected hand, but another latent (i.e., underlying unmeasured influence) factor represented the possibility of positive outcomes despite poor function of the affected hand. It remains challenging to measure participation after PNI because existing measures fail to capture hand-specific activity domains (Thomas, 2012; Walker et al., 2003) or are insufficiently sensitive to detect change in activity engagement over time (Mallinson & Hammel, 2010).
A commonly used assessment in upper extremity rehabilitation is the Quick Disabilities of Arm, Shoulder, and Hand questionnaire (QuickDASH; Beaton et al., 2001, 2005; Hudak et al., 1996). Although it includes items on activity limitations such as the ability to use a knife to cut food, it primarily measures disability rather than engagement in meaningful activities (Franchignoni et al., 2014). Its brevity may also limit sensitivity to individual differences in activity participation after PNI (Novak et al., 2010).
The Activity Card Sort (ACS; Baum & Edwards, 2008) is a widely used measure of participation that has been used in research and clinical practice to quantify activity engagement and change in patients with varying performance levels (Baum & Edwards, 2008; Chan et al., 2006). Scores are reported in terms of percentage of preinjury or illness activities retained, where higher scores indicate greater retention. Recent work has increased the ACS’s specificity by classifying activities into one or more of 12 “dimensions” representing skill demands required to perform the activity (Anthony et al., 2024), as rated by a group of several hundred people. Examining these dimensions separately should make it possible to characterize the effects of an isolated sensorimotor disorder such as PNI on participation; but to our knowledge, the ACS has not been used to measure participation after PNI, particularly since the development of demand-based activity dimensions.
The objectives of this study were to understand the effects of PNI on participation in specific kinds of activities on the basis of their motor demands (i.e., fine motor [FM], gross motor [GM], bimanual [BM]) and to promote the adoption of patient-centered methods to guide more activity-focused and targeted interventions. Our hypotheses were as follows: After injury to the dominant hand (DH), reduced participation is more likely for activities with FM demands versus activities with only GM or no motor demands. Activity retention scores in FM activities will be correlated with DH dexterity among patients with DH injury. Among patients with injury to the nondominant hand (NDH), activities with BM demands will show reduced retention compared with activities with unimanual demands.
Method
Study Overview and Participants
This was a cross-sectional observational study of 48 adults with unilateral PNI to the upper extremity. We produced this sample by contacting all potentially eligible patients from the total patient census at two recruitment sites over a period of 16 mo (see Philip et al., 2022, Figure 1, for full flowchart). The recruitment sites were the nerve injury clinic at the Center for Nerve Injury and Paralysis and the Milliken Hand Center outpatient hand therapy clinic, both at the School of Medicine, Washington University in St. Louis. Demographics and historical details are listed in Table 1. Inclusion criteria included: ages 18 yr and older, English-speaking ability, unilateral upper extremity PNI (defined as nonpathologic), and QuickDASH scores of 18 and higher (Beaton et al., 2005; see Philip et al., 2022, for the threshold rationale) at the start of the study session. Exclusion criteria included cognitive disorders, uncorrected visual impairment, chronic pain diagnosis (unrelated to PNI), major mental health diagnosis, surgery within the preceding 2 mo, or motor function diagnosis that has affected the arm contralateral to their PNI in preceding 2 yr (Kim et al., 2024). All participants gave informed consent, and all procedures were approved by the Washington University in St. Louis Institutional Review Board. Data were stored and managed through the Research Electronic Data Capture System (REDCap; Harris et al., 2009). The dataset for this study is available online (Baune et al., 2024).
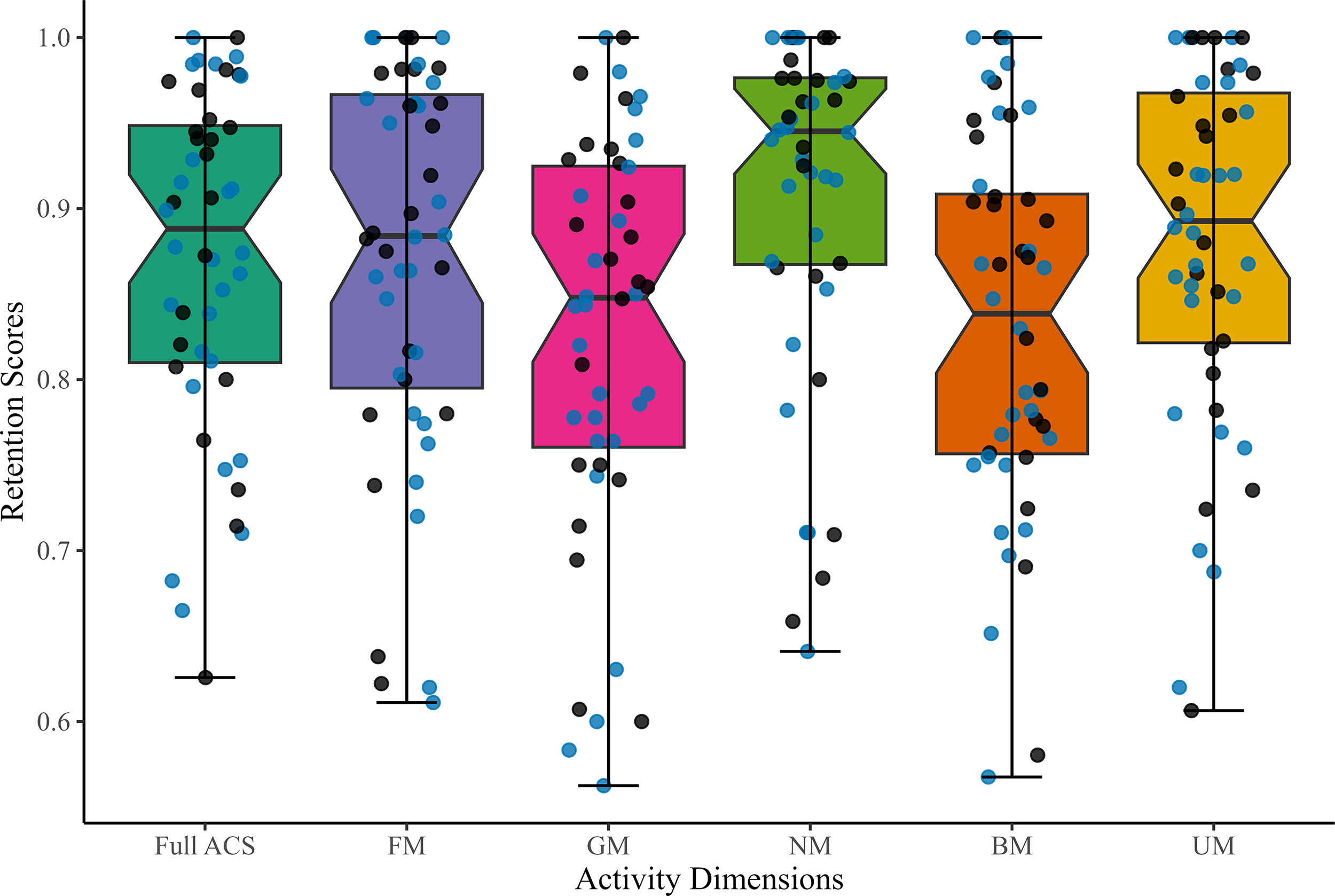
Retention scores for the full ACS and the five activity dimensions of interest. Note. N = 48. Boxplots represent quartiles, whiskers represent minimum and maximum, and dots represent individual participants (black = dominant hand injury; blue = nondominant hand injury). Overall, retention scores appear relatively similar across the five dimensions (FM, GM, NM, BM, and UM) compared with the full ACS scores. The GM and BM dimensions exhibit lower retention among participants. ACS = Activity Card Sort; BM = bimanual; FM = fine motor; GM = gross motor; NM = nonmotor; UM = unimanual.
Demographic and Injury Characteristics of Study Participants
Note. M (SD) or Mdn (range) are presented for numerical data; n (%) are presented for categorical data. No participants identified as Asian American/Pacific Islander or Hispanic/Latino. Group differences were analyzed using t tests for normally distributed numerical data, signed-rank tests for nonnormally distributed numerical data (U), and χ2 tests for categorical data. Correction-adjusted statistics are provided for cells with counts less than 5. “Other” injury causes = one tumor, one infection, one unknown. DH = dominant hand; NDH = nondominant hand; OT = occupational therapy; PT = physical therapy; QuickDASH = Quick Disabilities of Arm, Shoulder, and Hand questionnaire.
Measures and Procedures
Primary Measure
Participants in this study completed the second edition of the ACS (ACS–2; Baum & Edwards, 2008), which included 97 activities. Because activity dimensions (Boone et al., 2022) were based on the 100 activities in the third edition of the ACS (Anthony et al., 2024), and our data were collected with the ACS–2, we reviewed the entire ACS–2 to ensure that the dimensions of interest for this study included all relevant ACS–2 items. We identified 24 activities in the FM dimension (“activities needing the ability to manipulate small objects with hands”), 23 in the GM dimension (“activities that require the ability to coordinate body parts and limbs”), and 31 in the BM dimension (“using both hands to accomplish the activity”), as shown in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
In addition, two new dimensions were developed by the authors as logical transformations of existing dimensions. Twenty-one activities were identified as the Unimanual (UM) dimension (“activities that require motor skills in one hand”; [FM or GM, but not BM]), and 29 activities were identified as the Nonmotor (NM) dimension (“activities that do not require motor skills” [neither FM nor GM]; see Table A.1 in the Supplemental Material). The classification process was performed independently by two members of the research team, both with expertise in upper extremity rehabilitation. Discrepancies were resolved through consensus. To further minimize potential bias and enhance validity, an external reviewer with expertise in activity participation assessment (one of the developers of the ACS) independently reviewed the activity mapping, and their feedback was incorporated into the final classifications.
An inherent challenge in classifying complex activities is that some tasks may logically fall into more than one dimension. Three activities fell into both FM and GM categories (6.4% of all FM or GM activities): “fixing things around the house and grounds,” “car maintenance,” and “rock climbing.” The presence of multidimensional activities follows the original mapping by Anthony et al. (2024). Although this approach improves ecological validity by reflecting the complexity of real-world activity performance, it could potentially introduce some minor ambiguity in interpreting dimension-specific outcomes.
The primary outcome for each dimension was the percentage of activities retained, calculated as [(no. of activities performed currently + (0.5 × no. of activities performed less)]/(no. of activities performed before injury) × 100 (Katz et al., 2003).
Secondary Outcome Measures
ACS activity retention was compared with 39 variables: four hand dexterity, two muscle strength, three patient-centered, and 30 injury-related variables (14 constructs plus dummy variables). To make positive scores indicate better performance, variables were transformed through the equations score × −1 or 1 − score where needed.
Dexterity Variables
To identify the relationship between the FM retention scores and dexterity, three assessments produced a total of four hand dexterity variables (all in the affected hand only).
The first was the Jebsen–Taylor Hand Function Test (JTHFT; Jebsen et al., 1969). Four of its eight subtests were selected for analysis in this study (small object grasp, simulated feeding, stacking checkers, and stacking heavy objects) on the basis of factor analysis showing that only these four subtests measure unique constructs (Jarus & Poremba, 1993). The outcome variable was the average time across subtests (ceiling minus actual time, in seconds).
The second assessment was the Nine-Hole Peg Test (NHPT; Kellor et al., 1971) from the NIHToolbox (Gershon et al., 2013), which measures finger dexterity by asking participants to move pegs as quickly as possible. The outcome variable was completion time (ceiling minus actual time, in seconds).
The third assessment was the Precision Drawing Task (Philip & Frey, 2016; Philip et al., 2021). In brief, participants use a stylus and a Cintiq 13HD Touch digitizing tablet (Wacom Company) to draw a line within hollow geometric shapes (see Figure A.1 in the Supplemental Material) as quickly as they can while minimizing errors (e.g., going outside shape boundaries). Dexterity was quantified using several variables drawn from data at 30 Hz (Philip & Frey, 2016), of which two were used here. The first variable, “velocity smoothness” (“smoothness” for brevity), which represents fewer submovements per movement, was calculated as –1 × the number of velocity peaks per 45-mm shape segment (Philip et al., 2021). The second variable was “speed accuracy tradeoff,” which was calculated as speed (centimeters per second) divided by number of errors per segment (Kim et al., 2024).
Muscle Strength Variables
Grip strength was assessed using the Jamar dynamometer (Mathiowetz et al., 1984). Pinch strength, including tip, key, and palmar pinch, were measured using the pinch gauge (Mathiowetz, Kashman, et al., 1985). For each assessment, participants completed three trials, and the mean scores (reported in pounds) were z-scored across participants.
Patient-Centered Variables
We assessed disability with the QuickDASH (Beaton et al., 2001, 2005). The outcome variable was converted to “ability” (0–100) using the formula of ceiling − score.
Health-related quality of life (HRQoL) was assessed with the Patient-Reported Outcome Measurement Information System–29 (PROMIS–29; Cella et al., 2010), a questionnaire of physical functioning, anxiety, depression, fatigue, sleep disturbance, social functioning, and pain. The outcome variable was HRQoL, measured as the PROMIS–29 total score (range = 0–100).
Depression was assessed with the Patient Health Questionnaire–9 (PHQ–9; Kroenke et al., 2001). The outcome variable was converted to “not depressed” (%) through the equation 1 − (PHQ9 depression score/PHQ9 maximum possible score).
Injury-Related Variables
To explore possible influences on participation from clinical factors (demographic, injury related, and treatment related), we analyzed an additional 30 clinical and potential confounding variables (14 constructs). Variables included age (in years); gender; months since injury; months since surgery; number of occupational therapy prescriptions; number of physical therapy prescriptions; affected side (DH/ NDH); nerve transfer surgery (yes–no); multiple nerves (yes–no); injury severity (ordinal; neuropraxia, axonotmesis, or neurotmesis; Seddon, 1942); and four constructs that require detailed description: low pain, injured nerve, lesion location, and injury cause.
Pain was rated as “recent injury–related pain” (range = 0–10), and scores were then converted to “low pain” through 1 − (score/ceiling score) transformation, so higher scores indicate lower pain level as a percentage. One participant did not report their pain, so their value was imputed as equal to the pain question on the PROMIS–29.
Three nerve-related constructs (injured nerve, lesion location, and injury cause) were described by a series of categorical dummy variables (yes–no). “Injured nerve” was converted into seven dummy variables: ulnar, median, radial, posterior interosseous, anterior interosseous, cutaneous, and other. “Lesion location” was converted into seven dummy variables: brachial plexus or thoracic outlet (treated as a single “medial–superior” location because only one patient had thoracic outlet syndrome), upper arm, elbow, forearm, wrist, hand, and digit. “Injury cause” was converted into four dummy variables: trauma, surgical complication, chronic compression, and other.
Data Analysis
We completed all statistical analyses using the R package (Version 4.2.1). Normality was tested using the Shapiro–Wilk test (Shapiro & Wilk, 1965). All analyses were performed at two-tailed α = .05.
Hypothesis 1: Comparing Activity Retention Rates Between Activity Dimensions
To identify the predictors of multiple outcome variables (dimensions) with a large proportion of zeros (i.e., participants who retained 100% of activities in a dimension), we used a two-part random effects model (Liu et al., 2019). In this model, the probability of observing a zero outcome is modeled using logistic regression (the zero part), whereas nonzero outcomes are handled using a linear regression model assuming a log-normal distribution (linear part). Random effects are included in both parts to address the correlation arising from repeated measurements (i.e., the multiple dimensions).
We used a two-step approach to select covariates in each part of the model (zero part and linear part). In the first step, a univariate analysis was conducted for each dimension (FM, GM, and NM) to identify predictors with notable associations (p ≤ .1) with outcomes, using a univariate test that was appropriate to the data type (continuous = Kendall’s τ correlation; two-level categorical = Mann–Whitney U test; more than two–level categorical = Kruskal–Wallis H test). In the second step, we performed a multivariate analysis using the predictors identified in the univariate step. This two-step approach was performed separately for each part (zero and linear), because a predictor could have different effects on each part. In other words, a predictor’s effect on whether activities were lost might differ from its effect on extent of activity loss.
For the zero part analyses, each participant’s score in each dimension was converted to a binary variable (1 if any activities were lost, and 0 if not). For the linear part analyses, we converted the participation scores from a left-skewed distribution to a γ distribution by converting “retained” to “lost” (100% − percent retained); all values were reconverted to “retained” for reporting.
Hypothesis 2: Comparing FM Activity Retention With Hand Dexterity
To test whether FM activity retention was associated with hand dexterity in patients with DH injury, we calculated Spearman correlation coefficients between FM activities’ percentage retained scores and the four hand dexterity variables. Only cases with complete observations were used (n = 20). We used the Holm method (Holm, 1979) to correct for multiple comparisons and maintain a significance level of .05.
Hypothesis 3: BM Activities After NDH
To test the hypothesis that BM activities would be more impaired than UM activities in the NDH-injured group (n = 26), we compared retention scores. Because of nonnormal distributions in both dimensions, comparisons used the Wilcoxon signed-rank test, a nonparametric version of the paired-samples t test.
Results
Descriptive Statistics
Retention scores were broadly similar across the five dimensions and the full ACS–2, as shown in Figure 1.
When Activities Were Lost After DH Injury, FM Skill Activities Were More Likely to be Retained than GM Skill Activities
To identify patient characteristics associated with the extent of activity retention after DH injury (n = 22), we first focused on the “linear part” of our two-part model. Seven predictors were identified by our univariate analysis: months since injury, nerve-posterior interosseous, location-digit, location-hand, low pain, not depressed, and HRQoL. Using these seven predictors, our multiple “linear part” model found a significant effect of only HRQoL (estimate, 5.58; 95% confidence interval [CI] [0.64, 10.52], p = .03), which indicated that higher HRQoL was associated with higher retention for all dimensions; a significant main effect of GM versus NM activity retention (estimate −0.80; 95% CI [−1.16, −0.45], p < .001); and a marginally significant trend of FM versus NM activity retention (estimate, −0.35; 95% CI [−0.71, −0.00], p = .05). For full model results, see Table 2. In brief, FM activities were better retained than GM activities, and FM activities were retained only marginally less than NM activities, which contradicts our hypothesis that FM activities would be least retained.
Two-Part Model Results for the Dominant-Hand Injured Group
Note. N = 22. Values in bold indicate statistically significant p values (p < 0.05). CI = confidence interval; FM = fine motor; GM = gross motor; HRQoL = health-related quality of life; LL = lower limit; UL = upper limit.
Whether Activities Were Lost After DH Injury Depended Only on Pain
We identified predictors that were associated with the odds of activities being lost (binary, yes–no) through the zero part of our model. Here, two predictors (low pain and location-digit) met our univariate criterion, but low pain had a significant main effect in our multiple model (estimate, 3.37; 95% CI: [0.24, 6.49], p = .03). In other words, participants with lower levels of pain were more likely to report retention of all activities.
Hand Dominance Did Not Affect Activity Retention
On a post hoc basis, we repeated the aforementioned analysis on all patients (N = 48), with affected side (DH vs. NDH) forced into the model. We found no effect of affected side, and this analysis produced the same pattern of results as our initial analysis (patients with DH injury only), as shown in Table A.4.
FM Activity Retention Is Not Correlated With Hand Dexterity
We quantified the relationship between DH dexterity and FM activity retention (in patients with DH injury) by means of correlation analysis. We found weak correlations (|ρ| ≤ 0.31, p > .4) and similar results for GM activities (|ρ| ≤ 0.13, p = 1.0; Figures A.2, A.3, and A.4). Therefore, our data did not support the hypothesis that FM activity retention is correlated with dexterity.
Higher Retention for UM Activities than BM Activities, Regardless of Injury Side
We compared retention of BM activities with retention of UM activities in patients with NDH injuries using a Wilcoxon signed-rank test. BM activities (median = 0.83; range = 0.57–1.00) were less retained than UM activities (median = 0.89; range = 0.60–1.00; rank sum = 27, p = 2.8 × 10−4), as shown in Figure 2. This effect was consistent across participants, regardless of injury side, with consolidated data showing a similar trend (N = 48; rank sum = 70; p = 2.83 × 10−7), as shown in Figure 1 (orange vs. yellow). Further details and post hoc analyses are provided in Figure A.5 in the Supplemental Material.
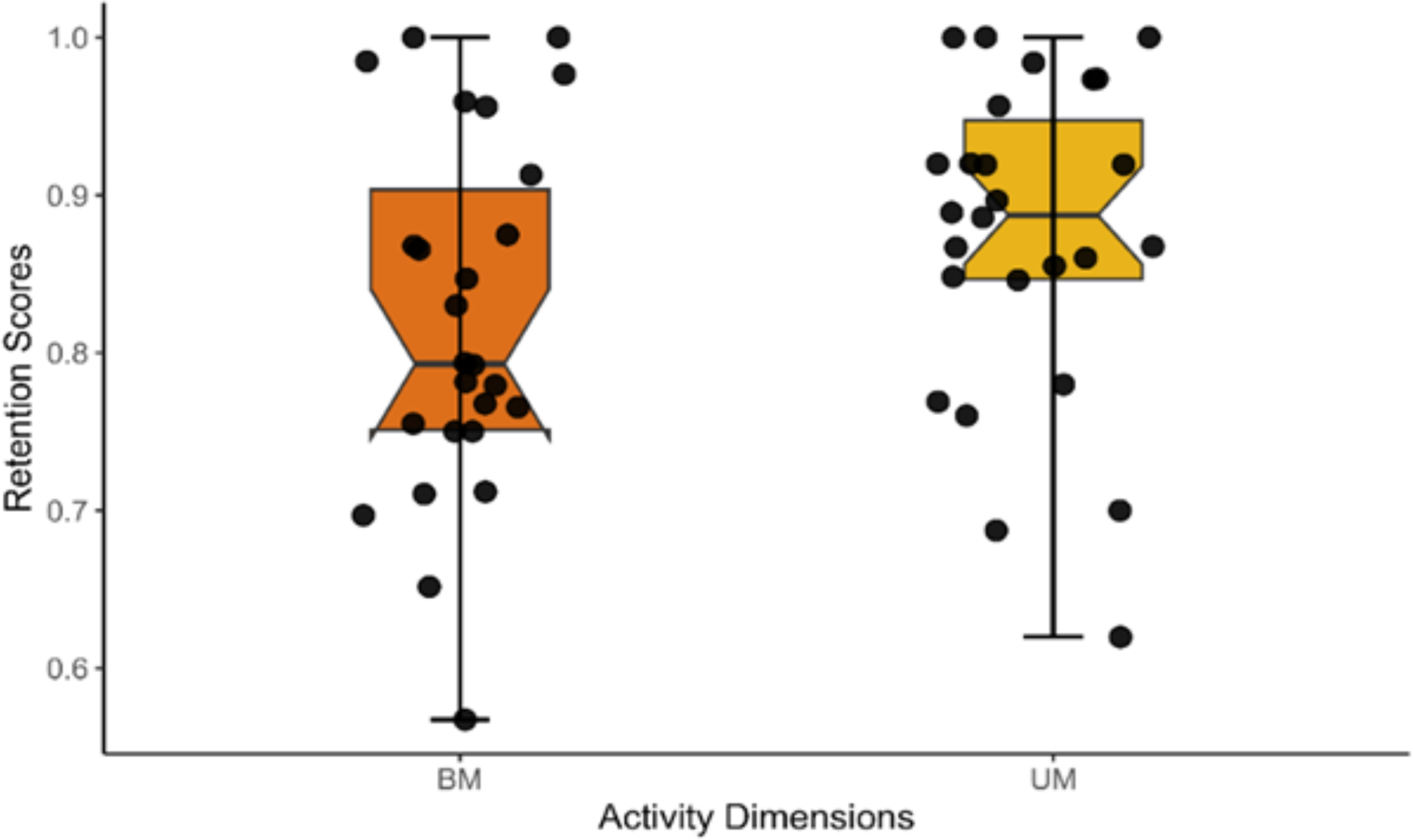
Higher retention for UM activities than BM activities for the group with nondominant hand injury. Note. N = 26. Boxplots represent quartiles, whiskers represent minimum and maximum, and dots represent individual participants. The plots show a greater variability in the retention scores observed in the BM dimension. BM = bimanual; UM = unimanual.
Discussion
After unilateral peripheral nerve injury (PNI), effects on activity participation have previously been difficult to quantify because of inadequate measurement tools. In this study, we separated the ACS activities into dimensions with distinct types of motor demands, which allowed us to identify three previously unknown consequences of PNI: Activities with GM demands were more likely to be lost than activities with FM demands; hand dexterity was not correlated with activity retention; and patients were more likely to retain UM than BM activities, regardless of whether their injured hand was their DH.
After DH Injury, GM Activities Had Lowest Retention
We hypothesized that retention would be lower for activities with FM demands than for those with GM or NM demands, because the hand’s intricate structure and dexterity are essential for the performance of daily activities and work. Most upper limb nerves innervate the hand, and even arm-specific injuries may impair the ability to deploy the hand (e.g., bring it to objects).
We found lowest retention for GM activities. One possible explanation is that these activities require coordination across multiple joints and the voluntary activation of large muscle groups. Proximal nerve injuries, which disrupt the innervation of these muscles, can impair motor unit recruitment and disturb normal muscle synergies, making GM tasks more difficult to perform and sustain (Enoka & Duchateau, 2017; He et al., 2014; Moscony, 2007). Other underlying patterns or confounds could also influence activity retention; for example, GM activities (16/23 activities outside) are more likely than FM activities (2/24 activities outside) to occur outside the home. Furthermore, GM activities on the ACS may also be BM in nature, because the dimensions were not orthogonal. However, the higher retention of FM activities should be interpreted with caution, because the apparent weak effect of PNI on FM retention could also simply arise from limitations of the ACS, as discussed later (see Limitations).
Overall, we did not find support for our hypothesis that FM activities would be less retained than other activities after PNI, despite the self-evident potential for nerve injuries to affect FM activities. Future research should identify new ways to isolate the unique impacts of nerve injuries on different motor skills.
Activity Retention Is Associated With Quality of Life and Low Pain, but Not Hand Dominance
The only variable associated with the extent of activity lost was HRQoL. This includes various dimensions of well-being, including physical, emotional, and social aspects, all of which could directly influence a person’s ability, desire, or motivation to engage in daily activities or could arise from stronger social support networks that also enable engagement in activities.
The only variable associated with the retention of activities was pain. Participants who experience lower pain levels are more likely to maintain participation in activities, reflecting improved functional outcomes. Our findings highlight the importance of addressing pain as a key factor in occupational therapy for patients with PNI. This is consistent with previous research showing that lower pain levels are associated with greater participation and improved quality of life (Bailey et al., 2009; Stonner et al., 2021). Pain can limit activity participation, but effective management strategies can support continued activity engagement and a sense of well-being.
We found no effects of hand dominance (i.e., which hand was injured) on activity retention, whether we analyzed DH-injured patients alone or all patients. It remains unclear why hand dominance has no visible impact on activity participation, even though the DH typically has greater dexterity (Azad et al., 2017) and is more frequently used (Gonzalez et al., 2007). Preserved participation after DH injury is unlikely to arise from compensatory increased use of the NDH, because most patients with PNI do not engage in such compensation (Philip et al., 2022), at least for activities previously studied. Alternatively, the ACS might be relatively insensitive to asymmetric impairment, as discussed later (see Limitations).
Motor Activity Retention Was Not Correlated With Dexterity
We found no significant correlations between hand dexterity and retention of FM (or GM) activities. This lack of dexterity–participation relationship is consistent with previous findings that performance-based measures of dexterity often do not strongly correlate with participation outcomes after PNI (Kim et al., 2024; Philip et al., 2022). This implies that activities with motor demands may depend more on factors other than pure dexterity, such as cognitive aspects, motivation, compensatory strategies, or social support (Heinzel et al., 2021). Most studies in the PNI population have focused on impairment and functional recovery, with relatively few examining how these outcomes translate to meaningful activity engagement. Future studies should investigate the role of compensatory mechanisms and adaptive techniques used by patients to maintain activity participation despite dexterity limitations.
Although measures such as the JTHFT and NHPT do not directly correlate with participation outcomes, they remain useful for quantifying impairment during the early stages of FM and GM recovery (Lang et al., 2013), but their limitations should be recognized. The JTHFT may not fully capture subtle residual deficits because of its reported decreased responsiveness (Sears & Chung, 2010). Similarly, the NHPT may be less effective for evaluating intervention effectiveness in higher functioning patients (Mathiowetz, Weber, et al., 1985) with more skilled functional demands.
Unimanual Activities Were Better Retained Than BM Activities
Partly consistent with our third hypothesis, UM activities were better retained than BM activities, but this effect was not unique to patients with NDH injury. UM activities may be better retained because of their lower complexity and/or because the reliance of those activities on a single limb makes compensation easier to achieve (e.g., by using the other arm). Because most daily activities are BM (Ahn & Hwang, 2018), the greater impact on BM activities highlights the functional limitations faced by patients after PNI.
Implications for Occupational Therapy Practice
This study highlighted differences between dexterity and participation as well as the difficulty of identifying FM limitations with standard activity assessments such as the ACS. These findings suggest several implications for occupational therapy practice in the rehabilitation of individuals with peripheral nerve injury: Tailor rehabilitation strategies to each patient’s needs, using individualized assessments such as the Canadian Occupational Performance Measure (Law et al., 1990). Design interventions that specifically target improvements in bimanual coordination and muscle strength. Encourage compensatory strategies when bimanual function is limited, provided they support participation in meaningful activities.
Limitations
The apparent weak effect of PNI on FM retention could arise from limitations of the ACS. Despite the ACS’s good test–retest reliability and internal consistency of subtests (Baum & Edwards, 2008; Katz et al., 2003), it was designed as a measure of participation in instrumental activities and, thus, may not capture functionally significant activities that require precision motor control in other domains, such as specific work activities (e.g., handling tools) or activities of daily living that require sustained precision grips (e.g., buttoning clothes). Similarly, the ACS does not evaluate the relative importance of different activities—only the variety of activities.
The ACS might also be insensitive to asymmetric impairment: Self-reported hand use does not accurately reflect hand use patterns (Flindall & Gonzalez, 2019), and multiactivity surveys can obscure dominance-dependent effects that emerge only in a few high-demand or lateralized activities (Philip et al., 2017).
A small number of activities (6.4%) were classified into both FM and GM dimensions. This was an intentional choice to reflect complex demands in real-world participation. Although this approach enhances ecological validity, it may introduce minor ambiguity in dimension-specific interpretations. We addressed this through a structured classification process with external expert validation. Moreover, these multiple classifications reflect a ground truth (some activities do require, e.g., both FM and GM skills), so this problem is a necessary tradeoff when studying complex multidimension activities.
This study had a small sample size; therefore, its conclusions may not be universally applicable across the heterogenous spectrum of nerve injury cases. Additionally, our sample predominantly contained participants who identified as White (77%), which limits generalizability. Future studies should aim to recruit more representative cohorts to examine cultural and demographic influences on participation outcomes.
Conclusion
Although FM activities were more frequently retained than GM activities, the effect was weak and may arise from multiple causes: preserved FM function, compensatory strategies, and/or limitations of the ACS in detecting subtle FM impairments. Rehabilitation should address both GM and FM activities, recognizing that many tasks involve overlapping motor demands. Because standardized assessments may not always capture these impairments, activity-based evaluations are essential to identify functional limitations and guide individualized treatment. In addition, although motor demands contribute to activity retention, they do not fully explain it. Participation is shaped by multiple, interacting factors including pain, perceived quality of life, compensatory strategies, and the unique demands of BM coordination. Even in unilateral injuries, difficulties with BM tasks may emerge and should be considered in rehabilitation planning. Effective pain management is also essential to support activity engagement and enhance recovery. Together, these findings highlight the need for individualized, targeted interventions that are based on each patient’s specific impairments and participation goals.
Supplemental Material
Supplementary material for Activity Loss and Retention Patterns Following Unilateral Peripheral Nerve Injury: Implications for Rehabilitation
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051142.pdf for Activity Loss and Retention Patterns Following Unilateral Peripheral Nerve Injury: Implications for Rehabilitation by Samah Gassass, Ruiwen Zhou, Robin Hattori, Lei Liu, Lisa Tabor Connor and Benjamin Allen Philip in The American Journal of Occupational Therapy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.