
Abstract
The authors developed the Virtually Guided Infant Developmental Abilities (VIDA) screening tool to address the lack of virtual developmental assessments for children with complex medical conditions.
Advances in neonatal medicine have increased the survival of infants born with complex medical conditions, such as prematurity, genetic syndromes, and metabolic disorders, which necessitate treatment in a neonatal intensive unit care (NICU; Helenius et al., 2017). Approximately 13% of all live births in the United States require NICU care, which represents an annual rate of up to 3.6 million newborns (Schulman et al., 2018). Survivors of the NICU are at increased risk of long-term medical issues and neurodevelopmental sequelae that affect both their and their families’ quality of life (Payot & Barrington, 2011).
The timely identification of developmental delays is critical to the future well-being of infants treated in the NICU (Majnemer & Rosenblatt, 2000). Important health care services are traditionally performed during in-person, neonatal follow-up visits, when important care is undertaken. Neonatal follow-up involves a multidisciplinary team, which can consist of occupational therapists, physical therapists, speech-language pathologists, and neonatologists, who work together to integrate information obtained from inquiries about parental concerns, clinical observations, and the use of standardized developmental measures to identify children at increased risk for developmental or physical delays (Synnes et al., 2006). Standardized developmental measures encompass direct hands-on assessments of the child’s gross motor, fine motor, cognitive, social, and language skills at specific ages to determine whether that child is reaching age-defined milestones. Standardized developmental assessments must meet several criteria, including adequate reliability and validity, to be considered appropriate for clinical purposes (Furnham, 1998).
Even before the coronavirus disease 2019 (COVID-19) pandemic, myriad geographic, socioeconomic, and provider-level factors presented significant barriers that hindered numerous families from accessing the neonatal follow-up care they required (Ballantyne et al., 2014, 2020; Brady et al., 2018; Lipner & Huron, 2018). Most health care providers are concentrated in metropolitan areas, requiring some families to travel long distances. Neonatal follow-up visits may take half-days or longer, meaning some family members have to miss work. These challenges disproportionately affect underresourced families who are facing financial constraints or geographic limitations (Ballantyne et al., 2015, 2020; Brady et al., 2018; Lipner & Huron, 2018; Swearingen et al., 2020). These challenges, combined with the fact that in-person nonurgent hospital visits were canceled during the COVID-19 pandemic, strongly highlight the need for a novel way of providing critical neonatal follow-up care (Albayrak et al., 2021; DeMauro et al., 2021).
The COVID-19 pandemic temporarily rendered telerehabilitation the only means by which to provide essential neonatal follow-up care to this population (Abdel-Wahab et al., 2020; Adelman et al., 2021; Ajami & Mohammadi, 2020; Albayrak et al., 2021; DeMauro et al., 2021). Providers and families recognize the benefits of telerehabilitation, including reduced financial and transportation barriers, improved flexibility, and greater access for underresourced areas (DeMauro et al., 2021; Haffner & Bauer Huang, 2023; Ray et al., 2017). Virtual visits also create a family-centered approach that allows clinicians to observe children in their natural environment, where they are more comfortable and likely to demonstrate skills not always performed in the clinical setting (DeMauro et al., 2021; Haffner & Bauer Huang, 2023; Ray et al., 2017). However, telerehabilitation has certain challenges, such as connectivity issues, poor video quality, and privacy issues (Desai et al., 2023). Despite these challenges, it remains a valuable approach for facilitating follow-up care accessibility (Montoya-Williams et al., 2024).
Several studies have demonstrated a possible role for telerehabilitation in addressing the medical and developmental needs of infants after NICU discharge (Albayrak et al., 2021; Church et al., 2021; Del Lucchese et al., 2024; DeMauro et al., 2021; Ke et al., 2024). However, these studies used standardized in-person developmental tools in a virtual medium, and the authors have acknowledged that as a significant limitation. To be specific, these assessments, which are typically designed for in-person assessments, rely on direct interaction between the child and the assessor or require specific manipulatives that are difficult to replicate remotely (Albayrak et al., 2021; DeMauro et al., 2021). As a result, when health care practitioners, including occupational therapists, attempt to conduct adapted forms of assessments during telerehabilitation neonatal follow-up visits, the data collected are unreliable because none of the tools have been validated with respect to psychometric adequacy when delivered through a virtual platform. This lack of appropriate validation has raised concerns regarding the accuracy and consistency of the assessments, limiting their usefulness in a virtual medium (DeMauro et al., 2021). Widespread failure to acquire timely and accurate developmental outcomes threatens the integrity of important neonatal follow-up care, potentially affecting the quality of life of millions of children and their families. A novel method for evaluating infants born with complex medical conditions is critically needed. Therefore, the goal of this study was to create the Virtually Guided Infant Developmental Abilities (VIDA) screening tool, which is intended for children ages 1–18 mo.
Method
Study Design
To create the VIDA screening tool, we used the Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research framework (Boateng et al., 2018). This framework outlines three phases for creating an assessment tool: Phase 1, item development and content validity; Phase 2, scale development; and Phase 3, evaluation through psychometric testing. This article focuses on Phases 1 and 2. This research project was approved by the Queen’s University Health Science Research Ethics Board.
Conceptual Basis
A conceptual basis was used to help guide the overall development of the VIDA screening tool. Infant development theory has progressed from early brain-centric models, such as neuromaturation theory, which describes the appearance and maturation of motor skills, to contemporary frameworks, such as neuronal group selection theory, which emphasizes the intricate interplay of multiple factors within the infant, the task at hand, and the surrounding environment, which collectively shape development (Calvin, 1988; Hadders-Algra, 2000; Polovina et al., 2010). Given the complexity of infant development, the creation of the VIDA screening tool was guided more by various principles that underlie neonatal, infant, and toddler development than by adherence to a single theory. The VIDA tool is notably influenced by Myrtle McGraw’s work in 1985 (e.g., McGraw & Haka-Ikse, 1985), which emphasizes that infant development involves a multisystem process in which different aspects emerge and progress at varying times and rates, eventually converging, integrating, and synthesizing to form new abilities or traits. This approach underscores the dynamic and interconnected nature of infant development, moving beyond linear theories to embrace the holistic and evolving nature of developmental progressions (McGraw & Haka-Ikse, 1985). The VIDA screening tool is unique in that it take a multifaceted screening approach that entails a combination of prompted responses and parent-identified abilities to assess a child’s developmental abilities. The tool’s focus is on the attainment of developmental milestones at specific ages rather than on movement patterns or characteristics. This approach to timing milestones was deliberately chosen for two primary reasons: because (1) delays in achieving these milestones can reveal underlying issues and (2) difficulties in mastering one skill can potentially lead to a cascade effect in which subsequent developmental progressions are affected.
Phase 1: Item Development
Identification of domain and item generation refers to creation of domains, the definition of each domain, and the identification of items within each domain (Boateng et al., 2018). To classify the domains of a child’s development, define each domain, and generate items, we used a deductive method via a literature scoping review to identify areas of child development and existing developmental assessment tools with robust validity and reliability properties.
Four independent researchers performed the scoping review using the Preferred Reporting items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA–ScR) as a guide (Tricco et al., 2018). The search strategy included four online databases, including MEDLINE, CINAHL, Embase, and Web of Science; identification of key search terms; inclusion and exclusion criteria; online database searches; and a well-defined search approach, including screening of full-text reviews. A total of 20 articles were included in the scoping review (Tricco et al., 2018). This scoping review revealed that no validated tools for virtual screening have been identified thus far. However, three assessments—including the Bayley Scales of Infant and Toddler Development, Third Edition (BSID–III; Bayley, 2006); the Caregiver Reported Early Development Instruments (CREDI; McCoy et al., 2021), and the Ages and Stages Questionnaire®, 3rd Edition (ASQ–3; Squires & Bricker, 2009)—were found to have the most supporting evidence. This scoping review has been published (Ghimire et al., 2024), and readers can refer to that article for an in-depth description of the methodology and findings. The three developmental assessments identified in the scoping review (i.e., BSID–III, CREDI, and ASQ–3), along with relevant literature, were subsequently used by the research team, which consisted of four experts in the field (two occupational therapists, one nurse, and one neonatologist), to identify the developmental domains, define the screening tool’s domains, and generate items.
Content validity refers to the adequacy with which a measure assesses the domain of interest. Content validity also specifies content relevance and content representations, that is, that the items capture the domain (Boateng et al., 2018). We used a modified Delphi survey technique (Niederberger & Köberich, 2021) to evaluate the content validity of the VIDA screening tool. We selected this methodological approach because there are no data on virtually guided standardized developmental assessments, and thus a computational approach could not be taken. Moreover, the Delphi survey method is ideal for generating items for tool development because it enables the systematic collection of expert opinions and facilitates consensus-building through multiple rounds of feedback, ensuring the inclusion of relevant and comprehensive content. It is especially effective in complex areas, such as developmental assessments administered through a virtual medium, where diverse expert input is crucial. In contrast, content validity measures, such as Cohen’s kappa or the content validity index (CVI), are more suitable for evaluating the validity of an already-developed set of items. The Delphi method focuses on refining and developing the tool’s items, whereas Cohen’s κ or the CVI would be applied later, to assess the degree of agreement among raters with respect to the clarity of the finalized items.
The research team developed an online survey using Queen’s University’s Qualtrics platform. The survey included a list of all the domains, their definition, a list of all items generated within each domain, and scoring type. Respondents were asked to judge the appropriateness of the domains, definitions, items generated, and scoring type using a 3-point Likert scale (1 = essential; 2 = useful, but not essential; 3 = not essential) and to add additional comments. A two-round self-completed online questionnaire with individual feedback also was conducted, to determine a consensus from a group of 12 experts. The experts were required to have at least 5 yr of experience in pediatrics, specifically in the developmental follow-up of high-risk infants, and a least some experience with developmental assessments administered through a virtual medium. Expert participants from a diverse group of multidisciplinary health practitioners, including an occupational therapist, a physical therapist, and neonatologists, were invited to participate. An analysis of the responses was performed by the research team between each round. As defined in the Delphi approach, for the child development domains, definition, items, and scoring methods to be deemed validated a respondent consensus of >70% must be reached (Niederberger & Köberich, 2021). A content analysis was performed on commentaries provided in the questionnaire that addressed item selection and scoring system.
Phase 2: Scale Development
A pilot test study is a critical step to ensure an instrument’s clarity and feasibility (Boateng et al., 2018). Its purpose is to determine the extent to which the domain and items are meaningful to the target audience, to ensure that the tool’s instructions and items are easily understood by the target audience, and to confirm content relevance. Two occupational therapists participated in the pilot testing of the VIDA screening tool until saturation was reached. All infants and their primary caregivers who met the eligibility requirements were recruited from the Kingston Health Sciences Centre’s neonatal follow-up clinic in Kingston, Ontario, Canada. Eligibility criteria included the following: infants born with a complex health condition that necessitated follow-up care after being discharged from the NICU, whose caregivers are designated decision-makers according to hospital policy and who are able to read and understand English. The person who considered themselves the child’s primary caregiver was asked to participate. After written consent was obtained, the caregiver was given an appointment. The occupational therapists who administered the VIDA screening tool were asked to provide written and verbal feedback on item relevance, clarity, and ease of administration. The feedback provided was used to gain insight into clarity (format, wording, and scoring system) and feasibility (logistic challenges, linguistic biases). The pilot test was conducted to confirm that the VIDA tool is practical for real-world application before formal psychometric testing is conducted.
Results
The VIDA screening tool development took place from March 2022 to September 2023 and was led by a multidisciplinary research team at the Kingston Health Sciences Centre. Figure 1 illustrates a flow diagram of the development strategy.
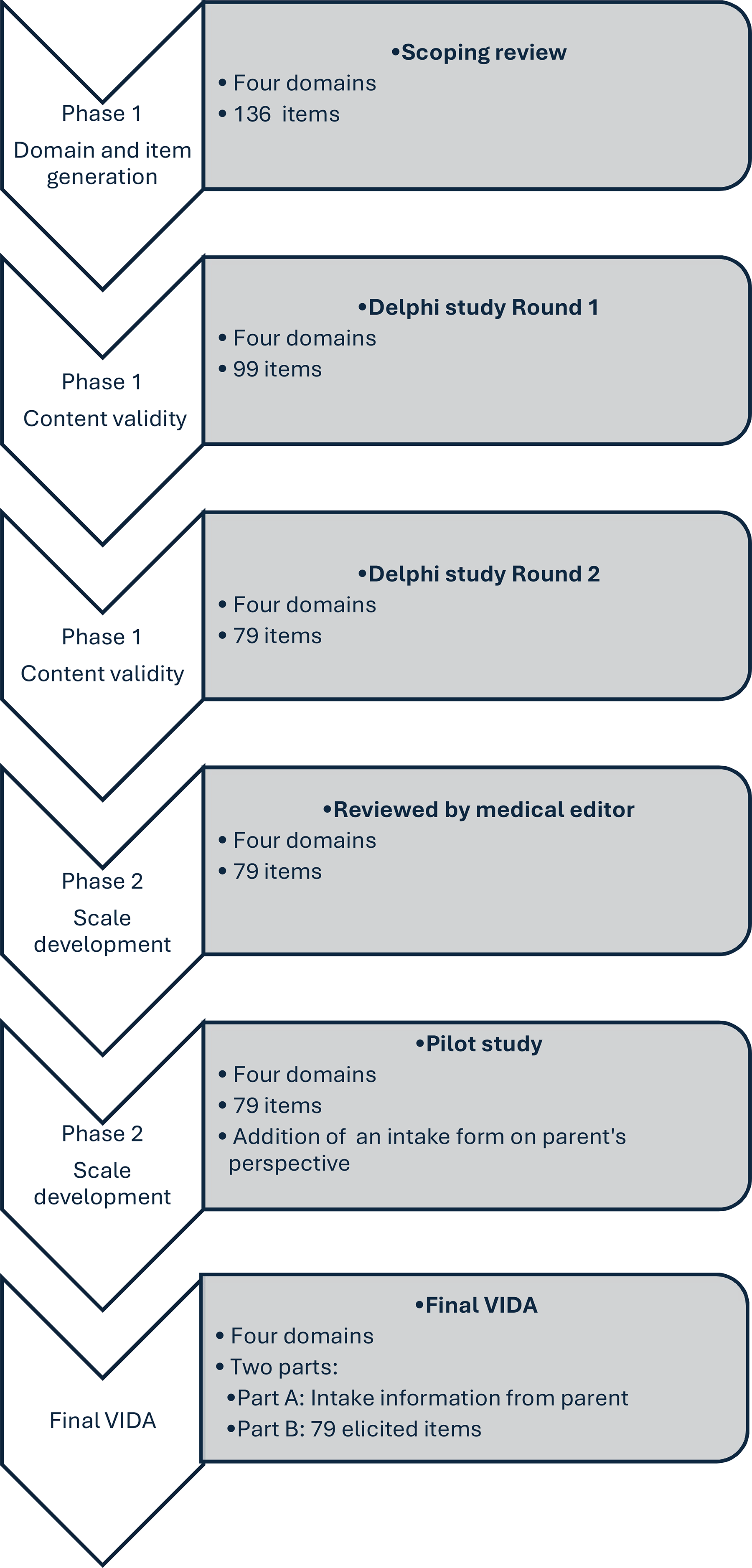
Flow diagram of the development strategy.
Phase 1: Item Development
Domain Identification and Item Generation
Using the relevant literature, along with the three developmental assessments mentioned earlier, (BSID–III, CREDI, and ASQ–3) we identified four child developmental domains. These include (1) Gross Motor Abilities, defined as skills that involve the control of large muscle groups responsible for major body movements in supine, prone, sitting and standing positions; (2) Fine Motor Abilities, described as skills that involve the control of small muscles, in particular those of the hands and fingers in different positions; (3) Social Communication and Cognitive Abilities, which are the cognitive processing skills needed to effectively interact and express one’s needs, emotions, and intentions with others in different contexts, such as pointing to objects, making gestures, and putting things (objects) together, which reflects early social and cognitive development; and (4) Self-Care Abilities, the skills needed to care for the self, such as feeding, toileting, and dressing. An initial list of items and types of scoring method to be included in the VIDA screening tool also was generated. This initial list consisted of 136 items.
Content Validity
A two-round Delphi survey study was then conducted using the Queen’s University Qualtrics platform. A total of 12 experts (12 in the first round and nine who continued in the final round) participated. Respondents consisted of a diverse group of interdisciplinary clinicians who included 10 occupational therapists, one physiotherapist, and one neonatologist. Each respondent was asked to judge the appropriateness of each of the 136 previously identified items using a 3-point Likert scale (1 = essential; 2 = useful, but not essential; 3 = not essential) and were asked to add additional commentaries. The first round generated 99 items, and the second round generated 96 items. Additional commentaries were reviewed, and 17 items were excluded because of duplication, resulting in a total of 79 items after the second round and commentary revision. The following items were included: 33 in the Gross Motor Abilities domain (six related to being supine, nine related to being prone, six related to being in a sitting position, and 12 related to being in a standing position), 10 in the Fine Motor Abilities domain, 18 in the Social Communication and Cognitive Abilities domain, and 18 in the Self-Care Abilities domain.
With respect to the scoring system, respondents were provided an opportunity to describe their preferred method for scoring and reporting and to provide feedback on either a 3-point (present, not present, unsure) or a 2-point rating scale (a dichotomous [e.g., yes/no] response to items). The majority of respondents preferred a dichotomous rating scale. On the basis on their feedback, we modified the dichotomous rating scale to include “Yes” or “No/Unsure” response options. A “Yes” response was intended to be used for item descriptors observed in session by an examiner or when a parent reported that they had observed their child accomplish the item. A “No/Unsure” response was intended to be used for item descriptors not observed by examiner or when parent reported did not know, or were unsure of, whether the child could accomplish the item.
An experienced medical editor reviewed the VIDA screening tool for clarity and comprehension and specifically to assess whether the instructions, item descriptions, and format were clear. No changes were made in the number of items after this review; however, adjustments were made to the wording and formatting to ensure that the tool is easily understood by the target audience.
Two occupational therapists participated in the pilot testing of the VIDA screening tool on three infants and their primary caregiver. Only three infants were tested because at this point saturation had been reached in the feedback provided. On the basis of the therapists’ feedback, two more items in the Fine Motor Abilities domain were included. Furthermore, reporting of results was simplified as having “delayed” or “not delayed” abilities in each domain if the child performs below their age in months in any one of the four domains. The occupational therapists also suggested the addition of information to obtain feedback on the parents’ perspective of the child’s developmental abilities, family well-being, and access to follow-up services.
Final VIDA Screening Tool
The VIDA screening tool is a virtually guided, family-centered approach that was designed to assess developmental abilities in infants age 1–18 mo because early identification of delays during this critical period will maximize the potential for timely support and improved outcomes. The VIDA screen consists of parent reports and examiner observations. It comprises two parts. Part 1 includes an intake form to gather information on family concerns regarding their child’s development and their own well-being. Part 2 consists of 79 items that focus on the infant’s performance across four domains: (1) Gross Motor Abilities (33 items, e.g., supine, prone, sit, stand), (2) Fine Motor Abilities (10 items) (3) Social Communication and Cognitive Abilities (18 items), and (4) Self-Care Abilities (18 items, e.g., feeding, sleeping, playing skills). Table 1 illustrates the items included in the VIDA screening tool.
VIDA Screening Tool Domains and Items
Note. VIDA = Virtually Guided Infant Developmental Abilities.
It takes approximately 30 min to administer. Items are scored dichotomously (yes = observed by the examiner or reported by parent, no/unsure = refers to items that are not observed by therapist or parent reports unsure/unable for child to complete the item). The VIDA screen does not provide a numerical score; instead, it classifies children as either developing typically (at their expected age level) or delayed (below their expected age level). A child is considered to have delayed development if they perform at least 3 mo below their age-expected level in any of the domains. We recognize that although the dichotomous classification of “delayed” versus “not delayed” simplifies reporting, it may overlook borderline cases. Dichotomous classifications are easier to use but less precise, whereas tools that use cutoff scores offer more accuracy but require greater expertise. However, the VIDA screening tool also incorporates parents’ concerns about their child’s development, which is valuable input. Furthermore, follow-up is recommended if any parental concern arises or if the child performs 3 mo below their expected age (delayed development) in any domain.
Discussion
The aim of this study was to create the VIDA screening tool for children ages 1–18 mo, with the intent of addressing the current gap in developmental assessment and screening tools that can be administered through a virtual medium. The process of using the Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research framework, led by a multidisciplinary team, along with expert consultation and a medical editor to develop the VIDA screening tool, provides confidence in its content validity (Boateng et al., 2018).
This study has several strengths. One is the use of a conceptual framework, which helped frame the development of the VIDA screening tool in the context of various principles that underlie neonatal, infant, and toddler neuronal development rather than by simple adherence to a single theory. Another strength is the methodological, stepwise fashion in which the two phases of the VIDA development were undertaken. In Phase 1, the item development was guided by the PRISMA–ScR framework, a well-established method for identifying current evidence. This was followed by a two-round Delphi survey study that encompassed 12 experts in various health professional fields, for the content development step. An advantage of using 12 expert opinions in an online format is that it ensures that all participants can express their own ideas anonymously (Niederberger & Köberich, 2021).
An additional strength is that Phase 2 included a review of the VIDA screening tool for clarity and comprehension by an experienced medical editor. It also involved conducting a pilot test study with practitioners and families to assess its clarity and effectiveness. A third and last strength of this work is the representation of multiple disciplines across members the research team. Expert opinion is important in developing a tool because it brings diverse knowledge and perspectives, ensuring that the tool is comprehensive and accurate and applicable across various contexts.
This study has several limitations. First, the small sample size of, and limited diversity among, the professionals involved in the Delphi study could have affected the representativeness of the expert input. Another limitation is the small sample size in the pilot test. In addition, the lack of parental feedback is a notable omission given that their perspectives are crucial in ensuring that the VIDA screening tool is applicable to a diverse group of parents. In future research, we plan to evaluate the VIDA screening tool with numerous and diverse families and health professionals to assess its acceptability and feasibility as well as to rigorously examine its psychometric properties (reliability and validity) in a broader population of children and their families.
Implications for Occupational Therapy Practice
The development of the VIDA screening tool offers occupational therapists a promising approach to support early developmental monitoring of high-risk infants, particularly those facing barriers to traditional, in-person follow-up care. By incorporating the VIDA tool into their practice, therapists can enhance access to timely developmental assessments, facilitate early identification of delays, and provide targeted interventions regardless of limitations. This tool represents a step toward more equitable care and underscores the importance of integrating virtual solutions into neonatal follow-up services.
Conclusion
In this study, we developed the VIDA screening tool, which was designed to support infants born with complex medical conditions, in particular those whose families encounter significant barriers to accessing in-person neonatal follow-up care. By leveraging virtual platforms, this tool aims to bridge gaps in health care access, ensuring that high-risk infants receive timely developmental assessments despite challenges such as geographical distance, financial constraints, or limited health care infrastructure. It also has the potential to improve the early identification of developmental delays, which ultimately will contribute to better long-term outcomes among high-risk infants. Furthermore, this study lays the foundation for future research to refine and validate this tool across larger and more diverse populations, thereby enhancing its effectiveness and scalability in addressing the needs of high-risk infants and their families.
Footnotes
Acknowledgments
We thank all the parents who participated in this study and the panel of 12 anonymous health professional experts. We also extend gratitude to Eleftherios Saleos, Director of Lifelong Learning & Innovation at Queen’s University, and the Office of Professional Development and Educational Scholarship at Queen’s University, for their support with converting the VIDA screening tool into an online software program.