
Abstract
This review identifies assessments that can be used by occupational therapy practitioners to measure and monitor their cultural effectiveness.
Culture is an internalized and evolving network of schemas that form a lens for members of a group to perceive, interpret, and interact with reality (Gupta, 2016; Kagawa Singer et al., 2016). The existing literature recognizes culture as a critical factor that can both positively and negatively affect an individual’s health care experience, participation, and outcomes (Anderson et al., 2003; Butler et al., 2016; Flynn et al., 2020; Grandpierre et al., 2018; Jongen et al., 2018; Matteliano & Stone, 2014; McGregor et al., 2019). Because of its powerful influence on clients’ health care trajectory, health care providers must weigh culture as a critical factor and evaluate their cultural effectiveness in the provision of care (Butler et al., 2016; Cooper et al., 2002; Meade et al., 2015; National Institute on Minority Health and Health Disparities, 2017). A myriad of culture-based and related concepts has evolved over time and across academic disciplines (Alizadeh & Chavan, 2016; Butler et al., 2016; Wells et al., 2016). Within the occupational therapy and physical therapy professions, for example, cultural safety (Curtis et al., 2019; Dickson et al., 2022; Tremblay et al., 2023) and cultural humility (American Occupational Therapy Association [AOTA], 2020; Agner, 2020) have gained increasing endorsement, signaling a shift away from the traditionally clinician-centric framework of cultural competency.
Cultural Effectiveness Model
Among such recent frameworks, the cultural effectiveness model (CEM) proposed by Wells et al. (2016) has a distinguished relevance to occupational therapy and physical therapy contexts. Designed for health care professionals to deliver culturally effective care, the CEM addresses how the provider can reflectively apply culture-based knowledge and skills in cross-cultural interactions with clients to enhance the quality of care (Wells et al., 2016). The foundational assumptions of the CEM include the following: (a) Everyone is a multicultural being, and differences exist among and within cultures; (b) becoming culturally effective is a lifelong process; and (c) the provider is viewed as a cultural learner, whereas the client is recognized as a cultural expert (Wells et al., 2016). The model (Wells et al., 2016) consists of four components: self-awareness and exploration (i.e., self-introspection of existing biases, assumptions, and attitudes and how they affect behavior and practice), cultural knowledge (i.e., the process of obtaining an educational base on diverse cultural groups by knowing what, who, and how to ask for information), cultural skills (i.e., use of obtained knowledge of self and others to improve cultural communication, interaction, and intervention), and critical reflection (i.e., continuous description, analysis, synthesis, and evaluation of thoughts, actions, and experiences before, during, and after client engagement). The mutuality-fostering, interactive, and transformational features of the CEM are particularly applicable to occupational therapy and physical therapy professions, in which practitioners often engage with clients in their rehabilitative trajectory long term and across home, school, work, and community contexts.
To minimize confusion arising from the varied and inconsistent assumptions, definitions, and conceptualizations surrounding culture-based constructs, we applied the CEM as the central framework to inform and guide this review. Several factors further justify the selection of the CEM as the grounding framework: (1) it was developed by a team of occupational therapy practitioners and researchers; (2) it integrates both cultural safety—a decolonizing approach that respects and supports the needs, rights, and identities of Indigenous peoples while actively resisting systemic power imbalances and inequities within the health care system (Curtis et al., 2019; Dickson et al., 2022; Tremblay et al., 2023)—and cultural humility, a lifelong learning that emphasizes clinician reflexivity on personal biases and assumptions, respect for clients from diverse backgrounds, and a commitment to addressing power imbalances (AOTA, 2020; Agner, 2020); and (3) it offers a comprehensive and well-operationalized four-domain structure that includes cultural knowledge and cultural skills, components also recognized as important in a widely cited framework, the Process of Cultural Competemility in the Delivery of Healthcare Services (Campinha-Bacote, 2018; Fitzgerald & Campinha-Bacote, 2019).
Culturally Effective Care in Occupational Therapy and Physical Therapy Professions
Culturally effective care involves health care professionals who can “interact with people from different cultures so as to optimize the probability of mutually successful outcomes” (Stone, 2006, p. 338). The provider is effective in interacting with clients from diverse backgrounds and assumes that neither the provider’s nor the client’s culture offers the preferred view (Stone, 2006; Wells et al., 2016). This mutuality prevents health care professionals from assuming a reductionist/static approach, advancing stereotypes and overgeneralizations, and instigating power imbalance, which are the risks more commonly associated with the cultural competency literature (Agner, 2020; Alizadeh & Chavan, 2016; AOTA, 2020; Curtis et al., 2019; Dickson et al., 2022; Grenier, 2020; Lekas et al., 2020; Lie Ken Jie et al., 2022; Mahoney & Kiraly-Alvarez, 2019; Muñoz, 2007; Van Kessel et al., 2022; Vella et al., 2022). Promoting culturally effective care to reduce disparities and enhance equity in health care has been well established as a pressing matter for occupational therapy and physical therapy practitioners (Crawley, 2022; Dickson et al., 2022; Grandpierre et al., 2018; Grenier, 2020; McKivigan, 2020; Ozcan Edeer & Rust, 2022). The profession-wide commitment to and pursuit of cultural effectiveness is further catalyzed by the changing landscape of contemporary health care, with its focus on social justice (Curtis et al., 2019; Hoyt et al., 2025; Taff et al., 2024). To ensure individuals can be provided with fair and just opportunities to achieve their highest level of health, occupational therapy and physical therapy practitioners must be attuned to clients’ cultural contexts and their impact on accessing, navigating, and acquiring equitable health care.
The Accreditation Council for Occupational Therapy Education (ACOTE®) and Commission on Accreditation in Physical Therapy Education (CAPTE) require occupational therapy and physical therapy programs to meet specific standards related to cultural humility, diversity, equity, inclusion, and justice, ensuring cultural effectiveness of occupational therapy and physical therapy practitioners, respectively (ACOTE, 2023; CAPTE, 2023). Occupational therapy and physical therapy practitioners recognize how cultural values and beliefs powerfully affect clients’ perceptions of illness; decision-making in when, how, and with whom to access health care services; engagement and adherence to treatment; and outcomes (Butler et al., 2016; Kagawa Singer et al., 2016; Meade et al., 2015). Despite the importance of providing culturally effective care and the progressive shift toward cultural safety, humility, and responsiveness (Agner, 2020; Dickson et al., 2022; Grandpierre et al., 2018; Lauwers et al., 2024; Muñoz, 2007; Wells et al., 2016; Wray & Mortenson, 2011), the cultural competency framework continues to dominate the available knowledge base in occupational therapy and physical therapy professions (Alizadeh & Chavan, 2016; AOTA, 2020; Curtis et al., 2019; Dickson et al., 2022; Lekas et al., 2020; Lie Ken Jie et al., 2022; Vella et al., 2022). The cultural competency literature, however, has been critiqued for its skewness to provider-centric focus, emphasis on static and closed-ended mastery of culture, potential for othering nondominant cultures, and weak linkage to social justice (Agner, 2020; Alizadeh & Chavan, 2016; AOTA, 2020; Campinha-Bacote, 2018; Curtis et al., 2019; Dickson et al., 2022; Lekas et al., 2020; Lie Ken Jie et al., 2022; Van Kessel et al., 2022; Vella et al., 2022). Moreover, the existing cultural competency research is overwhelmingly focused on enhancing culture-based attitude, knowledge, and skills/behaviors of health care providers within educational contexts (Butler et al., 2016; Horvat et al., 2014; Jager et al., 2021). These observations are concerning, because the prevailing cultural competency education and training that target health care providers have not been clearly and directly linked to improved client experiences and outcomes (Chae et al., 2020; Lie et al., 2010; Renzaho et al., 2013; Vella et al., 2022). Despite noteworthy advancements in the cultural competency literature, it remains elusive how the critical elements of culturally effective care, including the clinician’s ability to organically interact with clients from diverse cultures and foster mutuality, are defined, operationalized, and integrated into occupational therapy and physical therapy contexts.
Instruments Assessing Cultural Effectiveness of Occupational Therapy and Physical Therapy Practitioners
Despite the shortcomings, based on the availability and continued endorsement in the existing literature, examining the instruments that measure cultural competence of health professionals is necessary. The operationalization and measurement of cultural competency vary considerably because of its multifaceted nature and ongoing conceptual evolution (Huish et al., 2023; Jager et al., 2021; Lin et al., 2017). Nevertheless, several systematic reviews were completed to synthesize the available instruments that assess cultural competence in health care contexts. Alizadeh and Chavan (2016) identified 13 outcome measures on cultural competence that can yield empirical data on client outcomes. They found that most of the included measures addressed the dimensions of cultural awareness, cultural knowledge, and cultural skills/behaviors. Seven of these measures were self-ratings provided by health care professionals, pointing to the need for more patient-oriented instruments to measure patient outcomes. Lin et al. (2017) identified 10 instruments in their systematic review of assessments that measure cultural competence of health care providers. They found that most of these instruments assessed cultural attitudes; specifically, 7 instruments measured cultural awareness and 6 instruments measured cultural sensitivity. In congruence with Alizadeh and Chavan (2016), all the included instruments were self-assessments used by health care professionals. To address the dominance of self-assessments, Jager et al. (2021) completed a systematic review of observation-based cultural competence assessments targeting health care providers. Although the five observational instruments included in their review addressed cultural attitudes, cultural knowledge and skills aspects were mostly unaddressed. Across these systematic reviews, the researchers found that the available literature on measuring cultural competence is significantly limited because of the high variability in the definition, operationalization, and combination of components included; the absence of grounding theoretical frameworks; and poor methodological quality and scientific rigor (Alizadeh & Chavan, 2016; Jager et al., 2021; Lin et al., 2017).
When we focused on the occupational therapy and physical therapy literature, we found a dearth of recent research on measuring the cultural competence of occupational therapy and physical therapy students and practitioners. It is plausible that the aforementioned limitations may have similarly impeded the cultural effectiveness research in occupational therapy and physical therapy contexts. To advance the science of cultural effectiveness a step forward, we aimed to review and characterize studies and instruments that addressed cultural effectiveness within contemporary occupational therapy and physical therapy education and practice. Specifically, we explored the theoretical foundation, assessment type, target audience, key cultural domains, and response format of the instruments systematically identified. We were particularly interested in capturing a battery of assessments that were used in the most recent decade to evaluate evidence of the professions’ movement toward more recently emerged concepts and frameworks in culturally effective care.
Method
Study Design
We conducted a scoping review to identify and examine the instruments that measure cultural competency and cultural effectiveness in the recent occupational therapy and physical therapy literature. A scoping review allows researchers to rigorously review, establish the extent of, and identify gaps in the available knowledge, more commonly on topics that have not been comprehensively studied (Daudt et al., 2013; Levac et al., 2010). We followed the five-stage scoping review framework proposed by Arksey and O’Malley (2005): (1) identifying the research question; (2) identifying relevant studies; (3) selecting relevant studies for review; (4) charting the data; and (5) collating, summarizing, and reporting the results. In addition, we partnered with a community stakeholder, consulted with a librarian certified in systematic and meta-analysis reviews, and incorporated Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA–ScR) recommendations to further enhance methodology (Daudt et al., 2013; Levac et al., 2010; Tricco et al., 2018).
Identifying the Research Question
The interdisciplinary research team comprised experts in occupational therapy, physical therapy, and health services research (n = 3); occupational therapy and physical therapy graduate assistants (n = 3); and a community stakeholder (n = 1) whose child received occupational therapy and physical therapy services at the time of the study. Collaboratively, the team developed the following research question: What are the characteristics of instruments used to assess cultural effectiveness of occupational therapy and physical therapy professionals in the recent literature?
We used the term cultural effectiveness in the research question to align this review with the profession’s evolving emphasis on contemporary concepts and frameworks that have advanced beyond cultural competency. However, given the more widespread use of cultural competency in the existing literature and recognizing that some studies do not clearly distinguish between cultural effectiveness and related constructs, we included cultural competency, cultural humility, and other synonymous terms in the search strategy to enhance the comprehensiveness of the review (see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot).
Identifying Relevant Studies
We developed a search strategy with key terms associated with cultural competency and cultural effectiveness specific to occupational therapy and physical therapy contexts. Based on consultation with a librarian who is certified in systematic and meta-analysis reviews (Bergjord), the search strategy was refined to cast a wide-net search across four databases: Academic Search Premier, CINAHL, MEDLINE, and PsycINFO. A sample combination of key terms used with MEDLINE is presented in Table A.1. To identify relevant studies that satisfy the scope of this review, we established a set of inclusion and exclusion criteria. The articles were included for screening and full-text reviews if they (a) were published in English in the United States between January 2010 and June 2022; (b) were peer-reviewed; and (c) measured aspects related to cultural competency and effectiveness of occupational therapy and physical therapy students, educators/researchers, managers, providers, and other relevant individuals. In addition to straightforward psychometric studies, articles were included if the outcome measure assessed cultural constructs of the sample. Articles were excluded if they were based on personal and professional opinion or a nonsystematic review of available evidence. To further increase comprehensiveness, we completed a hand search of all included articles as well as key review articles identified from relevant textbooks and web searches.
Selecting Relevant Studies for Review
Once the initial searches were completed across the databases, the returned articles were pooled and duplicates were removed. Then, two independent reviewers screened the returned articles by using a predefined checklist containing inclusion and exclusion criteria. Another team of three independent reviewers then provided a full-text review of the screened articles. The team engaged in regular discussions to resolve differences in judgment and disagreements until they reached consensus. The PRISMA flow diagram of returned and included articles is provided in Figure 1.
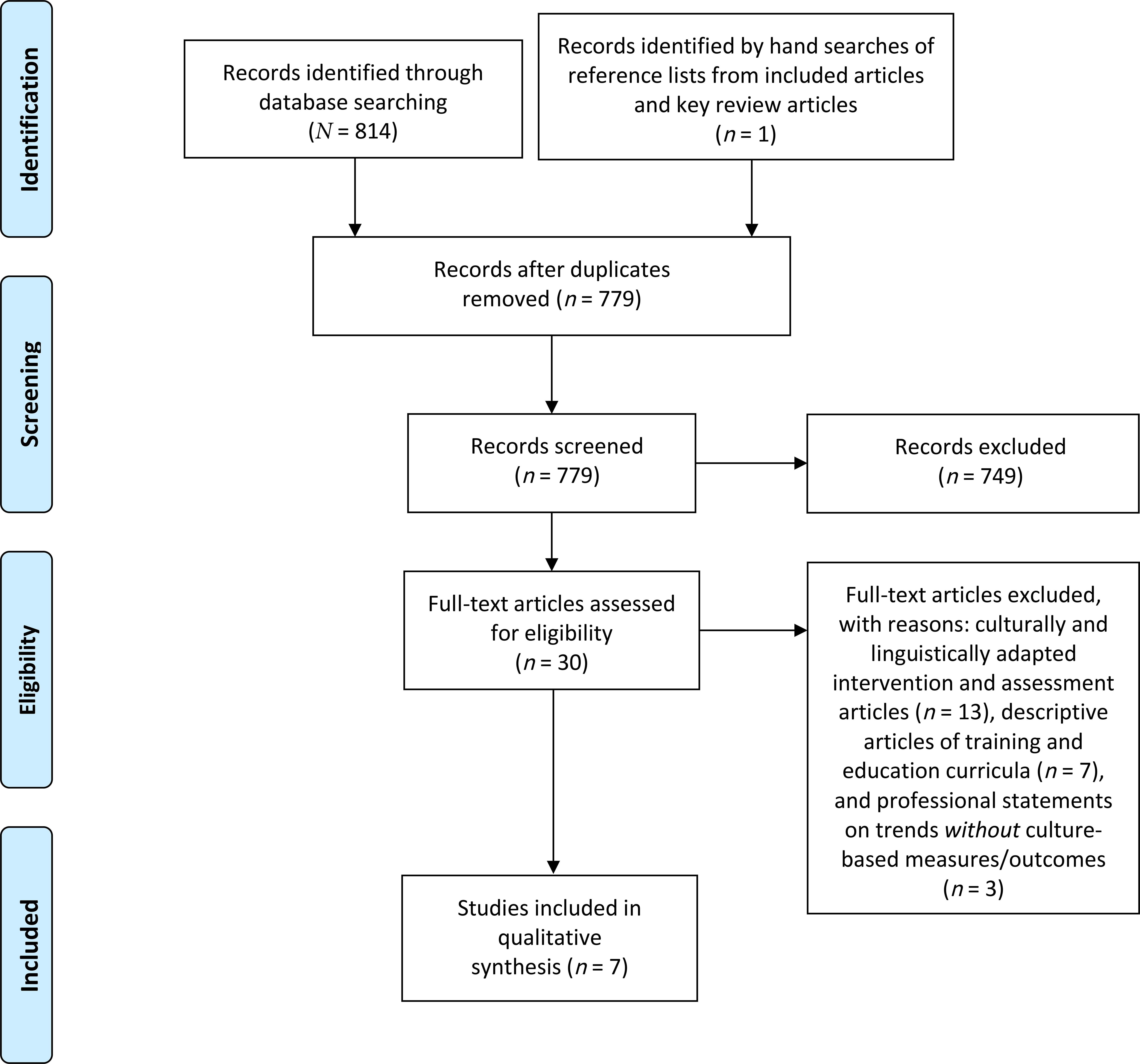
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow of study selection process.
Charting the Data
We compiled and extracted the final list of included articles for summary and comparative analysis. Specifically, the included articles were indexed and summarized across the domains of purpose/aim, study design, participants, instrument, and psychometric properties as reported within the article (see Table A.2 in the Supplemental Material). Then, copies of the identified instruments were collected via further literature search, communication with the corresponding authors, and purchase following the copyright policies. If the article used an adapted version of the instrument, the original version of the instrument was searched for and retrieved as appropriate. The instruments were summarized across the domains of theoretical foundation, type of assessment, target audience, key domains and number of items, and response format (see Table A.3), with additional literature search as needed. Finally, we pooled and sorted the items across the identified instruments into the CEM domains of Self-Awareness and Exploration, Cultural Knowledge, Cultural Skills, and Critical Reflection. Any items that could not be sorted into the four domains were placed in the “other” category. Within each domain, example items that aligned to the operational definition of the CEM were selected and organized into a table (see Table A.4).
Collating, Summarizing, and Reporting the Results
We reviewed and synthesized the summaries of the included articles and instruments. The emerged key patterns were summarized, reported, and agreed upon iteratively until we reached a consensus. The finalized results revealed the characteristics of recently published studies and instruments on cultural competency specific to occupational therapy and physical therapy contexts.
Results
Of 815 returned articles, 7 articles were included in this review (see Table A.2). Four were methodological studies (Fike et al., 2016; Palombaro & Lattanzi, 2012; Schwarz et al., 2015; Suarez-Balcazar et al., 2011), 2 were descriptive cross-sectional studies (Doherty et al., 2017; Oluwole-Sangoseni & Jenkins-Unterberg, 2018), and 1 was a single-group quasi-experimental study (Chappell & Provident, 2020). Four out of 7 studies were completed with Doctor of Physical Therapy (DPT) students in university settings (Doherty et al., 2017; Fike et al., 2016; Oluwole-Sangoseni & Jenkins-Unterberg, 2018; Palombaro & Lattanzi, 2012). Two studies involved occupational therapy practitioners in clinical practice (Chappell & Provident, 2020; Suarez-Balcazar et al., 2011). One study involved 242 health care professionals, including speech-language pathologists and other therapists at a large midwestern children’s hospital in the United States (Schwarz et al., 2015). Across the articles, six instruments were identified as outcome measures used to collect the study data (see Table A.3). One instrument, the Inventory for Assessing the Process of Cultural Competence Among Healthcare Professionals–Student Version (IAPCC–SV®), was used in 2 of the 7 articles (Fike et al., 2016; Palombaro & Lattanzi, 2012). The articles reported a varying degree of psychometric properties of the instruments used in their studies, from none to citing internal consistency, test–retest reliability, construct validity, and minimal detectable change identified from the existing literature. The 4 methodological studies (Fike et al., 2016; Palombaro & Lattanzi, 2012; Schwarz et al., 2015; Suarez-Balcazar et al., 2011) further established psychometric properties of their targeted instruments.
The six instruments revealed from this review (see Table A.3) were the Clinical Cultural Competency Questionnaire (CCCQ; Chappell & Provident, 2020), Cultural Competence Assessment Instrument from the University of Illinois at Chicago (CCAI–UIC; Suarez-Balcazar et al., 2011), Healthcare Provider Cultural Competence Instrument (HPCCI; Schwarz et al., 2015), IAPCC–SV (Fike et al., 2016; Palombaro & Lattanzi, 2012), Multicultural Sensitivity Scale (MSS; Oluwole-Sangoseni & Jenkins-Unterberg, 2018), and Self-Assessment of Cultural Competence (SACC; Doherty et al., 2017). The IAPCC–SV was the only instrument that required purchasing prior to review and user agreement submitted via mail. With an additional literature search, we confirmed that four instruments (CCAI–UIC, HPCCI, IAPCC–SV, and MSS) were explicitly founded on theoretical frameworks when conceptualizing and developing the instrument. In the process of instrumentation, the CCAI–UIC and SACC pooled items from existing assessments that measure culture-based constructs. From the battery of 13 assessments named, only the Cultural Self-Efficacy Scale by Coffman et al. (2004) informed both the CCAI–UIC and SACC.
All the instruments were self-assessments that can be used to measure cultural aspects of health care professions’ students and professionals. The instruments assessed varied combinations of cultural domains with differing conceptualizations and definitions. The three most common cultural domains were Attitude (n = 4), Knowledge (n = 4), and Skills (n = 4). The Encounter domain was addressed in the CCCQ and IAPCC–SV out of the six instruments. Additional domains reflected across the instruments were desire, practice orientation, self-assessment, patient-centered communication, organizational support, and education and training. Congruently, the response format significantly varied across the instruments, with the Likert scale ranging from strongly disagree to strongly agree used in four instruments (CCAI–UIC, HPCCI, IAPCC–SV, and MSS). Finally, a total of 249 items were pooled and sorted across the CEM domains of Self-Awareness and Exploration, Cultural Knowledge, Cultural Skills, Critical Reflection, and “other.” With the exception of items sorted under “other,” three items from each category that align to the definition of the CEM domain and exemplify the possible operationalization and measurement of the construct were selected (see Table A.4). For the CEM domain of Critical Reflection, only one item—from the HPCCI—was identified to address the aspect of continuous self-evaluation before, during, and after client engagement.
Discussion
The included instruments that measure culture-based care aspects of occupational therapy and physical therapy students and practitioners varied widely in theoretical foundation, conceptualization, and operationalization, which were previously reported (Crawley, 2022; Gozu et al., 2007; Jongen et al., 2018; Lin et al., 2017). This variability can potentially limit how cultural effectiveness is examined in occupational therapy and physical therapy contexts. For example, to address the aspect of provider engagement with clients across diverse communities, the HPCCI included an item, “I enjoy working with people who are culturally different from me,” under the Awareness and Sensitivity domain. In contrast, the SACC used a statement, “I am more comfortable with patients from backgrounds similar to my own,” as part of the Attitude domain. In addition, this provider trait is operationalized and measured as a degree of enjoyment for HPCCI and a level of comfort for SACC. In other words, enhanced cultural effectiveness in one study using HPCCI may not translate to another study that targeted the same outcome but used other instruments. Although the complexity is recognized, the observed threats to measurement validity can prohibit replication of findings, synthesis of evidence, and advancement of the knowledge base in the cultural effectiveness literature. It also introduces methodological challenges to establishing standardized benchmarks across health care professions for objective goal setting, tracking progress, and quality improvement with a possible ceiling effect (Garin, 2014).
To mitigate these issues, educators, clinicians, and researchers are recommended to strive toward minimizing ambiguity when designing their cultural effectiveness interventions and studies, selecting outcome measures, and reporting the results. Specifically, the target cultural characteristics should be clearly defined within the parameters of the study—regardless of the term’s popularity or widespread use—without assuming consistent interpretation in the scientific communities. Furthermore, the cultural constructs should be anchored to a sound theoretical framework and measured by using instruments with established psychometric properties. When synthesizing and evaluating evidence on cultural effectiveness, on the other hand, researchers must pay careful attention and consideration to how the key cultural variables are defined, operationalized, and measured across studies. The database of cultural assessment tools compiled by the Transcultural C.A.R.E. Associates (n.d.) may be a valuable resource for rehabilitation educators and researchers.
Despite the previous researchers’ warnings about social desirability bias (Alizadeh & Chavan, 2016; Jager et al., 2021; Lin et al., 2017), all instruments included in this review were self-assessments. To be socially favorable, especially in educational and clinical contexts, occupational therapy and physical therapy students and clinicians may overreport more culturally effective attitudes and behaviors than they actually exhibit on items, such as “It is not easy to treat all people the same way” in the SACC and “I do not enjoy associating with persons of other ethnic groups” in the MSS. The discrepancy between self-reported and actual demonstration of cultural effectiveness can mask important areas for improvement and lead to overly optimistic conclusions about providers’ cultural effectiveness. It is plausible that this gap may have contributed to the weak linkage between cultural competency education and training and direct client experiences and outcomes (Chae et al., 2020; Lie et al., 2010; Renzaho et al., 2013; Vella et al., 2022). In addition to observation-based assessments (Jager et al., 2021), more assessments that capture client perceptions and experiences of providers’ cultural effectiveness are needed. As cultural experts, according to the CEM (Wells et al., 2016), clients can provide valuable and objective input on what attributes and behaviors of rehabilitation providers can improve for their care experiences and outcomes (Alizadeh & Chavan, 2016; Black et al., 2016). The availability of client-administered assessments can produce objective data that can be triangulated with clinician-reported assessments and outcomes.
This scoping review sought to document evidence of the professions’ movement toward more recently emerged concepts and frameworks in culturally effective care by evaluating the instruments used in the most recent literature. Although no instruments captured all the domains within the CEM (Wells et al., 2016), multiple items aligned to the domains of Self-Awareness and Exploration, Cultural Knowledge, and Cultural Skills (see Table A.4). However, only one item was aligned to the domain of Critical Reflection across all the instruments. The theoretical frameworks of the CEM (Wells et al., 2016) and the Process of Cultural Competemility in the Delivery of Healthcare Services (Campinha-Bacote, 2018; Fitzgerald & Campinha-Bacote, 2019) emphasize that instead of reaching competency or mastery, a provider must engage in a continuous, lifelong process of becoming culturally effective. As a key mechanism with immediate impact on client engagement and outcomes, self-reflection plays a critical role in this transformative process (Campinha-Bacote, 2018; Fitzgerald & Campinha-Bacote, 2019; Wells et al., 2016). The literature reviews completed by McLeod et al. (2015), Robinson et al. (2022), and Ziebart and MacDermid (2019) revealed self-assessment and self-directed learning, peer-supported learning, and writing including journaling and narrative essays as common strategies to foster self-reflection among health professionals based on Schön’s (1983) “reflection-on-practice and reflection-in-practice” framework. The professions of occupational therapy and physical therapy are encouraged to focus their education, training, and research on enhancing students’ and providers’ ability to continuously self-evaluate thoughts, actions, and experiences when engaging with clients from diverse cultural backgrounds and examine the impact on clinical practice and client outcomes. Amid the abundance of self-assessments measuring perceived mastery of cultural effectiveness, there remains a need for more instruments that assess the clinician capacity for reflexivity—an essential component to ascertain the implementation of culturally safe, humble, and effective practices in occupational therapy and physical therapy.
Limitations
Limitations of this review include a specific focus on the recent literature published between 2010 and 2022, which was intended to capture the latest trends and to circumvent duplication of previous work in the cultural competency literature. The articles were also required to be published in English in the United States, which could have excluded relevant work completed in international occupational therapy and physical therapy contexts. In addition, further evidence could have been gathered from gray literature sources, including dissertations, theses, and white papers.
Implications for Occupational Therapy Practice
The overarching aim of this review was to explore the characteristics of instruments used to assess cultural effectiveness of occupational therapy and physical therapy professionals in recent literature. The results revealed the following implications and opportunities for occupational therapy practice: ▪ Based on the theoretical frameworks of the CEM (Wells et al., 2016) and the Process of Cultural Competemility in the Delivery of Healthcare Services (Campinha-Bacote, 2018; Fitzgerald & Campinha-Bacote, 2019), occupational therapy practitioners recognize that instead of reaching competency or mastery, they must strive towards becoming culturally effective from their daily encounters with clients across diverse communities. ▪ Occupational therapy practitioners can consider completing self-assessments on cultural effectiveness as identified from this scoping review and engage in regular self-reflection of their culture-based beliefs and attitude, knowledge, and skills/behaviors. They are cautioned, however, about the risk of social desirability bias and potential overestimation of their cultural effectiveness. ▪ Occupational therapy practitioners, managers, and educators can consider implementing objective measures such as observation-based or client-administered assessments and client feedback to enhance objectivity in monitoring the quality of culturally effective care provided in clinical practice and fieldwork.
Conclusion
This scoping review characterized seven articles and six instruments that addressed cultural effectiveness in the recent occupational therapy and physical therapy literature. The identified assessments, all of which were self-administered, varied in theoretical framework, conceptualization, and operationalization in measuring cultural effectiveness. The observed ambiguity and inconsistencies may limit the advancement and translation of knowledge in the literature on cultural effectiveness. There is a critical need for additional assessments that can capture client perceptions and experiences of a provider’s cultural effectiveness. The availability of client-administered instruments can contribute to more objective and comprehensive evaluation by providing data that can be triangulated with self-reported and observation-based assessments. Additional work is recommended to explore how self-reflection training and tools can catalyze the lifelong process of becoming culturally effective.
Supplemental Material
Supplementary material for Measuring Cultural Effectiveness in Occupational Therapy and Physical Therapy: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051186.pdf for Measuring Cultural Effectiveness in Occupational Therapy and Physical Therapy: A Scoping Review by Julia Shin, Sarbinaz Bekmuratova, Jamie Nesbit, Inhyun Han, Allison Tung, Jordan Ortiz, Tyler Wright, Sarah Chamoun and Judith Bergjord in The American Journal of Occupational Therapy
Footnotes
*Indicates articles included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.