
Abstract
The findings of this review reinforce the role of occupational therapists in supporting mental health and inform future practice and education.
Pregnancy is a life-altering period in a woman’s life, characterized by significant physical, mental, emotional, and psychological changes (Bjelica et al., 2018). For as many as 1 in 5 women, this journey is further complicated by the pregnancy being designated as high risk (Johnson et al., 2024). High-risk pregnancies necessitate specialized monitoring and care because of factors such as preexisting medical conditions, pregnancy-related complications, or advanced maternal age (Curbelo, 2021; Holness, 2018). Conditions that commonly result in classifying a pregnancy as high risk include gestational diabetes mellitus, hypertensive disorders of pregnancy, chronic infections such as HIV or hepatitis, recurrent pregnancy loss, and premature rupture of membranes, as well as other conditions (Barinov et al., 2022).
A diagnosis of high-risk pregnancy often triggers significant emotional turmoil, manifesting as fear, anxiety, or uncertainty (Isaacs & Andipatin, 2020; Williamson et al., 2023). This psychological burden is exacerbated by hospitalizations, lifestyle adjustments, and the demands of increased medical monitoring and prenatal appointments (Mirzakhani et al., 2020; Rodrigues et al., 2016). Additionally, high-risk pregnancy is associated with disruptions in performance of personal and familial roles, ambivalent feelings about the pregnancy, reduced self-efficacy, and psychological distress (Isaacs & Andipatin, 2020; Oliveira & Mandú, 2015). Studies have highlighted the negative effects of a high-risk pregnancy on women’s coping mechanisms and overall well-being, linking these experiences to adverse mental health outcomes, including depression and stress (Gourounti et al., 2015; Holness & Barfield, 2023).
Occupational therapists play a pivotal role in addressing the multifaceted needs of women during the perinatal period. According to the Occupational Therapy Practice Framework (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020), occupational therapy practitioners facilitate participation in meaningful occupations by addressing the interplay of client factors, performance patterns, and environmental contexts. Occupational therapy practitioners aim to support mothers in adapting to new routines in activities of daily living and instrumental activities of daily living, managing increased responsibilities, and maintaining personal health (AOTA, 2020; Royal College of Occupational Therapists, 2025). They promote overall well-being and strong mother–infant attachment by enabling occupational participation (Baker et al., 2024; Slootjes et al., 2016).
Occupational therapy practitioners use a holistic approach by considering the social, physical, mental, and emotional factors associated with matrescence to provide person-centered care that improves maternal health (Fernandes, 2018; Payne, 2019; Pollari et al., 2022; Slootjes et al., 2016). Interventions include role adaptation training, psychosocial support, ergonomic adjustments, psychoeducation, and stress management strategies, addressing aspects of the mother and her environment (Barbic et al., 2021). This promotes occupational adaptation and engagement (Baker et al., 2024). Studies demonstrate that occupational therapy interventions, such as aquatic exercise (Sechrist et al., 2015) and group therapy sessions (Sponseller et al., 2021), can improve physiological outcomes and enhance psychological well-being among mothers. By adopting a holistic and client-centered approach that focuses on physical, emotional, and psychosocial well-being, occupational therapy practitioners assist women to navigate the complex transitions of pregnancy and motherhood (Fernandes, 2018; Payne, 2019; Pollari et al., 2022).
Psychosocial interventions are central to occupational therapy practice, particularly in managing anxiety, depression, and stress (Kirsh et al., 2019). They are defined as “nonpharmacological interventions having a psychological or social aim, which can improve symptoms, global functioning, quality of life, and social inclusion” (Barbui et al., 2020, p. 6). AOTA (2016) emphasizes the role of occupational therapy practitioners in “addressing the psychological and social aspects of human performance” (p. 1), highlighting that “addressing psychological and social factors of mental health through interventions designed to enhance or restore well-being, occupational balance, and occupational engagement is a critical component of the therapeutic process” (p. 4). Evidence-based psychosocial interventions, such as cognitive–behavioral therapy (CBT), mindfulness-based cognitive therapy, acceptance and commitment therapy, stress management training, and psychoeducation, have demonstrated efficacy in enhancing coping mechanisms and promoting occupational engagement for populations facing chronic illness, posttraumatic stress disorder, and depression (Barber et al., 2021; Fox et al., 2019; Hunter et al., 2017; Wheeler et al., 2016).
In the perinatal context, occupational therapists have implemented a range of interventions to enhance well-being and mental health. These include ergonomic programs to manage the physical demands of pregnancy and support maternal health and stress management techniques to promote resilience and reduce stress (Berglund & Peterman, 2021; Bochenek et al., 2017). Occupation-based interventions have also addressed issues such as pregnancy loss, postpartum depression, and reduced occupational performance while encouraging social participation and well-being (Barbic et al., 2021; Hanish et al., 2019; Merkel et al., 2023; Slootjes, 2022).
Despite the growing recognition of occupational therapy’s role in women’s health, research on psychosocial interventions for women with high-risk pregnancies remains limited. This population faces unique physical, emotional, and psychological challenges that can significantly affect maternal well-being, fetal outcomes, and postpartum recovery. Effective psychosocial support during a high-risk pregnancy has the potential to reduce stress, improve coping strategies, and enhance mother–infant bonding, yet its efficacy remains underexplored. Although practitioners report anecdotal success, the absence of a systematic review limits the ability to translate these interventions into standardized, evidence-based practice. By critically evaluating the existing research, this review aims to bridge this gap, guiding clinicians toward interventions that promote better health outcomes and ensure comprehensive, equitable care.
This systematic literature review evaluates the effectiveness of psychosocial interventions in occupational therapy practice for managing anxiety, depression, and stress among women with high-risk pregnancies. By synthesizing existing evidence, we aim to provide insights into how these interventions can enhance maternal mental health and quality of life (QoL), ultimately guiding occupational therapy practice with this vulnerable population.
The research question guiding this review was “What is the evidence for the effectiveness of psychosocial interventions within the scope of occupational therapy practice to improve mental health and QoL among women with high-risk pregnancies?”
Method
This systematic review was conducted in accordance with the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Version 6.5; Higgins et al., 2024), and the reporting adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). The review protocol was registered in the PROSPERO database under ID CRD42025633376.
A systematic search was performed across eight databases: MEDLINE via PubMed, Embase via Ovid, Cochrane Library, AMED, SocIndex, OTseeker, PsycINFO, and CINAHL. These databases were selected for their relevance to the research question. The search strategies were developed in collaboration with a medical librarian, informed by a review of the existing literature. The CINAHL search strategy is presented in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot). The review team included an assistant professor (Sabina Khan) and a clinical lecturer in occupational therapy (Thuy Tran) who provided subject expertise, an experienced systematic review researcher (Christianah Edema) who ensured methodological rigor, and three master’s-level occupational therapy students (Jessica Grant, Laritza Olivares, and Viviana Ferreira) who assisted with title and abstract screening.
Inclusion and Exclusion Criteria
This review included primary research published in peer-reviewed journals between January 2000 and December 2024.
Population
The population of interest was women with high-risk pregnancies. Studies addressing a broad population classified as high risk or those specifying conditions such as gestational diabetes, hypertensive disorders of pregnancy, preterm labor, premature rupture of membranes, recurrent miscarriage, or chronic infections were included.
Intervention
Psychosocial interventions were defined as those using psychological, behavioral, or social approaches aimed at improving mental and emotional well-being. To ensure relevance to occupational therapy practice, eligible interventions were carefully selected on the basis of their alignment with the OTPF–4 (AOTA, 2020). Interventions that directly involved activities of daily living or occupation-based strategies or that were aimed at enhancing participation in meaningful life roles were prioritized. Although interventions administered by occupational therapists were preferred, those conducted by other allied health professionals were also eligible if they adhered to principles and methods that align with occupational therapy practice. Interventions that fell outside the scope of occupational therapy—such as those focused solely on medical or pharmacological approaches—were excluded to maintain focus on the profession’s unique contributions.
Outcomes
Eligible studies reported outcomes related to anxiety, depression, stress, or QoL. Studies focusing solely on nonpsychosocial outcomes, such as birth outcomes or changes in blood pressure or glucose levels, were excluded.
Study Types
The review included publications with Level 1b, 2b, or 3b evidence, as defined by the Oxford Centre for Evidence-Based Medicine (Burns et al., 2011; see Table A.2 in the Supplemental Material). Conference proceedings, theses, and dissertations were excluded. No language restrictions were applied to minimize bias. Citation chasing of relevant systematic reviews was conducted to identify additional primary research.
Study Selection
Search results from the databases and gray literature were deduplicated using EndNote (Version 19). Title and abstract screening were conducted in duplicate by four authors (Edema, Grant, Olivares, and Ferreira) using predefined inclusion and exclusion criteria. Screening was conducted manually in Microsoft Excel, and discrepancies were resolved through discussion. For disagreements that could not be resolved, input from a third reviewer was sought. Studies meeting inclusion criteria on the basis of abstract screening underwent a full-text review, which was also conducted independently by two authors (Khan and Edema). Any disagreements during the full-text review were resolved through discussion.
Data Extraction
After the full-text review, data extraction was performed for studies that met the inclusion criteria. Extracted data included baseline characteristics of the population (e.g., age, pregnancy stage), study design, interventions, comparators, outcomes, and results. One author (Edema) completed the initial extraction using a piloted template in Microsoft Excel, and a second author (Tran) independently reviewed the extracted data for accuracy. Discrepancies were discussed and resolved collaboratively.
Risk-of-Bias Assessment
Two authors (Khan and Edema) independently assessed the risk of bias for each included study. Randomized and nonrandomized trials were evaluated using the Cochrane Collaboration’s Risk-of-Bias Tool 2 (Higgins et al., 2011). Pretest–posttest studies were assessed using the Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group, developed by the National Heart, Lung, and Blood Institute (2014).
Data Synthesis
We used a narrative thematic synthesis to analyze and interpret the findings of the included studies (Snilstveit et al., 2012). Results were first organized by reported outcomes: anxiety, depression, stress, and QoL. Within each outcome category, interventions were further classified by their primary modality: cognitive-based, emotion-based, sensory-based, or integrated approaches. The strength of evidence for each category was determined on the basis of the U.S. Preventive Services Task Force (2018) ratings: Strong evidence: consistent results from two or more well-conducted Level 1 studies. Moderate evidence: findings from one or more well-conducted randomized controlled trials or multiple moderate-quality studies (Level 2 or 3), with some limitations, such as small sample size or inconsistent results. Low evidence: findings from a small number of low-quality studies or studies with major design flaws or inconsistent outcomes.
Results
Thirty-four articles were deemed eligible for inclusion in this study. The flow of literature is illustrated in Figure 1.
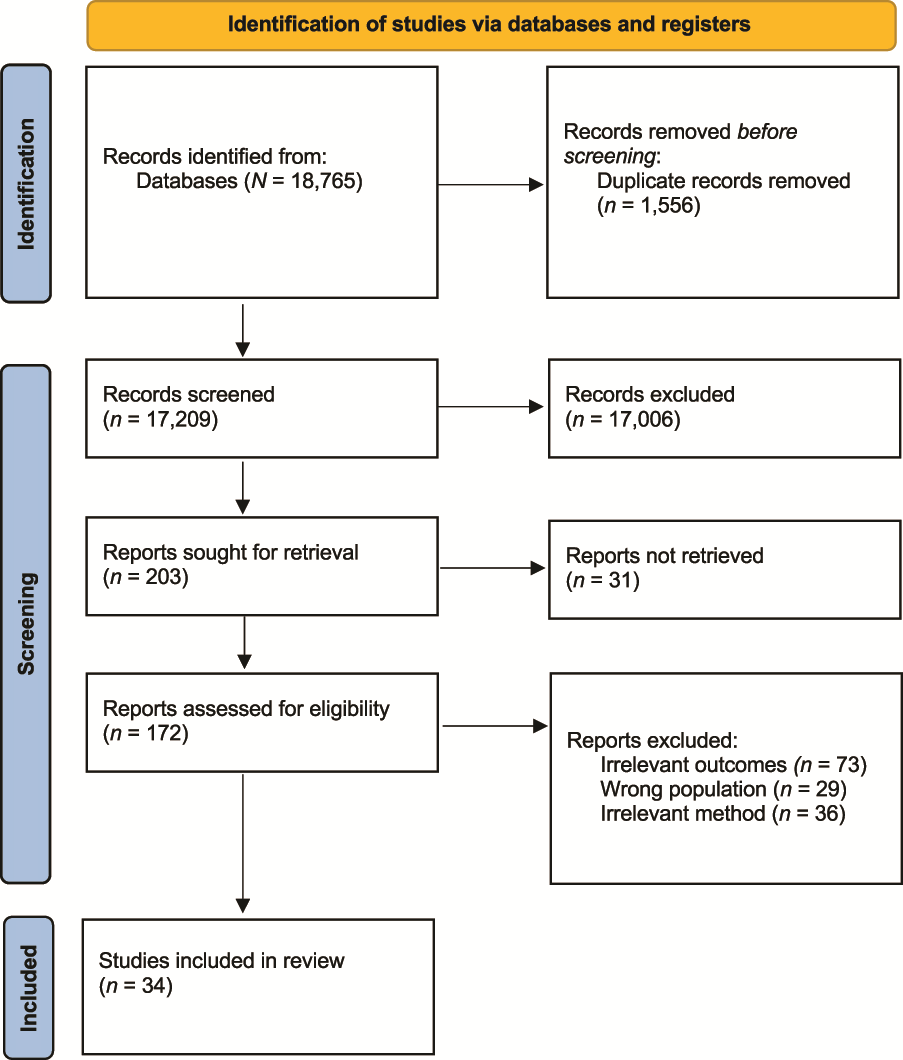
Flow of literature through the systematic review. Note. Format from Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71.
The majority of the included studies were conducted in Iran (n = 16; 47%), followed by Turkey (n = 5; 15%). More than half of the studies (n = 18; 53%) were carried out in outpatient settings. This review captured various conditions associated with high-risk pregnancies, including hypertensive disorders of pregnancy (n = 9; 26%), gestational diabetes (n = 6; 18%), adolescent pregnancy (n = 4; 12%), recurrent miscarriage (n = 2; 6%), and preterm labor (n = 4; 12%), and a cohort of women with multiple forms of high-risk pregnancies (n = 9; 26%).
We report this study’s findings by outcome: anxiety, depression, stress, QoL, and other occupational therapy–related outcomes. We further categorize the findings regarding each outcome by the type of intervention: cognitive-based, counseling-based, emotion-based, sensory-based, and integrated approaches. A summary of the findings for each outcome by intervention group is presented in Figure 2.
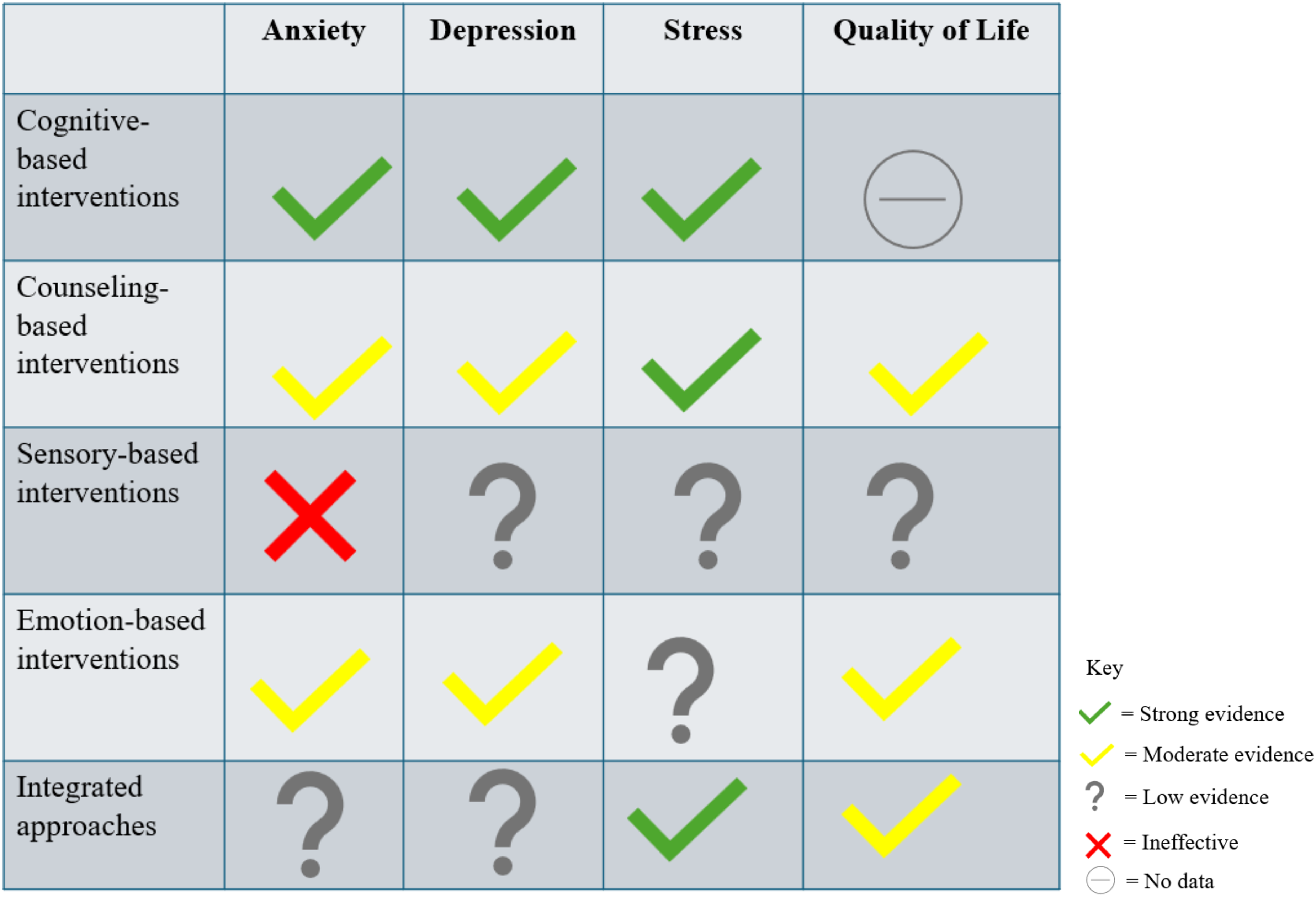
Summary of the strength of evidence for the effectiveness of psychosocial interventions in high-risk pregnancies. Note. No study assessed the effectiveness of cognitive-based interventions on quality of life.
Anxiety
Twenty-two studies evaluated the effectiveness of psychosocial occupational therapy interventions on anxiety among women with high-risk pregnancies. The most commonly used tools for assessing anxiety were the State–Trait Anxiety Inventory (n = 10; 45%) and the Pregnancy-Related Anxiety Questionnaire (n = 6; 27%).
Cognitive-Based Interventions
Seven studies—three Level 1b (Mirtabar et al., 2020; Urech et al., 2017; Zhihui & Zhang, 2020) and four Level 2b (Asghari et al., 2016; Hassan et al., 2020; Madigan et al., 2015; Scherer et al., 2016)—investigated the impact of cognitive-based interventions on anxiety among women with high-risk pregnancies.
Four studies (two Level 1b and two Level 2b) compared cognitive–behavioral interventions with routine care alone (Asghari et al., 2016; Hassan et al., 2020; Mirtabar et al., 2020; Zhihui & Zhang, 2020). These studies demonstrated a significant reduction in anxiety scores among participants who received the intervention compared with the control groups.
Two additional studies (one Level 1b and one Level 2b) evaluated internet-based cognitive–behavioral stress management against control groups engaged in distraction activities, such as writing stories, solving puzzles, and completing quizzes (Scherer et al., 2016; Urech et al., 2017). Although no significant differences were found between the experimental and control groups, both groups exhibited significant improvements in mean anxiety scores compared with their baseline levels.
The seventh study focused on trauma-focused CBT for pregnant adolescents who had experienced trauma. It found no significant difference in anxiety scores between the intervention and control groups (Madigan et al., 2015).
Despite some variability in individual study findings, the consistent results from multiple well-designed studies, including four Level 1b randomized controlled trials, provide strong evidence supporting the effectiveness of cognitive-based interventions in reducing anxiety symptoms among women with high-risk pregnancies.
Counseling-Based Interventions
Five studies—one Level 1b study (Bazrafshan et al., 2020) and four Level 2b studies (Abazarnejad et al., 2019; Elsharkawy et al., 2021; Khazaei Fadafan et al., 2024; Madigan et al., 2015; Rafie et al., 2023)—examined the effects of counseling-based interventions on anxiety among women with high-risk pregnancies. Various forms of counseling were used, including psychoeducational counseling (Abazarnejad et al., 2019), acceptance and commitment-based counseling (Khazaei Fadafan et al., 2024), solution-focused counseling (Rafie et al., 2023), happiness counseling (Elsharkawy et al., 2021), and educational counseling (Bazrafshan et al., 2020).
In the Level 1b study (Bazrafshan et al., 2020), significant improvements in anxiety scores were observed in the intervention group compared with the control group, with the effects persisting for up to 1 mo postintervention. Similarly, the Level 2b studies demonstrated significant reductions in anxiety scores across the different types of counseling interventions. However, one study (Abazarnejad et al., 2019) reported that although anxiety levels improved postintervention, no significant difference was observed between the treatment and control groups.
Overall, there is moderate evidence supporting counseling-based interventions for managing anxiety among women with high-risk pregnancies. This conclusion is based on one Level 1b study and multiple moderate-quality studies with consistent findings.
Emotion-Based Interventions
Four studies—one Level 1b study (Ibıcı Akca et al., 2023), two Level 2b studies (Gallagher et al., 2020; Wang et al., 2021), and one Level 3b study (Goetz et al., 2020)—evaluated the impact of emotion-based interventions on anxiety among women with high-risk pregnancies. Three of these studies used mindfulness-based interventions, and one (Gallagher et al., 2020) used yoga.
In the Level 1b study, postintervention mean anxiety scores were significantly lower in the treatment group compared with the control group (Ibıcı Akca et al., 2023). The results of two additional studies (Gallagher et al., 2020; Goetz et al., 2020) supported these findings. Goetz et al. (2020) reported a significant reduction in anxiety scores from baseline among participants receiving the intervention, and Gallagher et al. (2020) observed significantly lower anxiety levels in the intervention group compared with the control group.
However, Wang et al. (2021) did not report a significant change in anxiety scores from baseline among participants who received the intervention. Notably, in the control group, anxiety levels increased significantly postintervention, but this study did not statistically compare changes in anxiety levels between the groups.
Taken together, there is moderate evidence supporting the use of emotion-based interventions, such as mindfulness and yoga, to reduce anxiety among women with high-risk pregnancies. This conclusion is based on one Level 1b study and corroborative findings from multiple lower-quality studies.
Sensory-Based Interventions
Five studies—three Level 1b studies (Aksoy et al., 2024; Teckenberg-Jansson et al., 2019; Toker & Kömürcü, 2017) and two Level 2b studies (Go & Park, 2017; Yüksekol & Başer, 2020)—investigated the effects of sensory-based interventions on anxiety among women with high-risk pregnancies. Four studies used music therapy, and one study (Go & Park, 2017) used aromatherapy.
Among the Level 1b studies, two (Teckenberg-Jansson et al., 2019; Toker & Kömürcü, 2017) found no significant difference in mean anxiety scores between participants in the intervention and control groups postintervention. However, one Level 1b study (Aksoy et al., 2024) reported a significant reduction in both state and trait anxiety in the intervention group compared with the control group after music therapy.
The two Level 2b studies also reported no significant reductions in anxiety scores. Specifically, Yüksekol and Başer (2020) found no meaningful improvement after music therapy, and Go and Park (2017) observed similar results for aromatherapy.
On the basis of these findings, there is strong evidence to support the ineffectiveness of sensory-based interventions, such as music therapy and aromatherapy, in alleviating anxiety among women with high-risk pregnancies.
Integrated Approaches
Only one Level 2b study, involving 30 participants, evaluated the impact of an integrated approach using mindfulness-based cognitive therapy. The study reported significantly lower mean anxiety scores in the intervention group compared with the control group postintervention (Musavi & Narimani, 2015).
Given the limited evidence from a single study, there is low strength of evidence supporting the use of integrated interventions, such as mindfulness-based cognitive therapy, for managing anxiety among women with high-risk pregnancies.
Depression
Fourteen studies reported on depression, with the most commonly used assessment tools being the Edinburgh Postnatal Depression Scale (n = 4; 29%), the Beck Depression Inventory (n = 4; 29%), and the Depression Anxiety Stress Scales (n = 3; 21%).
Cognitive-Based Interventions
Six studies—two Level 1b studies (Urech et al., 2017; Zhihui & Zhang, 2020) and four Level 2b studies (Asghari et al. 2016; Chaharrahifard et al., 2021; Hassan et al., 2020; Madigan et al., 2015)—evaluated the effects of cognitive-based interventions on depression among women with high-risk pregnancies.
The Level 1b studies demonstrated significant within-group improvements in depression scores from baseline in the intervention groups (Urech et al., 2017; Zhihui & Zhang, 2020). In one study (Zhihui & Zhang, 2020), the improvement in the intervention group was significantly greater than that in the routine-care control group, in which no change in depression scores was observed. However, in the study by Urech et al. (2017), in which the control group received a distraction-based intervention, both the intervention and the control groups showed improvement from baseline, with no significant difference between the two groups postintervention.
Among the Level 2b studies, one reported significant within-group improvements in depression scores from baseline in the intervention group (Chaharrahifard et al., 2021), and two reported significant reductions in mean depression scores in the intervention group compared with the control group (Asghari et al., 2016; Hassan et al., 2020). However, one study, which evaluated trauma-focused CBT, found no significant changes in depression scores after the intervention (Madigan et al., 2015).
Overall, there is strong evidence supporting the effectiveness of cognitive-based interventions for managing depression in women with high-risk pregnancies.
Counseling-Based Interventions
Three studies—one Level 1b study (Burgio et al., 2024) and two Level 2b studies (Elsharkawy et al., 2021; Rafie et al., 2023)—investigated the effects of counseling-based interventions on depression among women with high-risk pregnancies.
In the Level 1b study by Burgio et al. (2024), psychological counseling was delivered to pregnant women with high-risk pregnancies and their spouses. Although depression scores were significantly reduced among fathers in the experimental group compared with the control group, no significant change was observed in the depression scores of pregnant women who received counseling in the intervention group compared with the control group.
In the Level 2b studies, both solution-focused counseling (Rafie et al., 2023) and happiness counseling (Elsharkawy et al., 2021) demonstrated significant reductions in mean depression scores in the intervention group compared with the control group.
Given the observed inconsistencies in the findings, there is moderate-level evidence supporting the effectiveness of counseling-based interventions for managing depression among women with high-risk pregnancies.
Emotion-Based Interventions
Three studies—two Level 2b studies (Gallagher et al., 2020; Wang et al., 2021) and one Level 3b study (Goetz et al., 2020)—examined the effects of emotion-based interventions on depression among women with high-risk pregnancies. The interventions included yoga (Gallagher et al., 2020) and mindfulness-based interventions (Goetz et al., 2020; Wang et al., 2021).
Both Level 2b studies reported significant reductions in depression scores postintervention (Gallagher et al., 2020; Wang et al., 2021). In contrast, the Level 3b study found no significant change in mean depression scores after the electronic mindfulness-based intervention (Goetz et al., 2020).
Thus, there is moderate evidence supporting the use of emotion-based interventions for managing depression among women with high-risk pregnancies, although some variability in findings warrants further investigation.
Sensory-Based Interventions
One Level 2b study investigated the impact of aromatherapy, a sensory-based intervention, on depression scores of women with high-risk pregnancies. The study found no significant change in mean depression scores in the treatment group compared with the control group postintervention. Therefore, there is low evidence to support the effectiveness of sensory-based interventions for managing depression among women with high-risk pregnancies (Go & Park, 2017).
Integrated Approaches
One Level 2b study examined an integrated approach involving mindfulness-based cognitive therapy for depression among women with high-risk pregnancies. The study reported that mean depression scores were significantly lower in the intervention group compared with the control group postintervention. Thus, there is low-strength evidence supporting the use of integrated interventions for managing depression among women with high-risk pregnancies (Musavi & Narimani, 2015).
Stress
Eighteen studies reported on stress, with the majority assessing it with the Perceived Stress Scale (n = 8; 44%).
Cognitive-Based Interventions
Two Level 1b studies (Mirtabar et al., 2020; Urech et al., 2017) and four Level 2b studies (Asghari et al., 2016; Chaharrahifard et al., 2021; Hassan et al., 2020; Scherer et al., 2016) assessed the effects of cognitive-based interventions on stress in high-risk pregnancies. In both Level 1b studies, significant reductions in mean stress scores were reported after cognitive-based interventions. However, whereas Mirtabar et al. (2020) observed significant improvement in comparison with a routine-care-only control group, Urech et al. (2017) found no difference in postintervention scores compared with a control group receiving occupation-based intervention. The findings from the Level 2b studies were consistent with those from the Level 1b studies, indicating strong evidence supporting cognitive-based interventions for stress.
Counseling-Based Interventions
One Level 1b study (Burgio et al., 2024) and four Level 2b studies (Aliabadi et al., 2022; Elsharkawy et al., 2021; Rafie et al., 2023; Ugurlu et al., 2021) assessed the impact of counseling-based interventions on stress among women with high-risk pregnancies. All studies reported significant improvements in stress scores after treatment, demonstrating strong evidence to support counseling-based interventions for stress among women with high-risk pregnancies.
Emotion-Based Interventions
Three studies evaluated emotion-based interventions. The first, a Level 1b study (Ibıcı Akca et al., 2023), found no significant difference in mean stress scores between participants who underwent a mindfulness-based stress reduction program and those who received routine care only. However, lower-level studies presented contrary findings. Flynn et al. (2016; Level 3b) observed improvements in stress scores with guided imagery, and Wang et al. (2021; Level 2b) found significant reductions in stress with a mindfulness intervention. Therefore, there is low-strength evidence to support emotion-based interventions for stress among women with high-risk pregnancies.
Sensory-Based Interventions
Two studies, one Level 1b (Teckenberg-Jansson et al., 2019) and one Level 2b (Go & Park, 2017), assessed sensory-based interventions for stress among women with high-risk pregnancies. The findings were mixed: Teckenberg-Jansson et al. (2019) found no significant difference in mean stress scores among women who underwent music therapy, whereas Go and Park (2017) reported a significant reduction in stress scores among those who received aromatherapy. Hence, there is low-strength evidence for sensory-based interventions in this context.
Integrated Approaches
Two Level 2b studies used integrated approaches for managing stress among women with high-risk pregnancies: mindfulness-based cognitive therapy (Musavi & Narimani, 2015) and mindfulness-based counseling (Zeinabeh et al., 2023). Both studies found significant reductions in stress scores in the experimental groups compared with the control groups postintervention, providing strong evidence to support the use of integrated approaches for managing stress among women with high-risk pregnancies.
QoL
Five studies assessed QoL, with the most commonly used tools being the 36-Item Short Form Health Survey (SF–36; n = 2; 40%) and the World Health Organization Quality of Life (n = 2; 40%).
Counseling-Based Interventions
Three studies examined the effectiveness of counseling interventions on QoL among women with high-risk pregnancies. Two were Level 2b studies (Ahmadinejad et al., 2022; Atef et al., 2022), and one was a Level 1b study (Ghasemi et al., 2021). All three studies found significant improvements in QoL scores after counseling among the intervention group compared with the control group. Ghasemi et al. (2021) compared two modes of delivery—WhatsApp versus face-to-face counseling—and found both to be equally effective. Atef et al. (2022) compared cognitive-based counseling with relaxation techniques and reported that the increase in QoL scores was significantly higher in the cognitive counseling group than in the relaxation group. Hence, there is moderate evidence supporting counseling interventions for improving QoL among women with high-risk pregnancies.
Emotion-Based Interventions
Two studies explored emotion-focused approaches to improving QoL. The first, a Level 2b study by Atef et al. (2022), compared cognitive counseling with relaxation techniques. The relaxation group underwent four sessions of Jacobson’s relaxation exercises. Compared with baseline scores, significant improvements in QoL scores were observed at the end of the study. Khoraminejad et al. (2021), in a Level 2b pretest–posttest study, also reported that compassion-focused therapy and acceptance and commitment therapy led to significant improvements in QoL scores compared with the control group. Therefore, there is moderate-strength evidence supporting emotion-focused interventions for improving QoL among women with high-risk pregnancies.
Integrated Approaches
One Level 1b study (Moghimi et al., 2022) examined the effect of mindfulness-based CBT on QoL among 88 women with high-risk pregnancies, using the SF–36 scale to assess QoL. The study found a significant increase in total QoL scores postintervention compared with the control group, providing moderate evidence to support the use of mindfulness-based CBT in improving QoL for high-risk pregnancies.
Other Occupational Therapy–Related Outcomes
This review also identified other key occupational therapy–related outcomes assessed in the included studies.
Self-efficacy was evaluated in five studies (Bakhteh et al., 2018; Ghasemi et al., 2021; Rafie et al., 2023; Ugurlu et al., 2021; Zhihui & Zhang, 2020). In two studies, one Level 1b study (Zhihui & Zhang, 2020) and one Level 2b study (Bakhteh et al., 2018), cognitive-based interventions significantly improved self-efficacy in the intervention group compared with the control group.
In three studies, one Level 1b (Ghasemi et al., 2021) and two Level 2b (Rafie et al., 2023; Ugurlu et al., 2021), counseling-based interventions were administered. Two of these studies (Ghasemi et al., 2021; Rafie et al., 2023) showed improvements in self-efficacy, and one study (Ugurlu et al., 2021) found contrary results. As a result, there is strong evidence supporting the effectiveness of cognitive-based and counseling-based interventions in improving self-efficacy.
One Level 2b study (Chaharrahifard et al., 2021) assessed parental competency, and another (Hassan et al., 2020) evaluated coping patterns. In both studies, cognitive-based interventions significantly improved parental competency and coping patterns. However, given the limited number of studies, further research is needed to strengthen these findings.
Risk of Bias
The quality assessment of the included studies identified 16 with a low risk of bias and 18 with a moderate risk of bias. Full details are provided in Tables A.3 and A.4.
Discussion
This systematic review aimed to examine the evidence regarding psychosocial occupational therapy interventions for anxiety, depression, stress, and QoL among women with high-risk pregnancies. To the best of our knowledge, this is the first systematic review to explore this topic.
Our review underscores the significance of cognitive-based interventions as a powerful tool in occupational therapy for supporting women experiencing a high-risk pregnancy. This aligns with the findings of Loughnan et al. (2019), Puertas-Gonzalez et al. (2021), Shortis et al. (2020), and Sockol (2015), who demonstrated the efficacy of cognitive–behavioral interventions in managing perinatal anxiety, depression, and stress. Cognitive-based interventions—centered on cognitive restructuring, emotional regulation, and adaptive coping—directly enhance a woman’s ability to engage in meaningful occupations such as self-care, household management, work, and social participation (Curtiss et al., 2021; McCoyd et al., 2020; Nakao et al., 2021; Suzuki et al., 2011). For occupational therapy practitioners, this calls for the inclusion of cognitive–behavioral techniques in activity-based sessions and a greater emphasis on emotional and cognitive assessments during the perinatal period. Interdisciplinary collaboration, particularly with mental health providers, can ensure more cohesive and effective care that supports both emotional well-being and occupational performance.
Counseling-based interventions also demonstrated moderate to strong evidence in managing anxiety, depression, and stress among women experiencing a high-risk pregnancy. These findings, consistent with those of prior studies (Fooladiha et al., 2022; Yeşildere Sağlam et al., 2025), highlight the role of counseling in improving psychological well-being in perinatal populations. Counseling aligns with the client-centered ethos of occupational therapy and offers a therapeutic avenue to support emotional health in conjunction with functional goals (Mroz et al., 2015). It enhances key psychosocial capacities such as self-awareness, emotional regulation, and cognitive reframing that are essential for sustaining engagement in meaningful occupations. All of these interventions foster resilience, enabling clients to better manage the unpredictable challenges of high-risk pregnancy while continuing to participate in valued roles and routines (Bakhtari-Aghdam et al., 2023; Dewidar et al., 2023; Helmreich et al., 2017). Actionable steps for occupational therapy practitioners include incorporating brief, structured emotional check-ins during sessions, using guided journaling or values clarification exercises to promote self-awareness, and facilitating problem-solving dialogues to reframe negative thought patterns. These methods, integrated into routine occupational therapy practice, support mental well-being while advancing occupational performance.
Emotion-based interventions, such as mindfulness and yoga, demonstrated low to moderate evidence for managing mental health symptoms and improving QoL among women with high-risk pregnancies. These findings contrast with those of prior research (Hoge et al., 2021; La Torre et al., 2020; Li et al., 2024) that support mindfulness-based approaches as effective tools for reducing perinatal depression, anxiety, and stress. The discrepancy may be attributed to variability in intervention delivery, inconsistent protocols, and methodological limitations, such as small sample sizes and lack of standardization, as noted by Butterfield et al. (2017). Despite these challenges, the potential benefits of mindfulness and yoga for relaxation, emotional regulation, and stress reduction make them relevant modalities for occupational therapy, particularly when emotional vulnerability impedes engagement in daily occupations (Srisopa et al., 2021). Future research should focus on developing standardized occupational therapy protocols that integrate mindfulness and yoga into activity-based frameworks, examining their impact on both psychological outcomes and occupational performance in perinatal care.
Sensory-based interventions, including music therapy and aromatherapy, showed low overall effectiveness in managing anxiety, depression, stress, and QoL among women with high-risk pregnancies. This raises important considerations for their utility in occupational therapy practice. Although some studies have reported momentary reductions in stress and anxiety (Ebrahimi et al., 2022; Janthasila & Keeratisiroj, 2023; Zamanifar et al., 2020), the largely passive nature of these interventions likely limits their capacity to facilitate lasting psychological change. Unlike cognitive or counseling-based approaches, sensory interventions may not sufficiently engage clients in active self-reflection, problem-solving, or behavior change—all critical processes for improving mental health outcomes. This aligns with concerns noted in the literature about the lack of depth and standardization in such approaches (Fung et al., 2021; Kuriyama et al., 2005). Despite their limitations, sensory-based interventions may still have a role as adjunctive strategies within a broader occupational therapy framework. Occupational therapists can use them intentionally to create calming environments that prepare clients for more active therapeutic engagement. These tools could also be incorporated into personalized sensory kits for clients to use at home, helping them manage acute stress in the moment. However, occupational therapy practitioners should be cautious not to rely on these methods as stand-alone interventions for addressing the complex emotional and psychological needs of women with high-risk pregnancies.
Integrated approaches, such as combining mindfulness-based interventions with cognitive therapy, showed mixed evidence for managing anxiety, depression, stress, and QoL among women with high-risk pregnancies. The small number of studies in this area limits the ability to draw firm conclusions, underscoring the need for further research into the effectiveness of these combined methods. Given the complex psychosocial demands of high-risk pregnancies, combining cognitive, emotional, and behavioral techniques may offer more comprehensive support than single-modality approaches. Occupational therapy practitioners working in prenatal care settings can integrate CBT techniques during prenatal visits to help women identify stressors that interfere with self-care and ADL routines. In home-based occupational therapy, practitioners can use emotion-based interventions such as mindfulness training to help expectant mothers develop self-regulation strategies that support infant bonding and role adaptation.
Similarly, interventions targeting self-efficacy and coping mechanisms were underexplored in the literature, making it difficult to form a definitive conclusion. Further studies in these areas would provide valuable insights into the effectiveness of such interventions in supporting mental health and occupational engagement in women with high-risk pregnancies.
Limitations
Our review has some limitations that should be acknowledged. More than half of the included studies were conducted in countries with health care systems that differ significantly from that of the United States, which may limit the generalizability of the findings to U.S.-based health care and occupational therapy settings. Also, not all of the studies were occupational therapy–led, meaning that the interventions may not have been designed or delivered with an occupation-centered focus, which affects the direct applicability of findings to occupational therapy practice.
The narrative synthesis approach introduced potential subjectivity in interpreting the results, and the variation in study designs, interventions, and outcome measures made it difficult to compare findings across studies. Additionally, some studies had methodological weaknesses, limiting the strength of the evidence. Despite these limitations, the review provides valuable insights into the potential role of psychosocial interventions in improving mental health and occupational outcomes for women with high-risk pregnancies, highlighting areas for further research and development in occupational therapy practice.
Implications for Occupational Therapy Practice
Occupational therapists are uniquely positioned to integrate evidence-based psychosocial interventions into holistic care plans for women experiencing high-risk pregnancies. By embedding CBT and counseling strategies into daily routines, occupational therapy practitioners can address both mental health and occupational performance. For instance, an occupational therapist working with a client managing gestational diabetes might incorporate brief journaling exercises before meal preparation to facilitate stress management and nutritional planning. Similarly, solution-focused questioning can be used during home safety assessments to empower clients in problem-solving and adapting their environments.
Emotion-based strategies such as mindfulness and gentle yoga can serve as “microbreaks” during activities such as folding laundry or as tools to facilitate task pacing. By incorporating these interventions in everyday occupations, occupational therapists help clients develop and apply coping strategies in meaningful, real-life contexts.
Although current clinical protocols and expert consensus support the relevance of occupational therapy in maternal health, there remains a critical need for empirical studies to validate and expand the evidence base. Increasing occupational therapy services in maternity wards and community settings could significantly improve maternal health outcomes, ensuring care remains client centered, culturally responsive, and occupation focused. From a policy perspective, there is strong support for positioning occupational therapists in maternity care settings, including hospitals and community services, to provide evidence-based, comprehensive care. Future research should focus on evaluating the impact of occupational therapy interventions on maternal mental health and daily functioning, solidifying the profession’s role in supporting women during high-risk pregnancies.
Conclusion
In conclusion, although cognitive-based and counseling-based interventions show strong evidence for improving mental health and QoL, emotion-based and sensory-based interventions offer more limited evidence. Integrated approaches may hold promise but require further investigation. These findings underscore the importance of tailoring interventions to the unique needs of women with high-risk pregnancies and highlight the potential for occupational therapy to integrate these approaches into holistic care models. Despite the growing body of evidence on psychosocial interventions for high-risk pregnancies, the research on occupational therapy–specific interventions that address both mental health and occupational engagement is limited. Future studies should explore how occupational therapy practitioners can adapt and deliver established interventions—such as CBT and mindfulness—in the context of everyday routines. For example, piloting occupational therapy–led CBT programs in U.S. prenatal clinics could help support functional participation in parenting, work, and self-care during pregnancy. Further research should also aim to identify which strategies are most effective in addressing areas of limited or mixed evidence, ultimately strengthening the role of occupational therapy in perinatal mental health care.
Supplemental Material
Supplementary material for Psychosocial Occupational Therapy Interventions for High-Risk Pregnancies: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051199.pdf for Psychosocial Occupational Therapy Interventions for High-Risk Pregnancies: A Systematic Review by Sabina Khan, Thuy Tran, Christianah Edema, Jessica Grant, Laritza Olivares and Viviana Ferreira in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We sincerely thank Nadia Hommerding for her guidance and expertise in designing the literature searches that supported this study.
*Indicates articles included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.