
Abstract
This study examined task-oriented circuit training, a structured program delivered through face-to-face, telerehabilitation, and home-based methods.
Given the fast pace where the population is aging—in developed countries, in particular—rehabilitation interventions with good efficacy that are tailored for the older adults are increasingly needed (Krzyzaniak et al., 2023; Yáñez-Yáñez et al., 2023). Nursing homes play a key role in supporting the health and well-being of elderly people, especially those experiencing decline. Factors such as health status, social relationships, social support, and physical activity significantly affect their quality of life (Dung et al., 2020).
Task-oriented circuit training (TOCT) is a rehabilitation technique involving a series of functional tasks in a structured circuit, which has demonstrated positive results in improving motor functions and daily activities (Gbiri & Amusa, 2020). Such improvements are likely facilitated through multiple neural pathways and could thus promote neuroplasticity, as suggested by similar research on functional rehabilitation (Moon et al., 2018; Ozkul et al., 2020). The face-to-face rehabilitation method improves the therapeutic alliance, one of the most important factors in successful rehabilitation (Sánchez-Guarnido et al., 2021). The literature suggests that comprehensive and face-to-face interventions promote favorable rehabilitation outcomes, particularly in the motor function of patients (Wang et al., 2014). In this regard, telerehabilitation methods may be one of the answers to meet elderly people’s needs for rehabilitation, considering both home-based rehabilitation and nursing home settings (Saito & Izawa, 2021). Recent systematic reviews support this approach, demonstrating that telerehabilitation is an effective and acceptable alternative to conventional rehabilitation methods, particularly for improving functional performance and quality of life among older adults (Gamble et al., 2024; Man et al., 2024; Velayati et al., 2020).
Feasibility is considered by the fact that it may allow access to rehabilitation services, particularly in cases where people live in a widely dispersed manner in countries with inadequate traditional services. In support, studies have indicated that telerehabilitation provides an opportunity to overcome the visit-associated barriers in many clinics, thus enhancing access to older adults who may have mobility challenges or reside in underserved areas (Gün & Gün, 2022). However, for successful implementation of telerehabilitation, quite a few challenges must be overcome, such as technology barriers, patient engagement, and adequate training for health care providers, especially in the context of elderly patients (Peretti et al., 2017). Home-based rehabilitation programs offer immense benefits to older adults by helping them get care in a familiar environment, which helps provide them with comfort and independence (Velez et al., 2023). Such programs can improve both cognitive and motor functions through targeted exercises tailored to the specific needs of older adult patients (Parvatham et al., 2022). However, there are challenges, including variability in service delivery between regions and the reluctance of some older adults to engage in home-based programs, arising from their inclination to social interaction offered in traditional rehabilitation settings (Polgar et al., 2022). Furthermore, the lack of resources and support for caregivers serves as a barrier to successful home-based rehabilitation interventions (Lee et al., 2018). Of the rehabilitation programs aimed at improving the functional abilities of residents and applied in nursing homes, TOCT has been considered an accessible method among rehabilitation programs (Aravind et al., 2021). This approach highlights the value of structured activities that mirror daily tasks, thereby promoting skill transfer and improving overall quality of life (Yoo & Park, 2015). However, some of the barriers to effective rehabilitation in these settings include staff shortages, restrictive regulations, and requirements for specialist training of nursing staff (Aravind et al., 2021; Yoo & Park, 2015).
Despite the growing literature on various rehabilitations, there are some significant gaps in literature available on the different rehabilitation methods, especially in terms of comparative effectiveness of face-to-face, telerehabilitation, and home-based rehabilitation methods. These represent literature gaps that indicate a need for rigorous, comparative studies, not only in assessing the efficacy of these various rehabilitation modalities but also in exploring their integration into a cohesive strategy that optimizes patient outcomes across diverse settings (LaMarca et al., 2023; Mohr et al., 2012).
Despite the brevity of a 2-wk intervention, prior research suggests that even short-term, structured TOCT programs can yield substantial benefits. For example, Jeon et al. (2015) found that interventions lasting 2 wk yielded the largest effect sizes for motor outcomes such as strength, balance, and gait. Similarly, Gbiri and Amusa (2020) reported significant improvements in cognition, physical functioning, and social participation among patients with dementia after a progressive TOCT program. Building on these findings, in the present study, we aimed to evaluate the feasibility of delivering a short-term (2-wk) TOCT program to older adults through various (face-to-face, telerehabilitation, and home-based) modalities and to explore preliminary evidence of its impact on cognitive and motor functions. In light of this evidence, we hypothesize that even a brief, 2-wk intervention will be sufficient to elicit measurable improvements in cognitive and motor functioning among older adults.
Method
Study Design
We conducted this single-blind, parallel-group, randomized feasibility study with 54 older adults residing in a state-operated skilled nursing facility (SNF) in Cankiri, Turkey, from June 2023 to November 2023. The SNF offers assistance with activities of daily living; a physician and nursing staff are present on-site for routine monitoring and emergency care, but no intensive medical services are provided.
This study was conducted in accordance with the Declaration of Helsinki guidelines, reviewed and approved by the Cankiri Karatekin University, University Ethics Committee in Cankiri, Turkey (Ethics no. d897232bb89442f7). It also complied with the CONSORT reporting guidelines (Schulz et al., 2010).
Participants
We conducted this study in a nursing home for older adults who generally have independent living skills and are able to perform most of their daily activities independently. The eligibility criteria required participants to be 65 yr or older, residing in the designated nursing home, and in stable physical health that allowing them to safely participate in the interventions. The participants needed to demonstrate sufficient cognitive function, indicated by a Mini-Mental State Examination (MMSE; Crum et al., 1993) score of 18 or higher. Exclusion criteria included adults with severe cognitive impairments, such as those diagnosed with advanced Alzheimer’s disease or other forms of dementia, characterized by an MMSE score lower than 18 (Monroe & Carter, 2012). Older adults with severe mobility restrictions, including those who were unable to walk unaided, who were reliant on mobility aids, or who had a recent stroke that caused functional limitations, were excluded. Those with advanced arthritis causing significant pain or movement limitations were also not eligible. The diagnoses received by the older adults were determined through the review of documents required during their admission to the nursing home.
Sample Size and Random Sampling
In this study, we did not perform a power calculation, because our primary aim was to determine feasibility. Participants were assigned to intervention groups (face-to-face, telerehabilitation, or home-based) using balanced block randomization (blocks of six) through an online platform. An independent researcher managed randomization and retained group assignments. To ensure unbiased assessment, allocation was concealed from assessors. The initial set included 18 participants each in the face-to-face, telerehabilitation, and home program intervention groups, created using the block method.
Study Procedure
After obtaining informed consent, we collected demographic data from participants or caregivers. A single occupational therapist, trained by a senior specialist, administered the interventions to ensure consistency. Attendance was recorded daily, and the program was coordinated with nursing home management. The home program was monitored by facility staff, providing feedback twice a week.
The 60-min daily sessions over 2 wk aimed to achieve measurable short-term outcomes while preventing fatigue. This duration balanced intensive treatment with the practical constraints of the nursing home setting.
Interventions
Participants were assigned to face-to-face, remote (video conference), or self-administered, home-based occupational therapy. Each group completed nine individually tailored activities designed to enhance cognitive processes, manual dexterity, and physical functioning, supporting independence and quality of life. Such activities included a range of tasks targeted at the stimulation of cognitive processes, manual dexterity, and the maintenance of physical activity, in view of addressing the multifaceted needs of the older adults. All groups engaged in nine structured activities during a single intervention session. The activities were carried out sequentially on the same day, with short 2-min breaks between activities to support sustained attention and minimize fatigue. This standardized structure was applied consistently across all three intervention formats to ensure procedural uniformity and comparability between groups. In the Energy Conservation Station, for example, a participant who reported early fatigue while cleaning the kitchen counter was guided to explore alternative methods, such as sitting while wiping surfaces, using long-handled tools, and performing the task in shorter segments. The occupational therapist also introduced the use of a visual activity planner to help the participant break the task into manageable steps across the day rather than completing it all at once.
The activities at each station were selected on the basis of real-life difficulties and delivered under the guidance of an occupational therapist who adapted the tasks according to each participant’s functional limitations and daily life priorities (Maggio et al., 2024; Ozkul et al., 2020; Park & Son, 2022): Joint Protection Station: The patients learned the joint protection techniques through tasks, (e.g., hanging and retrieving shirts from a bar set at a specific height). This activity was meant to teach ways of performing daily tasks efficiently with minimum stress on the joints. Attention Station: This included observing a picture and drawing to replicate it or following a numerical sequence to complete an image. These were meant to boost the patients’ visual attention and focus. Fine Motor Skills Station: Participants threaded beads in a specified color sequence to build fine motor and color recognition skills. This station aimed to enhance hand coordination through fine motor tasks that required precise movement and visual–motor integration, similar to chopstick use, which improves dexterity and cortical excitability. Energy Conservation Station: Activities of daily living, such as opening a jar lid, were used to teach participants how to save energy while doing various activities, being as effective as possible with the least amount of effort. Gross Grasp Skills Station: Manipulating cups from an upside-down to a right-side-up position assisted in developing gross grasp and arm coordination. Memory Station: Memory cards were used to improve short-term memory and object-matching skills, targeting the cognitive functions essential for maintaining healthy cognition and preventing decline. Distal Tip Pinch Skills Station: Cutting square pieces from newspaper clippings helped develop precise distal tip pinch skills by focusing on the fine hand and finger movements. Hand Skills Station: Activities such as buttoning or placing specific shapes in their respective slots helped improve fine motor skills and problem solving. Precision Hand Skills Station: Filling a spoon with a certain amount of rice helped patients deal with precise hand skills and estimated quantities.
The telerehabilitation program was conveyed across the internet through Zoom (Zoom Video Communications Inc., San Jose, CA), a synchronous videoconferencing platform. Initially, staff reported issues. TeamViewer (TeamViewer, Göppingen, Germany) was used for remote control. A two-way audiovisual communication enabled all parties to interact, and the participants were guided by the therapist through an occupational program. In this way, the therapist was able to provide real-time feedback and modification.
Individualized interventions of the home-based occupational therapy program were executed in the nursing home environment of the participant. The aim was to enhance the participant’s functional abilities in daily activities, emphasizing adaptation to the home environment. These trainings were assigned as “homework,” ensuring that more than 90% of the training days and circuits were completed. The materials for the home program were prepared in advance and set up in a designated room. Participants were expected to complete the circuit under the supervision of the nursing home staff to ensure both safety and adherence to the program. The therapist contacted the staff regularly to provide guidance and monitor progress.
Measures
Outcome measures were administered by a blinded assessor to make the measures objective with least bias. The mode of administration of outcome measures was standardized for all groups; the administration was conducted face-to-face, independent of the method of intervention that a participant received.
Primary Outcomes
Recruitment and Retention Rates
We used a detailed checklist to accurately measure the registration and retention rates. This checklist was designed to capture key information, including the time to begin participation, frequency of engagement, intention to continue, and reasons for potential dropout. Each checklist was carefully reviewed to ensure completeness and accuracy of the data (Frampton et al., 2020).
MMSE
The MMSE is a 30-point instrument that remains the benchmark for rapid evaluation of global cognition, probing orientation, memory, attention and calculation, language, and visuospatial abilities within minutes. Beyond its ubiquity in clinical practice, the MMSE has been rigorously validated among older adults, demonstrating acceptable test–retest reliability (intraclass correlation coefficient [ICC] = .75) and thus serving as a reliable metric for repeated cognitive assessments in this population (Feeney et al., 2016; Truong et al., 2024).
A 30-point scale, the MMSE is one of the most widely used tools for quick assessment of the status of a patient’s cognition. The domains assessed in this test include orientation, memory, attention and calculation, language skills, and visuospatial abilities. A score of 24 and higher generally indicates that a person has normal cognitive functioning, whereas a score less than 24 shows potential cognitive impairment (Güngen et al., 2002). Patients with mild cognitive impairment who scored higher than 18 were included in our study, whereas those classified as moderate (scores between 10 and 18) or severe (scores ≤10) and scored below 18 were excluded from the study.
Montreal Cognitive Assessment
The Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005) provides a broad assessment for the detection of mild cognitive impairments and early dementia. It specifically tests attention and concentration, executive functions, memory, language, visuospatial skills, abstraction, calculation, and orientation. The maximum score is 30 points. Scores of 26 and higher are regarded as normal. A score below this limit indicates cognitive impairment (Ozdilek & Kenangil, 2014). The MoCA has shown high internal consistency (Cronbach’s α ≈ .83) and excellent test–retest reliability in older adults (rs = .75–.93), supporting its use as a reliable and valid cognitive screening tool for detecting subtle cognitive changes in this population (Daniel et al., 2022; Nasreddine et al., 2005).
Secondary Outcomes
The Nine-Hole Peg Test (NHPT; Mathiowetz et al., 1985) is used to evaluate fine motor skills and hand–eye coordination in the upper extremities. A participant is required to insert a series of small pegs into holes on a board and then to remove the pegs as quickly as possible. The time is measured separately for each hand, thus giving an objective measure of the participant’s motor skills. Shorter completion times indicate better manual dexterity and enhanced motor performance (Earhart et al., 2011). Among older adults, the NHPT has demonstrated excellent interrater reliability (ICC = .983) and solid construct validity, confirming its suitability as a reliable and valid outcome measure of manual dexterity in this population (Brandon et al., 2023; Proud et al., 2020).
The 36-Item Short Form Health Survey (SF–36; Brazier et al., 1992) is one of the most commonly used questionnaires for a person’s physical and mental health status. Its 36 questions measure a wide range of variables related to quality of life: physical functioning, bodily pain, general health perception, energy and vitality, social functioning, role limitations because of physical problems, role limitations because of emotional problems, and mental health. The scores for each dimension range from 0 to 100, with higher scores indicating better health status. The SF–36 has achieved international recognition because of its ability to carry out an objective quality-of-life assessment in a wide variety of patient and population groups effectively (Demiral et al., 2006). Among older adults, the SF–36 demonstrates strong psychometric properties, with ICCs exceeding .80 for most subscales and good-to-excellent test–retest reliability over 1 wk (ICC = .55–.82). These findings endorse the SF–36 as a valid and reliable tool for assessing health-related quality of life in older populations, including residents of long-term care settings (Andresen et al., 1999; Brazier et al., 1992; Walters et al., 2001).
Statistical Analysis
We performed data analyses using IBM SPSS Statistics (Version 28). Descriptive statistics are presented as means and standard deviations for continuous variables and frequencies and percentages for categorical variables. We assessed the normality of continuous variables using the Kolmogorov–Smirnov test, histogram analysis, and Q-Q plot examinations, all of which supported the assumption of normality. Initially, we used a one-way analysis of variance to assess the homogeneity of groups. A significance level of p < .05 was set for all statistical tests. We calculated Cohen’s d for each outcome to assess the effect size, providing 95% confidence intervals to offer a comprehensive interpretation of the results. Cohen’s d interprets effect size: small, 0.2; moderate, 0.5; and large, 0.8 (Panjeh et al., 2023). Additionally, missing data were handled using a complete-case analysis, wherein only data from participants who completed the intervention were included in the final analysis. To maintain the integrity of the study, the statistical analyst was blinded to the group allocations. All data provided to the analyst were coded, ensuring that blinding was preserved throughout the analysis process.
Results
Figure 1 illustrates the participant flow and study process, highlighting key feasibility steps such as recruitment, eligibility assessment, group assignment, and intervention participation. Of the 132 participants screened, 21 were excluded for not meeting inclusion criteria, and 22 declined because of social anxiety, discomfort, or difficulty participating. Older adults with mild cognitive impairment (MMSE scores >18) were included, whereas those with moderate or severe impairment (MMSE scores ≤18) were excluded.
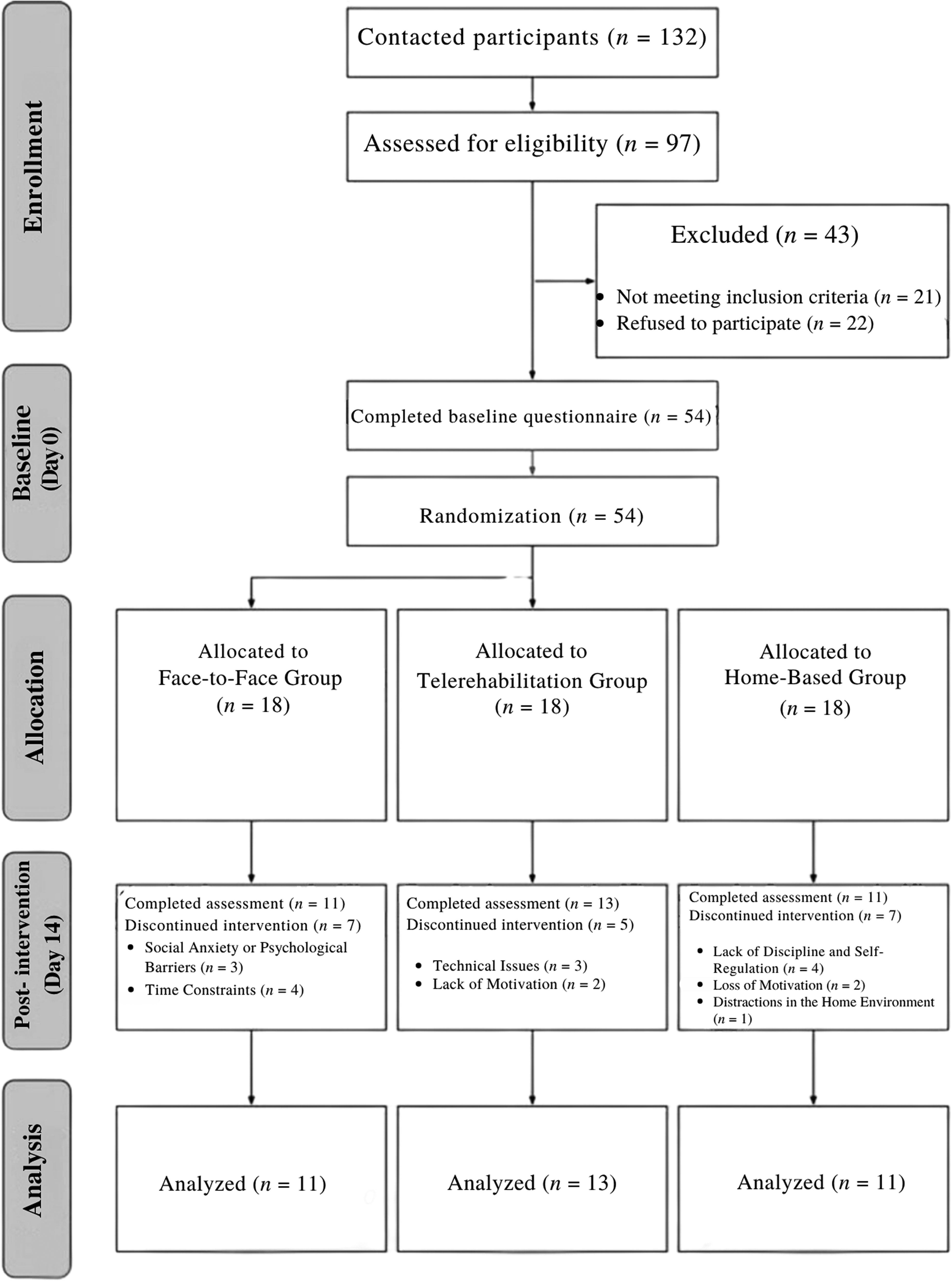
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of participant selection.
Participants were randomly assigned to three groups (18 each): face-to-face, telerehabilitation, and home-based. In the face-to-face group, 11 participants completed the intervention, whereas 7 dropped out because of social anxiety or time constraints. The telerehabilitation group had 13 completions, with 5 dropouts because of technical issues or lack of motivation. In the home-based group, 11 completed the study, whereas 7 dropped out because of lack of discipline, motivation, or home distractions. Self-regulation challenges affected adherence, particularly in home-based programs (Figure 1).
According to the results in Table 1, there was no significant difference between the groups in terms of gender; marital status; education level; social security; age; or MoCA, MMSE, or NHPT scores. The home-based group showed higher energy and vitality levels compared with the other groups at baseline. However, no significant differences were observed between the groups on the other subscales of the SF–36.
Comparison of Demographic Characteristics and Baseline Functional and Cognitive Scores Among Face-to-Face, Telerehabilitation, and Home-Based Program Groups
Note. A one-way analysis of variance was used for numeric variables, and a χ2 test was used for categorical variables. Boldface indicates p < .05. CCI = Charlson Comorbidity Index; MMSE = Mini-Mental State Examination; MoCA = Montreal Cognitive Assessment; NHPT = Nine-Hole Peg Test; SF–36 = 36-Item Short Form Health Survey.
aRange = 0–30.
bRange = 0–100.
cRange = 0–37.
The study showed high participant engagement, with registration and retention rates exceeding 90%. Between-groups comparisons revealed that face-to-face training led to the greatest cognitive improvements, with moderate advantages over home-based training and slight differences from telerehabilitation; specifically, this group achieved a 2.46-point gain on the MoCA (d = 1.12) in addition to the largest MMSE change. Telerehabilitation improved energy and vitality levels more than the home-based program, whereas social functioning was significantly better in telerehabilitation than home-based training: It also produced a 2.18-point MoCA increase (d = 0.68), underscoring meaningful cognitive benefit. Fine motor improvements were similar across groups, with no major differences in nondominant hand performance. Within-group analyses showed that all interventions improved cognitive and motor functions, although to varying degrees: Face-to-face training showed the largest cognitive gains; telerehabilitation enhanced energy and vitality levels and social functioning; and home-based training—although yielding the smallest cognitive change of 1.09 on the MoCA (d = 0.44)—showed the most improvement in fine motor skills, particularly in the nondominant hand (Table 2). Between-groups effect sizes indicated that face-to-face delivery produced greater improvements in cognitive outcomes, with a Cohen’s d of 0.57 for the MoCA and .56 for the MMSE, compared with home-based training. In contrast, telerehabilitation was more effective in enhancing quality-of-life domains, particularly energy and vitality (Cohen’s d = 0.91) and social functioning (Cohen’s d = 1.41), relative to home-based delivery (Table 3).
Within-Group Changes and Effect Sizes for TOCT Delivered via Face-to-Face, Telerehabilitation, and Home-Based Methods on Cognitive, Motor, and Quality-of-Life Outcomes
Note. Effect size is presented as Cohen’s d. CI = confidence interval; MMSE = Mini-Mental State Examination; MoCA = Montreal Cognitive Assessment; NHPT = Nine-Hole Peg Test; SF–36 = Short Form Health Survey–36; Δ: Change score (Time 1 – Time 2); TOCT = Task-Oriented Circuit Training.
aRange = 0–30.
Between-Groups Comparisons of TOCT Delivered Through Face-to-Face, Telerehabilitation, and Home-Based Methods on Cognitive, Motor, and Quality-of-Life Outcomes
Note. CI = confidence interval; MMSE = Mini-Mental State Examination; MoCA = Montreal Cognitive Assessment; NHPT = Nine-Hole Peg Test; SF–36 = Short Form Health Survey–36; TOCT = Task-Oriented Circuit Training.
Discussion
This study evaluated the feasibility and effectiveness of TOCT delivered through face-to-face, telerehabilitation, and home-based methods in improving cognitive function, fine motor skills, and quality of life in older adults. Face-to-face training led to the greatest cognitive improvements, whereas telerehabilitation had the strongest impact on quality of life, particularly in energy and vitality and social functioning. The home-based program showed the most improvement in fine motor skills but had limited effects on cognitive function and quality of life. Fine motor skill improvements were similar across groups, with no significant differences in nondominant hand performance on the NHPT. All three interventions resulted in positive changes, although effect sizes varied. The high retention and registration rates (above 90%) indicate strong feasibility and adherence. These findings support the potential benefits of short-term interventions in older adults, with structured, supervised programs proving more effective than self-directed home programs.
Short-term interventions (around 2 wk) have been shown to yield measurable improvements in MMSE, MoCA, NHPT, and SF–36 scores in older or rehabilitation populations. For example, a 10-d cognitive training program in older adults with mild cognitive impairment produced significant gains on both the MMSE and MoCA, with mean improvements of approximately 4.9 and 6.4 points, respectively, compared with minimal changes among control participants (Li et al., 2025). Similarly, performance-based tests such as the NHPT have demonstrated responsiveness to short-term interventions, with notable improvements in hand dexterity after 3 wk of intensive arm therapy in patients during the subacute stroke period (Horn et al., 2016). Patient-reported outcome measures such as the SF–36 have also captured substantial improvements after brief rehabilitation programs; for example, a 2-wk comprehensive intervention led to a 9.5-point increase in SF–36 scores among breast cancer survivors at follow-up (Kwiatkowski et al., 2013). These findings support the selection of the outcome measures used in the present study and suggest that the observed cognitive, motor, and quality-of-life improvements are likely attributable to the intervention rather than solely to practice effects or measurement artifacts.
Although the MMSE was designed as a screening tool, numerous studies have repurposed it as an outcome measure to detect cognitive change after short-term interventions. Its brevity and familiarity have made it a convenient way to track cognitive status before and after a therapeutic program. In fact, the MMSE is often administered at baseline and at discharge in geriatric and neurorehabilitation settings to document cognitive progress (Stern et al., 1994). Many clinical trials and rehabilitation studies explicitly use MMSE change scores as a primary outcome. For example, a large intervention study in patients with dementia who were treated with 2–4 wk of cognitive therapy reported modest but significant MMSE improvements postintervention, and the authors used the MMSE change as the primary metric of cognitive outcome (Jo et al., 2018). Similarly, in a short-term music-based rehabilitation trial for older adults, researchers administered the MMSE before and after the 2-wk intervention to quantify overall cognitive change, observing a significant increase in MMSE scores in the treatment group (Shinada et al., 2025). Research consistently shows that the MMSE, although initially a screening instrument, is effectively applied to detect cognitive changes during brief rehabilitation periods. In this study, the MMSE was similarly used to assess short-term cognitive improvements after a 2-wk TOCT intervention in older adults. Given the intervention’s intensive daily structure and its high feasibility, it was reasonable to anticipate observable cognitive gains. The observed improvements, particularly in the face-to-face and telerehabilitation groups, corroborate prior findings and underscore the MMSE’s responsiveness under structured, high- frequency rehabilitation protocols.
The dropout rates in the face-to-face group highlight the vulnerability of older adults to social factors, with reasons including social anxiety and time constraints. Future interventions should be more flexible to fit daily routines. Research supports that social support enhances mental well-being and reduces dropout rates (Hanevik et al., 2023; Upasen et al., 2024). Adapting TOCT to foster social connectedness may improve retention, whereas flexible programs can better accommodate those with social anxiety. These studies emphasize components that can be meaningfully integrated into the TOCT framework. Qadir et al. (2022) highlighted the role of psychoeducational approaches in reducing anxiety through personalized and knowledge-based support, which aligns with TOCT’s emphasis on person-centered task adaptation and cognitive–motor engagement (Qadir et al., 2022). Similarly, Keller et al. (2021) demonstrated that incorporating digital training tools into rehabilitation improved patient satisfaction and reduced dropout rates (Keller et al., 2021). These findings suggest that combining psychoeducation and digital elements with task-oriented circuit models can enhance engagement and address emotional or motivational barriers that may limit participation in structured motor–cognitive interventions. Recruitment and retention rates exceeding 90% were achieved in the 2-wk occupational therapy program with older adults. The accessibility and convenience of the program, which likely reduced or eliminated transportation barriers, along with its duration of 2 wk, may have influenced the high participation rates among the older adults (Bourdeau et al., 2008; Maresova et al., 2023).
Dependence on the technical infrastructure in the telerehabilitation group is a notable challenge, with some participants dropping out for reasons such as connection issues and difficulties using the device. Some psychological aspects of telerehabilitation may be a barrier for the older adults while they engage in TOCT programs. Therefore, many older adults have doubts about the efficiency of remote rehabilitation compared with one-on-one sessions, leading them to a passive position in telerehabilitation programs (Buabbas et al., 2022). Designing a telerehabilitation program that aligns with the needs and skills of the older adults can play a crucial role in boosting their commitment and adherence to the program.
Home-based TOCT offers flexibility but has high dropout rates because of self-regulation challenges, environmental distractions, and lack of motivation. Many older adults struggle with self-regulation, leading to poor adherence. Distractions in nursing homes and nonclinical settings further reduce concentration and commitment, resulting in intermittent participation (Narsakka et al., 2022). Additionally, the absence of therapist supervision and direct encouragement in home-based programs contributes to lower motivation and higher dropout rates (Farragher & Jassal, 2012; Sommer et al., 2022; Zhang et al., 2023). Developing multiple support systems, including family involvement and regular check-ins with health care providers, can increase adherence to home-based TOCT programs.
The results of the study highlight clear benefits for each delivery method within TOCT programs, particularly in improving cognitive and motor function among older adults. The face-to-face group showed the largest effect sizes, particularly on the MMSE, suggesting that face-to-face interactions can provide essential support and motivation and improve cognitive outcomes. This finding is consistent with those of other studies that emphasize the importance of therapeutic alliances in face-to-face interventions, known to promote better patient engagement and compliance (Heredia-Callejón et al., 2023; Kinney et al., 2020). As for the telerehabilitation group, there were improvements in both the SF–36 Energy/Vitality and Social Functioning subscales, suggesting that remote delivery of TOCT can effectively improve quality-of-life indicators, particularly when physical accessibility is a challenge. Previous studies similarly indicate that telerehabilitation interventions can enhance vitality and social participation among older adults, providing a viable alternative to conventional rehabilitation methods when direct access is limited (Man et al., 2024; Velayati et al., 2020). In terms of the same subscales, the moderate within-group effect sizes between the telerehabilitation and home-based groups, however, suggest that telerehabilitation may be a viable alternative to face-to-face settings, particularly in scenarios where direct physical interaction is limited. In contrast, the home-based TOCT program showed less effects; we found within-group improvements only for the nondominant hand on the NHPT. These findings suggest that, although home-based programs offer flexibility, the absence of structured supervision and external motivation may limit their effectiveness, as highlighted by previous research on the challenges of self-directed rehabilitation adherence in older adults. Future implementations of TOCT could consider hybrid models that incorporate regular check-ins or motivational support to address the limitations observed in home-based programs. Accordingly, future trials should test a modular hybrid intervention that deliberately blends the strengths of each delivery mode—initial face-to-face skill acquisition, synchronous telerehabilitation follow-up, and structured home practice—to maximize individualization, adherence, and ecological validity.
This study has several limitations. The first limitation is the lack of detailed demographic and clinical information about the participants, which may limit the applicability of the findings for practitioners seeking to determine the intervention’s relevance to their specific client populations. The second limitation is the absence of a usual-care control group, which restricts our ability to compare the intervention’s effects with standard care practices and may affect the interpretation of the intervention’s true efficacy. Third, although validated outcome measures such as the MMSE, MoCA, NHPT, and SF–36 were used, each has inherent measurement limitations, including potential ceiling effects and varying sensitivity to short-term changes in cognitive and motor functions among older adults. Additionally, participant-related factors such as daily mood fluctuations, motivation levels, and varying levels of staff support may have influenced performance independently of the intervention. Finally, the same versions of the assessment tools were used at both pre- and posttest stages, introducing the possibility of learning effects, wherein familiarity with the test format could have artificially inflated posttest scores. These factors should be considered when interpreting the observed improvements.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: TOCT improves cognitive and motor functions in older adults, with significant gains in motor skills and social functioning (MMSE, MoCA, NHPT). The face-to-face and telerehabilitation methods were effective, whereas home-based programs showed limited improvements. The findings support the need for intensive, tailored rehabilitation programs, particularly in face-to-face and telerehabilitation formats, to optimize care for older adults in nursing homes.
Conclusion
The present study highlights important considerations for tailoring TOCT interventions, such as the need for structured support systems in home-based programs and addressing technological infrastructure in telerehabilitation. We encourage researchers in future large-scale studies to explore these methods further, with a focus on optimizing intervention adherence and assessing the long-term impact on the quality of life of older adults. Future studies should include implementing graded tasks in TOCT programs to investigate the impact of personalized progressions on participant outcomes.
Footnotes
Acknowledgments
This research was supported by the X Project and was registered with ClinicalTrials.gov (NCT06417073) on May 13, 2024. The study protocol was reviewed and approved by the Çankırı Karatekin University Health Sciences Ethics Committee (d897232bb89442f7).