
Abstract
This review included research articles addressing what is known about the impact of pediatric acute-onset neuropsychiatric syndrome (PANS) on children’s daily functioning and the role of occupational therapy in managing challenges.
Pediatric acute-onset neuropsychiatric syndrome (PANS) is a neuroimmune condition marked by the sudden onset of obsessive–compulsive disorder (OCD), severely restricted food intake, or both, alongside at least two additional neuropsychiatric or somatic symptoms, such as developmental regression, sensory or motor abnormalities, school performance decline, sleep disturbances, enuresis, and anxiety (American Academy of Pediatrics [AAP], 2025; Chang et al., 2015; Swedo et al., 2012). Symptoms typically escalate rapidly, reaching peak severity within 24 to 48 hr (Swedo et al., 2012). Although PANDAS, a subset of PANS, is characterized by symptom exacerbations following streptococcal infections, PANS encompasses a broader range of potential triggers, including not only streptococcal infections but also other infections, as well as environmental and metabolic factors (Swedo et al., 2012). Prevalence data are limited, but clinical cohort studies reveal significant comorbidity, with 52% of children in an eating disorder clinic, 11% with tic disorders, and 5% in an OCD clinic meeting PANS criteria (Aman et al., 2022; Jaspers-Fayer et al., 2017; Singer et al., 2000). PANS typically follows a relapsing–remitting course, with periods of acute exacerbation and partial or full remission, although some cases persist in chronic or progressively worsening forms, complicating management (Frankovich et al., 2017; Gromark et al., 2022). The condition significantly disrupts children’s functioning across home, school, and social environments, creating widespread challenges (Calaprice et al., 2017; Chang et al., 2015; Newby et al., 2024a; 2024b; Tona et al., 2017).
The PANS Research Consortium treatment guidelines outline three pillars of intervention: managing neuroinflammation and autoimmunity, treating underlying infections, and addressing psychiatric and behavioral symptoms (Cooperstock et al., 2017; Frankovich et al., 2017; Thienemann et al., 2017). Interventions for neuroinflammation and autoimmunity include corticosteroids, intravenous immunoglobulin, and other anti-inflammatory treatments to reduce symptom severity (Frankovich et al., 2017). Treating underlying infections involves antimicrobial therapies targeting pathogens that may trigger symptoms (Cooperstock et al., 2017). The psychiatric and behavioral intervention pillar takes a multimodal approach, incorporating cognitive–behavioral therapy (CBT) for obsessive-compulsive behaviors and severe anxiety, psychoactive medications for symptom management, and psychoeducation for families. Environmental modifications, such as sensory-friendly spaces, workload adjustments, and school accommodations, are also recommended (Thienemann et al., 2017).
Despite their comprehensive nature, these guidelines do not explicitly address the impact of PANS on occupational performance or include occupation-based interventions as a distinct pillar. Recent guidance from the AAP (2025) highlights function-based interventions, including occupational therapy, as a key aspect of psychiatric care within a multimodal treatment approach. In this context, function-based and occupation-based interventions are used interchangeably, both focusing on improving a child’s ability to participate in meaningful daily activities. The AAP recommends early implementation of function-based interventions, with specific guidance for addressing occupations such as sleep disturbances and food restriction (AAP, 2025). Although these recommendations represent progress, they lack comprehensive guidance for addressing broader occupational challenges, such as daily activities beyond sleep and eating, school participation, play, and social interactions. Evidence consistently shows that PANS significantly disrupts children’s engagement in these occupations, which are critical for development and well-being (Calaprice et al., 2017; Chang et al., 2015; Newby et al., 2024a; Tona et al., 2017).
When children struggle to engage meaningfully in daily occupations, they may experience reduced self-efficacy, disrupted habit formation, and declining motivation and health (Case-Smith, 2014; Feldhacker et al., 2018; Taylor, 2023). These disruptions are not limited to immediate effects and can influence occupational engagement over the life course (Feldhacker et al., 2018; Taylor, 2023). Occupational therapists play a key role in mitigating these challenges by assessing the dynamic interaction between the child, their environment, and occupational demands. They identify barriers and develop tailored interventions to address performance gaps (Case-Smith, 2014; Hinojosa & Segal, 2012), helping children achieve a better fit between their abilities and daily activities and promoting overall well-being.
For children with PANS, these principles are especially relevant. The fluctuating nature of PANS, with cycles of exacerbation and remission, creates unique occupational challenges (Tona & Posner, 2011). Exacerbations can severely disrupt school, self-care, play, and social participation (Calaprice et al., 2017; Chang et al., 2015; Newby et al., 2024a; Tona et al., 2017), and residual difficulties may persist even in remission (Frankovich et al., 2017; Gromark et al., 2022). Occupational therapists are uniquely positioned to help children navigate these fluctuating impacts on daily life. However, more research is needed to understand the specific effects of PANS on occupational performance, develop appropriate assessments, and design targeted interventions. Addressing these gaps will strengthen occupational therapy’s role in improving quality of life and developmental outcomes for these children.
Although individual studies offer insights into PANS-related occupational challenges, a comprehensive synthesis is lacking. By bringing together the existing research, we can identify key patterns, highlight gaps, and uncover opportunities for future studies, ultimately providing a clearer framework for understanding the specific challenges of this population. These gaps in understanding, particularly regarding how occupational performance challenges are identified, measured, and addressed, underscore the need for further investigation. In this scoping review, we addressed these gaps through the overarching question: What is known about occupational performance for children with PANS? To explore this, our study was guided by three subquestions targeting occupational performance challenges and how they are identified, and the occupational therapy interventions used with this population: What is known about occupational performance challenges experienced by children with PANS? How are data regarding occupational performance of children with PANS being collected? What is currently known about the use of occupational therapy interventions for children with PANS?
Mapping what is currently known and identifying gaps will not only clarify the evidence base but also guide future research toward the most pertinent areas. This, in turn, will highlight occupational performance as a critical and foundational aspect of the multidisciplinary approach supporting these children. By focusing on improving occupational performance, it is anticipated that children with PANS will experience enhanced participation in daily routines and activities across home, school, and community environments.
Method
Our methods followed the Arksey and O’Malley (2005) framework and its five-stage reporting process: (1) formulating the research question, (2) identifying the relevant literature, (3) selecting studies, (4) charting the data, and (5) synthesizing and reporting the results. We also adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA–ScR) checklist (Tricco et al., 2018) for clear reporting.
Stage 1: Formulating the Research Question
This review explored the current available research regarding occupational performance of children with PANS. Three subquestions guided the analysis focusing on commonly reported areas of occupational performance, tools and assessments used for evaluation, and the application of occupational therapy interventions with this population. These questions structured the review and ensured a thorough examination of the evidence.
Stage 2: Identifying the Relevant Literature
We searched seven databases: MEDLINE, CINAHL, Cochrane Library, PsycINFO, SCOPUS, ERIC, and EMBASE, focusing on concept, target population, and occupational performance outcomes as per Levac et al. (2010). (For the CINAHL search strategy, see Table A.1 in the Supplemental Material, available online with this article at https://research.aota.org/ajot.) To capture all historical terms for PANS, we included related diagnoses, such as childhood acute neuropsychiatric syndrome and pediatric infection-triggered autoimmune neuropsychiatric disorders, as suggested by Sigra et al. (2018). The age range was limited to birth through 18 yr. Occupational performance was defined by using the domains of the Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020), which outlines occupations, contexts, performance patterns, skills, and client factors. These domains informed the search terms. Inclusion criteria required peer-reviewed, English-language studies on PANS, PANDAS, and related conditions among children, addressing occupational performance outcomes within OTPF–4 domains.
Stage 3: Selecting Studies
The selection process had two phases: (1) screening titles and abstracts for relevance and (2) reviewing full-text articles to confirm eligibility. Reference lists of retained studies were also hand-searched. Articles were excluded if they did not address occupational performance, were unrelated to PANS, or did not meet the inclusion criteria. Studies did not need to address all three subquestions to be included; eligibility required that a study address at least one. This broader inclusion strategy allowed for a more comprehensive mapping of the literature across these interrelated areas. The PRISMA–ScR flow diagram (Figure 1) outlines the number of sources screened, included, and excluded. Screening was conducted in Covidence, with two authors independently reviewing all titles and abstracts (Michelle J. Newby, Kirsti Haracz) and full texts (Newby, Shelly J. Lane, Haracz, or Janice Tona, with Newby screening all articles). Disagreements were resolved through discussion to ensure accuracy.
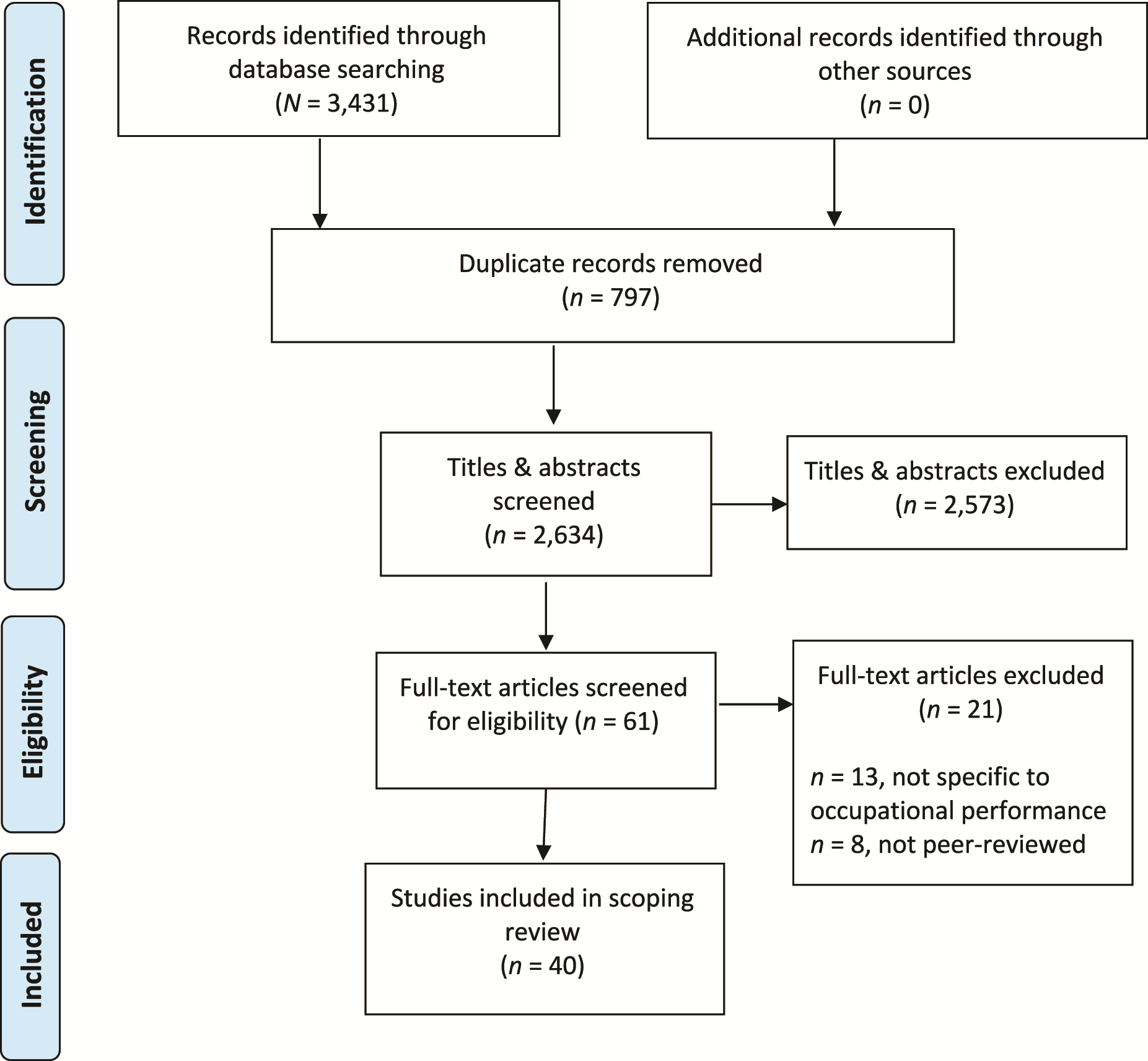
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) flow of study selection process. Note. Format from Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., … Straus, S. E. (2018). PRISMA extension for Scoping Reviews (PRISMA–ScR): Checklist and explanation. Annals of Internal Medicine, 169, 467–473. https://doi.org/10.7326/M18-0850.
Stage 4: Charting the Data
Using Covidence for data extraction ensured a systematic and organized approach. We developed a data extraction template to capture key information, including article details (title, lead author, year, country), study design, and participant characteristics. The extraction template was piloted with four articles, with Newby and Haracz independently extracting data, comparing results, and resolving discrepancies to ensure accuracy. Data fields included assessment tools related to occupational performance, study findings categorized by functional domains, and intervention details. Additional contextual factors, such as environmental influences, habits, and routines, were also recorded. Newby extracted data from all included articles.
Stage 5: Synthesis and Reporting the Results
In the final stage, we synthesized the data to provide a comprehensive overview of occupational performance of children with PANS. Synthesis was structured around three key themes: occupational performance challenges, assessment methods, and occupational therapy interventions. Findings were organized into tables for clarity and systematic presentation.
Results
The initial search strategy identified 3,431 records (Figure 1). After removing 797 duplicates, we screened 2,634 titles and abstracts, resulting in 61 full-text articles assessed for eligibility. Of these, 21 were excluded with reasons specified in Figure 1. Ultimately, 40 studies met all the inclusion criteria and were included in the scoping review. Hand searching yielded no additional articles.
Table A.2 in the Supplemental Material lists and characterizes the included studies. Of the 40 studies, 2.5% (n = 1) focused exclusively on occupational performance, examining multiple domains such as activities of daily living (ADLs), play, school participation, and social engagement (Tona et al., 2017). An additional 22.5% (n = 9) explored specific occupational performance domains, including sleep (Estivill-Domènech et al., 2024; Gaughan et al., 2016; Santoro et al., 2018), school participation (Doran & O’Hanlon, 2019), communication (Prosell et al., 2022), and eating (Biswas et al., 2022; Calkin & Carandang, 2007; Sokol & Gray, 1997; Toufexis et al., 2015). The remaining 75% (n = 30) did not directly address occupational performance as a primary focus but provided insights into functional impacts through broader participant characteristics.
What Is Known About Occupational Performance Challenges Experienced by Children With PANS?
To explore the occupational performance challenges experienced by children with PANS, we analyzed occupations, contexts, performance patterns, performance skills, and client factors by using the OTPF–4. Table A.3 summarizes the number and percentage of studies reporting on each domain, offering a snapshot of current knowledge. Data on ADLs and instrumental activities of daily living (IADLs) were collected by individual task areas rather than overall categories, allowing for a more detailed account of the specific occupational challenges reported. Challenges with ADLs were reported across 13 studies (Bernstein et al., 2010; Biswas et al., 2022; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Calkin & Carandang, 2007; Colvin et al., 2021; Cross et al., 2021; Demchick et al., 2019; Miglioretti et al., 2024; Santoro et al., 2018; Spartz et al., 2017; Tona et al., 2017; Toufexis et al., 2015), with toileting identified in seven studies (Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Calkin & Carandang, 2007; Colvin et al., 2021; Miglioretti et al., 2024; Spartz et al., 2017; Tona et al., 2017) and personal hygiene and eating/feeding noted in three studies each (Biswas et al., 2022; Santoro et al., 2018; Spartz et al., 2017; Tona et al., 2017; Toufexis et al., 2015).
IADLs were reported more broadly in 22 studies (Bernstein et al., 2010; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Demchick et al., 2019; Dolce et al., 2022; Doran & O’Hanlon, 2019; Estivill-Domènech et al., 2024; Gagliano et al., 2020; Gamucci et al., 2019; Gaughan et al., 2016; Hesselmark & Bejerot, 2019; Miglioretti et al., 2024; M. L. Murphy & Pichichero, 2002; T. K. Murphy et al., 2015; Santoro et al., 2018; Shimasaki et al., 2020; Sorensen et al., 2020; Spartz et al., 2017; Swedo et al., 1998; Tang et al., 2021; Tona et al., 2017; Toufexis et al., 2015), with communication management emerging as the most prominent concern, reported in all 22 studies. Beyond ADLs and IADLs, education was reported as a significant challenge across 24 studies, reflecting difficulties such as school participation, academic performance, and interactions within educational environments (Bernstein et al., 2010; Biswas et al., 2022; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Colvin et al., 2021; Cross et al., 2021; Demchick et al., 2019; Dolce et al., 2022; Doran & O’Hanlon, 2019; Frankovich et al., 2015; Gagliano et al., 2021; Gamucci et al., 2019; Gao et al., 2022; Gromark et al., 2019; Hesselmark & Bejerot, 2019; Miglioretti et al., 2024; T. K. Murphy et al., 2015; O’Dor et al., 2022; Rea et al., 2021; Santoro et al., 2018; Spartz et al., 2017; Srivastava et al., 2011; Swedo et al., 1998; Tona et al., 2017). Health management (n = 23) and rest/sleep (n = 22) were also common concerns (Bernstein et al., 2010; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Colvin et al., 2021; Cross et al., 2021; Demchick et al., 2019; Doran & O’Hanlon, 2019; Estivill-Domènech et al., 2024; Frankovich et al., 2015; Gagliano et al., 2020; Gagliano et al., 2021; Gao et al., 2022; Gaughan et al., 2016; Gromark et al., 2019; Gromark et al., 2022; Miglioretti et al., 2024; T. K. Murphy et al., 2015; Rea et al., 2021; Shimasaki et al., 2020; Sokol & Gray, 1997; Sorensen et al., 2020; Spartz et al., 2017; Srivastava et al., 2011; Tang et al., 2021; Tona et al., 2017; Toufexis et al., 2015). Social participation was discussed in 15 studies (Bernstein et al., 2010; Biswas et al., 2022; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Demchick et al., 2019; Dolce et al., 2022; Doran & O’Hanlon, 2019; Estivill-Domènech et al., 2024; Farmer et al., 2018; Gaughan et al., 2016; Miglioretti et al., 2024; M. L. Murphy & Pichichero, 2002; T. K. Murphy et al., 2015; Newby et al., 2024c; Tona et al., 2017). Only one study specifically addressed play and leisure (Tona et al., 2017).
Performance patterns were infrequently reported, with habits appearing in one study (Gaughan et al., 2016) and rituals in four (Calkin & Carandang, 2007; Colvin et al., 2021; Gaughan et al., 2016; Murphy & Pichichero, 2002). Performance skills, including motor skills (n = 12; Calaprice-Whitty et al., 2023; Colvin et al., 2021; Dolce et al., 2022; Doran & O’Hanlon, 2019; Gamucci et al., 2019; Miglioretti et al., 2024; Newby et al., 2024c; O’Dor et al., 2022; Sorensen et al., 2020; Tang et al., 2021; Thorsson et al., 2023; Tona et al., 2017), social interaction skills (n = 15; Bernstein et al., 2010; Biswas et al., 2022; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Colvin et al., 2021; Cross et al., 2021; Doran & O’Hanlon, 2019; Frankovich et al., 2015; Gagliano et al., 2020; Gao et al., 2022; Gaughan et al., 2016; Prosell et al., 2022; Santoro et al., 2018; Sorensen et al., 2020; Tang et al., 2021), and process skills (n = 2; Colvin et al., 2021; Hirschtritt et al., 2009), were broadly reported. The body functions most frequently reported were mental functions (n = 35; Bernstein et al., 2010; Biswas et al., 2022; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Calkin & Carandang, 2007; Colvin et al., 2021; Demchick et al., 2019; Dolce et al., 2022; Doran & O’Hanlon, 2019; Estivill-Domènech et al., 2024; Frankovich et al., 2015; Gagliano et al., 2020; Gagliano et al., 2021; Gamucci et al., 2019; Gao et al., 2022; Gaughan et al., 2016; Gromark et al., 2019; Gromark et al., 2022; Hesselmark & Bejerot, 2019; Hirschtritt et al., 2009; Miglioretti et al., 2024; M. L. Murphy & Pichichero, 2002; T. K. Murphy et al., 2015; O’Dor et al., 2022; Prosell et al., 2022; Rea et al., 2021; Santoro et al., 2018; Shimasaki et al., 2020; Sokol & Gray, 1997; Sorensen et al., 2020; Spartz et al., 2017; Swedo et al., 1998; Tang et al., 2021; Tona et al., 2017; Toufexis et al., 2015), sensory functions (n = 25; Bernstein et al., 2010; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Colvin et al., 2021; Cross et al., 2021; Demchick et al., 2019; Dolce et al., 2022; Frankovich et al., 2015; Gagliano et al., 2021; Gamucci et al., 2019; Gao et al., 2022; Gaughan et al., 2016; Gromark et al., 2019; Hesselmark & Bejerot, 2019; Miglioretti et al., 2024; T. K. Murphy et al., 2015; Newby et al., 2024c; Santoro et al., 2018; Shimasaki et al., 2020; Sorensen et al. (2020); Spartz et al. (2017); Swedo et al., 1998; Tang et al., 2021; Tona et al., 2017; Toufexis et al., 2015), and neuromusculoskeletal functions (n = 29; Bernstein et al., 2010; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Colvin et al., 2021; Cross et al., 2021; Demchick et al., 2019; Dolce et al., 2022; Frankovich et al., 2015; Gagliano et al., 2020; Gamucci et al., 2019; Gao et al., 2022; Gaughan et al., 2016; Gromark et al., 2019; Gromark et al., 2022; Hesselmark & Bejerot, 2019; Miglioretti et al., 2024; M. L. Murphy & Pichichero, 2002; T. K. Murphy et al., 2015; Prosell et al., 2022; Rea et al., 2021; Santoro et al., 2018; Shimasaki et al., 2020; Sorensen et al., 2020; Spartz et al., 2017; Srivastava et al., 2011; Tang et al., 2021; Thorsson et al., 2023; Tona et al., 2017; Toufexis et al., 2015). Other functions, such as cardiovascular, immune, and respiratory functions (n = 24; Bernstein et al., 2010; Biswas et al., 2022; Calaprice et al., 2017; Calaprice-Whitty et al., 2023; Calkin & Carandang, 2007; Cross et al., 2021; Doran & O’Hanlon, 2019; Estivill-Domènech et al., 2024; Frankovich et al., 2015; Gagliano et al., 2020; Gagliano et al., 2021; Gamucci et al., 2019; Gromark et al., 2019; Gromark et al., 2022; Miglioretti et al., 2024; M. L. Murphy & Pichichero, 2002; T. K. Murphy et al., 2015; O’Dor et al., 2022; Sokol & Gray, 1997; Sorensen et al., 2020; Srivastava et al., 2011; Tang et al., 2021; Tona et al., 2017; Toufexis et al., 2015), were less frequently addressed.
How Are Data Regarding Occupational Performance of Children With PANS Being Collected?
The methods used to report occupational performance challenges varied. Most studies relied on quantitative surveys or scales, such as the Children’s Yale–Brown Obsessive Compulsive Scale (CYBOCS; Scahill et al., 1997). Only a few studies used qualitative approaches, such as caregiver interviews, to gain deeper insights into the lived experiences of children and families (Demchick et al., 2019; Dolce et al., 2022; Doran & O’Hanlon, 2019). This reliance on survey methods often led to general descriptions of difficulties, with limited exploration of the specific impacts on daily life.
Data on occupational performance and its contributing factors among children with PANS were collected by using 40 standardized assessment tools, covering various domains of the OTPF–4, with some tools applied across multiple domains and studies (Table A.4). Nonstandardized tools were excluded from the analysis to ensure a focus on tools that could be used in clinical practice.
Most of the assessments (n = 33) focused on client factors, particularly mental functions (n = 29). For example, the CYBOCS was frequently used to measure severity of obsessive-compulsive behaviors. Additional client factors assessed included neuromusculoskeletal and movement-related functions (n = 4) and sensory functions (n = 1), evaluated using tools such as the Yale Global Tic Severity Scale and the Sensory Processing Measure Home Form, respectively. Beyond client factors, four tools evaluated performance skills, targeting motor skills (n = 2), social interaction skills (n = 2), and process skills (n = 2), with the same two tools used for both motor and process skills. Measures such as the Beery–Buktenica Developmental Test of Visual–Motor Integration (Beery VMI) and the Social Responsiveness Scale were frequently used. Similarly, occupations were assessed by four tools, focusing on rest and sleep (n = 2) and education (n = 2), with key assessments including polysomnography and the Gray Oral Reading Test. Finally, four tools evaluated contexts, divided between environmental factors (n = 1) and personal factors (n = 3). Examples include the Caregiver Burden Inventory and the Child Health Questionnaire Parent Form. Some tools spanned multiple OTPF–4 levels, such as the Beery VMI, reflecting their multidimensional applications within the assessment of occupational performance.
What Is Currently Known About the Use of Occupational Therapy Interventions for Children With PANS?
No studies specifically examined occupational therapy interventions for children with PANS. Only 2 of the 40 studies in this review mentioned occupational therapy interventions. Demchick et al. (2019) briefly described an occupational therapist assisting with handwriting remediation, but a parent reported it was ineffective during symptom exacerbation. O’Dor et al. (2022) noted that 14.56% (n = 68) of their cohort had received occupational therapy in the past month, 16.92% (n = 79) had accessed it over a month ago, and 68.52% (n = 320) had never received it. However, the study did not detail the types or effectiveness of these interventions.
Discussion
We explored the impact of PANS on children’s occupational performance to address gaps in our understanding of the challenges and how they are identified, measured, and addressed. As mentioned, our research focused on three questions. Although individual studies provided insights, a comprehensive synthesis had not been conducted.
What Is Known About Occupational Performance Challenges Experienced by Children With PANS?
Our review indicated that most occupational performance domains were affected for children with PANS, although some have received more attention than others. Most studies reported challenges across a broad range of occupations, including ADLs, IADLs, communication, nutrition management, education, rest and sleep, and social participation. Education was frequently highlighted as a major area of disruption, reflecting its central role in a child’s daily life and the burden placed on caregivers when schooling is affected (e.g., Doran & O’Hanlon, 2019). Similarly, rest and sleep were commonly reported as disrupted (Santoro et al., 2018), likely because of their effects on emotional regulation, cognitive functioning, academic performance, and caregiver burden (Farmer et al., 2018; Woodfield et al., 2024). Nutrition management was another critical concern (e.g., Toufexis et al., 2015), because difficulties in this area can significantly affect health and overall well-being (Proctor et al., 2023).
Despite the widespread impact of PANS across occupations, certain areas received less attention in the literature. Although toileting was commonly discussed (e.g., Calaprice et al., 2017; Tona et al., 2017), other ADLs, such as bathing, dressing, and personal hygiene, were less frequently explored. This may be because toileting disruptions are more visible and socially disruptive, whereas other ADL challenges may be more manageable within the home environment. Play and leisure were notably overlooked, with only one study addressing them (Tona et al., 2017). This limited attention may be attributed to their relatively lower perceived impact on caregiver burden compared with challenges in education, sleep, or nutrition. Similarly, performance patterns, including habits, routines, and roles, were rarely discussed, despite their importance in maintaining stability for children experiencing fluctuating symptoms.
How Are Data Regarding Occupational Performance of Children With PANS Being Collected?
Our review highlighted the need for more occupation-focused assessments to better evaluate the impact of PANS on children’s daily lives. A top-down approach, which emphasizes understanding the child’s participation in daily routines and meaningful activities within their natural environments, is essential for a comprehensive evaluation (Case-Smith, 2014; Richardson, 2014). Coupled with an ecological perspective, this approach considers the dynamic interaction between the child and their physical, social, cultural, and economic environments, enabling the identification of barriers and supports to participation (Case-Smith, 2014; Llewellyn, 2012). Although tools such as the Canadian Occupational Performance Measure, Child and Adolescent Scale of Participation, and the Adaptive Behavior Assessment System are well suited to measure participation priorities (Bedell, 2009; Harrison & Oakland, 2015; Law et al., 2019), these assessments have not yet, to our knowledge, been used in PANS research. Instead, existing studies predominantly rely on bottom-up tools, such as the Wechsler Abbreviated Scale of Intelligence and the Beery VMI, which evaluate foundational skills like cognition and visual–motor integration but provide limited insight into how potential deficits affect occupational performance (Beery & Beery, 2010; Wechsler, 2011). Although bottom-up tools are valuable for understanding performance limitations, they do not address the broader contexts critical for occupation-focused interventions.
Given the episodic and often rapidly fluctuating nature of PANS (Chang et al., 2015; Swedo et al., 2012), assessments should be conducted frequently and interpreted with caution, because a child’s occupational performance can shift significantly over short periods (Newby et al., 2024a). This variability is a distinguishing feature of PANS and must inform both assessment and intervention planning. In addition, occupational therapists may be among the first professionals to observe sudden, unexplained changes in a child’s occupational performance and should therefore be prepared to recommend medical evaluation when such changes are noted. Raising awareness of these fluctuations can support earlier identification and more coordinated care.
What Is Currently Known About the Use of Occupational Therapy Interventions for Children With PANS?
The lack of research on occupational therapy interventions for children with PANS highlights the urgent need for occupation-based approaches that prioritize meaningful engagement in daily activities. Of the 40 studies reviewed, only 2 studies mentioned occupational therapy, with neither detailing intervention strategies or effectiveness (Demchick et al., 2019; O’Dor et al., 2022). Although occupational therapists focus on the interplay between the child, environment, and daily activities, this evidence gap limits our understanding of occupational therapy’s role in supporting children with PANS (Case-Smith, 2014; Richardson, 2014). Given identified challenges in self-care, education, social participation, and sleep, occupational therapy can provide essential strategies to promote engagement, adapt routines, and build resilience (Calaprice et al., 2017; Chang et al., 2015; Newby et al., 2024a; Tona et al., 2017).
Occupational Performance—The Fourth Pillar?
Our review highlights the need to assess occupational performance and expand treatment guidelines to explicitly address occupational participation of children with PANS. Current guidelines provide limited guidance on interventions that support meaningful engagement in daily life beyond sleep and food restriction (AAP, 2025; Cooperstock et al., 2017; Frankovich et al., 2017; Thienemann et al., 2017). However, as outlined in the literature and synthesized in this review, children with PANS experience widespread disruptions across multiple occupations, including self-care, education, sleep, social participation, and play (Calaprice et al., 2017; Chang et al., 2015; Newby et al., 2024a; Tona et al., 2017). Despite these significant occupational challenges, there is no standardized framework for assessing or addressing occupational performance in this group of children, which creates a substantial gap in care.
Given the fluctuating and complex nature of PANS, interventions must extend beyond symptom management to actively support participation in meaningful occupations (Newby et al., 2024a; Tona & Posner, 2011). Treatment guidelines should integrate evidence-based strategies that promote function, engagement, and participation across daily activities, ensuring a more holistic approach to care. Occupational performance should be established as a fourth pillar of intervention for children with PANS, alongside managing neuroinflammation, treating infections, and addressing psychiatric symptoms (AAP, 2025; Cooperstock et al., 2017; Frankovich et al., 2017; Thienemann et al., 2017). Occupational therapists play a critical role in multidisciplinary teams, providing the necessary supports to enhance children’s engagement in daily occupations and improve overall well-being (AOTA, 2020; Case-Smith, 2014; Feldhacker et al., 2018). Expanding intervention frameworks to emphasize occupational performance will ensure a more comprehensive, child-centered approach, ultimately improving long-term outcomes and quality of life for children with PANS.
Future Research
Future research should use occupation-focused, top-down approaches coupled with bottom-up assessments to fully capture the daily participation and performance challenges experienced by children with PANS. Although tools such as the Canadian Occupational Performance Measure (Law et al., 2019) exist, current studies rely on bottom-up measures that assess skills but overlook broader occupational engagement.
The significant impact of PANS on occupational performance highlights the need for targeted occupational therapy interventions beyond symptom management. Research should document and evaluate occupational therapy strategies across core activities (ADLs, IADLs) and broader occupations (play, leisure) to strengthen evidence-based practice. Examining interventions such as environmental modifications, goal-directed training, sensory-based strategies, and caregiver education, which have been proven effective in other pediatric conditions (Case-Smith, 2014; Lane, 2012; Novak & Honan, 2019), will support occupational therapy integration into multidisciplinary care. Standardizing protocols and outcome measures will ensure consistent, high-quality support that prioritizes participation.
Limitations
This scoping review had several limitations. First, it was limited to peer-reviewed literature published in English within the identified databases, which may have excluded relevant studies in other languages or nonindexed sources. Restricting the review to peer-reviewed publications may have omitted valuable insights from gray literature, such as reports and conference proceedings, that could have enriched the findings.
Second, although the OTPF–4 domain areas guided aspects of the content analysis, the process components of the OTPF–4 were not systematically applied. This may have limited the depth of analysis related to assessment and intervention practices. Third, although the included studies involved children of varying ages and genders, this review did not examine age- or gender-specific differences in occupational performance. As such, any potential influence of these factors remains unexplored within the current review and should be considered in future studies.
Finally, as is true of scoping reviews, we did not appraise included studies for methodological quality or strength of evidence. All included studies were given equal weight during synthesis, despite variability in research design, sample size, and rigor. This may limit the generalizability and interpretability of some findings.
Implications for Occupational Therapy Practice
This review highlights the following implications for occupational therapy practice: Addressing occupational challenges: Occupational therapists play a critical role in supporting children with PANS experiencing challenges with occupational performance. Using occupation-based tools: Using occupation-based assessments provides a holistic view of the child’s abilities and ensures that interventions align with the child’s and family’s priorities. Integrating occupational performance in multidisciplinary care: Occupational performance is a key aspect of multidisciplinary care of PANS, with occupational therapy offering expertise in capacity building, task modification, environmental adaptation, and family-centered support to improve functional outcomes and quality of life.
Conclusion
Our findings underscore the profound impact of PANS on children’s occupational performance. At the same time, they reveal critical gaps in the evidence base, most notably, a paucity of clearly defined occupational therapy interventions and a lack of systematic application of occupation-based assessments for this population. To address these gaps, we recommend prioritizing occupation-focused assessments that identify participation challenges and inform tailored interventions. Effective assessment is essential for understanding the impact of PANS on daily life and integrating occupational performance into multidisciplinary care. This foundation will support the development of occupation-based interventions, and thereby promote meaningful participation, improve quality of life, and ultimately strengthen the role of occupational therapy for this underserved population.
Supplemental Material
Supplementary material for Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS) and Occupational Performance: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2025.051238.pdf for Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS) and Occupational Performance: A Scoping Review by Michelle J. Newby, Kirsti Haracz, Shelly J. Lane and Janice Tona in The American Journal of Occupational Therapy
Footnotes
*Indicates articles included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.