
Abstract
The study findings highlight the need for education programs, social support, and culturally sensitive occupational therapy interventions to help refugees regain balance in their daily lives.
Forced displacement remains a global crisis, with approximately 122.6 million people forcibly displaced as of 2023 (Fabianek et al., 2023; United Nations High Commissioner for Refugees [UNHCR], 2024). One of the largest mass migrations in history is the displacement of Syrian refugees. With 3.6 million refugees, Turkey hosts about 10% of the world’s displaced population and remains the leading refugee-hosting country (UNHCR, 2023). As of early 2025, Turkey accommodates 4,171,000 registered refugees, including 2,814,402 Syrians under temporary protection (Republic of Turkey Ministry of Interior Directorate General of Migration Management, 2025).
Forcibly displaced people often experience deprivation of meaningful occupations, leading to disrupted daily activities and diminished well-being (Thornton & Spalding, 2018). Many endure trauma from persecution and conflict, further exacerbated by prolonged loss of structured, purposeful engagement (Nilsson et al., 2019). Refugees constitute one of the most disadvantaged groups regarding occupational participation because of cumulative barriers such as forced displacement, trauma, lack of legal work status, language barriers, and limited access to education and health care. Compared with native-born populations or even voluntary migrants, refugees often face more severe and multidimensional restrictions that hinder their ability to engage in meaningful occupations (Altuntaş et al., 2021; Mirza, 2012). Research highlights the positive effects of occupational engagement on health and well-being (Bar & Jarus, 2015), yet refugees face substantial barriers to occupational performance, including access to housing, health care, education, and social integration (Altuntaş et al., 2021). Occupational balance (OB)—the equilibrium between necessary, desired, and enjoyable activities—is essential for well-being (Backman, 2004), yet it is frequently disrupted among refugee populations because of economic hardship, language barriers, limited social support, and psychological distress (Yazdani et al., 2018).
After the onset of the Syrian Civil War in March 2011, over 13 million Syrians were forcibly displaced, both internally and across borders. Turkey became the primary host country because of its geographic proximity and open-door policy in the early years of the conflict. Many Syrian refugees fled with minimal belongings, experiencing multiple traumas, including loss of home, family separation, and long-term uncertainty. Unlike shorter term displacement crises, the protracted nature of the Syrian conflict—now spanning over a decade—has deepened the complexity of integration, social participation, and daily functioning for these people (Murakami & Akilova, 2023).
Social determinants, shaped by economic, cultural, and societal factors, significantly influence refugees’ participation in meaningful occupations (Huot et al., 2021). Social determinants influence lifelong experiences related to health, education, social interaction, and economic well-being (Chang, 2019; Hynie, 2018b; Rami et al., 2023). According to the World Health Organization (WHO), social determinants may have a greater impact on health and well-being than biological factors (WHO Regional Office for South-East Asia, 2008).
Key social determinants for refugees include ethnicity, education, gender, income, family structure, social support, and the host region’s socioeconomic development (Doğan et al., 2024). For instance, lower education levels limit economic opportunities, increasing the risk of unemployment and poverty, which restricts participation in meaningful activities (Li & Wu, 2022). Similarly, gender norms often hinder female refugees’ labor market integration, reinforcing caregiving roles and occupational imbalance (Al-Hamad et al., 2024). Language proficiency is another critical factor, with limited fluency increasing social isolation and reducing opportunities in education and employment (Nguyen et al., 2024).
Understanding the social determinants that influence OB among refugees is essential for protecting their health and well-being (Bennett et al., 2012; Rami et al., 2023). In this context, identifying the social factors that affect the OB of Syrian refugees is of great significance (Yazici & Akyurek, 2025). On the basis of this premise, in this study, we sought to answer the research question: How do social factors, either independently or in combination, influence the OB of refugees? In this study, conducted in the context of Turkey, we aimed to provide insight into the social integration processes of refugees in developing countries. Furthermore, it is expected to contribute to the development of social policies for refugees and inform occupational therapy intervention programs aimed at improving their quality of life.
Method
Ethical approval for this study was obtained from the Uskudar University Non-Interventional Clinical Research Ethics Committee (Approval ID 61351342/020–888). Informed consent was obtained from all participants who agreed to participate, and ethical guidelines were strictly followed throughout the study. Participants were informed that their responses would remain confidential, and they retained the right to withdraw at any time.
Study Design
This study used a cross-sectional design, with a direct survey approach to examine the relationship between OB and social factors among Syrian refugees. The survey included questions regarding information that could be considered sensitive or confidential. The direct survey method was chosen to minimize nonresponse bias, ensuring that people with lower socioeconomic status or similar characteristics that might influence study participation were adequately represented (Maitland et al., 2017).
Participants
We conducted an a priori power analysis using G*Power (Version 3.1) to determine the minimum sample size required to detect a moderate effect size (f 2 = 0.15) in a multiple linear regression. The statistical parameters were set as follows: α = .05, desired power = .80. On the basis of these parameters, the minimum required sample size was calculated to be 112 participants.
The study was conducted with 420 Syrian refugees residing in four different provinces of Turkey—Istanbul, Ankara, Elazig, and Bingol—which were selected because of their diverse living conditions and socioeconomic dynamics. The inclusion criteria included age 18 yr or older, being a Syrian citizen, and having migrated to Turkey after the outbreak of the Syrian Civil War in March 2011. Exclusion criteria included having sufficient proficiency in understanding and speaking Turkish (n = 16) and having a cognitive impairment that would prevent comprehension of the survey questions (n = 4).
A total of 400 Syrian refugees were included in the final analysis. A post hoc power analysis indicated that the achieved power was 92.4%, demonstrating that the study had sufficient statistical power and that the findings were reliable.
Data Collection and Assessments
Before data collection, participants were provided with detailed information about the study. Explanations were given as needed, and informed consent was obtained from all volunteers. The data collection process involved administering a sociodemographic information form and the Turkish Occupational Balance Questionnaire–11 (OBQ11–T). Participants retained the right to withdraw from the study at any time. Data collection was conducted between December 10, 2024, and March 10, 2025.
Sociodemographic Information Form
The sociodemographic information form, developed by the researchers, was used to collect data on participants’ demographic characteristics. The form included questions regarding age, gender, marital status, place of residence, nationality, and other relevant sociodemographic factors.
OBQ11–T
The OBQ11–T measures the satisfaction of people with the quantity and diversity of their daily activities and identifies their OB status (Wagman & Håkansson, 2014). The original version consists of 14 self-report items, whereas the final validated Turkish version includes 11 items with a test–retest reliability coefficient of .922 and a Cronbach’s α of .785, confirming its reliability and validity (Günal et al., 2020). Each item is rated on a 4-point Likert scale, ranging from 0 (strongly disagree) to 3 (strongly agree). The total score ranges from 0 to 33, with higher scores indicating greater OB (Håkansson et al., 2020).
Data Analysis
We conducted all statistical analyses using Python (Version 3.8) and the Stats models library for regression modeling. The dataset was first explored through descriptive statistics, including mean, standard deviation, and minimum–maximum (min–max) values for numerical variables, as well as frequency tables for categorical variables. We used data visualization techniques, such as histograms and probability plots, to inspect the distribution of numerical variables. We assessed the normality of the data using the Kolmogorov–Smirnov and Shapiro–Wilk tests.
In the dataset, the dependent variable is OBQ11–T score, whereas the independent variables include both numerical variables (e.g., age, number of household members) and categorical variables (e.g., gender, marital status, ethnicity, education level, place of residence, city of residence). Categorical variables were encoded using the one-hot encoding (a.k.a. dummy coding) method. Reference categories were designated in the model (e.g., male for gender, single for marital status), and the remaining dummy variables were included in the analysis. Multicollinearity check was conducted using the variance inflation factor (VIF). To assess multicollinearity among predictor variables, we calculated the VIF. This step was important to ensure that the predictors were not excessively correlated, which can distort the estimation of regression coefficients and undermine the interpretability and reliability of the model (Cheng et al., 2022).
We then used a multiple linear regression model to assess the impact of selected independent variables on the OBQ11–T. Only variables that remained statistically significant (p < .05) in the regression model were retained, ensuring that the model included only relevant predictors. This approach minimized the risk of overfitting and enhanced the model’s ability to generalize findings to broader populations. We conducted all analyses to ensure robustness and accuracy. Specifically, we checked for multicollinearity using VIF values, tested for normality with the Kolmogorov-Smirnov and Shapiro-Wilk tests, and applied stepwise variable selection to minimize overfitting. In addition, we performed post hoc power analysis to confirm adequate statistical power and used min–max normalization to standardize variable scales, improving model stability. Data preprocessing, model validation, and assumption checks were systematically performed to derive reliable statistical conclusions.
Results
A total of 400 Syrian refugees participated in this study. Participants’ mean age was 38.05 yr (SD = 3.45), and the mean OBQ11–T score was 12.6 (SD = 3.43). Other sociodemographic data were summarized in Table 1.
Demographic Characteristics and OBQ11–T Scores
Note. N = 400. OBQ11–T = Turkish Occupational Balance Questionnaire–11.
We used ordinary least squares regression to fit a multiple regression model to the data. Dummy variables were generated for categorical variables during the data-processing phase. The OBQ11–T score followed a normal distribution. To prevent variables with larger ranges from disproportionately influencing the regression model, we applied min–max scaling, transforming all variables so that their maximum and minimum values corresponded to 1 and 0, respectively, with other data points adjusted accordingly.
In the initial model, all social factors were included as potential predictors of OB. This model yielded an R 2 value of .39 and an adjusted R 2 value of .24. The discrepancy between these values indicated the presence of independent variables with minimal or no effect. On the basis of the p values and model-generated coefficients, a stepwise feature selection process was applied until only significant (p < .05) predictors remained in the model.
The second regression model included gender, marital status, education level, ethnic background, and the number of people living together as independent variables to predict OB. The model was statistically significant, F(10, 389) = 21.77, p < .001; and it explained 30.5% of the variance in OBQ11–T scores (R 2 = .305). The model showed that the predicted OB score was equal to 9.673 (intercept) + 0.869 (male) − 0.542 (married) − 3.858 (illiterate) − 2.062 (primary school) − 1.087 (middle school) + 1.26 (university) + 2.478 (postgraduate) − 1.282 (Arab) − 2.022 (Kurdish) + 1.288 (Turkish or Turkoman) − 0.624 (number of people living together); values are β coefficients. The regression coefficients and their corresponding confidence intervals are presented in Table 2 and Figure 1, illustrating the impact of significant predictors on OB.
Significant Predictors of Occupational Balance
Note. N = 400. CI = confidence interval; ref. = reference.
*p < .05.
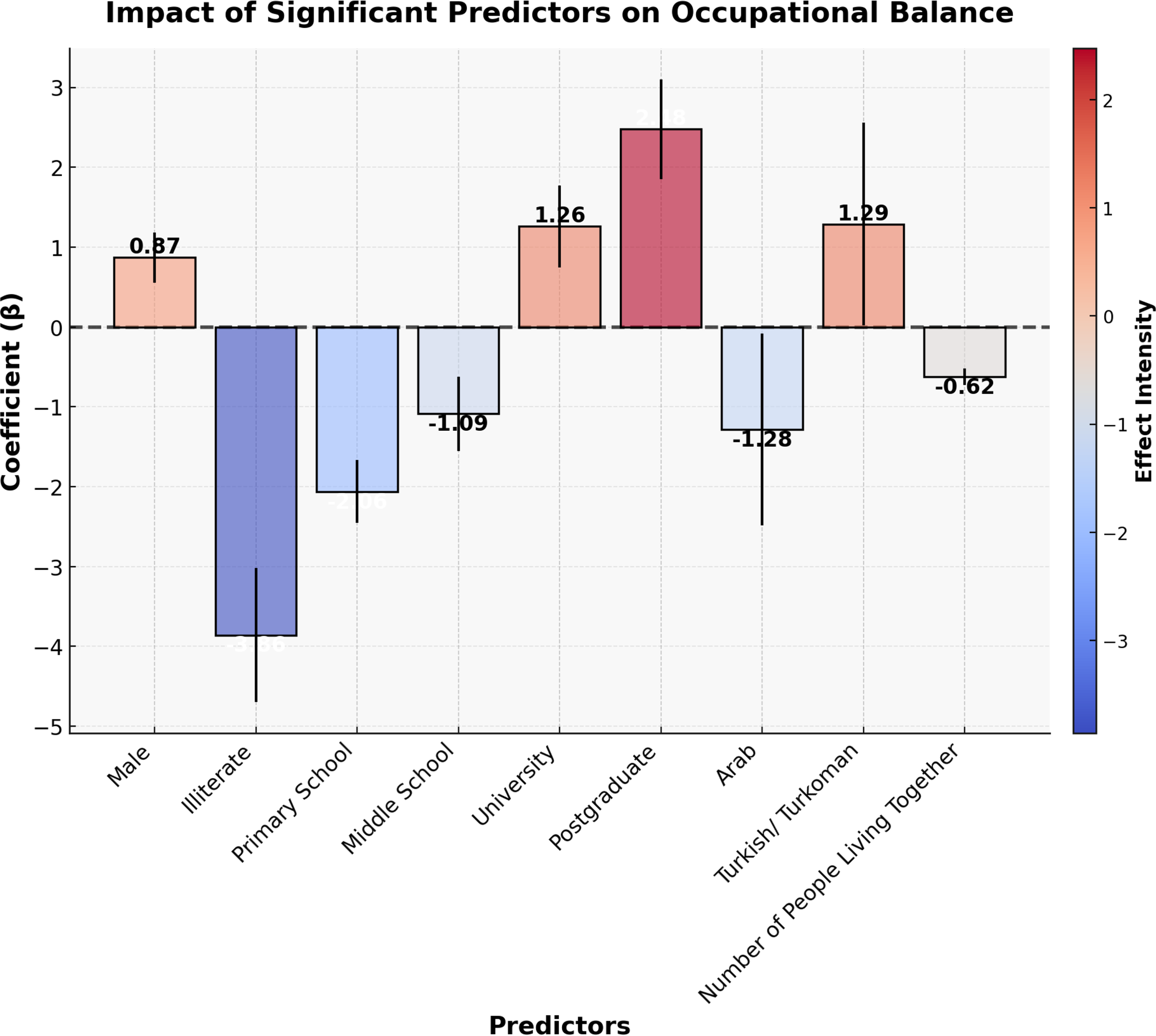
Bar chart with error-bar representation of regression coefficients for significant predictors of occupational balance.
Discussion
In this study, we aimed to identify the social factors influencing OB among Syrian refugees. The findings revealed that gender, educational level, ethnicity, and household size are significant social determinants of OB. Specifically, people with lower education levels and women were found to face greater challenges in achieving OB. Furthermore, it was observed that refugees of Arab ethnicity had significantly lower OB scores, whereas Kurdish refugees exhibited similarly low scores, although the difference was not statistically significant. This study provides a novel contribution by being among the first to examine the social determinants of OB among Syrian refugees, offering critical insights for future research and intervention development.
The study demonstrated that men had higher OB scores than women. Among Syrian refugee women, occupational participation is often influenced by a combination of cultural, religious, and socioeconomic factors. In the context of Syrian society, especially in more conservative communities, women have historically been positioned primarily in domestic and caregiving roles, with limited access to formal employment or participation in public life (Al-Hamad et al., 2024; Canefe, 2018). However, we acknowledge that the Middle East is not a monolith and that women’s roles vary widely across countries, regions, and sociopolitical settings. For instance, in some areas, including under repressive regimes, women have continued to participate in economic life and public affairs in meaningful ways.
In the case of Syrian refugees, caregiving responsibilities—particularly child care—play a central role in shaping occupational imbalance, limiting women’s participation in both social and economic activities. Language barriers and experiences of social exclusion further restrict their ability to access the labor market, contributing to lower OB (Magan & Elkhaoudi, 2024; Ozturk et al., 2019). Additionally, the concept of leisure may differ across cultural contexts. In Levantine societies, leisure is often framed as social and family-oriented activities rather than individualistic or recreational time, which is more common in Western societies. These culturally specific definitions may influence how refugee participants interpret the items on the OBQ11–T and report their sense of OB (Canefe, 2018). Given these findings, future interventions should aim to develop programs that promote refugee women’s access to education, employment, and community participation while taking into account cultural expectations and caregiving responsibilities (Al-Hamad et al., 2024).
Education emerged as one of the strongest determinants of OB. Higher education levels were associated with better OB, with postgraduate-educated people having the highest scores. Conversely, illiterate people had the lowest levels of OB. This finding aligns with previous studies indicating that education facilitates access to stable employment, enhances social integration, and improves overall well-being (Hynie, 2018a). Moreover, literacy and higher education levels are often linked to a person’s ability to adapt to new socioeconomic environments and develop self-efficacy (Nilsson & Bunar, 2016). Policymakers and occupational therapists working with refugee communities should prioritize educational initiatives that promote literacy, vocational skills, and lifelong learning opportunities.
The findings also indicate that ethnicity significantly influences OB. Refugees of Turkish or Turkoman origin had higher OB scores compared with those for other ethnic groups. This suggests that cultural and linguistic proximity plays a critical role in the integration process. Previous research has shown that migrants who settle in communities that align with their ethnic background tend to benefit more from social support mechanisms (Vaughn et al., 2017). Turkish or Turkoman refugees, in particular, do not experience language barriers and can integrate into Turkish society more quickly.
In contrast, Syrian refugees of Arab ethnicity had significantly lower OB scores, whereas Kurdish refugees also had low scores, but the difference was not statistically significant. This finding suggests that Arab and Kurdish refugees in Turkey face different socioeconomic, cultural, and linguistic challenges.
The significantly lower OB among Arab refugees can be attributed to a range of interrelated factors. Many face substantial language barriers, which hinder their ability to learn Turkish and restrict participation in the labor market and broader social life (Alnajjar & Alsaman, 2020; Doğan et al., 2019). These challenges not only limit employment opportunities but also contribute to social isolation, making integration into Turkish society more difficult. As a result, Arab refugees often reside in ethnically similar communities, which may reduce daily interaction with the host population (Gürsoy & Ertaşoğlu, 2019; Smits & Gündüz-Hoşgör, 2003). However, this pattern should not be interpreted as voluntary self-isolation. Residential clustering often emerges from a combination of shared language and cultural familiarity, as well as protective responses to marginalization or discrimination in the host society. Research indicates that attitudes toward refugees—particularly Arabs—vary widely across Turkish cities and that ethnic and religious identity can be a basis for exclusion (Gürsoy & Ertaşoğlu, 2019; Smits & Gündüz-Hoşgör, 2003). For many, living within familiar communities provides a sense of safety, support, and belonging. Additionally, past experiences of authoritarian state control in Syria may foster mistrust toward formal institutions, influencing both how refugees engage with public systems and how they choose where to live (Refai & McElwee, 2023). Therefore, their residential preferences can be more accurately viewed as a coping mechanism in response to structural and psychological barriers, rather than as resistance to integration. Previous research further supports this view, showing that refugees in ethnically homogeneous neighborhoods often experience delayed social adaptation and face greater barriers to labor market access (Fadhlia et al., 2025; Glorius et al., 2021), reinforcing the need for targeted, culturally responsive integration strategies.
Despite Kurdish refugees having similarly low OB scores, the lack of statistical significance suggests that they may have certain advantages in the integration process compared with Arab refugees. Many Kurdish refugees settle in regions with a significant Kurdish population, allowing for greater interaction with local communities and facilitating their integration. Additionally, some Kurdish refugees are bilingual, speaking both Kurdish and Turkish, which enhances their employment prospects and social networks. In contrast, Arab refugees predominantly speak only Arabic, which slows their social adaptation process (Refai et al., 2024; Refai & McElwee, 2023). Kurdish refugees may expand their social support networks more quickly, particularly in job-seeking processes. Studies have shown that strong social networks enhance refugees’ occupational participation and accelerate their adaptation (Newman et al., 2018; Niemi et al., 2019). Kurdish refugees may have greater access to social support in areas with a large Kurdish population, whereas Arab refugees tend to live more isolated from local communities.
These findings emphasize the importance of increasing interaction between refugees and local communities to support integration. Social cohesion programs should be developed to facilitate greater engagement between Arab and Kurdish refugees and the local population, ultimately improving their OB.
Additionally, household size was negatively associated with OB: As the number of people living in a household increased, OB decreased. This could be due to crowded living conditions, financial burdens, and overlapping family responsibilities, which may limit the ability of people to engage in personally meaningful activities. Similar trends have been observed in previous studies on housing conditions among refugees, where insufficient living space and high dependency ratios increased stress levels and reduced participation in daily activities (Bennett et al., 2012; Brown et al., 2024). Improving housing policies and promoting independent living arrangements may enhance OB, particularly for refugees residing in urban areas.
Various national and international initiatives have been developed to support Syrian refugees in Turkey—including access to education, vocational training, and psychosocial support—but these interventions often prioritize economic integration and basic health needs. However, few programs explicitly address OB, particularly as it relates to cultural expectations, gender norms, or meaningful leisure and social engagement. These findings have important implications for occupational therapy practice and policy development. Occupational therapists working with refugee communities should adopt a holistic approach that considers gender, education, ethnicity, and living conditions when designing intervention plans. Community-based programs that focus on skill development, social participation, and equitable access to resources can enhance the OB of refugees. Additionally, policymakers should prioritize improving refugees’ access to education, employment, and stable housing to support their long-term well-being and integration.
This study offers important insights into the social determinants influencing OB among Syrian refugees; however, it has certain limitations. Because of its cross-sectional nature, this study cannot establish causality between social determinants and OB. Future longitudinal research is needed to track changes over time and confirm the directionality of these relationships. Future studies should also incorporate variables such as time since displacement to better understand long-term adaptation patterns and occupational participation. Additionally, whereas OB scores were significantly lower among Arab refugees, the absence of a similar statistically significant trend for Kurdish refugees may be due to sample size imbalances. Future studies with larger and more representative samples, as well as diverse methodological approaches, will contribute to a more comprehensive understanding of this issue.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: ▪ Occupation-based interventions need to be developed that align with refugees’ cultural values and daily routines, ensuring meaningful engagement. ▪ Occupational therapy programs need to be designed that empower women by facilitating access to education, work, and social participation. ▪ Group-based interventions need to be implemented that strengthen social support, mentorship, and integration within the host society.
Conclusion
This study explored the social determinants influencing OB among Syrian refugees, shedding light on the multifaceted nature of occupational engagement in displaced populations. The findings indicate that gender, education level, ethnic background, and household size significantly affect OB. In particular, women, people with lower educational attainment, and those from larger households reported lower OB, suggesting that social structures and access to resources play a crucial role in shaping daily functioning and participation in meaningful activities.
By identifying key social determinants of OB, this study highlights the importance of targeted interventions that address systemic barriers to occupational participation, ultimately improving refugees’ quality of life and integration into host communities. Addressing barriers such as language proficiency, employment opportunities, and gender disparities can facilitate improved occupational participation and integration into host societies. Moreover, the study highlights the importance of social support and inclusive policies that promote equitable access to education, work, and community participation for refugee populations.
The study objectives were met, as the research successfully identified key social determinants affecting OB among Syrian refugees. However, future studies should further investigate longitudinal changes in OB and the effectiveness of intervention programs designed to enhance engagement and satisfaction in daily occupations. By addressing these factors, practitioners and policymakers can develop strategies that foster greater occupational well-being and quality of life for displaced people.
Footnotes
Acknowledgments
We sincerely thank all the participants who took part in this study. Data are available on reasonable request from the corresponding author but remain restricted because of ethical considerations, as required by the ethical committee. The study received approval from the Ethics Committee at Uskudar University Non-Invasive Clinical Investigation Ethics Committee and was also reviewed by the Ministry of Health, which confirmed its compliance with regulations (ID: 61351342/020-888). All procedures were conducted in accordance with national research standards and the ethical principles outlined in the 1964 Helsinki Declaration and its subsequent amendments.