
Abstract
Translation of knowledge about the evidence for occupational therapy interventions is critical to support the profession’s evidence base. It has become increasingly important to guide occupational therapy practice in an evidence-based, outcomes-oriented way and to identify strategies that can foster dissemination and integration of evidence into practice. In this Eleanor Clarke Slagle Lecture, Roseann C. Schaaf introduces the concept of precision occupational therapy using data-driven decision-making (DDDM) as a process to enhance practice, create evidence for occupational therapy, and foster knowledge translation. Precision occupational therapy embodies a personalized approach that respects the individual and considers multiple streams of information simultaneously to design treatments that are individually tailored and measure meaningful, personalized outcomes. It considers the individual’s strengths and needs and customizes interventions to enhance wellness and quality of life; it thus can be a guide for practice and research and can create evidence through practice. Schaaf presents three case examples to exemplify the application of precision occupational therapy using DDDM.
In this Eleanor Clarke Slagle Lecture, Roseann C. Schaaf introduces the concept of precision occupational therapy using data-driven decision-making (DDDM) as a process to enhance practice, create evidence for occupational therapy, and foster knowledge translation.
Occupational therapy is a science-based profession whose mission is to enrich the lives of individuals and society by supporting meaningful engagement in everyday activities, tasks, and occupations (American Occupational Therapy Association [AOTA], 2025). Occupational therapy serves a wide array of people and populations who are diverse in their diagnoses and their racial, ethnic, and cultural backgrounds and who lead complex, multifaceted lives. With this diversity comes the richness of occupational therapy, a profession that addresses the whole person in the context of their natural environments. Occupational therapy works because it considers each person’s uniqueness and complexity and meets them where they are to foster participation in wanted, valued, and needed activities, tasks, and occupations.
Despite the merits that occupational therapy brings to people, populations, and society, it can be misunderstood or undervalued. Its unique focus on occupation and the inherent complexity of clinical practice can make it challenging to articulate the profession’s evidence and contributions to health and well-being (Thomas et al., 2023). Furthermore, as with most interventions, evidence-based practices in occupational therapy have been slow to become integrated into everyday practice (Krueger et al., 2020). Thus, it has become increasingly important to not only guide occupational therapy practice in an evidence-based, outcomes-oriented way but also to identify strategies that can foster the dissemination of knowledge and the integration of evidence into practice.
Precision occupational therapy is a useful concept to facilitate this. Precision occupational therapy builds on an emerging concept in health care: precision medicine (Scala et al., 2023; Seymour et al., 2017), which places a greater emphasis on a highly personalized approach. Precision medicine uses data about a client’s unique genotype and phenotype, combined with evidence and theory, to make clearly defined treatment recommendations (Lim et al., 2024).
Like precision medicine, precision occupational therapy embodies a personalized approach that respects the individual and considers multiple streams of information simultaneously to design treatments that are specifically tailored to each client and measures meaningful, personalized outcomes. Precision occupational therapy considers the individual’s strengths and needs and customizes interventions to enhance wellness and quality of life. This approach is in keeping with current health care trends, where a focus on the individual is recognized as a vital component of evidence-based health care, shared decision-making, and client-oriented outcomes research (Canadian Institutes of Health Research, 2011; Patient-Centered Outcomes Research Institute [PCORI], n.d.).
Data-Driven Decision-Making
The data-driven decision-making process (DDDM) is a systematic guide for clinical reasoning that can be used to guide precision occupational therapy. DDDM was developed to ensure that practice is methodologically sound, occupation focused, theory driven, data based, and outcomes oriented (Schaaf, 2015; Schaaf & Mailloux, 2015). It guides the practitioner to describe explicitly “What we do and how we do it” (Holm, 2000, p. 576) by clearly articulating the process used to craft individually tailored interventions, how they are implemented, the recommended frequency and duration, and the outcomes expected for each particular client.
As shown in Figure 1, DDDM begins in occupation. The Occupational Profile and personalized interactions with the client are used to identify their strengths, needs, and interest in participation in valued occupations. Once the reasons for seeking occupational therapy services are clear, it is important to identify an appropriate theory to guide practice. A theory is an explanation for the organized set of ideas that clarifies how things work, or an organized schema of how factors may be related to each other (Cole & Tufano, 2024). The choice of theory is always personalized and chosen on the basis of the client and the contextual factors that match the client’s needs. There is a vast array of theories that can be used in occupational therapy practice (Cole & Tufano, 2024), and in DDDM the practitioner is guided to choose the theory that best helps explain concepts related to the client’s health and well-being.
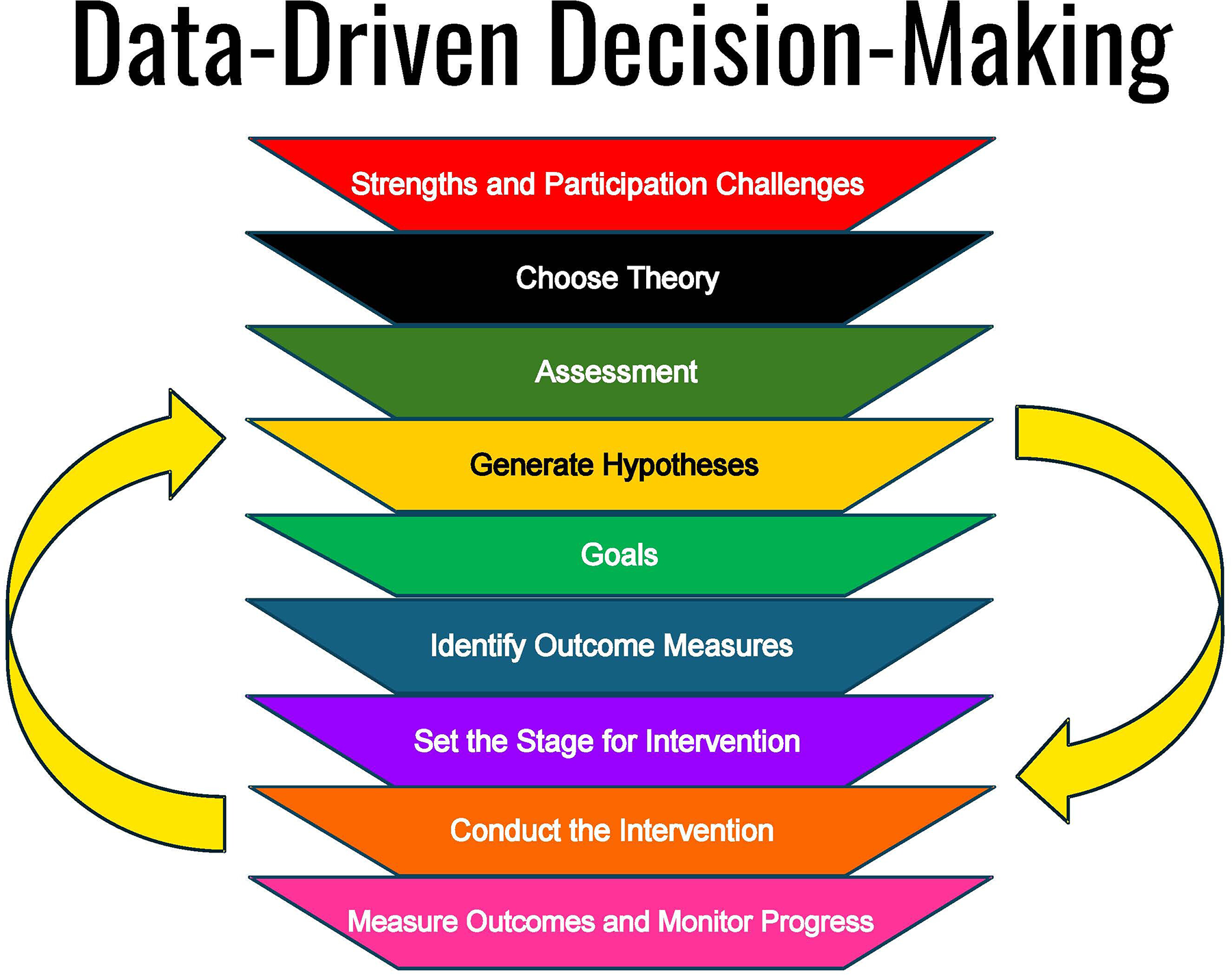
Data-driven decision-making.
The clinician or researcher then identifies assessment measures that are in keeping with the chosen theoretical framework and conducts a comprehensive assessment to identify factors affecting the client’s successful participation in occupations. The assessment data analysis process leads to the generation of hypotheses, a pivotal step in DDDM that I describe in more detail shortly. Hypotheses are testable predictions about the relationship between two or more variables—in this case, between participation challenges, strengths, and interests and the underlying factors found in the assessment data. The hypotheses are a starting point for treatment because they define the specific factors that will be addressed in treatment.
Next, client-specific goals are cocreated with the client and key stakeholders. The expected outcomes of the intervention are determined, and strategies for measuring them are identified at the proximal and distal levels (i.e., outcomes). With these pieces in place, the occupational therapy intervention is crafted in keeping with the chosen theoretical perspective and scope of practice (AOTA, 2020).
First, the stage for the intervention is set. This is accomplished by identifying the setting, the approach (e.g., direct, consultative, group, telehealth), and the dosage (duration and frequency) that best match the context and the client’s needs.
Next, a detailed plan that guides the treatment process is created (this is described in more detail later). This might include direct intervention with the client; consultations with stakeholders; environmental adaptations or supports; and a specific focus on tasks, activities, and occupations. Finally, after the specified dosage of intervention, outcomes are measured and documented to monitor progress and share the client’s response to the intervention. The hypotheses or intervention may be modified or adapted on the basis of the outcome data. This is the blueprint for precision occupational therapy using DDDM. The process is dynamic, personalized, and responsive to the client’s response to intervention.
Case Examples of Precision Occupational Therapy
Three case examples are used to exemplify how to create a precision occupational therapy approach using DDDM to guide the occupational therapy process across practice settings. Each case demonstrates the ways in which precision occupational therapy can guide practice to be individualized, personalized, and evidence based while also offering the potential to create evidence through practice. Acknowledging that people are complex and multifaceted, these cases have been simplified for illustrative purposes. Case 1: Sophie. Sophie is a delightful and social 5-year-old who has strengths that include many friends and an interest in learning. Sophie’s parents are concerned about her difficulty managing crayons and other materials for participation in learning activities. Case 2: Jaylynn. Jaylynn is a young adult with mental health challenges who is experiencing homelessness. Jaylynn is motivated, displays interests in cooking, and would like to create a more stable and supportive living environment for herself. Case 3: Maria. Maria is a social and previously active 80-year-old experiencing chronic pain and fatigue from an autoimmune disease. Maria would like to continue to live independently and host a card club with her peers.
Sophie, Jaylynn, and Maria bring unique personal and contextual factors that affect their lives and must be considered in the occupational therapy process. Identified strengths; occupational or participation challenges; and personal, contextual, and environmental factors direct us toward choosing a theoretical model and assessment measures that match each client’s needs and personalized factors. Assessment data are collected and analyzed using clinical reasoning that considers the client’s strengths, needs, interests, and contextual factors to identify the patterns or aspects of function, or characteristics of the person–environment–occupation fit (Christiansen et al., 2014) that are affecting successful participation. Next, hypotheses are generated.
Hypothesis Generation and Testing
Hypothesis generation follows a thoughtful and analytical process. As shown in Figure 2, to create a hypothesis the strengths and participation challenges are identified, and assessment data are analyzed. These data are linked and guide the generation of the hypothesis. A hypothesis is tested by applying appropriate outcome measures that will generate data about whether the client has improved in identified areas.
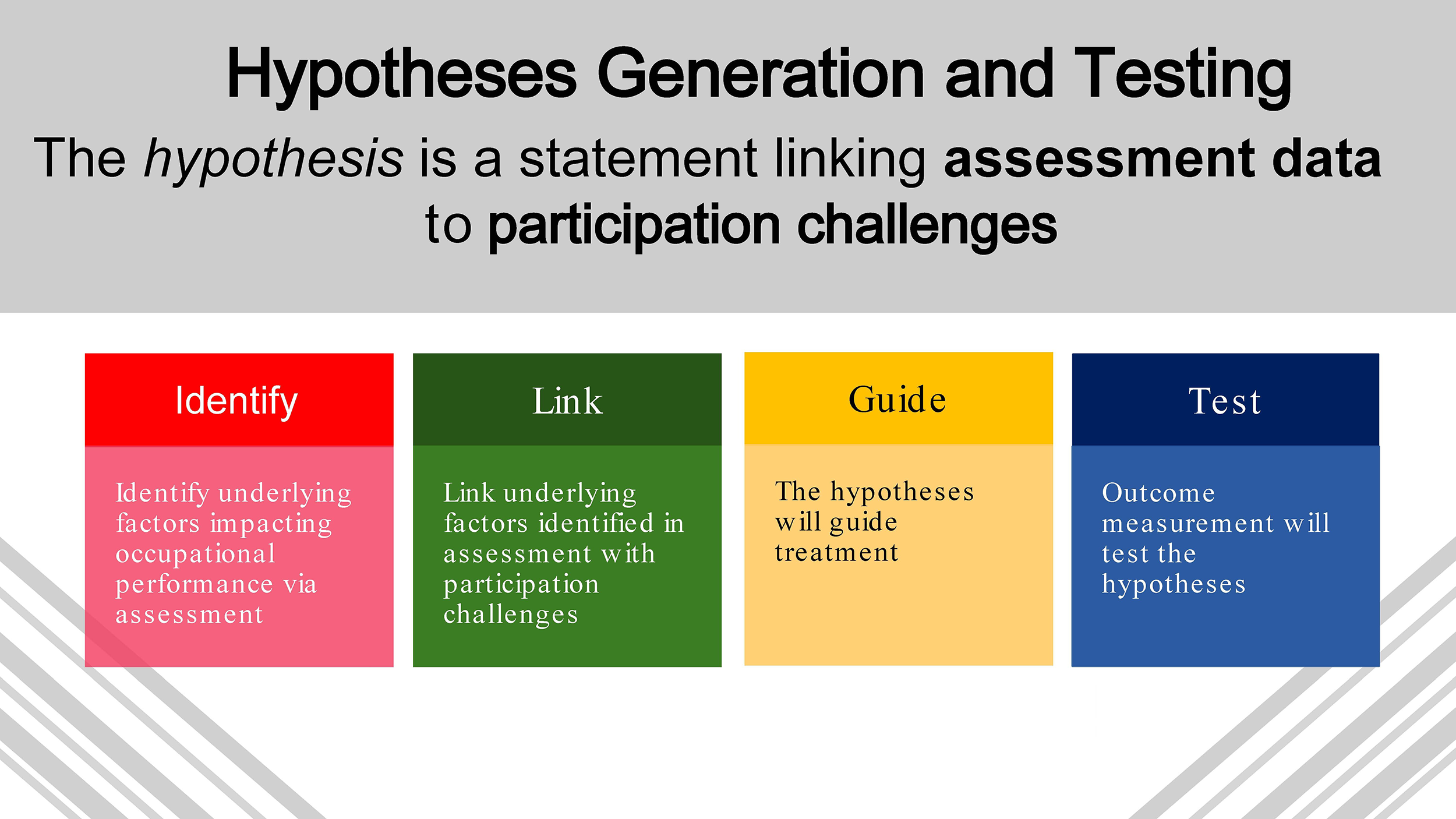
Hypothesis generation and testing.
Sophie
To create hypotheses for Sophie, we consider her strengths (i.e., that she is social and enjoys learning) as well as her challenge (i.e., difficulty participating in learning activities in her kindergarten classroom because she is struggling to manage crayons and other materials). Several factors may be influencing this challenge. Sophie’s history and Occupational Profile point to a focus on the sensorimotor aspects, and thus an evidence-based occupational therapy intervention, Ayres Sensory Integration® (ASI; Ayres, 1972) is used to guide assessment, intervention, and outcome measurement. The assessment data show that Sophie has a less-than-expected ability to discriminate and perceive tactile and proprioceptive sensations, which affects her ability to plan and execute actions with her hands. These data are linked with her participation challenges, and a data-based hypothesis is created: Decreased tactile and proprioceptive perception and praxis are affecting Sophie’s ability to use her hands effectively to participate in learning activities. This statement also identifies the targets of treatment (Hart et al., 2019; Van Stan et al., 2019) or the aspects of functioning directly targeted for change (i.e., tactile and proprioceptive perception and praxis) and guides the setting, materials, and dosage as well as the focus of the occupational therapy intervention. The process of hypothesis generation and outcome testing for Sophie is illustrated in the top panel of Figure 3.
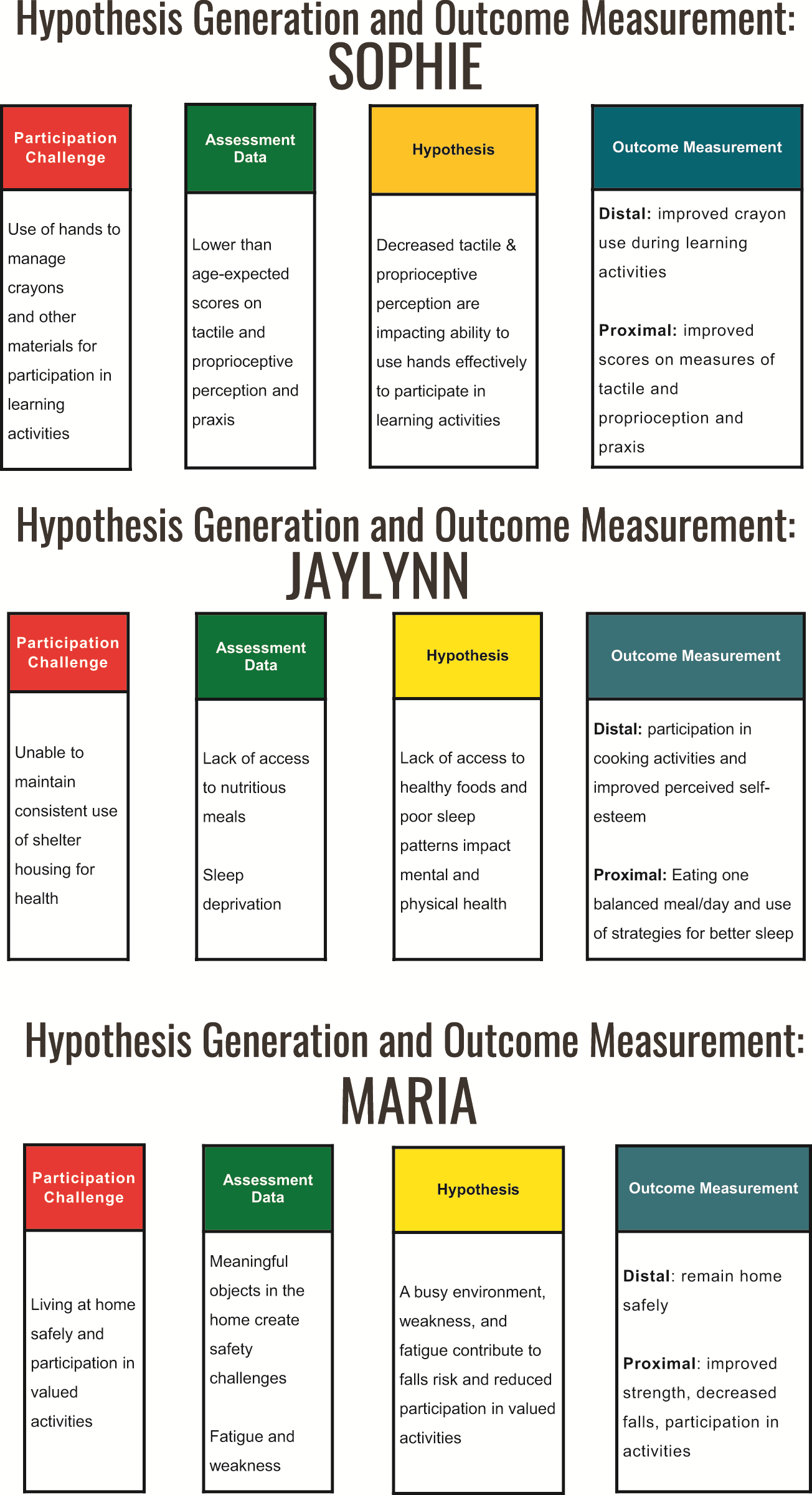
Hypothesis generation and outcome measurement for Sophie, Jaylynn, and Maria.
Jaylynn
Jaylynn brings strengths in that she is motivated to work, and she has a skill set to do so, but she is currently unhoused and experiencing mental health challenges related to schizophrenia and generalized anxiety disorder. The Occupational Profile data show that she enjoys cooking and has previously worked in a kitchen. An occupational therapy theory showing that engagement in meaningful occupations can support mental health, such as the one on which the Person–Environment–Occupation Model (Law et al., 1996) is based, is used to organize our approach with Jaylynn. Assessment data reveal that a lack of access to nutritious meals and sleep deprivation, caused by sleeping in a crowded and often-noisy shelter environment, are key factors affecting Jaylynn’s mental health and well-being. One hypothesis for Jaylynn is that a lack of access to healthy foods, as well as poor sleep patterns, are affecting her mental and physical health (middle panel, Figure 3).
Maria
Maria is an older adult who values socializing and living at home but is struggling to do so because of chronic pain and fatigue. Maria has experienced several falls and has been admitted to the hospital twice in the past 3 mo. The Person–Environment–Occupational Performance Model guides our approach (Baum et al., 2014); assessment data show that Maria loves to host her card club but is struggling to do so because of fatigue and safety challenges. Her home is filled with many meaningful objects, such as her collection of Lladró figurines; folding tables and chairs for her card club; and a variety of assistive devices to help with walking, carrying, and reaching during daily tasks and activities. Maria is weak and becomes fatigued easily, and her environment is creating many potential safety hazards. While ensuring respect for Maria’s culture, and building on her interests and strengths, hypotheses are identified to create a two-pronged precision occupational therapy approach: (1) Maria’s busy environment creates a risk for falls that make it difficult for her to live at home safely, and (2) Maria’s weakness and fatigue have an impact on her successful participation in wanted and valued activities (bottom panel, Figure 3).
Outcome Measurement
As described earlier, hypotheses are tested by measuring outcomes. What change is expected on the basis of the intervention? In precision occupational therapy using DDDM, outcomes are measured at the proximal and distal levels. Proximal changes are the underlying factors hypothesized to be influencing participation in occupations, and distal outcomes are the occupations themselves. This, then, links the intervention to occupation. As shown in the top panel of Figure 3, for Sophie, the change, or distal outcome, is improved use of crayons for participation in learning activities. This can be measured in a variety of ways; two examples are goal attainment scaling (GAS) and the charting of observational data. Both methods provide data that can be reviewed and evaluated to determine if the intervention is having the desired effect on occupational participation. The proximal factors that are hypothesized to affect this change are improved scores on measures of tactile and proprioceptive perception and praxis (the ability to plan and execute movement).
For Jaylynn (middle panel of Figure 3), the distal outcome is participation in cooking activities and improved perceived self-esteem, and the proximal factors are eating one balanced meal per day and the consistent use of client-centered resources and strategies for better sleep. These can be measured with standardized measures and staff-reported data.
For Maria (bottom panel of Figure 3), the distal outcomes are that she can remain in her home safely and participate in her card club once a week for 1 hr. Proximal factors influencing this outcome are improved strength, endurance, and decreased falls.
Of course, it is more nuanced than this, but these case examples illustrate a basic idea of precision occupational therapy using DDDM: Generate data-based hypotheses and then identify outcomes that will gauge the effectiveness of the intervention.
Intervention
Turning to intervention, in precision occupational therapy using DDDM the theory, assessment data, and hypotheses help specify the intervention. The factors identified during the assessment process are analyzed and operationalized in the hypothesis and used to create an individually tailored, data-driven intervention. Detailing and describing an intervention require sophisticated clinical reasoning so that the intervention is personalized, targeted, and individualized. The Rehabilitation Treatment Specification System (RTSS; Hart et al., 2019; Van Stan et al., 2019) can be used to further specify the intervention. The RTSS provides a universal system for describing or specifying rehabilitation interventions using a theory-based framework by depicting the targets of the intervention or the aspects of function that are expected to change; the proposed mechanisms of action, or how the treatment is expected to work; and the active components of the intervention, or what the clinician does. When treatment is specified in this way the causal factors are clarified and measured, and clinicians can better describe what they are doing, and why, with greater precision. Characterization of intervention in this way is illustrated next, for each case example.
Sophie
For Sophie, the guides for intervention are the principles of ASI (Parham et al., 2011). Therapeutic activities are guided by the identified active ingredients of this intervention, which for ASI are individually tailored, sensory motor activities contextualized in play at the just right challenge rich in tactile and proprioceptive sensations to promote use of her hands for learning activities (Schaaf & Mailloux, 2015). In the words of the RTSS, the “what” of intervention is described and is personalized on the basis of the client’s needs and responses. As shown in the top panel of Figure 4, the intervention for Sophie will be directed toward improving tactile and proprioceptive awareness and praxis so that she can use her hands more effectively during learning activities. The proposed mechanisms of action are change in somatosensory perception and praxis via neuroplasticity. Thus, the intervention has been specified, or detailed, in a way that is theoretically driven using the active ingredients and proposed mechanisms of action (based on the chosen theory), which are directed toward specific targeted outcomes. It looks like play as Sophie goes on a treasure hunt in a ball pit and then plays a game using a crayon to circle pictures of the treasures she has found, and sophisticated/precise deductive clinical reasoning underlies this process.
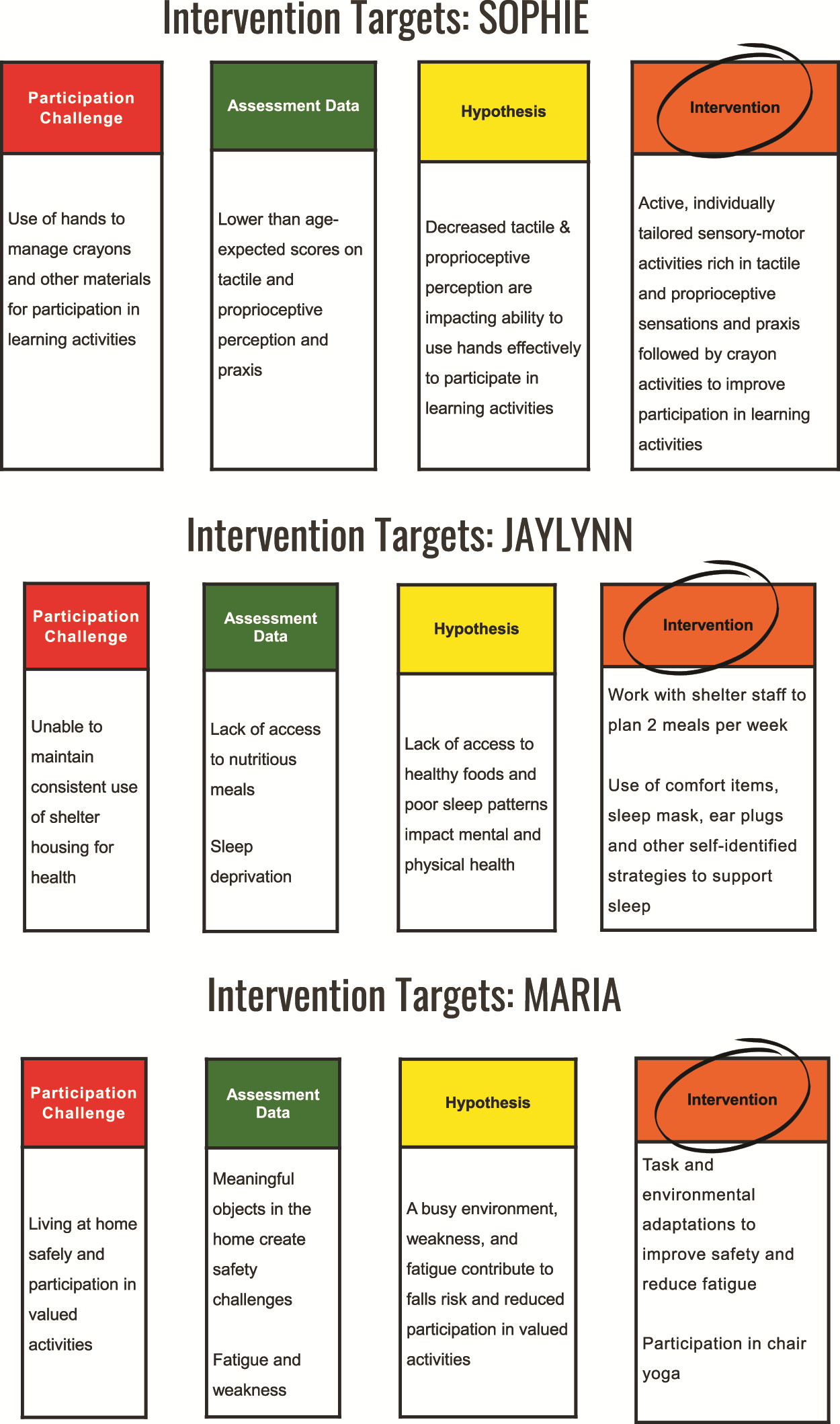
Interventions for Sophie, Jaylynn, and Maria.
Jaylynn
The intervention process for Jaylynn is shown in the middle panel of Figure 4. Recall that although Jaylynn is motivated to work, she is experiencing mental health and wellness needs because of a lack of access to nutritious foods as well as inadequate sleep and housing insecurity. The many issues that may be affecting her mental health are considered during the assessment and hypothesis generation and direct the intervention toward consideration of Jaylynn’s strengths and needs. Research suggests that engagement in meaningful activities and work fosters health outcomes in persons with mental illness (DeAngelis et al., 2019; Long et al., 2024). Given Jaylynn’s past interest and strength in cooking, the proposed mechanisms of action “learning by doing” and “task adaption” are used to collaborate with Jaylynn and the staff at the shelter and engage her in planning and preparing realistic and affordable meals. Also, in collaboration with Jaylynn, strategies to improve sleep are identified, such as a sleep eye mask, earplugs, and a familiar blanket to foster longer periods of rest and sleep in the shelter. Again, complex clinical reasoning grounded in theory and evidence are guiding intervention.
Maria
For Maria, evidence supports the use of thoughtful and acceptable environmental modifications to improve safety and reduce falls (Elliott & Leland, 2018; Leland et al., 2012; Washington et al., 2025). Evidence also shows that participation in meaningful physical activities reduces fatigue and improves strength (Leland et al., 2012); thus, identification of environmental adaptations to ensure safety and participation in valued activities while retaining objects that hold meaning for her is used. As shown in the bottom panel of Figure 4, to reduce fatigue and improve strength the interventionist helps Maria participate in a TV-based chair yoga class at home, an activity that she values and shows interest in. In a fashion similar to that used with Sophie and Jaylynn, an evidence-based precision occupational therapy approach was cocreated and implemented.
Examples of Precision Occupational Therapy Using DDDM to Create Evidence Through Practice, Extend Access and Reimbursement, and Broaden Impact
Clearly, precision occupational therapy using DDDM can serve as a road map for practice and research. As outcomes are measured, evidence is created, applied, documented, and disseminated, and the value of occupational therapy is bolstered. Importantly, DDDM can also be used to establish evidence that results in broader service access. One example of how precision occupational therapy using DDDM changed practice is a specific occupational therapy intervention for autistic children called occupational therapy using Ayres Sensory Integration® (OT–ASI; Schaaf & Mailloux, 2015). Implementation of precision occupational therapy using DDDM resulted in improved evidence for this intervention as well as enhanced recognition of and access to this intervention for autistic children and their families. It also launched a program of collaborative, interprofessional research that broadened its impact. This process is detailed next to exemplify that the same process can be used in other specialty areas of occupational therapy to create evidence, translate it to practice, and influence access to services and policy change.
OT–ASI is one of the most highly requested and valued occupational therapy interventions (Green et al., 2006; Interagency Autism Coordinating Committee, 2012; Reichow et al., 2018; Section on Complementary and Integrative Medicine et al., 2012; Shepherd et al., 2018) for autistic children; however, its theoretical foundations, mechanisms of action, and outcomes have often been questioned (Novak & Honan, 2019; Vargas & Camilli, 1999). OT–ASI intervention addresses the sensorimotor foundations needed for participation in occupations. Precision occupational therapy using DDDM guided the study of the efficacy of this intervention and changed the narrative about its evidence. First, a randomized controlled trial to study the outcomes of OT–ASI for autistic children ages 5–9 yr was designed and funded (Autism Speaks Foundation Treatment Grant 3797). This trial used rigorous characterization measures, blinded evaluators, careful allocation, standardized outcome measurement, timely posttesting, and intent-to-treat analyses, following the Consolidated Standards of Reporting Trials guidelines (Moher et al., 2010). Using precision occupational therapy, the OT–ASI process was manualized (Hunt et al., 2017; Schaaf & Mailloux, 2015) so that it could be implemented systematically and replicated in future studies.
The results of the trial showed that the children who received OT–ASI performed significantly better on their distal outcomes as measured with GAS (p = .003; d = 1.2), with a high level of significance and a large effect size (Schaaf et al., 2014). The treatment group also improved significantly, with strong p values and effect sizes compared with control children on other distal outcomes, including independence in self-care (p = .001; d = 0.9) and socialization (p = .04; d = 0.7) on the Pediatric Evaluation of Disabilities Inventory (PEDI; Haley et al., 1992). This study was published in the Journal of Autism and Developmental Disorders (Schaaf et al., 2014), one of the most highly regarded autism journals, and was listed as one of the most frequently downloaded articles in its publication year. By adding to the existing evidence base, this study tipped the scales and solidly established OT–ASI as an evidence-based intervention for autism, as noted in key evidence-based publications (Guirguis-Blake et al., 2007; Schoen et al., 2019; Steinbrenner et al., 2020). Subsequently, more insurance companies covered its costs (Lenhardt, 2023), and occupational therapy clinicians had the data needed to support its use in clinical work. Researchers had access to a manualized intervention for replication trials, and thus replications trials were conducted all over the world (Chan et al., 2023; Omairi et al., 2022; Randell et al., 2022). All found that children who received OT–ASI improved over control children in meeting individualized goals. Furthermore, McQuiddy et al. (2024) showed the long-term impact of this intervention, finding statistically significant postintervention improvements in individualized goals that were sustained at a 6- to 12-mo follow-up. They also noted that parents valued this intervention, stating a positive impact on their child and their family life. Client- or caregiver-reported outcomes, such as these, are emerging as important markers of clinically meaningful change (Weinfurt, 2019).
Building on this momentum, a large trial that compared the effectiveness of OT–ASI and applied behavioral analysis (ABA) was funded by the National Institutes of Health (Grant NIH R01 HD082814; Schaaf et al., 2014). This study found that OT–ASI and ABA resulted in significant improvements in GAS scores (p < .001) and Daily Activities T scores on the PEDI (change = 3.01, 95% confidence interval [CI] [0.1, 5.8], and change = 2.96, 95% CI [–0.05, 6.0] for the ABA and OT–ASI, respectively) in comparison with the no-treatment group (change = 0.75, 95% CI [–2.2, 3.68]; Schaaf et al., 2025), showing that OT–ASI is as effective as ABA in achieving individualized goals and participation in daily life activities for autistic children. Given that ABA is the standard of care for autism and substantial dollars are allocated toward this treatment, these findings have the potential to shift some of those funds toward occupational therapy and improve access to OT–ASI for more autistic children.
Implementation trials also emerged, with the goal of improving access to this intervention for underserved and minoritized/marginalized communities. The intervention was culturally adapted for Black and African-American families on the basis of their input and feedback to ensure its cultural relevance, acceptance, and satisfaction (Dumont et al., 2025). A telehealth adaptation was created and studied, showing it is feasible, safe, and acceptable to offer the intervention virtually so that rural and other underserved communities could have access to this intervention (Schiano et al., 2024), and an early-intervention adaptation was created and studied to extend it to younger children (Hunt et al., 2025).
Next, PCORI funded a project to improve access to and utilization of this intervention to Hispanic and Latino families with autistic children (Rios-Vega et al., 2025). Now, implementation trials to extend OT–ASI into pediatric school-based practice in an evidence-based and feasible manner are underway (Whiting et al., 2023). Preliminary findings show that occupational therapy using sensory integration improved functional regulation and active participation in school activities and that teachers and students had a positive opinion of this intervention (Whiting et al., 2023).
The importance and value of OT–ASI in school-based practice is also supported by research showing that occupational therapists, teachers, and administrators believe it is useful and appropriate in schools (Cerase McKeon et al., 2025; Loughery, 2024). Hence, precision occupational therapy using DDDM has provided a prototype for operationalizing OT–ASI in a manualized way and studying it with rigorous methods across contexts and populations. This has resulted in greater evidence for OT–ASI, greater respect for occupational therapy’s role with respect to autism, and greater access to this intervention for children and families who need it. Importantly, OT–ASI has taken a prominent seat at the table in autism in both research and practice.
Concluding Thoughts
Precision occupational therapy using DDDM is a useful way to elevate occupational therapy. It can be used to guide occupational therapy practice and research, resulting not only in greater evidence for occupational therapy interventions but also improved recognition and use of occupational therapy services. It can also be used in occupational therapy curricula to enhance students’ clinical reasoning and guide their ability to use evidence-based practices (Andelin et al., 2024; Schaaf et al., 2017). Educators, researchers, and clinicians are called to action: Use precision occupational therapy to guide your work. When you do, you will build evidence to help realize the profession’s vision of “enriching life for all individuals and society through meaningful engagement in everyday activities” (AOTA Vision 2030; AOTA, 2025, p. 1).
Footnotes
Acknowledgments
I thank my mentors, including Ruth Schemm, Laura Gitlin, Lucy Miller, and Janice Burke, and Jean Ayres, whose work set me on this scientific path. I also extend thanks to my many collaborators: first and foremost, Zoe Mailloux, who encouraged me to be fearless and stood beside me every step of the way; the team at Children’s Specialized Hospital in Tom’s River, New Jersey—Donna Kelly, Joanne Hunt, Elke van Hooydonk, Gina Freeman, and Patti Faller—and the team from the Rose F. Kennedy Center at the Albert Einstein College of Medicine in the Bronx, where our studies were conducted—Liz Ridgway, Tim Conly, Sophie Molholm, and John Fox. Thank you for supporting these studies and the many families that participated.
I also thank all my colleagues at the Collaborative for Leadership in Ayres Sensory Integration®, the Sensory Integration Research Consortium, and the international sensory integration community. Your support and encouragement help propel this work forward. I thank those associated with the Jefferson Autism Center of Excellence who engaged in this work and took it further than I thought possible.
I extend special thanks to all who contributed to this presentation by reviewing it, listening to it, and providing valuable feedback. Most important, I thank my family—my husband, David, and my daughters, Dayna, Lisa, and Laura—who give me the inspiration and encouragement to do this work.