
Abstract
Importance:
Schizophrenia typically requires long-term treatment, making cost-effective interventions essential, yet the cost-effectiveness of individualized occupational therapy (IOT) remains unclear.
Objective:
To compare the cost-effectiveness of IOT plus group occupational therapy (GOT) with GOT alone for inpatients with schizophrenia over 2 yr.
Design:
Secondary analysis of data from a multicenter, two-arm, parallel randomized controlled trial.
Setting:
Fourteen clinical facilities.
Participants:
Sixty-two inpatients with schizophrenia who completed 2-yr follow-up.
Intervention:
GOT alone or IOT+GOT during 3 mo of hospitalization.
Outcomes and Measures:
Quality-adjusted life-years (QALYs) and total medical costs from a health care payer perspective over 2 yr.
Results:
Compared with GOT alone (n = 30), IOT+GOT (n = 32) produced greater cumulative QALYs (M difference = 0.156) and lower total medical costs (M difference = −¥290,784). The incremental cost-effectiveness ratio was −¥3,304,420 per QALY gained. Incremental net benefit was positive at willingness-to-pay thresholds of ¥5,000,000 and ¥6,000,000 per QALY. The cost-effectiveness acceptability curves showed a 94.2% probability of cost-effectiveness at a threshold of ¥6,000,000. Cost data were complete for approximately 40% of participants; missingness was addressed using multiple imputation, with complete-case sensitivity analysis yielding directionally consistent findings.
Conclusions and Relevance:
IOT+GOT was more cost-effective than GOT alone over 2 yr, supporting its wider adoption as an economically sound rehabilitation strategy for clients with schizophrenia. Given the extent of missing cost data, the results should be interpreted with appropriate caution. These findings offer long-term economic evidence to inform mental health policies and resource allocation in psychiatric care.
Plain-Language Summary
Schizophrenia often requires long-term treatment, resulting in substantial health care costs. This study examined whether adding individualized occupational therapy to standard group occupational therapy offers a more cost-effective approach for inpatients with schizophrenia. Sixty-two patients were followed for 2 years after receiving either group occupational therapy alone or a combination of individualized occupational therapy and group occupational therapy during hospitalization. The results indicated that patients who received individualized occupational therapy and group occupational therapy experienced greater improvements in quality of life and slightly lower total medical costs. Furthermore, the cost-effectiveness analysis showed a 94.2% probability that the intervention would be cost-effective under Japan’s commonly accepted willingness-to-pay threshold. These findings suggest that individualized occupational therapy combined with group occupational therapy is a potentially cost-effective strategy for schizophrenia rehabilitation. This evidence supports the integration of individualized occupational therapy into standard psychiatric rehabilitation programs and may inform future mental health policy and resource allocation.
This study examined whether adding individualized occupational therapy to standard group occupational therapy offers a more cost-effective approach for inpatients with schizophrenia.
Cognitive impairment is a core feature of schizophrenia that affects domains such as processing speed, attention, memory, and problem solving. These deficits are strongly associated with poor functional outcomes and have been recognized as targets for therapeutic intervention (Fu et al., 2017; Green, 1996, 2006, 2016; Green & Harvey, 2014; Harvey & Isner, 2020; Javitt, 2022). Furthermore, long-term treatment of schizophrenia often leads to substantial health care expenditures, underscoring the importance of evaluating not only interventions’ clinical effectiveness but also their cost-effectiveness (de Oliveira et al., 2016; Knapp et al., 2004; Lin et al., 2023).
To address this issue, Shimada et al. (2016) developed an individualized occupational therapy (IOT) program tailored for patients with schizophrenia. The IOT program is a comprehensive, multicomponent psychosocial intervention designed to enhance cognitive functioning and adaptive behavior, with the ultimate goal of improving long-term functional outcomes. In a preliminary randomized controlled trial (RCT) conducted across six hospitals in Nagano Prefecture, we found that combining IOT with standard group occupational therapy (GOT) led to greater improvements in cognition, intrinsic motivation, psychiatric symptoms, and social functioning than GOT alone (Shimada et al., 2018). In addition, IOT+GOT significantly reduced the risk of psychiatric rehospitalization and prolonged the time to rehospitalization compared with GOT alone (Shimada et al., 2019). A subsequent cost-effectiveness analysis showed that IOT+GOT lowered total medical costs over 2 yr, mainly by reducing inpatient costs because of fewer readmissions (Shimada et al., 2020). However, the generalizability of these findings is limited by the regional scope of previous studies.
To address this limitation, we conducted a multicenter, two-arm, parallel RCT across 14 clinical sites in Japan to evaluate the impact of adding IOT to GOT on a range of outcomes, including cognition, motivation, health-related quality of life (HRQoL), social functioning, psychiatric symptoms, and overall functioning (Shimada et al., 2024). The results demonstrated that during the inpatient period the IOT+GOT intervention was significantly more effective than GOT alone in improving multiple domains, including cognitive and motivational functioning. Furthermore, a recent follow-up study demonstrated that the addition of IOT to GOT significantly reduced psychiatric rehospitalization rates over a 2-yr period (Shimada et al., 2025), highlighting the sustained impact of IOT on long-term patient outcomes.
Despite these promising clinical outcomes, the cost-effectiveness of the IOT+GOT intervention remains unclear, particularly in relation to long-term health care resource utilization. Therefore, the current study aimed to evaluate the cost-effectiveness of IOT+GOT compared with GOT alone over a 2-yr follow-up period using data collected alongside the RCT.
Method
Design
We conducted an economic evaluation alongside a multicenter, two-arm, parallel RCT from the perspective of health care payers. This analysis was based on a secondary data analysis of the original trial, which was conducted across 14 clinical facilities in Japan, enrolling hospitalized patients between January 2021 and June 2022, with a 2-yr follow-up.
In the original trial, patients were allocated to two groups: the GOT+IOT group and the GOT-only group. Both groups received treatment lasting approximately 3 mo from hospitalization to discharge. Outcome assessments were conducted at four timepoints: baseline (before randomization), discharge (or 3 mo after admission for prolonged hospitalization), 1 yr postdischarge, and 2 yr postdischarge. Per the prespecified protocol implemented in the parent trial, the primary inpatient clinical outcome was change in cognition from baseline to discharge (or to 3 mo if hospitalization exceeded 90 days), measured with the Brief Assessment of Cognition in Schizophrenia composite; assessments were conducted by trained, blinded assessors (details are provided in Shimada et al., 2024). In the same cohort, psychiatric rehospitalization over 24 mo was evaluated as a longer-term clinical outcome in a 2-yr follow-up report (Shimada et al., 2024, 2025).
For this secondary analysis, we extracted data from the original trial (Shimada et al., 2024) and focused on the economic evaluation of the intervention. Ethical approval for the primary study was obtained from the Ethics Committee of the Japanese Association of Occupational Therapists (Approval No. 2020001) and the ethics committees of all participating institutions. Written informed consent was obtained from all participants before enrollment. The original study was registered with the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR; UMIN000042532).
This article reports the prespecified trial-based economic evaluation of the cost-effectiveness outcome listed among the trial’s primary outcomes. In the publicly available UMIN-CTR registry, cognition, rehospitalization, and cost-effectiveness were listed as primary outcomes, with HRQoL as a key secondary outcome; however, the registry did not specify the metric for cost-effectiveness (e.g., quality-adjusted life-years [QALYs]). Following the prespecified analysis plan finalized before enrollment and included in the ethics and institutional review board documentation, we conducted a cost-utility analysis (CUA) by deriving utility values from the five-level EQ–5D (EQ–5D–5L; Ikeda et al., 2015); calculating QALYs; and estimating incremental costs, incremental QALYs, and incremental cost per QALY over 2 yr. Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot) clarifies this article’s position relative to parent trial reports by summarizing prespecified outcomes and mapping their reporting across the original publications and this article’s economic evaluation. Reporting of this economic evaluation followed the 2022 Consolidated Health Economic Evaluation Reporting Standards (Husereau et al., 2022).
Participants
Participants were recruited from multiple clinical sites between January 2021 and June 2022 as part of an RCT (Shimada et al., 2024). This study consisted of a secondary analysis of data from that trial.
The inclusion criteria for the trial were as follows: (1) age 20 to 60 yr, (2) confirmed diagnosis of schizophrenia based on the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; American Psychiatric Association, 2013), (3) capacity to provide informed consent, and (4) recent hospitalization in a psychiatric facility.
Participants were excluded if they met any of the following conditions: (1) a primary diagnosis other than schizophrenia as defined by the DSM–5, (2) a co-occurring intellectual disability, (3) a history of neurological disorders, (4) active substance abuse within 6 mo before consent, (5) a prior episode of substance-induced psychosis, (6) a current risk of suicide, or (7) the presence of a severe physical illness. The parent trial was designed to enroll 96 patients (48 per group), providing 80% power with a two-sided α of .05 to detect a rehospitalization hazard ratio of 0.543 over 2 yr, accounting for 5.15% attrition (Shimada et al., 2024). The trial ultimately randomized 68 patients because of practical constraints. As is typical for trial-based cost-effectiveness analyses, no separate power calculation was performed for costs or QALYs; instead, statistical uncertainty was characterized using nonparametric bootstrap resampling of incremental costs and QALYs and presented as cost-effectiveness acceptability curves (Ramsey et al., 2015).
Randomization Procedure
The details of the randomization procedure have been described previously (Shimada et al., 2024). Eligible participants were stratified according to age (20–29, 30–39, 40–49, and 50–60 yr), sex (male or female), and prior hospitalization frequency (three or fewer or four or more times) before being randomly assigned in a 1:1 ratio to either the GOT+IOT or the GOT-only group. Randomization was conducted independently using a computer-generated algorithm to ensure allocation concealment at the individual level.
Although the study was open label, the outcome assessors remained blinded to group allocation to minimize potential assessment bias. Assessors were designated separately at each study site and were solely responsible for conducting the evaluations, with no involvement in treatment allocation or occupational therapy sessions.
Intervention
Interventions consisted of IOT+GOT or GOT alone. For stand-alone clarity, we summarize the core elements as implemented in the parent trial (Shimada et al., 2016, 2018, 2024, 2025). In the GOT+IOT group, half of the total intervention time consisted of IOT. Patients in the GOT-only group received the same amount and duration of occupational therapy intervention as those in the GOT+IOT group.
IOT was delivered one-to-one by licensed occupational therapists during the approximately 3-mo inpatient period (from admission to discharge or at 3 mo if hospitalization exceeded 90 days). Therapists at participating sites received central training before trial initiation and implemented IOT according to the original IOT manual. IOT is a goal-oriented, manualized, multicomponent program consisting of motivational interviewing, self-monitoring, individualized visits, craft-based activities, individualized psychoeducation, and discharge planning; in this setting, these psychosocial components were delivered as occupational therapy. The component specific to the occupational therapist profession was the incorporation of craft activities with individualized coaching by occupational therapists designed to address cognition (Shimada et al., 2024, 2025).
GOT was provided as standard activity-oriented group treatment already implemented at each site and included physical fitness, crafts, cooking, music, recreation, and psychoeducation. Patients selected programs and participated at an individualized rate. Craft activities were also available in GOT, but occupational therapists assisted only on request. Treatment for each group lasted approximately 3 mo from hospitalization to discharge. Over the inpatient period, participants in GOT+IOT completed on average 61.8 sessions and 2,847.5 min of occupational therapy over 58.1 days, whereas those in GOT alone completed 54.9 sessions and 2,530.6 min over 63.0 days; between-groups differences were not significant (Shimada et al., 2024, 2025). To ensure standardization across sites, implementation was tracked with a standardized, study-specific checklist derived from the IOT manual and introduced during central training; because formal psychometric validation has not yet been conducted, we refer to the checklist as a preliminary fidelity checklist and report adherence descriptively.
Main Outcome and Cost Data
The main outcome of this study was cost-effectiveness, assessed as the incremental cost per QALY gained over a 2-yr follow-up. Because QALYs were used as the effectiveness measure, this analysis specifically constitutes a CUA, a form of cost-effectiveness analysis (Center for Outcomes Research and Economic Evaluation for Health, 2024; Kamae, 2019). HRQoL was assessed using the EQ–5D–5L (Ikeda et al., 2015) at baseline (admission), discharge (or 3 mo postadmission for those hospitalized for longer than 3 mo), 1 yr postdischarge, and 2 yr postdischarge. The EQ–5D–5L is a standardized measure of HRQoL that can be used to calculate QALYs, a key outcome in CUA. The resulting utility scores support value-based decision-making by translating quality-of-life (QoL) gains into a format that can be compared across rehabilitation interventions. QALYs were calculated as the area under the curve (AUC) of the QoL scores over time (Drummond et al., 2015).
Consistent with the protocol-defined timing rule (discharge if length of stay [LOS] < 90 days; 3 mo if LOS ≥90 days), inpatient QALYs were standardized to a 90-day period to account for variations in hospitalization duration. For patients discharged before 90 days of stay, their QoL was assumed to remain constant at the discharge value for the remaining period. The calculation formula was as follows: [(QoL score at admission + QoL score at discharge) × LOS/365]/2 + [(QoL score at discharge + QoL score at discharge) × (90 – LOS)/365]/2 + [(QoL score at discharge + QoL score after 1 yr) × 1]/2 + [(QoL score after 1 yr + QoL score after 2 yr) × 1]/2. To minimize bias from unequal observation windows, we aligned the inpatient segment to a fixed 90-day window. This is consistent with guidance for within-trial cost-effectiveness analyses to use a trial-aligned time horizon and to clearly justify standardization when measurement windows differ (Ramsey et al., 2015).
Medical costs were calculated for both the inpatient and the postdischarge periods. Inpatient costs included hospitalization-related expenses such as hospitalization fees, medication costs, psychiatric occupational therapy costs, IOT costs, and other inpatient expenses. Postdischarge costs included consultation fees, medication costs, psychiatric occupational therapy costs, psychiatric day care costs, home nursing costs, and other outpatient costs.
Cost data were extracted from the reimbursement claims (receipt data) of each participating hospital and compiled by site investigators. Unit costs were valued according to the Japanese national medical fee schedule (1 point = ¥10; Ministry of Health, Labour and Welfare, 2022).
Because there is currently no specific fee schedule for IOT in psychiatric settings, we adopted the reimbursement rate for individualized cerebrovascular rehabilitation (¥2,450 per 20-min session) as a proxy, citing the official fee schedule as the source (Ministry of Health, Labour and Welfare, 2022). The analysis was conducted from the psychiatric service cost perspective of health care payers. All costs were expressed in Japanese yen and converted to U.S. dollars using the 2022 Organisation for Economic Co-operation and Development (2023) annual average exchange rate ($1.0 = ¥131.5). Incremental net benefit (INB) values were reported only in Japanese yen because they are directly based on Japanese willingness-to-pay (WTP) thresholds. In addition to means and standard deviations, we also calculated medians and interquartile ranges for the variables presented in Table 1 and the QoL data; these are reported in Tables A.2 and A.3 in the Supplemental Material to account for potential skewness in the distributions.
Comparison of Total Health Care Costs and Cost Components Over a 2-yr Period for the GOT and GOT+IOT Groups
Note. Values are observed data without imputation for missing data. Component means are reported as observed, undiscounted available-case values, and therefore the row-wise means are nonadditive. The 2-yr total represents the mean of patient-level sums across complete cases (index inpatient + rehospitalizations + outpatient 0–12 mo + outpatient 12–24 mo). Outpatient costs are presented separately for 0–12 mo and 12–24 mo, which together cover the full 24-mo follow-up without double counting. GOT = group occupational therapy; IOT = individualized occupational therapy.
Missing Data
For transparency, complete 2-yr cost data were available for approximately 40% of participants; missing values were handled using multiple imputation by chained equations, and robustness was assessed in a complete-case analysis. This method is widely used to address missingness in health economic evaluations (Faria et al., 2014; White et al., 2011). The imputation process was conducted under the assumption of missing data at random, meaning that the probability of missing data depends on observed variables but not on unobserved values (Rubin & Schenker, 1991). The number of imputations was set to 50 to ensure stable estimates, with a burn-in period of 10 iterations before data collection to allow convergence. Linear regression models were used for continuous variables (e.g., LOS and QoL scores), whereas predictive mean matching with five nearest neighbors (k-nearest neighbors = 5) was applied to cost variables to account for skewed distributions.
The following variables were imputed: QoL scores at each timepoint, hospital costs, medical costs for the first year after discharge, and medical costs from 1 to 2 yr postdischarge. The imputation model included the intervention group and baseline QoL score as covariates to improve the accuracy of imputation.
Analysis was conducted in Stata (Version 17.1) using the mi impute chained command. After imputation, all estimates were pooled using Rubin’s rules to obtain valid standard errors and confidence intervals that accounted for uncertainty because of missing data (Rubin & Schenker, 1991).
Cost-Effectiveness Analysis
Cost-effectiveness was evaluated by calculating the incremental costs and QALYs between the intervention and control groups using 50 imputed data sets. For the economic evaluation, each cost component (inpatient, rehospitalization, outpatient 0–12 mo, and outpatient 12–24 mo) was first imputed separately using multiple imputation by chained equations. The imputed components were then summed at the patient level to construct 2-yr totals, ensuring that mutually exclusive categories were combined without double counting. Follow-up costs were discounted at 2% annually in the base case (0%–5% in sensitivity analyses). Group means and incremental costs were estimated after pooling across imputations using Rubin’s rules. QALYs were also constructed at the patient level as the AUC (trapezoidal rule) linking EQ–5D–5L utilities at admission, discharge (or 3 mo if LOS ≥ 90 days), 12 mo, and 24 mo; for early discharges (<90 days), discharge utility was carried forward to Day 90. Patient-level QALYs were then averaged and differenced between groups. To account for sampling uncertainty, nonparametric bootstrapping (1,000 replications per data set, totaling 50,000 replications) was performed. Following recommendations for trial-based economic evaluations with missing data, we handled missing data using multiple imputation under a missing-at-random assumption (Faria et al., 2014). Sampling uncertainty in incremental costs, incremental QALYs, and the incremental cost-effectiveness ratio (ICER) were characterized using nonparametric bootstrapping within each imputed data set.
For each imputed data set, 1,000 bootstrap replications were performed using ordinary nonparametric bootstrapping. Separate regression models were fitted for the total discounted costs and total discounted QALYs, with the treatment group as the independent variable. The incremental cost and QALY estimates were extracted from the regression coefficients and stored across all bootstrap iterations.
The ICER was calculated as the ratio of incremental costs to incremental QALYs. The INB was computed for WTP thresholds of ¥5,000,000/QALY and ¥6,000,000/QALY (Shiroiwa et al., 2010).
To assess decision uncertainty, cost-effectiveness acceptability curves were constructed by calculating the probability that ICERs fell below varying WTP thresholds (Fenwick et al., 2004). Additionally, cost-effectiveness planes were generated to visualize the joint distribution of incremental costs and QALYs.
Sensitivity Analysis
The base case applied a 2% annual discount rate to both costs and outcomes in line with Japanese health economic appraisal guidance (Center for Outcomes Research and Economic Evaluation for Health, 2024). We also varied the discount rate to 0% and 5% in one-way sensitivity analyses. QALYs and costs were discounted at their respective observation periods; that is, utilities measured at 12 and 24 mo were discounted by 1 and 2 yr, respectively, and cost components accruing in Years 1 and 2 were discounted by 1 and 2 yr.
In additional sensitivity analyses, we examined four alternative scenarios:
No 90-day standardization. We omitted the 90-day standardization of the inpatient QALY component and calculated inpatient QALYs using the observed LOS, allowing hospitalization QALYs to reflect each participant’s actual LOS.
Two-point AUC with LOS adjustment. We constructed 2-yr AUC QALYs using only baseline and 24-mo EQ–5D–5L utility values, assuming linear change between these two timepoints, and included LOS as a covariate in the regression models.
Complete-case analysis. We restricted the sample to participants with observed costs and EQ–5D–5L utilities at all required timepoints (baseline, discharge, 12 mo, and 24 mo), applied no multiple imputation, and quantified uncertainty in incremental outcomes using 1,000 nonparametric bootstrap replicates on the complete cases.
Covariate-adjusted analysis. Within each imputed data set, we additionally adjusted regression models for costs and QALYs for baseline physical comorbidity (any vs. none), age, sex, and baseline EQ–5D–5L utility to control for potential confounding.
All analyses were conducted using Stata (Version 17.1), with bootstrapping implemented via the bootstrap command and multiple imputations handled through mi estimate.
Results
Participants
Of the 315 individuals assessed for eligibility, 68 who met the inclusion criteria established in the previous study were randomly assigned to either the GOT+IOT group (n = 34) or the GOT-only group (n = 34). Of these, 67 (98.53%) completed the inpatient occupational therapy intervention. Among these, 66 participants met the eligibility criteria for the current study (34 in the GOT+IOT group and 32 in the GOT-only group); four participants (two from each group) withdrew from the study. A total of 62 participants completed the 2-yr follow-up and were included in the final analysis: 32 in the GOT+IOT group and 30 in the GOT-only group. A cost-effectiveness analysis was conducted on the final sample of participants who completed the 2-yr follow-up. Complete 2-yr cost data were observed for approximately 40% of participants, with the remaining cases contributing via multiple imputation, as specified in the “Method” section. At baseline, the participants’ mean age was 44.2 yr (SD = 9.34), and 35 participants (51.47%) were male. The mean EQ–5D–5L utility score at baseline was 0.71 (SD = 0.22) in the GOT+IOT group and 0.73 (SD = 0.17) in the GOT-only group.
Outcome and Cost
Table A.2 in the online supplement shows the mean EQ–5D–5L scores at each timepoint for both groups. At baseline (hospital admission), the overall mean QoL score was 0.72 (SD = 0.19), with 0.71 (SD = 0.22) in the GOT+IOT group and 0.73 (SD = 0.17) in the GOT-only group (p = .66). At discharge, the mean QoL score was 0.84 (SD = 0.16) overall, 0.87 (SD = 0.14) in the GOT+IOT group, and 0.80 (SD = 0.18) in the GOT-only group, showing no significant difference between groups (p = .10). At 1 yr postdischarge, the mean QoL score was 0.84 (SD = 0.14) overall, with 0.88 (SD = 0.10) in the GOT+IOT group and 0.81 (SD = 0.16) in the GOT-only group, demonstrating a significantly higher QoL in the GOT+IOT group (p = .046). At 2 yr postdischarge, the mean QoL score was 0.86 (SD = 0.15) overall, with 0.91 (SD = 0.10) in the GOT+IOT group and 0.81 (SD = 0.18) in the GOT-only group, again showing a significantly higher QoL in the GOT+IOT group (p = .011). These findings suggest that the GOT+IOT group had significantly higher QoL scores at both 1 and 2 yr postdischarge than the GOT-only group.
Table 1 presents the mean total health care costs at each timepoint for both groups along with their breakdown. The total inpatient costs (including IOT costs) were ¥2,128,996 (¥2,020,816) overall, ¥2,077,610 (¥1,931,962) in the GOT+IOT group, and ¥2,176,576 (¥2,135,434) in the GOT-only group, with no significant difference between groups (p = .86). The higher inpatient psychiatric occupational therapy costs in the GOT-only group likely reflect their somewhat longer hospitalization and greater exposure to reimbursed GOT. In the parent trial, the mean LOS was 113.1 (SD = 106.6) days for the GOT-only group versus 85.6 (SD = 58.9) days for the GOT+IOT group, and the duration of occupational therapy exposure during admission was also slightly longer for the GOT-only group (63.0 vs. 58.1 days), which would translate into more GOT units billed. IOT costs were recorded separately and not included in the inpatient psychiatric occupational therapy line (Shimada et al., 2024; 2025).
The total outpatient medical costs during the first year after discharge were ¥747,056 (SD = ¥555,864) overall, ¥892,421 (SD = ¥479,848) in the GOT+IOT group, and ¥617,844 (SD = ¥599,219) in the GOT-only group, with no significant difference between groups (p = .15). The total outpatient medical costs during the second year after discharge were ¥695,296 (SD = ¥566,846) overall, ¥744,457 (SD = ¥589,280) in the GOT+IOT group, and ¥656,669 (SD = ¥567,828) in the GOT-only group, with no significant difference between groups (p = .71). These results indicate that there were no significant differences in the inpatient or outpatient medical costs between the GOT+IOT and GOT-only groups.
Cost-Effectiveness
A cost-effectiveness analysis was conducted using a 2% discount rate. Table 2 presents the cost-effectiveness results of the GOT+IOT intervention compared with the GOT-only intervention over a 2-yr follow-up, based on multiple imputations (50 data sets) and nonparametric bootstrapping (1,000 replications per data set). Uncertainty was summarized using bootstrap percentile intervals (5th–95th percentiles). The mean incremental cost was −¥290,784 (5th–95th percentile interval = −¥1,386,711 to ¥766,612), indicating a tendency toward lower costs in the intervention group than in the control group. The mean incremental QALYs were 0.156 (5th–95th percentile interval = 0.044–0.271), suggesting an improvement in the QoL in the intervention group.
Cost-Effectiveness of GOT+IOT Compared With GOT Only Over 2-Yr Follow-Up
Note. Values are based on multiple imputation of 50 data sets and nonparametric bootstrapping with 1,000 replications per data set, applying a 2% annual discount rate to both costs and QALY. Uncertainty intervals are bootstrap percentile intervals. Standard errors reflect Monte Carlo uncertainty of the bootstrap mean and should be interpreted alongside the percentile intervals. For ICER ≤¥5,000,000, probability = 92.6%. For ICER ≤¥6,000,000, probability = 94.2%. ICER = incremental cost-effectiveness ratio; INB = incremental net benefit; QALY = quality-adjusted life year.
On the basis of these results, the ICER was −¥3,304,420 per QALY gained (5th–95th percentile interval = −¥13,419,454 to ¥6,617,950), suggesting that, on average, the intervention was dominant—both more effective and less costly than GOT alone. The INB was also calculated for different WTP thresholds. At a WTP of ¥5,000,000 per QALY, the INB was ¥1,072,624 (5th–95th percentile interval = −¥136,923 to ¥2,306,409), and at a WTP of ¥6,000,000 per QALY, the INB was ¥1,228,992 (5th–95th percentile interval = −¥40,980 to ¥2,523,253). These results suggest that the intervention is likely to be cost-effective at these WTP thresholds.
The cost-effectiveness plane further supported this finding because most bootstrap samples were located in the first or fourth quadrant, suggesting a trend toward cost savings and QoL improvement in the intervention group (Figure 1). The cost-effectiveness acceptability curve analysis showed that the probability of the intervention being cost-effective was 92.56% at a WTP of ¥5,000,000 per QALY and 94.23% at a WTP of ¥6,000,000 per QALY (Figure 2). This indicates a high probability that the intervention was a cost-effective option.
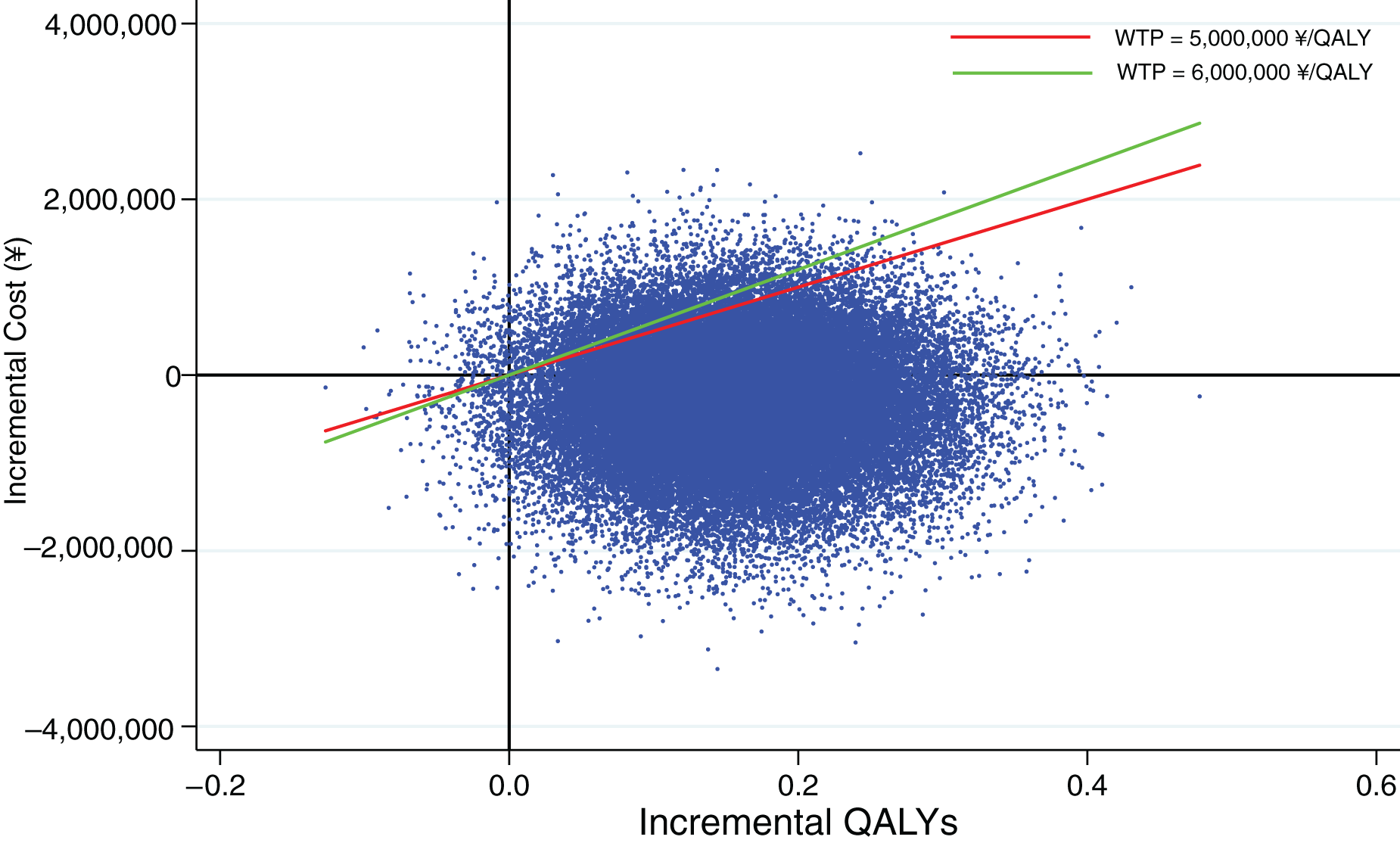
Cost-effectiveness plane.
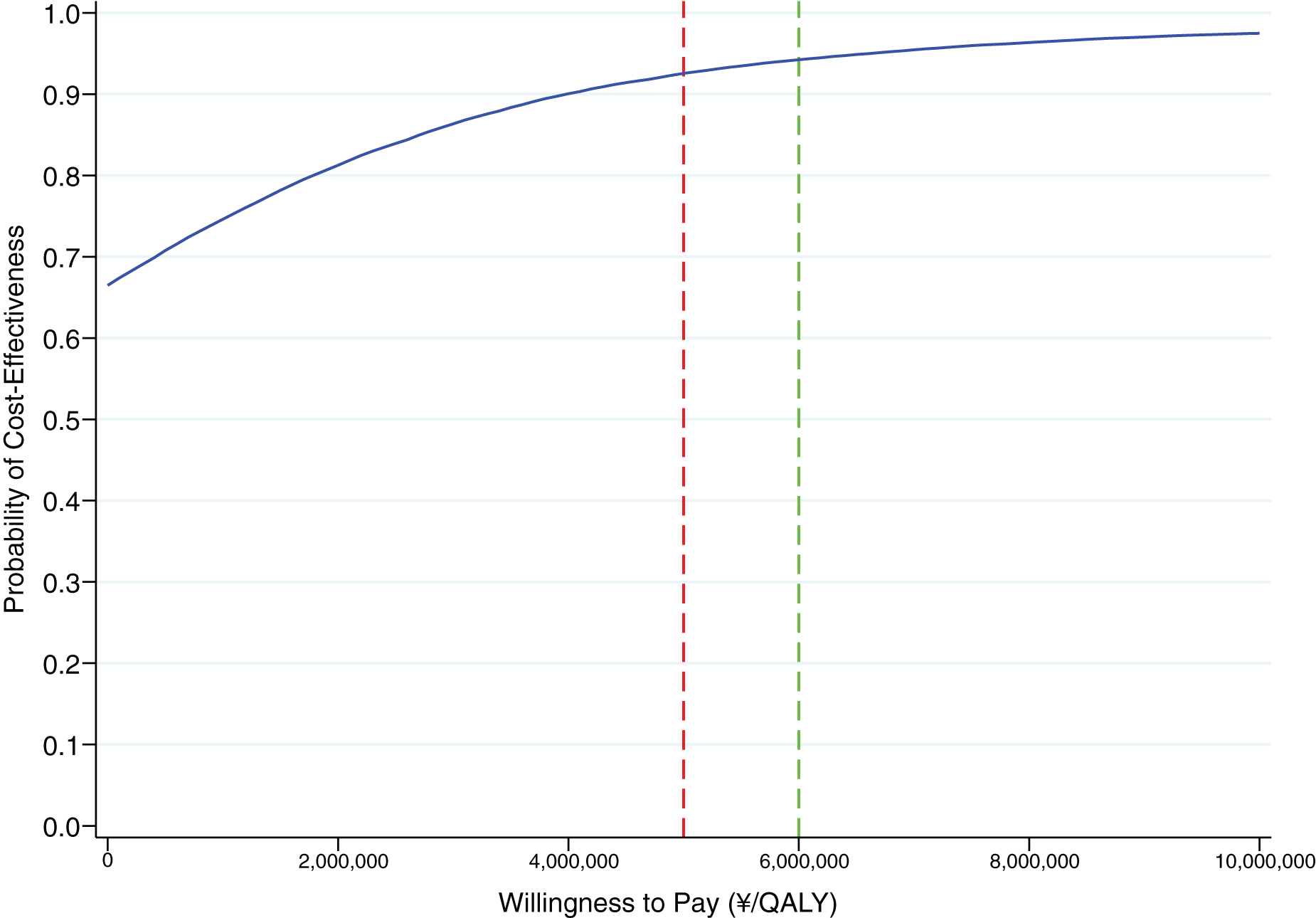
Cost-effectiveness acceptability curve.
Sensitivity Analysis
We conducted a sensitivity analysis by applying alternative discount rates of 0% and 5% (Table A.4). In both scenarios, the IOT+GOT intervention remained dominant, more effective, and less costly than GOT only. At a 0% discount rate, the ICER was −¥2,361,726 per QALY, with a 92.6% probability of cost-effectiveness at a ¥5,000,000 threshold and 94.3% at a ¥6,000,000 threshold. At a 5% discount rate, the ICER was −¥2,289,026 per QALY, with probabilities of 92.4% and 94.1%, respectively. These findings suggest that the cost-effectiveness results were robust to the discount rate assumptions tested. Four sensitivity analyses yielded results broadly consistent with the base case. As summarized in Table A.5, point estimates across all four scenarios continued to favor IOT+GOT over GOT alone (lower costs and higher QALYs). Incremental costs were negative in every scenario, and incremental QALYs were positive on average, although the 5th to 95th percentile intervals included zero in Scenarios 2 and 3. INB at WTP thresholds of ¥5,000,000 to ¥6,000,000 per QALY was also positive on average in all scenarios, with 5th to 95th percentile intervals excluding zero only in Scenario 4. ICERs were negative on average (indicating lower costs and higher QALYs) but accompanied by wide percentile intervals spanning both positive and negative values—consistent with the known instability of ratio estimators—thus, interpretation relies more heavily on INB. The proportion of bootstrap replicates in which the ICER fell below ¥5,000,000 to ¥6,000,000 per QALY exceeded approximately 65% in all scenarios and was highest in Scenarios 1 and 4. Taken together, these analyses support the base-case result while indicating that inference is most robust under Scenarios 1 and 4 and should be interpreted more cautiously under Scenarios 2 and 3.
Discussion
This study evaluated the cost-effectiveness of the combined IOT+GOT and GOT alone among inpatients with schizophrenia. The analysis was conducted alongside a multicenter, two-arm, parallel RCT. Total medical costs and QALYs were estimated over a 2-yr follow-up period. A nonparametric bootstrap method (1,000 replications per imputed data set) was used to calculate the incremental costs, effects, and ICER. The INB was calculated using WTP thresholds of ¥5,000,000 and ¥6,000,000 per QALY. The results indicated that the IOT+GOT intervention was both more effective and less costly than GOT alone, because the ICER was below zero, suggesting that IOT+GOT was a dominant strategy compared with GOT alone. The INB values were positive at both WTP thresholds, further supporting the economic advantage of the combined intervention. The probabilities that the ICER fell below the WTP thresholds of ¥5,000,000 and ¥6,000,000 per QALY were approximately 92.6% and 94.2%, respectively. These findings suggest that the addition of IOT to the standard GOT may represent a highly cost-effective rehabilitation strategy for patients with schizophrenia in Japan.
This study contributes to the growing body of evidence supporting the cost-effectiveness of psychosocial interventions for schizophrenia. Previous research demonstrated that combining IOT with GOT significantly reduced the risk and delayed the timing of psychiatric rehospitalization, resulting in lower total health care costs over a 2-yr period, primarily through reduced inpatient expenses (Shimada et al., 2019, 2020). Furthermore, a recent multicenter, two-arm, parallel RCT follow-up study demonstrated that the addition of IOT to GOT significantly reduced psychiatric rehospitalization rates over a 2-yr period (Shimada et al., 2025). The present study extends these findings by confirming the cost-effectiveness of IOT+GOT in a larger multicenter trial with nationwide representation. A systematic review concluded that psychological therapies for schizophrenia and bipolar disorder, including cognitive–behavioral therapy and integrated care, were cost-effective in most of the included studies, with probabilities ranging from 35% to 99.5% (Shields et al., 2019). However, this review highlights the limited availability of long-term data and considerable methodological heterogeneity. In this context, our study contributes to robust 2-yr follow-up data using a rigorous bootstrap-based cost-effectiveness framework. Moreover, recent studies have documented the substantial economic burden associated with schizophrenia, particularly because of repeated psychiatric hospitalizations (de Oliveira et al., 2016; Knapp et al., 2004; Lin et al., 2023). Our findings add valuable evidence from a nationwide, pragmatic trial, helping to close existing research gaps and supporting the broader implementation of IOT+GOT as a cost-effective rehabilitation strategy.
One likely reason for the favorable cost-effectiveness of the IOT+GOT intervention is the structured and individualized implementation of goal-directed occupational activities, particularly those based on craftwork. As demonstrated in a recent multicenter RCT (Shimada et al., 2024), therapist-guided craft-based interventions not only led to short-term improvements in cognitive function during the inpatient period but also contributed to long-term outcomes, most notably a significant reduction in psychiatric rehospitalization over a 2-yr follow-up (Shimada et al., 2025). These results suggest that the cognitively engaging and personalized nature of IOT plays a pivotal role in enhancing functional recovery and reducing subsequent health care utilization. In the current study, the cost of IOT was estimated on the basis of the Japanese medical reimbursement standard for cerebrovascular rehabilitation in the physical disability domain (Category 1: ¥2,450 per 20-min session). Although IOT is not currently reimbursed in the psychiatric care system in Japan, our findings indicate that such an intervention may constitute a cost-effective allocation of health care resources. This evidence may serve as an important reference point for future policy discussions regarding the potential inclusion of IOT in psychiatric reimbursement schedules.
Beyond the Japanese context, this study also provides broader implications. First, the analytic framework of cost-effectiveness analysis applied here represents a useful methodological approach to quantitatively demonstrate the value of rehabilitation, which is relevant internationally. Second, our findings highlight that, under the current reimbursement system in Japan, in which only GOT is covered, the demonstrated value of IOT may offer scientific evidence to bridge this policy gap.
Limitations
This study has some limitations. First, during the 2-yr follow-up period, complete cost data were available for approximately 40% of the participants. We addressed missingness using multiple imputation and confirmed robustness in a complete-case sensitivity analysis; nonetheless, the sample size and extent of missing cost data warrant cautious interpretation of the economic results. Second, the unit cost for IOT was estimated using the reimbursement rate for cerebrovascular rehabilitation in physical disability care in Japan (¥2,450 per 20-min session). Although this proxy is based on clinical plausibility, it may not fully reflect the actual cost of implementing IOT in psychiatric settings where no formal reimbursement framework currently exists. Third, our analysis considered only direct health care costs and did not account for indirect costs such as productivity losses. In addition, the analysis was limited to psychiatric service costs and did not include general medical costs unrelated to psychiatric care. Therefore, the findings should be interpreted as representing cost-effectiveness from the perspective of psychiatric service costs borne by health care payers. Moreover, this trial evaluated an inpatient occupational therapy program that was not designed as a vocational intervention, and we did not deliver or assess postdischarge vocational rehabilitation services. Accordingly, a societal perspective (e.g., productivity losses or benefits) lay outside our within-trial analysis. Any downstream societal effects—including employment—would be at most indirect (via improved functioning and a smoother transition to community living) and remain speculative; they warrant dedicated evaluation in future studies that explicitly include vocational rehabilitation services and adopt a societal cost perspective. Fourth, although implementation was monitored using a study-specific (preliminary) fidelity checklist, the formal psychometric properties of this instrument have not yet been established; adherence findings should therefore be interpreted with appropriate caution.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
In psychiatric inpatient settings, occupational therapists can consider adding IOT to standard group programs when more individualized, goal-directed intervention is needed to address a client’s cognitive needs, motivation, daily life challenges, and discharge planning.
When considering whether to implement IOT in routine care, services should evaluate not only clinical benefit but also whether the additional resources required for IOT may offer sufficient value for longer-term psychiatric care.
Under the current Japanese psychiatric reimbursement system, wider implementation of IOT may require formal consideration of reimbursement, and these findings may provide important support for such discussions.
Conclusion
This study determined that combining IOT with GOT is likely to be more cost-effective in the long term than GOT alone for inpatients with schizophrenia. The cost-effectiveness analysis demonstrated a 94.2% probability that the ICER remained below the ¥6,000,000/QALY threshold, thereby supporting IOT+GOT as a feasible and economically sound rehabilitation strategy in psychiatric care.
Footnotes
Acknowledgments
This work was supported by the Japanese Association of Occupational Therapists (Grant No. 2020001) and Japan Society for the Promotion of Science KAKENHI (Grant No. JP24K02671). We gratefully acknowledge Shinichi Yamamoto, president of the Japanese Association of Occupational Therapists. We thank the following individuals: Naoko Nakamura, Kaori Aisu, Aki Kito, Ryo Kojima, Ayumi Yamanushi, Kojiro Kawano, Noriaki Hikita, Kayano Yotsumoto, Tomoe Ebisu, Masashi Kawamura, Takao Inoue, Junya Orui, Tatsumi Asakura, Masafumi Akazawa, Seika Sato, Machiko Irifune, Koji Kunita, Shoko Ito, Ami Koizumi, Aya Makabe, Sonoko Miyasaka, Fumiko Natsumi, Yumi Tanaka, Mihoko Nishitani, Emiko Kobayashi, Yurika Nishida, Saori Haga, Atsushi Kimura, Yuki Kurihara, Yuko Nishimura, Aiko Hoshino, Jun Nishino, and Shuhei Fujita. We acknowledge the use of ChatGPT to support the drafting and refinement of sections of the manuscript of this article, including assistance with language editing, structuring of scientific content, and improving clarity. We take full responsibility for the accuracy of the information and the interpretation of the results. No generative AI tool was used to create, alter, or manipulate the original research data or results presented in this study.