
Abstract
Importance:
Cognitive impairment is a common manifestation of Parkinson’s disease (PD) that can limit participation. A clearer understanding of how people with PD (PwPD) use strategies to support their functional cognition can guide interventions designed to promote occupational performance.
Objective:
To investigate strategy use by PwPD during a functional cognitive task and how it relates to task performance.
Design:
Cross-sectional within and between groups.
Setting:
Participants’ homes.
Participants:
PwPD without dementia (N = 51) were allocated into two groups according to Montreal Cognitive Assessment score: ≥26 for those with PD and normal cognition (PD–NC; n = 27) and ≤25 for those with PD and mild cognitive impairment (PD–MCI; n = 24).
Outcomes and Measures:
Performance outcomes (accuracy, total time, and efficiency) and strategy use on the Level 2 Adult/Older Adult version of the Weekly Calendar Planning Activity (WCPA).
Results:
In the whole PD group, increased strategy use correlated with higher accuracy and longer total time, and four specific strategies correlated with higher accuracy (p < .04). The PD–NC group had higher accuracy and used more strategies than the PD–MCI group (p < .02), including three strategies associated with higher accuracy (cross off entered appointments, enter fixed appointments first, cross off free day; p < .03). In the PD–NC group, increased strategy use correlated with higher accuracy and longer total time (p < .02). Strategy use and WCPA performance outcomes did not correlate in the PD–MCI group (p > .10).
Conclusions and Relevance:
This study adds to the understanding of how PwPD select and use strategies to support their functional cognition and suggests that PwPD could potentially benefit from interventions to optimize strategy use in occupational performance.
Plain-Language Summary
People with Parkinson’s disease experience changes in thinking and memory that affect their ability to participate in daily activities, and they use fewer strategies to support their cognition than their peers without Parkinson’s disease. We investigated the strategies people with Parkinson’s disease use to support their thinking and memory during a simulated functional activity, the Weekly Calendar Planning Activity. We sought to understand whether the strategies they used were related to better performance on the activity, and we explored differences in strategy use between people with Parkinson’s disease with normal cognition and those with Parkinson’s disease with possible mild cognitive impairment. We found that people with Parkinson’s disease who used more strategies performed more accurately. Participants with Parkinson’s disease with normal cognition used strategies that supported their accuracy but took longer to complete the task. Participants with Parkinson’s disease with possible mild cognitive impairment used fewer strategies and ones that did not support their performance. Our findings indicate that people with Parkinson’s disease may benefit from interventions focused on selecting and using strategies to improve their daily functioning.
This study investigated the strategies people with Parkinson’s disease use to support their thinking and memory during a simulated functional activity, the Weekly Calendar Planning Activity.
Cognitive impairment is common among people with Parkinson’s disease (PwPD). About 40% of PwPD have mild cognitive impairment (PD–MCI; Baiano et al., 2020), and many have subjective cognitive decline even at the time of diagnosis (Benito-Leon et al., 2011). The cognitive domains most often affected are attention, executive function, memory, and visuospatial function (Monastero et al., 2018). Impaired cognition among PwPD limits their participation in instrumental, leisure, and social activities (Foster & Doty, 2021; Foster & Hershey, 2011; Kudlicka et al., 2018; Rosenthal et al., 2010) and reduces their and their care partners’ quality of life (Klepac et al., 2008; Klietz et al., 2020; Kudlicka et al., 2014; Lawson et al., 2016; Rosqvist et al., 2022). Furthermore, cognitive challenges have an emotional impact because they threaten a person’s sense of identity, confidence, and self-efficacy (Jethani et al., 2024; Kudlicka et al., 2018; Lawson et al., 2018). Developing interventions that help PwPD adjust to changes in their cognition is a priority in the PD community (Goldman et al., 2018).
People use cognitive strategies as a routine part of healthy occupational performance to assist in managing cognitive challenges, acquiring new skills, and improving performance outcomes (Toglia et al., 2012). A cognitive strategy is a mental plan of action that allows someone to accomplish a task in a systematic way (Toglia et al., 2012; Westwood, 2006). Breaking a task down into smaller parts, making a list of required steps or items, and verbally rehearsing important information are all examples of cognitive strategies. For older adults with normal cognition and those with MCI, strategy use can improve performance of daily tasks (Weakley et al., 2019), and higher strategy use relates to better daily functioning (Bottari et al., 2014; Tomaszewski Farias et al., 2018, 2020). However, PwPD report using fewer strategies than age-matched healthy adults (Johnson et al., 2005), so interventions that increase strategy use could improve daily function among PwPD. It is important to gain a clearer picture of strategy use among PwPD to guide selection or development of such an intervention.
One way to measure strategy use in context is with the Weekly Calendar Planning Activity (WCPA; Toglia, 2015). The WCPA is a standardized performance-based test of functional cognition that involves entering a list of appointments into a weekly calendar. Successful completion requires planning, keeping track of which appointments have already been entered, avoiding conflicts, and managing obstacles such as interruptions from the examiner or changes in the calendar format. A novel feature of the WCPA is that it allows for documentation of both observed and self-reported strategy use. Thus, it provides information on someone’s process of performing a cognitively challenging task, not only on their performance outcomes (e.g., task accuracy).
Our previous comparisons of WCPA performance among PwPD with normal cognition (PD–NC), possible MCI (PD–MCI), and healthy controls demonstrate that different groups approach the task differently in terms of their strategy use and suggest that this may lead to different performance outcomes. The PD–MCI group had impaired accuracy and both PD groups had impaired efficiency relative to healthy controls (Foster et al., 2022). Interestingly, PD–NC participants used more strategies during task performance than did PD–MCI and healthy participants, which appears to have supported their accuracy while resulting in longer overall task time and, thus, poorer efficiency. In contrast, PD–MCI participants had poor efficiency because of reduced task accuracy. These findings suggest that the number of strategies used in a task may influence accuracy, time, and efficiency, but the prior study did not directly compare or relate these factors. Additionally, we did not examine the types of strategies used and their relationships with performance. Understanding which strategies PwPD use in cognitively complex functional activities and how those strategies relate to performance can help therapists design targeted and effective interventions.
In this study, we more closely investigate strategy use during the WCPA in PwPD without dementia. Our first aim was to determine which strategies PwPD use. We examined the frequency of use of individual strategies (e.g., underlining key words, verbal rehearsal) and strategy categories (grouped according to purpose, e.g., keeping track of information). Our second aim was to determine how strategy use relates to task performance outcomes such as accuracy, completion time, and efficiency. We addressed these aims in the whole PD group and also explored differences between PD–NC and PD–MCI participants.
Method
Participants
Participants were PwPD without dementia who were enrolled in a pilot quasi-randomized controlled trial of a metacognitive strategy intervention (Multicontext Approach; ClinicalTrials.gov ID No. NCT040418122). Participants in the St. Louis metropolitan area were recruited via the Washington University School of Medicine (WUSM) movement disorders center and research participant registry, the American Parkinson Disease Association Missouri Chapter, flyers, and word of mouth. Men and women older than 50 yr, diagnosed with typical idiopathic PD and at Hoehn and Yahr Stages I to III were included. Participants were excluded if they had possible dementia (as per diagnostic criteria [Emre et al., 2007], a Montreal Cognitive Assessment score <21 [Nasreddine et al., 2005], or physician or informant report), other neurological disorders, brain surgery, a significant history of or current psychiatric disorder, or any condition that would interfere with participation (e.g., non-English speaking). Informed consent was obtained from all participants, and all procedures were approved by WUSM’s institutional review board.
Study Design
This cross-sectional study used baseline data collected during the intervention trial. Before in-person testing, electronic medical records were used to acquire clinical characteristics (e.g., Hoehn & Yahr stage), and a REDcap survey (Harris et al., 2009) provided demographic data (e.g., age, education). Participants completed in-person pretreatment testing during two 1- to 2-hr sessions while on their regular medications. The Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005) was administered during the first session as a cognitive screening test and to categorize participants into PD–MCI and PD–NC groups using, respectively, a cutoff of ≤25 or ≥26 (out of 30, as per Movement Disorders Society Level 1 diagnostic criteria for possible PD–MCI; Dalrymple-Alford et al., 2010; Litvan et al., 2012). The WCPA (described in detail in the next section) was administered during the second session.
Measure
This study used the Level 2 Adult/Older Adult version of the WCPA (Toglia, 2015). The WCPA is a reliable and valid assessment of functional cognition across ages, cultures, and clinical populations, including among PwPD (Foster et al., 2022; Toglia et al., 2017). Participants were to schedule a list of 17 appointments onto a weekly calendar while adhering to five rules, such as not scheduling any appointments on a certain day of the week. Some of the appointments had to be scheduled at a specific day and time (e.g., Monday at 1:00 p.m.) and others could be scheduled within certain parameters (e.g., any weekday morning at 9:00 a.m.). The assessment was administered by a trained occupational therapist and independently scored by two occupational therapists. Performance outcomes included the number of appointments entered accurately into the calendar (accuracy), the total time taken to complete the task (total time in minutes), and efficiency of task performance (efficiency). Efficiency scores were calculated as a function of accuracy and total time as outlined in the WCPA manual (Toglia, 2015).
During task performance, the examiner observed how the participant completed the task and recorded strategy use using a checklist of 12 strategies. After the participant completed the task, the examiner conducted an after-task interview during which the participant reported any strategies used that might not have been observed by the examiner. Individual strategies were combined into categories on the basis of their purpose (Toglia, 2015): Strategies for enhancing attention to important information (attend category) include underlining, highlighting, or circling key words and using a finger to point to information; strategies for organizing information (organize category) include rearranging materials, categorizing appointments before entering, entering fixed appointments first, using a written plan, talking out loud about the strategy, and crossing off the designated free day; strategies for keeping track (keep track category) include verbal rehearsal and crossing or checking off appointments entered; and strategies for self-monitoring performance (self-monitor category) include self- checking and rereading the instructions or materials. This yielded counts of total strategies used, as well as descriptive data regarding individual strategy use and strategy category use. Additionally, we considered time taken to enter the first appointment into the calendar (planning time) as reflecting the strategy of planning.
Statistical Analysis
Data were stored and managed using REDCap electronic data capture tools hosted at WUSM (Harris et al., 2009) and analyzed using IBM SPSS Statistics (Version 28). Descriptive statistics were calculated for all variables, and data were visually inspected for normality. We used χ2 and independent-samples t tests for group comparisons of demographic and clinical characteristics. Because of nonnormal distributions of some of the WCPA variables, we used nonparametric tests for the remaining analyses. We used Mann– Whitney U tests to compare the PD–NC and PD–MCI groups on WCPA variables (accuracy, efficiency, total time, number of strategies used, planning time) and to compare WCPA performance across those who did and did not use specific strategies or strategy categories. We used χ2 tests to compare frequency of use of individual strategies and strategy categories across the PD–NC and PD–MCI groups. We used Spearman’s ρ to correlate number of strategies used and planning time with WCPA performance. All tests were two-tailed; ps < .05 were considered significant. Because this was an exploratory and descriptive study, we did not correct for multiple comparisons.
Results
Participant Characteristics
Participant characteristics are shown in Table 1. Three participants timed out on the WCPA (took longer than 30 min), so their scores were not included, yielding a final sample of 51. Using the MoCA cutoff of ≥26 or ≤25 (Dalrymple-Alford et al., 2010; Litvan et al., 2012), 27 participants were categorized as PD–NC and 24 were categorized as PD–MCI. Other than MoCA scores, the PD–NC and PD–MCI groups did not differ on any demographic or clinical characteristics (p > .13).
Participant Characteristics and Weekly Calendar Planning Activity Scores
Note. Values are number of participants unless otherwise indicated. PD = Parkinson disease; PD–NC = Parkinson disease with normal cognition; MoCA = Montreal Cognitive Assessment; PD–MCI = Parkinson disease with mild cognitive impairment; WCPA = Weekly Calendar Planning Activity.
*PD–NC > PD–MCI, p < .05. **PD–NC > PD–MCI, p < .10.
WCPA Performance and Strategy Use
Scores on the main WCPA areas are shown in Table 1. Efficiency scores could not be calculated for five PD–MCI participants because of accuracy scores <7 (Toglia, 2015), and one PD–NC participant was missing total time data because of administrator error, so their efficiency score could not be calculated. The PD–NC group had higher accuracy scores and used more strategies than the PD–MCI group (p < .02), and there was a trend for longer total time in the PD–NC group (p = .096). There were no group differences in efficiency or planning time (p > .58).
Frequency of individual strategy use and strategy category use by group are depicted in Figures 1 and 2, respectively. The percentage of the entire PD group that used each individual strategy is as follows (in descending order): use finger, 94.1%; reread, 74.5%; self-check, 68.6%; cross off entered appointments, 54.9%; enter fixed appointments first, 41.2%; rearrange materials, 31.4%; verbal rehearsal, 29.4%; categorize appointments, 21.6%; underline, highlight, or circle key words, 15.7%; cross off free day, 15.7%; talk about plan, 13.7%; and use a written plan, 7.8%. The percentage of the entire PD group that used at least one strategy from each strategy category is as follows: attend category, 94.1%; self-monitor category, 84.3%; organize category, 62.7%; and keep track category, 35.3%. More PD–NC participants than PD–MCI participants used the strategies of cross or check off entered appointments, enter fixed appointments first, and cross off free days (p < .03; Figure 1). More PD–NC participants than PD–MCI participants used strategies in the organize category, χ2(50) = 8.62, p = .004, and there was a trend for more PD–NC participants to use strategies in the self-monitoring category, χ2(50) = 2.97, p = .09 (Figure 2).
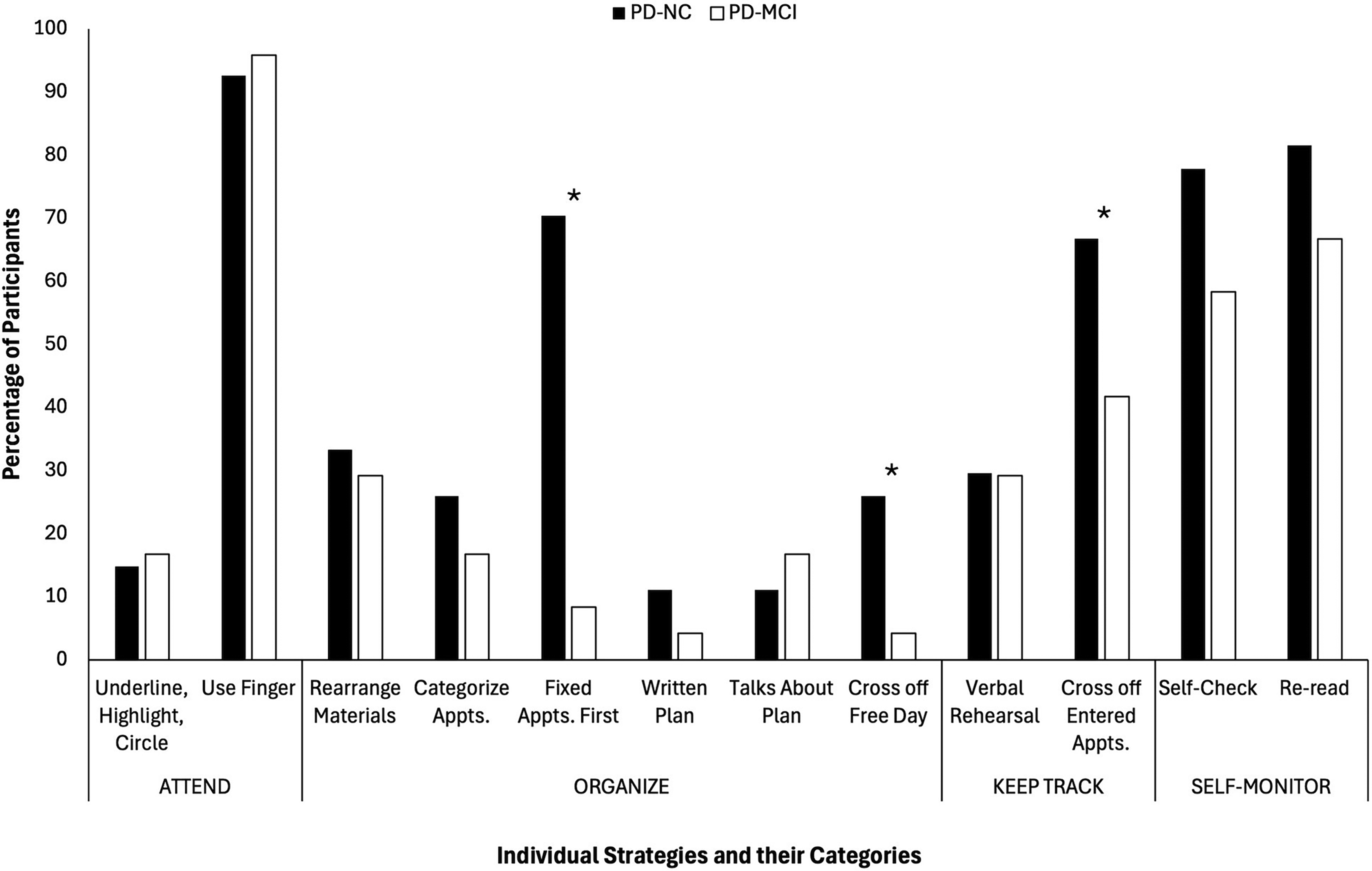
Frequency of individual strategy use by group.
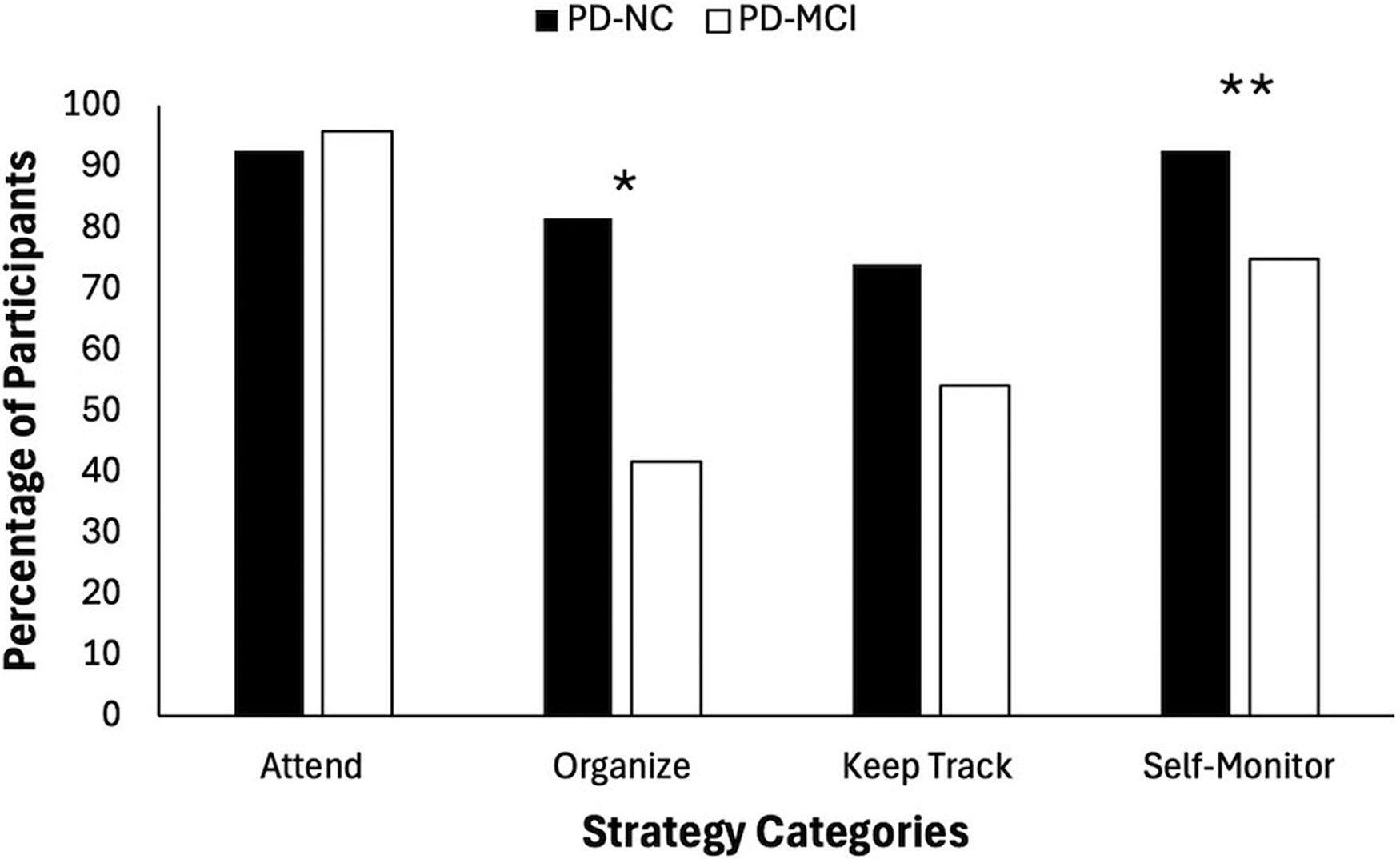
Frequency of strategy category use by group.
Association Between Strategy Use and Performance
For the entire PD group, a higher number of strategies used correlated with higher accuracy (r s = .35, p = .01) and longer total time (r s = .51, p < .001). Use of the following individual strategies related to higher accuracy: cross or check off entered appointments, enter fixed appointments first, cross off free day, and self-check (p < .04). Individual strategies related to longer total time were as follows: cross or check off entered appointments, enter fixed appointments first, use a written plan, talk about the plan, cross off free day, and reread (p < .05). Use of keep track, organize, and self-monitor strategies related to higher accuracy (p < .04); use of organize strategies related to longer total time (Mann–Whitney U = 135.50, p = .001); and there was a trend for use of keep track strategies to be related to longer total time (Mann–Whitney U = 196.5, p = .09).
Among PD–NC participants, higher number of strategies used related to higher accuracy (r s = .43, p = .02) and longer total time (r s = .63, p < .001). Use of the strategy cross off free day related to higher accuracy (Mann–Whitney U = 34.00, p = .04). Use of the strategies underline, highlight, or circle key words; enter fixed appointments first; use a written plan; and self-check related to longer total time (p < .05). Use of keep track and self-monitor strategies related to higher accuracy (p < .05), and use of organize strategies related to longer total time (Mann–Whitney U = 6.50, p = .001).
Among PD–MCI participants, strategy use and task performance were not related (p > .10). Additionally, strategy use did not relate to efficiency (p > .27), and planning time did not relate to any WCPA performance outcomes (p > .07) in any of the groups.
Discussion
We examined frequency and type of strategy use and how it relates to performance among PwPD during a complex functional cognitive activity (the WCPA). For the whole PD group, we found that increased number of strategies related to both higher accuracy and longer time. Furthermore, several specific strategies (cross or check off entered appointments, enter fixed appointments first, cross off free day, and self-check) related to higher accuracy. We also observed differences between PD–NC and PD–MCI participants in strategy use and effectiveness.
Although higher strategy use related to higher accuracy, it did not also relate to better efficiency. This is because participants used strategies that resulted in increased time to complete the task. Other studies on adults and at-risk adolescents have found a similar positive relationship between strategy use and accuracy (Arora et al., 2021; Weiner et al., 2012) and between strategy use and time (Marks et al., 2020; Weiner et al., 2012). Czernochowski et al. (2010) found that, when time is not an issue, older adults respond more slowly yet make fewer errors than younger adults when completing a cognitively challenging activity. They argue that older adults do not need to think quickly to complete most of their daily activities; consequently, they sacrifice speed for accuracy. Indeed, the verbal instructions for the WCPA include the phrase “I will be timing you, but it is more important for you to be accurate than to go quickly.” Thus, the PwPD in our study may have deliberately favored strategies they thought would improve their accuracy, regardless of how much time they took to implement, because they were told to prioritize accuracy over speed. Such a trade-off may not substantially negatively affect daily life function. However, qualitative studies have found that PwPD are concerned about the increased time it takes them to perform everyday activities (Kudlicka et al., 2018; Thordardottir et al., 2014). Thus, they may still benefit from learning how to use strategies more efficiently when time is a concern.
We found that four individual strategies (cross or check off entered appointments, enter fixed appointments first, cross off free day, and self-check) related to better accuracy for the whole PD group. Arora et al. (2021) also found that cross or check off entered appointments and enter fixed appointments first were associated with improved accuracy among older adults. Cross or check off entered appointments and cross off free day are external strategies that help participants keep track of information by eliminating irrelevant information, thereby decreasing cognitive load. Grouping appointments into fixed or flexible involves planning ahead and noticing similarities in the list of appointments. It makes the task more manageable by reducing the number of available options to schedule at a time and helps prevent potential schedule conflicts, thereby improving accuracy. Whereas the first three strategies help prevent errors from occurring, self-checking helps in recognizing errors that do occur and, consequently, provides an opportunity for remediation. Our findings indicate that using a range of strategies with a variety of purposes may be helpful when completing a complex functional cognitive activity. They also demonstrate that certain strategies may be more useful than others, because only four of the 12 individual strategies related to improved accuracy. This highlights the importance of investigating the relationship between specific strategies and accuracy for a specific task rather than merely focusing on the number of strategies used.
Notably, the strategy used most frequently by PwPD was not associated with accuracy. This finding is in line with that of Arora et al. (2021), who found that although use finger was the strategy most frequently used by older and middle-aged adults, it was not associated with accuracy in either group. The lack of association in our data may be attributed to a ceiling effect, because 94% of the PD participants used the use finger strategy. It is likely that this strategy supports performance, but the lack of variation in our data precluded our ability to detect a statistical relationship.
PD–MCI participants had less effective strategy use than PD–NC participants during the WCPA. Not only did they use fewer strategies overall, but they used fewer of the strategies that related to improved accuracy (cross or check off entered appointments, enter fixed appointments first, and cross off free day). These findings are consistent with those with other clinical populations associated with cognitive dysfunction, such as epilepsy (Zlotnik et al., 2020), attention deficit hyperactivity disorder (Lahav et al., 2018), and stroke (Jaywant et al., 2021). Moreover, we found no correlations between use of specific strategies or strategy categories and accuracy, time, or efficiency in the PD–MCI group. Thus, it appears that PD–MCI participants did not use many strategies, and the strategies they did use did not adequately support their performance.
In particular, it is interesting that PD–MCI participants used cross or check off entered appointments and cross off free day less frequently than PD–NC participants because these are simple external strategies that can reduce cognitive load. This may have stemmed from lack of initiation. Another explanation is that PD–MCI participants were not fully aware of task difficulty and thus did not recognize the need to use strategies to support their performance. Studies with other populations suggest that awareness of performance influences strategy use. For example, Salazar-Frías et al. (2025) found that persons with acquired brain injury who were aware of their performance used more strategies and did better than those who were less aware. Shaked et al. (2019) found lower memory awareness in older adults related to less concern and fewer activity modifications or reduced compensatory strategy use in everyday activities. In healthy adults, decreased awareness was also associated with fewer strategies, less self-monitoring, and lower performance on the WCPA (Arora et al., 2021). Our findings suggest that people with PD–MCI may benefit from interventions focused on building anticipation of task challenges and awareness of the type of strategies or task methods that contribute to efficient and effective performance. Focusing treatment on why and how strategies can support performance may help those with PD–MCI optimize their functional cognitive performance.
This study is limited by the relatively small number of PD participants in each group. Efficiency scores could not be calculated for six participants, potentially reducing the ability to detect group differences and fully understand the relationship between strategy use and efficiency. In addition, our PD sample was homogeneous in terms of race, limiting generalizability. Further studies that incorporate a larger, more diverse sample to understand how PwPD use strategies to support their performance of cognitively challenging activities are warranted. Future studies should also investigate factors that influence selection and use of strategies in PwPD, including online awareness of performance, knowledge of strategies, and strategy initiation.
Implications for Occupational Therapy Practice
This study examined how PwPD use strategies during a functional cognitive activity and how those strategies relate to task performance. PwPD with normal cognition can independently initiate and use strategies to support task accuracy but may benefit from intervention focused on strategy selection and use to optimize task efficiency. PwPD with MCI may benefit from intervention focused on building anticipation of task challenges, awareness of strategies, and strategy initiation. Planning ahead, eliminating irrelevant information, and self-checking improve task accuracy among PwPD.
Conclusion
This study adds to our understanding of how PwPD select and use strategies to support their functional cognition. In the whole group, strategy use in general and a few specific strategies (cross or check off entered appointments, enter fixed appointments first, cross off free day, and self-check) related to improved accuracy. PD–NC participants used strategies to support task accuracy but not efficiency, whereas PD–MCI participants used fewer strategies, and their strategy use was not associated with improved task performance. Our findings indicate that both PwPD–NC and PwPD–MCI use strategies but not in the most effective ways, and they may benefit from interventions that optimize strategy selection and use to support occupational performance.
Footnotes
Acknowledgments
This work was supported by the National Institutes of Health (R21 AG063974), the Missouri Chapter of the American Parkinson Disease Association (APDA), and the APDA Center for Advanced PD Research at Washington University in St. Louis. We thank occupational therapists Lisa Carson, Jill Jonas, and Becky Mollett for their contributions to this project.