
Abstract
Importance:
Sleep health supports child development and family well-being. Toddlers with Down syndrome experience elevated sleep difficulties, yet few studies have examined their sleep within a multidimensional framework.
Objective:
To apply the Pediatric Sleep Health framework (Peds B–SATED) to characterize multidimensional sleep health and sleep-related practices of toddlers with Down syndrome (12–36 mo).
Design:
Secondary analysis of cross-sectional descriptive data.
Setting:
Clinics and organizations serving families of children with Down syndrome.
Participants:
Twenty-four mothers of children with Down syndrome were recruited.
Outcomes and Measures:
Parent-reported Brief Infant Sleep Questionnaire items mapped onto the Peds B–SATED domains (Behavior, Satisfaction, Alertness, Timing, Efficiency, Duration). Descriptive statistics summarized sleep profiles and parental practices.
Results:
Fifty percent of the sample demonstrated multidomain sleep difficulties; 33% had difficulties in a single domain, and 17% had none. Behavior was the most problematic domain (63%), followed by satisfaction and efficiency (29% each), timing (25%), and duration (13%). Most children had structured sleep behaviors (consistent bedtimes/routines ≥80%; falling asleep independently, 70%; limited prebedtime screen exposure, 67%) and high parental satisfaction. Most children woke up happy and took one daytime nap (>90%). Sleep timing and efficiency were characterized by early bedtimes (median lights-out 8 p.m.; median wake 7 a.m.), no night awakenings (71%), and mean sleep latency of 13.5 min. Mean 24-hr sleep duration was 12.5 hr.
Conclusions and Relevance:
A multidimensional approach to characterizing sleep health reveals heterogeneous sleep profiles across domains and offers clinicians and researchers an in-depth view of intervention targets for toddlers with Down syndrome.
Plain-Language Summary
This study examined the sleep health of toddlers with Down syndrome ages 12–36 months by using the Pediatric Sleep Health framework, which looks at multiple aspects of sleep, including routines, quality, timing, and duration. Parents of 24 children completed a questionnaire about their child’s sleep, and then we mapped their responses to this sleep health framework. We found that most children went to bed and woke up early, slept about 12.5 hr per day, and were described as good sleepers. However, many children had at least one area of difficulty, most often related to bedtime behaviors (63%). In general, about 17% had no sleep-related concerns, whereas the remainder experienced challenges in one or more areas. These findings show that even when overall sleep appears good, specific sleep behaviors may still benefit from attention. Using a multidimensional sleep health framework can help identify these patterns and better describe sleep health of young children with Down syndrome.
This study examined the sleep health of toddlers with Down syndrome ages 12–36 months using the Pediatric Sleep Health framework.
Sleep is a fundamental occupation that underpins child development, playing a crucial role in supporting physical growth, cognitive development, emotional regulation, and overall well-being of young children (Schlieber & Han, 2021). Children with Down syndrome experience a high prevalence of sleep problems, influenced by multiple factors that shape their unique sleep health profiles (Santos et al., 2022). Personal factors include physiological features such as generalized hypotonia and distinctive craniofacial morphology, along with co-occurring medical conditions such as obstructive sleep apnea (Lee et al., 2018). In addition, external influences such as family routines, parental involvement in bedtime, and physical environment characteristics, including bright light exposure and use of electronic devices, may also shape sleep health of children with Down syndrome (Philbrook et al., 2022; Yau et al., 2019).
Toddlers experience rapid developmental changes in sleep architecture, routine formation, and behavioral regulation, making this period critical for establishing healthy, long-lasting sleep patterns (Bathory & Tomopoulos, 2017; Fucà et al., 2022). For children with Down syndrome, behavioral sleep difficulties often begin early and can persist or worsen over time. Poor sleep health among school-age children and adolescents with Down syndrome has been linked to increased internalizing and externalizing behavioral challenges, such as anxiety, depression, aggression, hyperactivity, and impulsivity (Fucà et al., 2023; Soltani et al., 2025). Moreover, disrupted sleep among children with Down syndrome can significantly affect family functioning by elevating parental stress and complicating daily routines (Churchill et al., 2015; Esbensen et al., 2021). Because sleep problems of toddlers may set the stage for such later difficulties, early identification of sleep health profiles is essential to enable timely, targeted interventions that support both child development and family well-being (Donovan et al., 2023).
Despite the essential role of sleep health in early childhood, existing research on children with Down syndrome has primarily focused on sleep-disordered breathing and often spans wide age ranges, limiting understanding of broader sleep health dimensions in early development (Santos et al., 2022). However, sleep health is multidimensional, shaped by biological, behavioral, and environmental influences, and cannot be fully captured by focusing on a single construct. The Pediatric Sleep Health framework (Peds B–SATED) provides a comprehensive structure for evaluating sleep across six interrelated domains: sleep-related Behaviors, Satisfaction with sleep, Alertness during waking hours, Timing, Efficiency, and Duration (Meltzer et al., 2021).
In this secondary analysis, we applied a Peds B–SATED lens to characterize sleep health of toddlers with Down syndrome (ages 12–36 mo) by mapping items from the Brief Infant Sleep Questionnaire–Revised (BISQ–R) onto its six domains. (Sadeh, 2004). The purpose of this study was to generate preliminary descriptive insights highlighting the potential utility of the framework for understanding sleep in this population and to lay groundwork for future research.
Method
Study Design
This cross-sectional descriptive study used data collected from a cohort investigating health behaviors of young children with Down syndrome (Caldwell et al., 2023). The design focused on characterizing multidimensional sleep health profiles of toddlers ages 12 to 36 mo. Web-based surveys were conducted from June 2020 to March 2021. Ethical approval was obtained from the University of Pittsburgh Institutional Review Board, and informed consent was obtained from all parent participants.
Participants
The analysis included 24 parent–child dyads recruited through specialty clinics and organizations serving individuals with Down syndrome via email lists and social media. Eligible parents were age 18 yr or older, English proficient, with a child age 12 to 36 mo diagnosed with Down syndrome. On the basis of the exclusion criteria from the broader cohort study, dyads were excluded if the child relied primarily on a feeding tube during data collection. For this secondary analysis, we excluded one additional dyad because of missing key sleep data, resulting in 24 dyads in the final analysis.
Measures
The study used the BISQ–R, a 33-item parent-report tool designed to assess sleep patterns, behaviors, and parental perceptions of infants and toddlers ages 1 to 36 mo (Sadeh, 2004). Most items are rated on a 5-point Likert scale, with higher scores indicating better sleep quality, more positive parent perceptions, and behaviors that promote healthy and independent sleep. We calculated total 24-hr sleep time by summing nighttime and daytime sleep durations. Sociodemographic data for parents and children were collected through a separate survey. The BISQ–R was not designed to measure pediatric sleep health domains directly but was used in this study as an existing parent-report source to explore sleep characteristics through a pediatric sleep health framework.
Mapping BISQ–R Questions to Peds B–SATED Domains
To apply a multidimensional framework to assess sleep health of young children with Down syndrome, we systematically mapped items from the BISQ–R onto the six domains of the Peds B–SATED framework (Meltzer et al., 2021): Behaviors, Satisfaction, Alertness, Timing, Efficiency, and Duration. This process intended to explore how parent-reported sleep characteristics captured by the BISQ–R may conceptually align with multidimensional domains of pediatric sleep health.
Mapping Rationale
The mapping process was guided by the domains’ definitions and descriptions outlined by Meltzer et al. (2021). Although the BISQ–R does not directly assess alertness, given its focus on infants and toddlers, related indicators such as daytime mood and napping patterns were incorporated to approximate aspects of this construct. Similarly, formal calculation of sleep efficiency was not possible; however, items related to sleep onset latency, night awakenings (frequency and duration), and uninterrupted sleep were used to reflect components related to this domain. Detailed item–domain mapping is presented in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Coding Procedure
Two independent researchers (Waad Aljurayyad, Angela R. Caldwell) coded the BISQ–R items according to the Peds B–SATED domains. The initial coding was reviewed by an expert in pediatric sleep health (Amy G. Hartman), and discrepancies were resolved through discussion until consensus was reached. Given the descriptive focus of this study, unequal numbers of items across domains were expected and considered acceptable to maximize representation of parent-reported sleep health characteristics.
Data Analysis
We report descriptive statistics of parent and child demographic characteristics to provide context for interpreting the sleep-related data. Sleep timing variables, collected in 30-min intervals, were summarized by using median and range to describe central tendency and variability. Continuous variables related to sleep onset latency, frequency and duration of night awakenings, and uninterrupted sleep were summarized by using the mean, standard deviation, and range. Frequencies and percentages were used to describe categorical variables within the domains of behaviors, alertness, and satisfaction. We calculated descriptive statistics by using complete data for each variable, with listwise exclusion applied only to variables containing missing values. All analyses were conducted with IBM SPSS Statistics (Version 30) software.
Results
Participant Demographics
The demographic and socioeconomic characteristics of 24 parent–child dyads included in the analysis are presented in Table 1. Children had a mean age of 26.17 mo (SD = 6.90) and were primarily female (54%, n = 13) and White/Caucasian (83%, n = 20). The most reported comorbidities included heart defects (33%, n = 8), hypothyroidism (25%, n = 6), and gastroesophageal reflux disease (17%, n = 4). Two parents reported their child was diagnosed with sleep apnea (8%). All 24 parent participants were mothers, with an average age of 36.71 yr (SD = 5.95).
Parent–Child Participant Demographic Characteristics
Sleep Health by Peds B–SATED Domain
Behaviors
Parents reported a range of bedtime behaviors, including screen use, schedule consistency, parental involvement at sleep onset, and responses to night awakenings. These behaviors are summarized in Table 2, along with evidence-based sleep recommendations to support interpretation.
Parent-Reported Behavior by Evidence-Based Sleep Recommendation (N = 24)
Note. Percentages are rounded to the nearest whole number. Totals represent 100% of available responses for each variable. Participants could select multiple responses for screen use and night awakening behaviors.
a N = 23 for that variable. b N = 22 for that variable.
Satisfaction and Quality
Parental reports indicated generally positive perceptions of their child’s sleep. Most parents (63%, n = 15) rated their child’s sleep as “very well,” 33% (n = 8) described it as “well” or “fairly well,” and only one parent reported “poor” sleep quality. Similarly, 71% (n = 17) of parents did not consider their child’s sleep as a problem, 25% (n = 6) considered it a “small” or “very small” problem, and only one parent reported a moderate problem.
Alertness, Sleepiness, and Napping
Most children (75%, n = 18) were described as “very happy” upon waking, with the remainder rated as somewhat happy (17%, n = 4) or neutral (8%, n = 2). Nearly all children (96%, n = 23) took one nap per day, with only one child reported to take two naps.
Timing
The median bedtime routine start time was 7:00 p.m. (range = 6:00–9:00 p.m.), with lights-out occurring at a median time of 8:00 p.m. (range = 7:00–9:30 p.m.). Wake-up times showed a median of 7:00 a.m. (range = 5:30–8:30 a.m.). These findings suggest that most of the children adhered to an early sleep schedule, although individual variability was observed.
Efficiency and Continuity
Sleep efficiency metrics are summarized in Table 3. On average, children took 13.5 min (SD = 5.6) to fall asleep and experienced 0.5 awakenings per night (SD = 1.1). Most children (71%, n = 17) reportedly did not wake during the night. Among those who did (29%, n = 7), the number of awakenings ranged from 1 to 4.5 per night, with a mean total awake time of 13.6 min (SD = 5.6). The mean duration of the longest uninterrupted sleep period was 10.3 hr (SD = 2.1).
Descriptive Statistics of Sleep Efficiency and Duration Variables (N = 24)
a N = 23 for that variable.
Duration
Children slept an average of 10.4 hr per night (SD = 1.1). Mean total daytime sleep was 2.2 hr (SD = 0.6), yielding an average 24-hr sleep duration of 12.5 hr (SD = 1.3), as summarized in Table 3.
Distribution of Problematic Peds B–SATED Domains Across Participants
Frequency analysis of problematic domains within the Peds B–SATED framework (Figure 1) revealed that 63% of participants (n = 15) had at least one problem in the behavior domain, making it the most frequently affected domain. Problems in the satisfaction and efficiency domains were each present in 29% of participants (n = 7), timing problems in 25% (n = 6), and duration problems were least common, affecting 13% (n = 3). No participants met criteria for difficulties in the alertness domain.
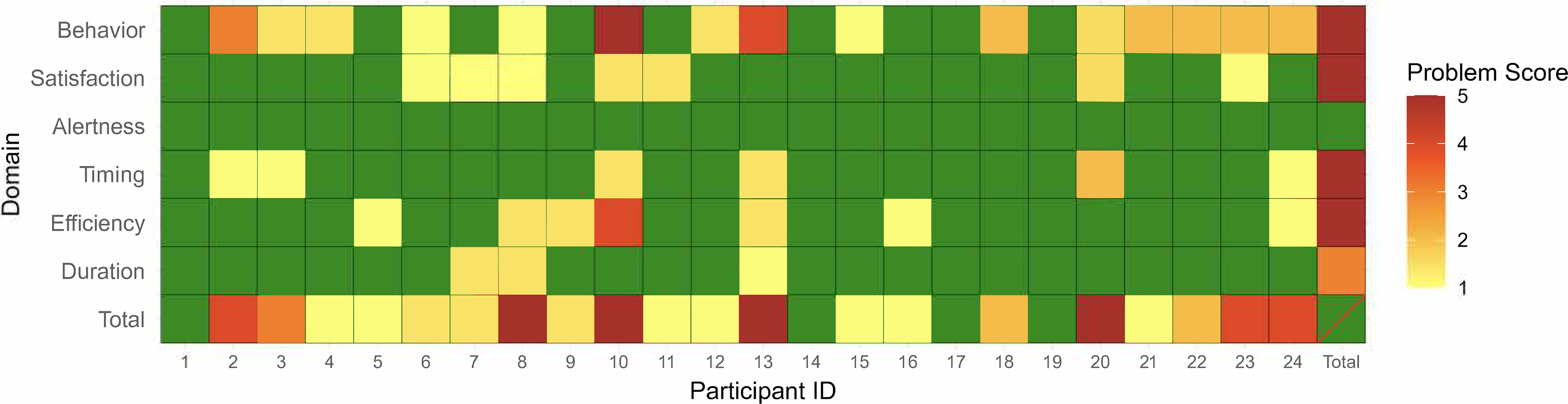
Heatmap displaying individual sleep health profiles of problematic (yellow–red) and nonproblematic (green) Peds B–SATED domains for 24 toddlers with Down syndrome.
Four participants (17%) had no problematic domains. Eight participants (33%) had problems isolated to a single domain (specifically behavior, efficiency, or satisfaction), whereas the remaining participants had difficulties across multiple domains. Operational definitions for each problematic domain are provided in Table A.1 in the Supplemental Material, specifying the criteria used to classify a domain as problematic.
Discussion
Sleep health is a critical determinant of growth, development, and family well-being for young children, particularly those with Down syndrome, who face heightened risks of adverse health trajectories (AlDarwish et al., 2025; Caldwell et al., 2023). To explore sleep health across multiple dimensions in our sample of children with Down syndrome, we mapped BISQ–R items onto the Peds B–SATED framework and examined domain-level patterns. Within this higher income, non-Hispanic White sample, the behavior domain was most frequently identified as problematic, a pattern that may reflect both reported behavioral challenges and the larger number of items in this domain (six items compared with two to four in the other domains). Despite this, mapping the Peds B–SATED framework also revealed several areas of relative strength. Most of the parents reported no prebedtime screen exposure and electronics-free sleep environments, practices associated with improved sleep quality and daytime alertness (Cook et al., 2024; Janssen et al., 2020). Consistent bedtimes and bedtime routines (5–7 nights per week) were also common, with most children falling asleep independently. These sleep-related behaviors align with rates reported in other Down syndrome samples, although some studies noted higher parental presence at bedtime when compared with typically developing children (Bassell et al., 2015; Yau et al., 2019).
During night awakenings, approximately one third of parents reported using brief waiting or rubbing/patting in the crib, practices consistent with behavioral sleep recommendations that emphasize minimal, calm parental responses (Morgenthaler et al., 2006). However, active soothing practices were also frequently reported in this sample, including rocking, lying next to the child, bottle or breastfeeding, diaper changes, or bringing the child into the parent’s bed. Prior research suggests that these practices may inadvertently reinforce sleep onset associations over time (Moore et al., 2008). Parental reports also indicated high overall satisfaction with their children’s sleep. Collectively, and given our sample’s relative homogeneity, these findings are best interpreted as demonstrating Peds B–SATED’s utility for descriptively mapping behavior domain data within a structured sleep health framework.
Within this framework, parent-reported findings across Peds B–SATED’s other domains can be examined in relation to established toddler sleep health guidelines. Indicators of alertness suggested positive morning affect and age-appropriate napping patterns, potentially supporting daytime alertness and homeostatic regulation (Galland et al., 2012). Sleep timing reflected typical toddler circadian patterns, with a median bedtime routine starting at 7:00 p.m., lights-out at 8:00 p.m., and wake time at 7:00 a.m. (Mindell et al., 2016). Efficiency profiles were characterized by rapid sleep onset and predominantly consolidated nighttime sleep. Sleep duration averaged 12.5 hr per 24 hr, with most children meeting recommended sleep durations of 11 to 14 hr (Paruthi et al., 2016). These group-level patterns demonstrate Peds B–SATED’s utility for benchmarking multidimensional sleep health against established guidelines. Nevertheless, these findings warrant cautious interpretation, because parent-reported measures may underestimate the frequency or severity of sleep health difficulties (Horne et al., 2023). Broader cultural attitudes toward Down syndrome may contribute to the normalization or acceptance of certain detriments to sleep health as intrinsic to the condition, potentially influencing parental perceptions and reporting (Chawla et al., 2023).
Individual-level Peds B–SATED mapping within our sample further revealed considerable heterogeneity despite group-level strengths. Reported nocturnal sleep durations ranged from 6.5 to 12 hr, night awakenings occurred as frequently as five times per night, and some children had bedtimes as late as 9:30 p.m. (Mindell et al., 2009). For three children with sleep durations outside recommended ranges, Peds B–SATED mapping revealed distinct multidimensional profiles, some characterized by differences across multiple domains and others by deviations within the single domain. These findings highlight the framework’s utility for capturing individualized sleep health profiles across domains, which may be obscured by group averages and extend beyond traditional item-level assessments.
Overall, Peds B–SATED mapping demonstrated utility at both group and individual levels within this sample of children with Down syndrome. Group-level analyses identified common patterns relative to established sleep health guidelines, whereas individual-level mapping captured meaningful heterogeneity across domains. The structured domain approach enabled parsing complex sleep profiles into actionable patterns, revealing co-occurring or isolated concerns. This capacity for detailed, domain-informed profiling is particularly valuable for characterizing sleep health during early development, when it affects both child developmental outcomes and family routines (Kocevska et al., 2017; Meltzer & Montgomery-Downs, 2011; Sadeh et al., 2010).
Limitations
This secondary analysis used a small (N = 24), highly homogeneous sample of higher income, non-Hispanic White families, which we recognize constrains statistical power and generalizability to the broader Down syndrome population. The cross-sectional, descriptive design identified the behavior domain within the Peds B–SATED framework as the most problematic domain but cannot establish causal relationships or longitudinal trajectories. Proxy measures for certain constructs (e.g., daytime alertness via morning mood/naps) and exclusive reliance on BISQ–R parent reports likely reduced granularity and introduced potential reporter bias, because parents may normalize suboptimal sleep patterns in this population. Findings demonstrate the descriptive utility of Peds B–SATED within this specific cohort rather than establishing normative sleep health profiles or domain-specific validation.
Future Directions
This study provides a foundational description of sleep health among young children with Down syndrome and highlights the need for longitudinal research on multidimensional sleep health and its downstream effects. Future studies should address current limitations by recruiting larger, more diverse samples to establish more representative Peds B–SATED sleep health profiles across socioeconomic and racial/ethnic groups. Multimethod assessments that combine parent reports with objective measures (e.g., actigraphy, polysomnography) would strengthen validation and mitigate potential parental normalization bias. Research examining and optimizing parental sleep practices—such as prebedtime screen time, bedtime routines, and night awakening responses—holds promise, given parents’ central role in shaping young children’s sleep environments and behaviors.
Implications for Occupational Therapy Practice
Findings from this sample of predominantly good sleepers suggest that families of children with Down syndrome can sustain healthy sleep within daily routines. Occupational therapists can leverage Peds B–SATED mapping to assess sleep health variability across domains and provide targeted family support. This study has the following implications for occupational therapy practice: Occupational therapists should support parents in establishing and maintaining consistent, calming bedtime routines to improve their children’s sleep onset and continuity. Occupational therapists should educate parents about limiting their children’s screen time in the hour before bedtime and removing electronics from the sleep environment. Occupational therapists should encourage parents to foster their children’s independence in falling asleep to reduce night awakenings. Occupational therapists should guide parents to use brief, calming strategies for their children’s night awakenings, such as waiting before intervening or offering brief reassurance to promote self-soothing.
Conclusion
This study used parent-reported BISQ–R data to describe sleep health among young children with Down syndrome ages 12 to 36 mo by using the multidimensional Peds B–SATED framework. Group-level analyses showed patterns aligned with guidelines, whereas individual mapping revealed domain variability, highlighting that one-size-fits-all approaches may not adequately address the unique sleep needs of this population. Despite sample limitations, multidimensional assessment identified actionable strengths and concerns obscured by traditional metrics. Overall, Peds B–SATED offers a promising tool for guiding both research and clinical practice in sleep health for children with Down syndrome.
Acknowledgments
The research was supported by the National Institutes of Health Comprehensive Opportunities in Rehabilitation Research Training K12 program (Grant K12 HD055931), Loan Repayment Program (Grant L40HD103240), Eunice Kennedy Shriver National Institute of Child Health and Human Development (K23HD119249), and the Clinical and Translational Sciences Institute at the University of Pittsburgh (Grant UL1-TR-001857).
Statement on Use of Generative AI
Waad Aljurayyad used ChatGPT and Perplexity AI only to improve clarity, grammar, and flow. All intellectual content and conclusions were developed by the authors, and all AI-assisted text was carefully reviewed for accuracy and originality.