
Abstract
Importance:
Rheumatoid arthritis (RA) causes persistent symptoms that limit individuals’ ability to engage in meaningful daily occupations. Occupational therapy plays a key role in integrating lifestyle and behavioral strategies into comprehensive RA management.
Objective:
To examine the efficacy of a client-centered, modular lifestyle intervention (LI) on occupational performance and health outcomes of individuals with RA.
Design:
A randomized controlled trial.
Setting:
Rheumatology outpatient clinic of a university hospital.
Participants:
Forty-five individuals diagnosed with RA were randomly assigned to an LI group (n = 23) or a control group (n = 22).
Intervention:
The LI group received an eight-session, occupation-based LI; the control group received twice-weekly well-being check phone calls over 4 wk.
Outcomes and Measures:
The primary outcome was the Canadian Occupational Performance Measure (COPM) Performance score. Secondary outcomes included COPM Satisfaction, Disease Activity Score–28, visual analog scale for pain, Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire, and Rheumatoid Arthritis Quality of Life Scale scores. Assessments were conducted at baseline, postintervention, and 6-mo follow-up.
Results:
Compared with the control group, the LI group demonstrated significantly greater improvements in the primary outcome (COPM Performance) as well as in secondary outcomes including COPM Satisfaction, pain, fatigue, and quality of life. A delayed reduction in disease activity was observed at the 6-mo follow-up.
Conclusions and Relevance:
The LI produced durable improvements in occupational performance and patient-reported outcomes, supporting its integration as a sustainable adjunct to pharmacological care for individuals with RA.
Plain-Language Summary
People with rheumatoid arthritis often have difficulty completing daily activities because of pain, fatigue, and limitations in movement. This study explored whether a structured lifestyle program based on occupational therapy principles could help improve these challenges. All participants continued their usual medical treatment throughout the study. In addition, one group received an eight-session lifestyle intervention focused on meaningful daily activities, healthy habits, energy conservation, and participation in social and leisure activities. The control group received their usual medical treatment along with brief well-being check phone calls. Participants who received the lifestyle program showed greater improvements in performing and enjoying daily activities and reported lower fatigue levels than those in the control group. These findings suggest that adding an occupation-based lifestyle program to standard medical care may provide meaningful benefits for people living with rheumatoid arthritis.
This study explored whether a structured lifestyle program based on occupational therapy principles could help address the challenges people with rheumatoid arthritis often have with completing daily activities because of pain, fatigue, and limitations in movement.
Rheumatoid arthritis (RA) is a chronic autoimmune disease marked by persistent synovial inflammation, progressive joint damage, and functional disability. Affecting 0.5% to 1% of the global population—with a 3:1 female predominance—RA imposes a substantial burden on quality of life and occupational participation (Bhakta et al., 2025). Despite pharmacological advances, many individuals with RA continue to experience residual symptoms such as pain, fatigue, and stiffness that restrict engagement in meaningful daily occupations (Fraenkel et al., 2021; Karstensen et al., 2022; Sagtaganov & Bekaryssova, 2024).
Recent European Alliance of Associations for Rheumatology (EULAR) guidelines emphasize combining pharmacological and nonpharmacological approaches, underscoring the need for individualized care targeting functional outcomes (Nagy et al., 2022). However, conventional rehabilitation often overlooks personalized occupational goals, despite up to 70% of individuals with RA reporting difficulties in self-care, work, and leisure (Drosos et al., 2022).
The lifestyle intervention (LI) is a client-centered, occupation-based intervention designed to support functional performance, participation, and self-management in daily life. The intervention was organized according to the COHPPE structure, an acronym formed from the initial letters of its guiding principle (Client-centered) and its five modules: Occupations and awareness, Healthy lifestyle habits, Protection, Participation and leisure organization, and Evaluation and home program. Within this structure, client-centered serves as an overarching principle rather than a separate module. LI was originally developed for individuals with fibromyalgia, demonstrating positive effects on symptom severity, functional outcomes, and quality of life (Salar et al., 2022, 2023). Building on this evidence base, the COHPPE-guided LI was systematically adapted for individuals with RA to address disease-related functional limitations and participation restrictions.
We hypothesized that there would be greater improvements in the LI group compared with the control group across multiple clinically relevant domains, including occupational performance and satisfaction, disease activity, pain intensity, fatigue severity, and health-related quality of life. We further hypothesized that these between-groups differences would be maintained at the 6-mo follow-up.
This randomized controlled trial provided a systematic LI evaluation specifically designed for individuals with RA, using an approach responsive to individual needs. The study addressed several important gaps in current RA management by (1) using an occupation-based intervention informed by client-centered principles, in which individually meaningful occupational challenges were identified via the Canadian Occupational Performance Measure (COPM) before the intervention and addressed during intervention sessions; and (2) integrating multiple evidence-based nonpharmacological strategies into a cohesive LI protocol with short-term and 6-mo follow-up assessment. The findings offer insight into the potential role of occupation-based, individualized LI in comprehensive RA care and may help inform future occupational therapy research and clinical practice.
Method
This randomized controlled trial investigated the effects of LI on individuals with RA. Conducted between February 2023 and May 2025, the study received approval from the Ethics Committee of Manisa Celal Bayar University, Faculty of Medicine (E.484791), and was registered at ClinicalTrials.gov (NCT05759585). The trial followed international ethical standards and the 2025 Consolidated Standards of Reporting Trials (CONSORT) guidelines (Hopewell et al., 2025).
Participants
The study included voluntary participants diagnosed with RA by a rheumatologist according to the 2010 American College of Rheumatology/EULAR criteria, recruited from the Rheumatology Clinic of Manisa Celal Bayar University Hafsa Sultan Hospital. Sample size estimation was performed by using G*Power. Because no published parallel-group effect size estimates were available for client-centered, occupation-based LIs for individuals with RA, the effect size was derived from the most conceptually comparable study (Tonga et al., 2015), which reported within-group changes in RA-related quality of life (d = 0.706). A two-tailed α of .05 and 90% power result in the required sample size of 19 participants per group. Allowing an anticipated 20% attrition rate, we set the recruitment target at 45 participants. Post hoc power analysis based on the observed primary outcome (COPM Performance; z = 3.34) indicated approximately 92% power at α = .05, confirming that the achieved sample size was adequate for detecting between-groups differences in the predefined primary endpoint.
We applied the upper age limit of 65 yr to reduce potential confounding related to age-associated comorbidities, cognitive changes, and functional decline that could independently influence occupational performance and responsiveness to the intervention, thereby enhancing sample homogeneity and internal validity. Participants had to maintain stable pharmacological treatment of at least 3 mo, have no surgery within 6 mo, and demonstrate sufficient literacy and cognitive capacity for cooperation. Exclusion criteria included other musculoskeletal or neurological disorders, visual or auditory impairments, and pregnancy.
A total of 81 individuals were screened; 11 declined participation, and 25 were excluded for not meeting inclusion criteria (8 individuals with Disease Activity Score–28 [DAS–28] > 5.1, 6 individuals with comorbidities, 2 individuals older than age 65 yr, 2 individuals with recent surgeries, and 7 individuals with other musculoskeletal or neurological disorders, visual or auditory impairments, or pregnancy). The remaining 45 eligible participants were randomly assigned to two groups. Following the intervention, postintervention data were available for 39 participants. However, in accordance with the prespecified analytic plan, we conducted longitudinal analyses by using a complete-case approach, which required participants to have valid data at all three assessment timepoints (baseline, postintervention, and 6-mo follow-up). Therefore, 33 participants with complete data across all timepoints were included in the final analyses.
We randomly assigned participants to the LI group (n = 23) or the control group (n = 22) by using an online randomization generator with allocation concealment. Because of the nature of the intervention, participants could not be blinded to group assignment. However, outcome assessors and statisticians were blinded, and datasets were anonymized by using group labels (Group A/B) for blinded analysis. Outcome assessors were independent from intervention delivery to minimize assessment bias. A flow diagram summarized recruitment, allocation, follow-up, and analysis in accordance with 2025 CONSORT guidelines (Figure 1).
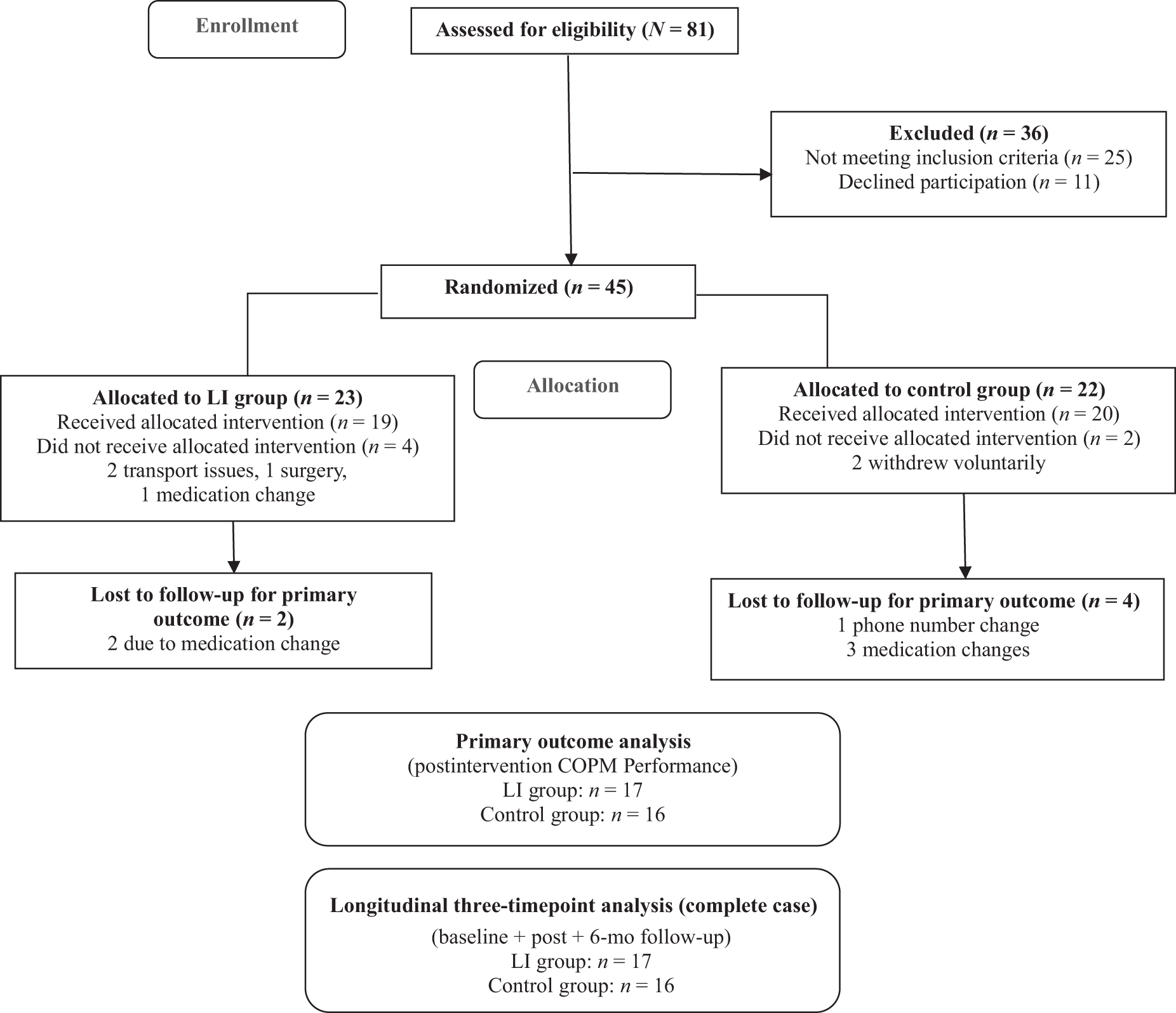
Consolidated Standards of Reporting Trials (CONSORT) diagram of flow of participants through the study.
Assessments
The prespecified primary endpoint was the between-group difference in COPM Performance scores at the postintervention assessment (Wk 4). Secondary outcomes included COPM Satisfaction, disease activity (DAS–28), pain intensity (visual analog scale [VAS]), fatigue severity (Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire [BRAF–MDQ]), and health-related quality of life (Rheumatoid Arthritis Quality of Life Scale [RAQoL]). These additional clinical and patient-reported outcomes were examined to provide a broader understanding of functional and symptom-related changes. All outcomes were assessed at baseline, postintervention, and 6-mo follow-up to evaluate both immediate and sustained effects. Demographic and clinical characteristics (age, body mass index, disease duration, gender, marital status, education, employment status) were recorded at baseline. Outcomes were evaluated by using the following standardized tools.
The COPM, developed by Law et al. (1990), identifies self-care, productivity, and leisure performance issues through a semistructured interview. Participants rate the importance of occupational activities (from 1 to 10), then rate performance and satisfaction for the five most important activities (from 1 to 10). Mean performance and satisfaction scores are calculated (Law et al., 1990). The Turkish version has demonstrated cultural validity and reliability (Altuntaş et al., 2024).
Disease activity was assessed by a rheumatologist using the DAS–28, which integrates tender or swollen joint counts, Patient Global Assessment (ranging from 0 to 100), and inflammatory markers (erythrocyte sedimentation rate or C-reactive protein). Scores ≤2.6 denote remission; scores of 2.6 to 3.2 denote mild; scores of 3.2 to 5.1 denote moderate; and scores >5.1 denote severe activity (Prevoo et al., 1995). Pain intensity was measured by using the 10-cm VAS (0 = no pain, 10 = worst pain), as developed by Huskisson (1974).
The 20-item BRAF–MDQ measures fatigue across physical, daily living, cognitive, and emotional domains. Items are rated on Likert scales from 0 to 3, with numerical responses for the first three items (0–10, 0–7, and 0–2). Total scores (ranging from 0 to 70) indicate fatigue severity (Nicklin et al., 2010). The Turkish adaptation has confirmed validity (Sari et al., 2018). The RAQoL comprises 30 yes/no items assessing disease-specific quality of life. Scores range from 0 to 30, with higher scores indicating poorer quality of life. The Turkish version is validated for reliability (Kutlay et al., 2003; Whalley et al., 1997).
Procedures
All evaluations were administered face-to-face and took approximately 60 min per participant. The DAS–28 was assessed by a rheumatologist, followed by the COPM interview (approximately 30 min). The COPM was administered by a licensed physiotherapist with graduate (master’s and doctoral) training in occupational therapy who is a faculty member in the Izmir Tinaztepe University Department of Occupational Therapy and has experience in COPM administration. Self-report questionnaires were then completed independently by participants under supervision.
Intervention
The LI program is a five-module, occupation-based program structured within the COHPPE framework. The modular structure included the following: Module 1 (Occupation and Awareness; one session); Module 2 (Healthy Lifestyle Habits; four sessions); Module 3 (Protection; one session); Module 4 (Participation and Leisure Organization; one session); and Module 5 (Evaluation and Home Program, final session; Salar et al., 2022, 2023). Tailoring was guided by each participant’s COPM results. COPM was administered before the intervention, and identified occupational priorities shaped subsequent sessions. For example, if morning self-care was prioritized, Module 2 incorporated sleep–wake restructuring, pacing, and fatigue management, whereas Module 3 emphasized joint-protection strategies for grooming. If meal preparation or home management was prioritized, Module 4 focused on participation planning, environmental modification, and task simplification.
The LI was delivered individually in eight face-to-face sessions over 4 wk (twice weekly; ∼60 min) in addition to pharmacological treatment. The intervention consisted of structured modules targeting occupational performance, lifestyle habits, and self-management skills (Table 1). The control group continued usual pharmacological care and received brief, standardized well-being phone calls (3–5 min) twice weekly for 4 wk. Calls followed a neutral, predetermined script and did not include advice, education, or problem-solving. This attention-control approach aligns with recommended procedures in behavioral randomized controlled trials to minimize expectancy and attention bias without introducing active therapeutic elements (Freedland et al., 2011).
RTSS-Based Specification of Components Used in the Lifestyle Intervention and Targets
Note. RTSS = Rehabilitation Treatment Specification System; COHPPE = Client-centered, Occupation-based, Healthy life habits, Protection, Participation, and Evaluation; COPM = Canadian Occupational Performance Measure; RAQoL = Rheumatoid Arthritis Quality of Life Scale; VAS = visual analog scale; BRAF–MDQ = Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire.
Statistical Analysis
We analyzed data by using IBM SPSS Statistics for Windows (Version 22) and assessed normality with the Shapiro–Wilk test. Continuous variables are presented as means (and standard deviations) and categorical variables as sample size (and percentages). We used independent samples t test for between-groups comparisons of normally distributed variables and the Mann–Whitney U test for nonnormal data. We analyzed within-group comparisons across three time points (baseline, postintervention, 6-mo follow-up) by using the Friedman test, with pairwise comparisons conducted via the Wilcoxon signed rank test. Analyses were conducted by using a complete-case approach. Only participants with complete baseline, postintervention, and 6-mo follow-up data were included in longitudinal analyses. No imputation was performed.
Because of limited sample size, categorical variables were described descriptively without inferential testing. Bonferroni correction was applied for multiple comparisons: Within-group analyses involved three comparisons per outcome (α = .05/3, p < .016), and between-groups analyses involved 18 comparisons (6 outcomes × 3 time points, p < .003). Unless otherwise stated, significance was set at p < .05.
Results
Data from 33 participants (LI group: n = 16; control group: n = 17) who completed all assessment timepoints were included in the analyses. Baseline sociodemographic and clinical characteristics are presented in Table 2. No statistically significant between-groups differences were observed at baseline for demographic variables or outcome measures (p > .05).
Comparison of Sociodemographic and Clinical Characteristics Between the Lifestyle Intervention (LI) and Control Groups
Note. Between-groups comparisons were performed by using independent samples t test for normally distributed continuous variables (age, BMI) and Mann–Whitney U test for nonnormally distributed variables (disease duration, COPM, DAS–28, VAS, BRAF–MDQ). Statistical significance was set at p < .05. BMI = body mass index; COPM = Canadian Occupational Performance Measure; DAS–28 = Disease Activity Score–28; VAS = visual analog scale; BRAF–MDQ = Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire.
Between-groups comparisons at baseline, postintervention, and 6-mo follow-up are presented in Table 3. No statistically significant differences were observed at baseline (p > .05). At postintervention, statistically significant differences favoring the LI group were identified in occupational performance and satisfaction (COPM), pain intensity (VAS), fatigue severity (BRAF–MDQ), and health-related quality of life (RAQoL; p < .003, Bonferroni adjusted). These between-groups differences remained statistically significant at the 6-mo follow-up. For disease activity (DAS–28), a statistically significant between-groups difference was observed only at the 6-mo follow-up (p = .002). Within-group changes over time are presented in Table 4 for descriptive completeness. These findings demonstrate statistically significant between-groups differences favoring the LI across multiple patient-reported outcomes at both postintervention and follow-up assessments.
Comparison of Changes in COPM, DAS–28, VAS, BRAF–MDQ, and RAQoL Scores Between Baseline, Postintervention, and 6-Mo Follow-Up in Lifestyle Intervention (LI) and Control Groups
Note. Baseline values are presented in Table 2. Within-group pairwise comparisons between time points (baseline vs. postintervention, baseline vs. 6-mo follow-up, postintervention vs. 6-mo follow-up) were analyzed by using Wilcoxon signed-rank test (p < .016, Bonferroni-corrected). Overall changes over time were analyzed by using Friedman test (p < .05). Boldface indicates statistically significant p values. COPM = Canadian Occupational Performance Measure; DAS–28 = Disease Activity Score–28; VAS = visual analog scale; BRAF–MDQ =Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire; RAQoL = Rheumatoid Arthritis Quality of Life Scale.
Comparison of COPM, DAS–28, VAS, BRAF–MDQ, and RAQoL Scores Between Lifestyle Intervention (LI) and Control Groups at Baseline, Postintervention, and 6-Mo Follow-Up
Note. Between-groups comparisons at baseline, postintervention, and 6-mo follow-up were analyzed by using Mann–Whitney U test. COPM = Canadian Occupational Performance Measure; DAS–28 = Disease Activity Score–28; VAS = visual analog scale; BRAF–MDQ =Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire; RAQoL = Rheumatoid Arthritis Quality of Life Scale.
* p < .003, based on Bonferroni correction.
Discussion
This randomized controlled trial demonstrated that a client-centered LI, based on COHPPE modules and delivered alongside pharmacological treatment, resulted in statistically significant between-groups differences favoring the LI group in occupational performance, pain, fatigue, and health-related quality of life for individuals with RA. These differences were not limited to the immediate postintervention period but were also observed at the 6-mo follow-up, indicating that between-groups differences were maintained over time. The between-groups differences for COPM Performance and Satisfaction may suggest clinical relevance but should be interpreted cautiously. Although a change of at least 2 points on the COPM is often considered clinically meaningful (Law et al., 1990), minimal clinically important differences were not predefined in this study.
Collectively, these findings indicate that a lifestyle-oriented, occupation-based intervention can positively influence patient-reported functional outcomes. In contrast, changes in disease activity were more modest, suggesting that lifestyle-focused occupational therapy interventions may primarily affect functional and experiential outcomes rather than inflammatory disease processes (Gavin et al., 2024; Tonga et al., 2015).
The favorable outcomes observed in this study may be partly attributable to the individualized and client-centered nature of the LI program. Although standardized multidisciplinary group interventions have been shown to yield modest reductions in disease activity, their effects on functional outcomes and fatigue are often limited, potentially because of insufficient personalization (Walrabenstein et al., 2023). In line with findings reported by Tonga et al. (2015), COPM-guided, client-centered interventions may enhance occupational performance and satisfaction by targeting individually meaningful activities, energy management, and home-based strategies, which formed the foundation of the present LI. Integrating joint protection and energy conservation strategies into meaningful occupations may support sustained functional adaptation, consistent with the American College of Rheumatology’s emphasis on a “treat-to-function” approach—that is, aligning disease management with the preservation and optimization of daily functional performance (American Occupational Therapy Association, 2020).
RA disease activity reflects interactions between persistent inflammation and psychosocial stressors, creating a cycle of symptoms and functional limitations (Weyand & Goronzy, 2021). Despite pharmacological advances, 30% to 40% of patients experience residual restrictions even in DAS–28-defined remission (Smolen et al., 2023). Postintervention DAS–28 improvements did not reach statistical significance following correction, whereas the 6-mo assessment revealed sustained reductions, highlighting the multidimensional treatment effects of LI. This delayed response potentially represents cumulative behavioral and psychosocial adjustments. Comparable client-centered approaches document similar patterns of disease activity improvement (Gautam et al., 2022; Kurt et al., 2024; Wagenaar et al., 2024). The eight-session COPPHE protocol targeted multiple domains, including exercise, stress management, sleep hygiene, and joint protection. Although the DAS–28 reduction was modest compared with conventional disease-modifying antirheumatic drug therapy, the sustained nature of this improvement confirms its clinical importance, especially for symptoms with psychosocial mediation or inadequate pharmacological response (Carpenter et al., 2020; Hewlett et al., 2011; Smolen et al., 2023). Lifestyle modification also targets modifiable risk factors implicated in RA pathogenesis (Davergne et al., 2024), consistent with 2024 EULAR physical activity guidelines.
Although mechanisms were not directly assessed, the observed pain reduction may be conceptually consistent with the intervention components. Increased social participation, reduced physical strain through joint protection and energy conservation, and enhanced perceived competence may have contributed to changes in pain experience. In addition, participation-focused and occupation-based elements of the intervention may have supported improved coping, self-efficacy, and engagement, which have been suggested to influence central pain modulation and pain-related fear among individuals with RA (Pope, 2020). Similarly, the substantial improvements observed in fatigue may reflect the combined effects of individualized energy management strategies, enhanced activity organization, and lifestyle balance, as supported by previous research emphasizing the value of comprehensive, person-centered approaches alongside pharmacological treatment (Katz et al., 2018; Kılıç & Parlar Kılıç, 2023). These interpretations remain speculative and should be further examined in future studies designed to explicitly investigate underlying mechanisms.
Significant improvements in quality of life and occupational performance were observed alongside reductions in pain, fatigue, and disease activity. Together, these findings indicate that a structured, occupation-based intervention may support multidimensional health outcomes for individuals with RA. This integrative approach aligns with contemporary guidelines that emphasize individualized, comprehensive, and function-oriented management of RA (England et al., 2023; Smolen et al., 2023; Tian et al., 2024).
Limitations
This study had several limitations. Our sample size estimate was informed by the most conceptually comparable available study reporting within-group effect sizes, because of the limited availability of parallel-group data in the field. Although this approach was justified, effect sizes derived from within-group analyses may not fully reflect between-groups effects in randomized designs. Post hoc analysis confirmed adequate power for the predefined primary endpoint. A slight imbalance in marital status was present between groups, which may have introduced minor residual confounding. The study did not include an active comparison group. Because of the modest sample size, we avoided multivariable adjustment to preserve model stability; therefore, results should be interpreted with caution.
Despite these limitations, the findings suggest that a client-centered, lifestyle-oriented occupational therapy intervention delivered alongside pharmacological treatment may positively influence occupational performance, pain, fatigue, and quality of life of individuals with RA. Observed between-groups differences at postintervention and at the 6-mo follow-up indicate the potential contribution of occupation-based LIs within nonpharmacological management approaches aligned with EULAR recommendations. Future studies should build on these findings by using larger, multicenter designs and mechanistic outcome measures to further clarify long-term effects and underlying pathways.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: Lifestyle-oriented, occupation-based interventions support occupational performance and daily life participation of individuals with rheumatoid arthritis, complementing pharmacological management by addressing functional challenges not fully managed by medical treatment alone. Integrating joint protection and energy conservation strategies into meaningful daily activities helps manage fatigue and pain and facilitates functional adaptation in everyday life. Client-centered goal setting within structured lifestyle interventions promotes engagement and adherence and supports sustainable functional outcomes in routine rheumatology care.
Conclusion
This study supports a client-centered, occupation-based LI as a structured complement to pharmacological RA care. Participants receiving the LI demonstrated greater improvements in occupational performance, pain, fatigue, and quality of life compared with those receiving standard care, with differences maintained at the 6-mo follow-up. Changes in disease activity were more modest, suggesting that lifestyle-oriented occupational therapy interventions may primarily influence functional and experiential outcomes.
Future research should include multicenter designs, active comparator conditions, and extended follow-up periods to further examine long-term effects and generalizability. The structured yet adaptable nature of the LI may offer occupational therapists a practical framework to support meaningful participation in daily life alongside medical management.
Footnotes
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The study was conducted as part of the authors’ academic responsibilities at İzmir Tinaztepe University. Participant recruitment and data collection were carried out at Manisa Celal Bayar University Hospital, following ethical approval by its Faculty of Medicine Ethics Committee (Approval No. E. E.484791). This randomized controlled trial was approved by the Ethics Committee of Manisa Celal Bayar University, Faculty of Medicine (Approval No. E.484791). The study was registered on ClinicalTrials.gov (Registration No. NCT05759585) and conducted in accordance with the Declaration of Helsinki and international scientific and ethical standards.