
Abstract
Importance:
Sleep is a fundamental occupation that supports children’s health and learning and family well-being. Children with Angelman syndrome (AS) experience some of the most severe and persistent sleep disturbances of any neurogenetic disorder, highlighting an underexplored need for nonpharmacological, occupation-centered interventions.
Objective:
To identify and synthesize current knowledge on nonpharmacological sleep interventions for children with AS, describe intervention strategies and reported outcomes, and outline implications for occupational therapy practice.
Data Sources:
We searched Web of Science, APA PsycINFO, PubMed, and CINAHL from inception through September 1, 2025, and reviewed AS foundation websites for gray literature.
Study Selection and Data Collection:
We included studies of nonpharmacological sleep interventions with children with AS. The first author screened titles and abstracts; two reviewers independently screened full texts and charted data using Joanna Briggs Institute and Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews guidance.
Findings:
Three studies were synthesized: one randomized controlled trial, one single-case experimental design, and one case report. Interventions were primarily behavioral or caregiver mediated; one involved a short-term sedative adjunct in a behavioral program. Collectively, these studies demonstrated improvements in sleep initiation, duration, and continuity, and caregivers reported reduced stress and high satisfaction with feasibility.
Conclusions and Relevance:
Behavioral and caregiver-mediated sleep strategies consistently improved children’s ability to fall asleep and remain asleep while supporting family functioning. Findings suggest that sleep is a modifiable occupation and highlight opportunities for occupational therapy practitioners to adapt and deliver family-centered interventions that establish healthy sleep routines and supportive environments.
Plain-Language Summary
Angelman syndrome (AS) is a rare neurodevelopmental condition that often causes severe sleep difficulties among children. Our scoping review looked at strategies to improve sleep for children with AS without using medication and considered their relevance to occupational therapy practice. We identified three studies, and the results were encouraging. The most effective approaches involved establishing consistent bedtime routines, gradually adjusting sleep schedules, and coaching parents to manage sleep behaviors. When these strategies were used, children with AS fell asleep faster, slept longer through the night, and woke up less often. Parents reported less stress and greater confidence in managing their child’s sleep. These nondrug methods are practical for families to use at home and align with occupational therapy’s focus on daily routines, the environment, and family well-being. Occupational therapy practitioners can guide caregivers to create structured, calming bedtime routines that promote better sleep, participation, and overall quality of life.
Positionality Statement
Joseph Barrett is a parent of a child with Angelman syndrome, which informed the motivation for this study but not its examination or interpretation. Shelly J. Lane is a professor in the Department of Occupational Therapy at Colorado State University. Throughout the review, we maintained reflexivity and transparency to support objectivity and methodological rigor. To minimize bias, we used predefined eligibility and data-charting templates, conducted calibration for full-text screening, and resolved discrepancies through consensus.
This scoping review looked at strategies to improve sleep for children with Angelman syndrome without using medication and considered their relevance to occupational therapy practice.
Sleep is a fundamental occupation essential for physical health, cognitive development, emotional regulation, and participation in daily life. Within occupational therapy, sleep is recognized as a restorative process and a critical determinant of occupational performance and well-being (American Occupational Therapy Association [AOTA], 2020). From a Person–Environment–Occupation–Performance (PEOP) perspective, sleep outcomes emerge from dynamic interactions among the person’s intrinsic factors, such as physiology, behavior, and sensory regulation; the environment, such as lighting and temperature; and the occupation of sleep as it is embedded in family and cultural contexts (Baum et al., 2015; Ho & Siu, 2018). This conceptual model highlights that modifying personal habits or environmental conditions can directly influence sleep quality, framing sleep as an activity that can be optimized through therapeutic intervention.
Children with neurodevelopmental disabilities frequently experience disrupted sleep that interferes with self-regulation, learning, and daily routines across settings (Angriman et al., 2015; Heussler, 2016). Among neurodevelopmental conditions, Angelman syndrome (AS) is a rare neurogenetic disorder notable for particularly severe sleep disturbances in addition to hallmark features such as profound developmental delays, motor impairments, seizures, and minimal or absent speech (Buiting et al., 2016; Qu et al., 2024). Clinically, the sleep problems associated with AS are among its most challenging aspects, affecting the child’s participation and daily regulation and family members’ well-being (Mindell & Williamson, 2018; O’Rourke et al., 2024; Trickett et al., 2017, 2019).
Epidemiologic studies indicate that 70% to 80% of children with AS have chronic sleep disturbances (Bruni et al., 2004; O’Rourke et al., 2024; Qu et al., 2024). These disruptions, marked by prolonged sleep onset, frequent night awakenings, and fragmented sleep, lead to behavioral dysregulation among children and elevated levels of caregiver fatigue and stress (Egan et al., 2020; Goldman et al., 2012; Qu et al., 2024; Trickett et al., 2019). In families, poor sleep in a child with AS can cascade into broader effects on parental sleep, mental health, and participation in work and home occupations (Goldman et al., 2012; Heussler, 2016; Trickett et al., 2019). Consequently, addressing sleep has significant implications for child development, caregiver well-being, and family quality of life.
Despite the prevalence and impact of sleep disorders among those with AS, management has traditionally relied on pharmacological approaches. Approximately two-thirds of individuals with AS are reported to use sleep medications (O’Rourke et al., 2024). However, common sleep medications often yield inconsistent results and side effects, leading many caregivers to prefer behavioral and environmental approaches that align with daily routines and occupational participation (Ascoli et al., 2022; O’Rourke et al., 2024). In recent years, emphasis on nonpharmacological interventions as alternatives or complements to medication has been growing (Allen et al., 2013; Bindels-de Heus et al., 2023). These interventions include behavioral and caregiver-mediated strategies such as consistent bedtime routines and parent training (Mindell & Williamson, 2018), complemented by environmental and sensory-based modifications that regulate arousal and support sleep participation (Lane, 2020).
Because sleep is both a biological necessity and a co-occupation involving children and caregivers, meaningful improvement often requires coordinated changes to family routines and environments (Browning et al., 2024). However, the evidence base for nonpharmacological sleep interventions for individuals with AS has not been consolidated to inform clinical practice.
Previous reviews of sleep among those with AS have primarily concentrated on medical treatments or offered only limited insight into behavioral and environmental approaches (Egan et al., 2020; McLay et al., 2019). As a result, clinicians and families lack clear guidance on the range of nonpharmacological strategies available and their potential benefits. Occupational therapy practitioners are ideally suited to address sleep-related participation challenges through behavioral coaching, environmental modification, and caregiver education, approaches grounded in daily routines and co-occupations, yet the evidence base supporting these strategies for children with AS has not been clearly examined (Ho & Siu, 2018).
To address this gap, we conducted a scoping review to map the breadth of available evidence on nonpharmacological sleep interventions for children with AS. This approach was deemed appropriate for broadly surveying the literature, describing the types of interventions and outcomes reported, and identifying remaining knowledge gaps (Arksey & O’Malley, 2005; Levac et al., 2010; Tricco et al., 2018). The review process was guided by the PEOP model to maintain an occupation-centered perspective, viewing sleep as an occupation rooted in the child’s family routines and highlighting its co-occupational nature in caregiving (AOTA, 2020; Baum et al., 2015).
The objective of this scoping review was to identify and synthesize current knowledge on nonpharmacological sleep interventions for children with AS, describe intervention strategies and their reported outcomes for children and caregivers, and outline implications for occupational therapy practice.
Method
Protocol and Design
The review team applied the methodological framework established by Arksey and O’Malley (2005) and refined by Levac et al. (2010). Reporting and synthesis followed Joanna Briggs Institute (JBI) guidance for scoping reviews (Peters et al., 2020) and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018). The protocol was preregistered on the Open Science Framework (https://doi.org/10.17605/OSF.IO/35CNJ) before data collection. Covidence was used to manage screening and data extraction. The PEOP model guided the interpretation of findings to maintain an occupation-centered perspective (AOTA, 2020; Baum et al., 2015). We selected the PEOP model because it explicitly links person factors, environmental context, and occupations, which matches the caregiver-mediated and routine-based mechanisms emphasized in the included interventions and supports the interpretation of sleep as a family-embedded occupation.
Eligibility Criteria
Eligibility was established using the population–concept–context framework (Peters et al., 2020).
Population: Children and adolescents (0–18 yr) with a confirmed diagnosis of AS. Studies with mixed neurodevelopmental samples were eligible if AS data were isolatable. When AS data could not be isolated but the study included at least one participant with AS, the record was retained for contextual interpretation only and did not contribute to numerical tallies or synthesis counts.
Concept: Nonpharmacological sleep interventions, including behavioral, caregiver-mediated, sensory–environmental, mind–body, or multicomponent approaches in which behavioral strategies were the primary mechanism of change.
Context: No geographic restrictions; settings included home, clinic, school, and community environments.
Exclusion criteria were nonhuman or adult-only studies, pharmacological-only interventions, studies lacking measurable sleep outcomes, and nonintervention articles (reviews or commentaries). Only English-language literature was included. Studies using short-term medication adjuncts in primarily behavioral programs were eligible.
Information Sources and Search
The review team collaborated with a university research librarian to develop and implement a comprehensive search strategy across the Web of Science, APA PsycINFO, PubMed, and CINAHL databases from inception through September 1, 2025. A three-tiered approach was used: initial broad identification searches (Tier 1), focused refinement (Tier 2), and final targeted searches (Tier 3). The finalized Tier 3 strategies combined controlled vocabulary and free-text keywords related to Angelman, sleep, and intervention. Gray literature sources included the Angelman Syndrome Foundation (https://angelman.org) and the Foundation for Angelman Syndrome Therapeutics (https://cureangelman.org). Zotero was used for citation management, and Covidence was used to organize deduplication and screening. Complete Tier 3 search strings, databases, dates, and retrieval counts are provided in Table A.1 in the Supplemental Material (available online with this article at https://research.aota.org/ajot).
Selection of Evidence Sources
Joseph Barrett conducted title and abstract screening because of the limited number of eligible records and the time constraints of the project, with secondary oversight introduced during full-text screening to enhance reliability and consistency. Joseph Barrett and a second independent reviewer screened full-text articles after calibration and training on inclusion and exclusion criteria. Each reviewer jointly reviewed two full-text studies to align screening decisions and ensure reliability, followed by three independent practice screenings to verify consistency. The remaining full texts were reviewed independently, and discrepancies were resolved through discussion and consensus.
Reasons for exclusion at the full-text level included adult-only samples, lack of intervention or sleep outcomes, or only pharmacological treatment. Given the rarity of AS-specific research, one study in which AS data could not be isolated was retained solely for contextual interpretation. This approach provided broader insight into behavioral sleep strategies across neurodevelopmental disorders.
A total of 1,555 records were identified, 1,183 duplicates were removed, 372 titles and abstracts were screened, and 27 full texts were reviewed; 4 studies met the inclusion criteria. As noted, AS-specific data could not be isolated in one study (Woodford et al., 2025); thus, three studies contributed to the synthesis. We did not contact the study authors to request disaggregated AS-specific outcome data. The selection process is illustrated in the PRISMA-ScR flow diagram (Figure 1).
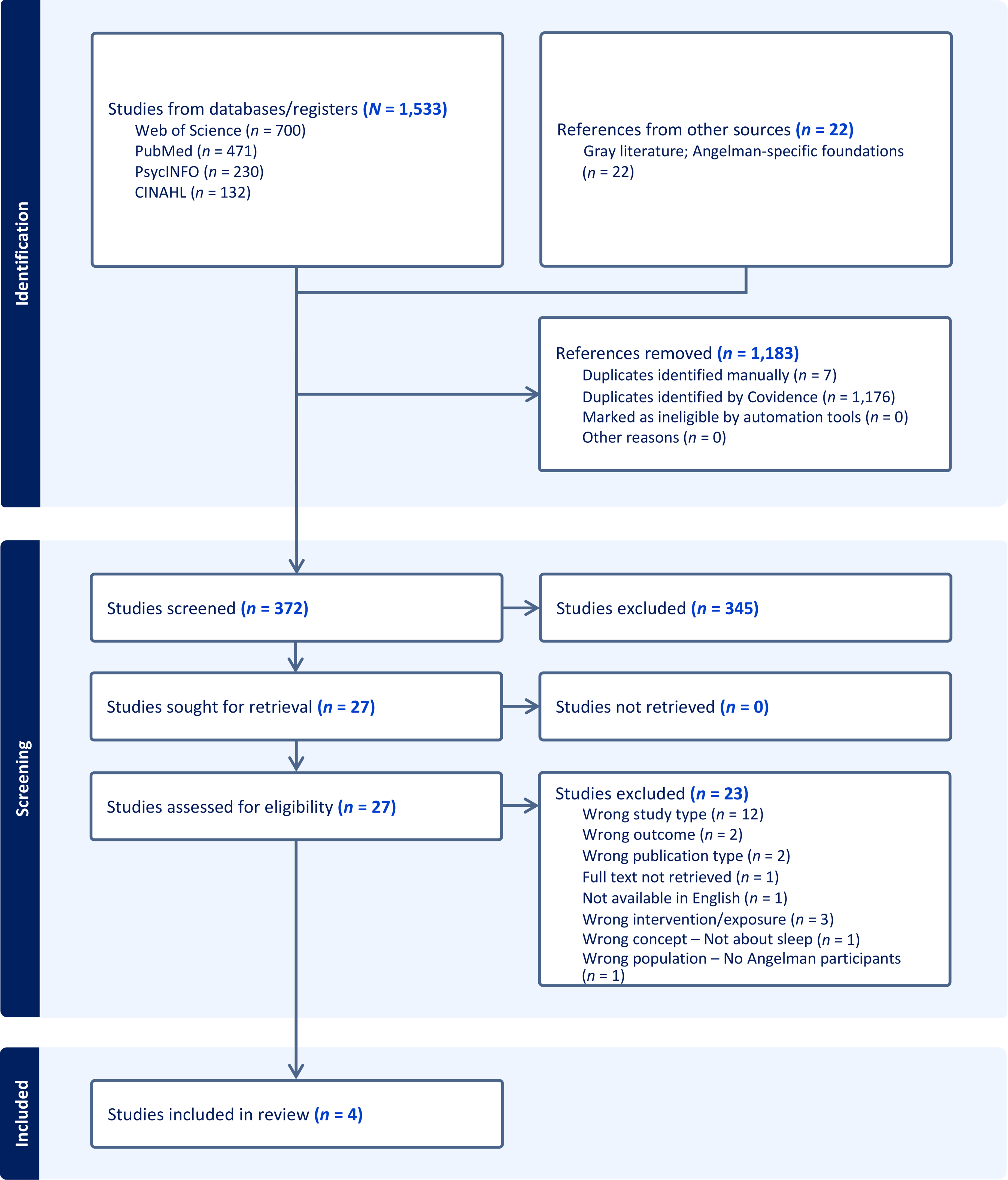
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-SCR) flow of study selection process.
Data Charting Process and Data Extraction
After study selection, Joseph Barrett and a second reviewer independently charted data using a standardized template adapted from the JBI (Peters et al., 2020). Extracted variables captured citation details, country, setting, study design, participant demographics, intervention characteristics, sleep and caregiver outcomes, and occupational therapy relevance. The reviewers compared and reconciled entries through discussion to achieve consensus. Variables, definitions, and purposes are detailed in Table A.2 in the Supplemental Material; study-level information appears in Table A.3.
Data Synthesis
We conducted a descriptive narrative synthesis consistent with JBI guidance, mapping the evidence without formal critical appraisal or strength-of-evidence ratings (Peters et al., 2020). Quantitative pooling was not appropriate because of heterogeneity in design and outcomes. We grouped findings by intervention type (behavioral, environmental, or sensory; caregiver mediated; or multicomponent) and by outcome domain (child and caregiver). Occupational therapy relevance was interpreted by examining how interventions addressed routines, environmental adaptation, and caregiver participation, consistent with the PEOP framework.
Results
Overview of Included Studies
We identified four studies that met inclusion criteria; three were synthesized (Allen et al., 2013; Bindels-de Heus et al., 2023; Summers et al., 1992), representing a small but growing evidence base on nonpharmacological sleep interventions for children with AS. The included studies consisted of one randomized controlled trial (RCT; Bindels-de Heus et al., 2023), one single-case experimental design (SCED) using multiple baselines across participants (Allen et al., 2013), and one case report (Summers et al., 1992), encompassing 26 participants with confirmed AS. Participants ranged in age from 2 to 18 yr, with both sexes represented. The three studies that were synthesized focused exclusively on AS; the fourth (Woodford et al., 2025) included a sample with mixed neurodevelopmental disorders in which the AS case could not be isolated. We retained this record for contextual interpretation only and excluded it from the synthesis. Details for this contextual source are provided in Table A.4. Collectively, the included studies reported improvements in child sleep parameters and family functioning after structured behavioral routines and caregiver coaching (Allen et al., 2013; Bindels-de Heus et al., 2023; Summers et al., 1992).
The three synthesized studies targeted sleep onset, maintenance, and total sleep duration (Allen et al., 2013; Bindels-de Heus et al., 2023; Summers et al., 1992). Summers et al. (1992) incorporated short-term pharmacological support into a combined behavioral program while maintaining a behavioral focus. Interventions were delivered in home contexts (Allen et al., 2013), in home and clinic contexts (Bindels-de Heus et al., 2023), and in the hospital with subsequent home implementation (Summers et al., 1992). Feasibility and acceptability were explicitly reported by Allen et al. (2013) and Bindels-de Heus et al. (2023).
Intervention Characteristics
Intervention duration was 4 wk in the SCED by Allen et al. (2013), 12 wk in the RCT by Bindels-de Heus et al. (2023), and 7 wk of inpatient treatment in the case report by Summers et al. (1992). Follow-up assessments occurred at 1 and 3 mo in Allen et al. (2013), at 3 mo in Bindels-de Heus et al. (2023), and at 45 days in Summers et al. (1992). Intervention components varied by study. Allen et al. (2013) implemented a behavioral treatment package that included bedtime fading, graduated withdrawal of nighttime attention, and reinforcement of independent sleep. Bindels-de Heus et al. (2023) delivered a structured behavioral sleep program that emphasized consistent bedtime routines and parent training and included strategies to address night awakenings. Summers et al. (1992) used a combined behavioral and pharmacological program centered on sleep–wake scheduling and behavioral routine implementation, supported by a short-term sedative adjunct. Caregiver training and treatment support were delivered remotely by Allen et al. (2013), using video telehealth connections at clinics proximal to families when available or phone contact when not. Bindels-de Heus et al. (2023) also incorporated structured parent training delivered through clinic-based sessions with remote support. In contrast, Summers et al. (1992) described behaviorally oriented sleep–wake schedule management implemented during inpatient hospitalization with subsequent caregiver implementation at home after discharge.
Outcome measures varied across studies. Allen et al. (2013) used parent sleep diaries and actigraphy to quantify sleep and bedtime or nighttime behavior, as well as caregiver questionnaires (Children’s Sleep Habits Questionnaire [CSHQ]; Developmental Behavior Checklist) and treatment acceptability ratings. Bindels-de Heus et al. (2023) assessed sleep using a multimethod package consisting of a sleep diary, actigraphy, and home videosomnography and measured sleep severity with the Composite Sleep Index. Secondary outcomes incorporated by Bindels-de Heus et al. (2023) included parent sleep diary parameters and standardized measures, including the Children’s Sleep Hygiene Scale, Parenting Stress Index, Infant-Toddler Quality of Life, and 36-item Short Form Health Survey. Summers et al. (1992) measured sleep using 24-hr sleep logs or recordings.
Study-Level Findings
Summaries of individual study findings are available in Table A.3. In all three studies, structured behavioral and caregiver-mediated programs improved nighttime sleep duration and reduced awakenings, with sustained benefits at follow-up (Allen et al., 2013; Bindels-de Heus et al., 2023; Summers et al., 1992).
Child Outcomes
In each investigation, researchers reported improvements in children’s sleep parameters, most pronounced in sleep onset latency, night awakenings, and total sleep duration. Bindels-de Heus et al. (2023) demonstrated meaningful increases in total sleep time and sleep efficiency for the intervention group, confirmed by actigraphy. Allen et al. (2013) documented stable gains in independent sleep onset and sustained reductions in night awakenings over time.
Caregivers in two studies (Allen et al., 2013; Bindels-de Heus et al., 2023) reported better daytime alertness, emotional regulation, and engagement in daily routines after treatment. Although these reports included observations of improved child engagement and regulation, such participation outcomes were not directly measured.
Caregiver Outcomes
Caregiver perspectives were described in all three studies, although measurement approaches varied. Allen et al. (2013) and Bindels-de Heus et al. (2023) reported improvements in caregiver management of bedtime routines after the intervention, with Bindels-de Heus et al. (2023) documenting changes in caregiver vitality and parental impact using standardized questionnaires, and Allen et al. (2013) reporting caregiver ratings of the behavioral program’s feasibility and acceptability. Summers et al. (1992) provided narrative descriptions of changes in family sleep routines and caregiver functioning but did not include formal caregiver-reported outcome measures.
Discussion
In this scoping review, we present the first synthesis of nonpharmacological sleep interventions for children with AS through an occupational therapy lens, showing that behavioral and caregiver-mediated interventions were feasible for home use and improved sleep initiation and family well-being (Allen et al., 2013; Bindels-de Heus et al., 2023; Summers et al., 1992). Because only three studies contributed to the synthesis, this review’s contribution is not to establish effectiveness with confidence but to consolidate what has been studied, identify consistent intervention components, and clarify where evidence is absent. Across heterogeneous designs, the studies converged on behavioral and caregiver-mediated strategies that targeted routines, caregiver implementation, and the home context. At the same time, the evidence base is characterized by small samples, variability in measurement approaches, and limited attention to occupation-centered outcomes. This synthesis therefore provides a preliminary summary of sleep interventions for AS that occupational therapy practitioners and researchers should interpret cautiously. Moving forward, future research that better reflects occupational performance, participation, and family routines will provide additional guidelines for occupational therapy interventions.
Examination of the included evidence revealed three consistent patterns: Behavioral and caregiver-mediated interventions were effective and feasible for home use, improving sleep quality and caregiver satisfaction. Environmental and routine-based strategies, such as consistent bedtime cues, minimizing sensory stimulation, and establishing structured daily schedules, were critical for success. Caregiver participation was the essential mechanism of change, indicating that family coaching and education were equally as influential as the behavioral techniques themselves (Allen et al., 2013; Bindels-de Heus et al., 2023; Summers et al., 1992).
Although the evidence base remains quite small, these findings mirror the broader pediatric sleep literature, which identifies behavioral and routine-based interventions as first-line approaches for childhood insomnia and bedtime resistance (Mindell & Williamson, 2018). More important, the interventions identified in this review parallel occupational therapy principles emphasizing environmental fit, structured daily routines, and family-centered practice (AOTA, 2020; Baum et al., 2015). However, occupational therapy practitioners did not deliver any of the included interventions, so their direct effectiveness in occupational therapy practitioner–led practice remains to be established.
Mechanistically, improvements were most plausibly driven by predictable routines, reduced arousal from environmental cues, and reinforcement of independent sleep behaviors (Mindell & Williamson, 2018; Pudasainee-Kapri et al., 2025). Viewed through the PEOP lens, change occurred through alignment of person factors (arousal and behavioral readiness) and environmental factors (light, noise, temperature, sensory load), as well as the occupation of sleep (sequencing and timing of the routine).
Caregiver participation consistently emerged as a central determinant of intervention success. Parents who received structured coaching demonstrated greater adherence to behavioral plans and sustained improvements beyond the intervention period (Bindels-de Heus et al., 2023). This reinforces the concept of co-occupation in pediatric occupational therapy, where caregiver involvement is both the means and the outcome of effective intervention (AOTA, 2020). Our review indicates that family-implemented behavioral programs may improve child sleep and caregiver well-being, consistent with the interdependent nature of co-occupation and family routines emphasized in occupational therapy.
Relevance to Occupational Therapy
Although behavioral procedures often originate outside occupational therapy, their focus on routines, environmental context, and caregiver collaboration closely aligns with occupation-centered practice. We noted strong conceptual alignment between behavioral sleep interventions and occupational therapy frameworks, which underscores how changes in routines and environments can influence participation and well-being.
From an occupational therapy perspective, these findings position practitioners to extend behavioral principles in holistic, family-centered interventions that promote rest and co-occupational balance. Integrating sensory and environmental knowledge along with behavioral coaching offers a comprehensive pathway to support sleep regulation and family resilience for children with AS, drawing on broader pediatric evidence showing that multimodal, context-focused interventions improve sleep and daily participation for children with neurodevelopmental challenges (Hartman et al., 2022; Mindell & Williamson, 2018; Phillips et al., 2020). Although not included in the synthesis, findings from Woodford et al. (2025) further contextualize this evidence by demonstrating similar benefits of behavioral sleep interventions across rare neurodevelopmental disorders, reinforcing their potential relevance to occupational therapy practice for children with AS. Expanding this integrated role can strengthen occupational therapy’s contribution to health promotion for, caregiver education on, and family-centered outcomes in neurogenetic conditions (AOTA, 2020).
Limitations
We followed a rigorous and transparent methodology consistent with JBI and PRISMA-ScR standards, including protocol preregistration, dual screening, and detailed data charting (Peters et al., 2020; Tricco et al., 2018). These processes increase confidence in the accuracy and reproducibility of the findings. Although we applied the PEOP model to guide our interpretation, we did not conduct formal theoretical mapping or codebook-based theory assignment.
We identified several limitations of this review. Title and abstract screening was conducted by a single reviewer, which may have introduced selection bias despite subsequent verification and consensus during full-text review. The small number of available studies and predominance of single-case and case-report designs limits generalizability (Allen et al., 2013; Summers et al., 1992). Heterogeneity in intervention formats, measures, and participant characteristics precluded quantitative synthesis. Only English-language studies were included, and one potentially relevant thesis could not be retrieved. In addition, one pooled single-case series included a participant with AS whose data could not be isolated, and we did not pursue author contact to obtain disaggregated outcomes; this source was retained for contextual interpretation only and not for synthesis (Woodford et al., 2025). None of the identified interventions were led by occupational therapy practitioners, and no standardized measures of occupational performance or participation were used. As a result, conclusions about the direct effectiveness of occupational therapy must be inferred conceptually rather than empirically.
Methodological and conceptual limitations further constrain interpretation. None of the studies incorporated occupation-centered or participation-based outcome measures, such as the Canadian Occupational Performance Measure (Law et al., 2019) or the Participation and Environment Measure for Children and Youth (Coster et al., 2012). Consequently, the broader impact of improved sleep on daytime functioning, family engagement, and caregiver occupational balance remains underexplored. Similarly, sensory-based and environmental interventions, core areas of occupational therapy, were rarely isolated or evaluated independently, limiting understanding of their specific contributions to sleep regulation in AS.
Given the rarity of AS and the early stage of nonpharmacological research with this population, the small number and heterogeneity of studies reflect the current state of the evidence rather than a limitation of the review process. Consolidating this early work establishes a necessary foundation for future empirical and occupational therapy–led investigations that integrate behavioral and caregiver-mediated approaches within occupation-centered frameworks.
Implications for Occupational Therapy Research
Future studies should expand the evidence base through multisite collaborations and mixed-methods designs, and they should include standardized measures capturing sleep and participation outcomes. Additional nonpharmacological approaches that align with occupational therapy practice warrant direct evaluation for individuals with AS because they were not represented in the included studies. These approaches include sensory–environmental adaptations intended to support arousal regulation at bedtime, occupation-based daytime activity, routine interventions that may influence sleep pressure and circadian timing, and caregiver coaching models embedded in natural family routines.
Integrating validated sleep measures such as actigraphy and the CSHQ (Owens et al., 2000) with occupation-based tools would provide a comprehensive understanding of how improved sleep contributes to daytime engagement, co-occupation, and caregiver well-being (Bindels-de Heus et al., 2023). Researchers should consider the heterogeneity of abilities and developmental levels of people with AS and include occupational therapy practitioners as coinvestigators or interventionists to strengthen integration of sensory, behavioral, and environmental strategies consistent with the PEOP model (Baum et al., 2015). A pragmatic, occupational therapy practitioner–led pilot integrating behavioral routines with individualized sensory–environmental adaptations and measuring sleep and participation outcomes is a logical next step.
Implications for Occupational Therapy Practice
The evidence supports practical ways occupational therapy practitioners can integrate sleep promotion into everyday practice for children with AS and their families. This review has the following implications for occupational therapy practice: Practitioners should partner with caregivers and provide structured guidance through sessions that model behavioral techniques, such as bedtime fading, graduated response, and reinforcement of independent sleep, to support consistency and build caregiver confidence. Predictable bedtime routines should be established. Practitioners can collaborate with caregivers to design calming, consistent presleep sequences and sleep–wake schedules that align with the child’s sensory and behavioral needs. Practitioners should recommend simple, individualized modifications in lighting, sound, temperature, and sensory inputs that promote rest and sustained sleep.
Conclusion
We met this scoping review’s objective by identifying and synthesizing the small but promising evidence on nonpharmacological sleep interventions for children with AS. Across three studies, behavioral and caregiver-mediated programs consistently improved children’s ability to fall asleep and remain asleep while reducing caregiver stress and increasing confidence in managing bedtime routines. These interventions were feasible for home implementation and well accepted by families, suggesting that sleep behaviors in AS are modifiable.
The reviewed studies demonstrated that aligning routines, environments, and caregiver participation improved sleep initiation, maintenance, and caregiver well-being. Viewed through the PEOP model, occupational therapy practitioners can interpret these findings as indicating that structuring routines and adapting environments may support rest, regulation, and family balance. Occupational therapy practitioners can collaborate with caregivers to create conditions that may promote rest and support occupational balance across the family system.
Footnotes
*
Indicates studies included in the scoping review.
Acknowledgments
Joseph Barrett thanks Jaewon Kang, PhD, OTR/L, for serving as faculty advisor and Erica Clewett, OTD student, for serving as a second reviewer.