
Abstract
Occupational therapy practitioners may encounter challenges when they try to incorporate evidence into practice. To embrace evidence-based practice (EBP), clinicians must have readily available, relevant, and concisely summarized evidence. Although researchers have described the importance and process of EBP, less has been written about how to efficiently integrate evidence into practice. Clinicians may benefit from examples of reasoning, strategies, and resources to successfully integrate evidence. This article reviews the steps of EBP and offers recommendations to overcome common barriers. For EBP to become integrated into practice, greater communication and collaboration among all stakeholders must occur. EBP and knowledge translation require multiple processes and coordinated efforts. Therefore, everyone from practitioners to employers has a role in increasing EBP and transferring knowledge for practice. To encourage discussion and actions, the article provides implications and recommendations for practitioners, researchers, educators, organizations, and policymakers.
Keywords
Many health care professionals have identified the steps for evidence-based practice (EBP; Bliss-Holtz, 2007; Corcoran, 2006; Tickle-Degnen, 2000a), but a critical part of the process is actual implementation of EBP at the point of care. Currently, a 17-year lag exists between evidence and practice (Clancy & Cronin, 2005) that is likely the result of many clinician barriers, including lack of time, resources, or training to locate and appraise research studies (Grol & Grimshaw, 2003). Moreover, clinicians may not receive support from their practice setting to incorporate evidence into practice.
Implementing EBP has become a priority in the health care professions. Changes in how health care is administered (e.g., increasing costs, reduced staffing, managed care systems, and shorter hospital stays) have increased clinicians’ accountability to provide EBP (Holm, 2000; Stube & Jedlicka, 2007). Because clinicians are under more pressure to justify the services they provide, not being able to use research evidence in practice may affect reimbursement and reduce the scope of practice in a variety of settings (Murphy & Lin, 2002), which in turn could decrease staffing levels and services provided.
Occupational therapy associations and organizations have responded by creating new resources and learning materials for EBP, such as OTseeker (www.otseeker.com), an online database of systematic reviews, and randomized controlled trials (Bennett, Townsend, Mancini, & Taylor, 2006). The American Occupational Therapy Association has produced many systematic reviews (see, e.g., Case-Smith & Arbesman, 2008; Hunt & Arbesman, 2008), has created an online EBP Resource Directory, and has featured EBP resources or information in OT Practice (Scheer, Arbesman, & Lieberman, 2008) and the 1-Minute Update e-newsletter.
However, focusing on evidence dissemination is not enough, because even robust evidence is insufficient to facilitate change in practice patterns (Dopson, FitzGerald, Ferlie, Gabbay, & Locock, 2002). A survey on how to better implement EBP revealed that most occupational therapists wanted short continuing education sessions, brief written information, and Web-based resources (Bennett et al., 2003). Yet research has suggested that passive forms of EBP training are not as effective as interactive workshops, educational outreach by clinical experts, and practice-based learning groups (Davis, Thomson, Oxman, & Haynes, 1995). Occupational therapists in Canada have pioneered many knowledge exchange and translation methods such as online communities of practice and community-based educational outreach (Law, Missiuna, & Pollock, 2008). Although many descriptions and examples of EBP have been published (Bailey, Bornstein, & Ryan, 2007; Holm, 2000; Law, 2000), clinicians may benefit from updated strategies and resources to successfully and efficiently integrate evidence into daily practice.
In this article, we outline the EBP process and suggest solutions to common challenges, describing strategies, decision making, and resources so that clinicians can be more successful when they search, appraise, and interpret evidence. Acknowledging that many occupational therapists do not have the same level of access to research articles as researchers and educators (Stube & Jedlicka, 2007), we identify resources for accessing and appraising research. Finally, we offer a summary of the challenges to EBP and recommendations for all stakeholders (educators, clinicians, researchers, organizations, and policymakers) to stimulate discussion and engender collaborative relationships.
Steps of Evidence-Based Practice
The EBP process has five basic steps: (1) formulating the clinical question, (2) searching efficiently for the best available evidence, (3) critically analyzing evidence for its validity and usefulness, (4) integrating the appraisal with personal clinical expertise and clients’ preferences, and (5) evaluating one's performance or outcomes of actions (Straus, Richardson, Glasziou, & Haynes, 2005). A sixth step, disseminating and communicating knowledge, was added later (Law, MacDermid, & Telford, 2007) so that the entire profession benefits. Although these steps appear straightforward, clinicians may encounter challenges at each step. As we review these steps, it may be helpful to consider examples, strategies, and resources to help transform EBP from an idea to a reality.
Step 1: Formulating the Clinical Question
New clinicians or clinicians who have switched to a new practice area frequently ask background questions, or questions that refer to general aspects of a phenomenon (i.e., who, what, where, when, how, and why; Sackett, Straus, Richardson, Rosenberg, & Haynes, 2000). For example, in working with a client diagnosed with a rare disorder, the clinician unfamiliar with this disorder may ask a broad question such as “What is occupational therapy's role with people who have this disorder?”
Experienced clinicians tend to ask foreground questions, specific questions that affect treatment (Onady & Raslich, 2003). Such questions usually follow a format called PICO, specifying a patient or problem, intervention, comparison intervention (if relevant), and outcome (Glasziou, Irwig, Bain, & Colditz, 2001; Institute of Medicine, 2008). The most efficient method of answering foreground questions is to find a relevant systematic review (SR) or meta-analysis. If no SR for the clinical question exists, clinicians can either look for intervention studies and single-subject–design studies, in which the participants serve as their own control, or conduct their own SR. Several resources are available for clinicians conducting a SR (Glasziou et al., 2001; Wright, Brand, Dunn, & Spindler, 2007). Partnerships between clinicians and academicians are recommended to conduct SRs that not only answer relevant clinical questions but are also of high quality.
Formulating a good clinical question depends on the purpose behind the question. If a clinician is asking a background question, the question may be broad or open ended. However, if the clinician is asking a foreground question, using the PICO format facilitates asking a focused, clinically relevant question by specifying the four components: patient, interventions, comparison group, and outcomes (Counsell, 1997). Evidence from a well-formulated research question will provide useful information for practice, whereas a search based on a weak clinical question may yield vague conclusions, limiting its applicability in practice (Onady & Raslich, 2003).
Step 2: Searching Efficiently for the Best Available Evidence
Clinicians may have limited time and resources to search for the best available evidence, so searching for reviews from trustworthy sources is an efficient strategy. Different types of reviews provide different information. If a clinical question is broad, narrative reviews, qualitative studies, and observational research may be helpful. If the question concerns intervention effectiveness (e.g., does treatment A affect outcome B?), then a traditional SR is considered the best approach to evaluating evidence.
SRs refer to “an extensive, systematic process of identifying, appraising, and summarizing all research on the review topic” (Evans & Kowanko, 2000, p. 35) and may contain a quantitative synthesis of study results, such as in the case of a meta-analysis. In terms of research quality, a well-conducted SR is stronger than a narrative review. One distinguishing characteristic of SRs is a method section describing the criteria for searching and selecting studies.
Narrative reviews are useful if a clinician asks a broad practice question, such as understanding a particular diagnosis or therapeutic treatment if few studies exist or if existing studies are flawed (Cook, Mulrow, & Haynes, 1997). In contrast to SRs, narrative reviews are less focused on a specific clinical question; often do not use literature that was sought in a systematic, reproducible manner; and may be influenced by author bias (Montori, Swiontkowski, & Cook, 2003). Thus, relying solely on narrative reviews for practice decisions may lead to incorrect conclusions regarding best practices (Montori et al., 2003; Wright et al., 2007).
Other useful sources of evidence are practice guidelines or clinical guidelines, which often incorporate SRs. A practice guideline can be viewed as an “amalgam of clinical experience, expert opinion, and research evidence” and can be helpful to the busy clinician by distilling evidence into practice recommendations (Cook, Greengold, Ellrodt, & Weingarten, 1997, p. 210). Other popular review formats are critically appraised topics and critically appraised papers, which are brief summaries and appraisals of a specific question or study (Law et al., 2007).
If clinicians cannot locate a review to answer their clinical question, then they may consider conducting their own review of the evidence. However, a significant barrier to EBP is that clinicians may lack access to the literature. Fortunately, an increasing number of medical journals and SRs are accessible online (Goldstand, 2006; Law et al., 2007). Although some Web sites list free journals or articles, these lists do not represent all journals available, so one should search carefully for relevant sources.
Clinical Example
We now consider an example of the first two steps of EBP, formulating the clinical question and searching for evidence. An occupational therapist working in an outpatient rehabilitation setting has finished evaluating a woman with rheumatoid arthritis (RA). If this diagnosis is unfamiliar to the therapist, she might start by asking background questions such as “What interventions do occupational therapists typically use with people who have RA?” Narrative reviews, case studies, and qualitative studies can describe interventions but generally do not answer questions about their effectiveness. If the occupational therapist could not find literature about interventions for people with RA, she might expand the diagnostic category to include arthritis or autoimmune disorders. By broadening her search, she can then determine which interventions were used for which symptoms and design an intervention plan.
If the occupational therapist is more experienced or familiar with RA, she may ask more foreground questions. For example, she may ask a PICO question—“Is there evidence to support the use of splints to increase daily functioning in adults with RA?” She could search the Cochrane Library's Web site, typing in rheumatoid arthritis and finding 59 reviews. Browsing the list, she would find a review called “Splints and Orthosis for Treating Rheumatoid Arthritis” (Egan et al., 2001) and learn that there is insufficient evidence to support splint use to increase function for people with RA. Although many adverse effects have not been reported, such as decreased range of motion (ROM), a risk is that some splints decrease grip strength and dexterity. The review also states that resting hand and wrist splints do not seem to affect ROM, although participants preferred wearing a resting splint to no splint. After discussing the review with her client, the occupational therapist fabricates a resting hand splint to be worn during sleep because the therapist was concerned about the possibility of decreased grip strength and dexterity.
Step 3: Critically Analyzing the Evidence for Its Validity and Usefulness
The third step is to critically evaluate the evidence by analyzing the research design and determining whether the evidence yielded has high internal and external validity. Internal validity refers to the strength and quality of the research design and method and whether the outcomes are unlikely to be caused by extraneous variables (Black, 1999). EBP and clinical guidelines are based on a research hierarchy in which articles that have high levels of internal validity are most important to treatment recommendations. For example, randomized controlled trials are rated as providing the highest levels of evidence because they have high internal validity as a result of their design, randomization, existence of a control group, and tight control of the intervention. However, with high internal validity, external validity or generalizability is weaker. Frequently, studies with high levels of internal validity are difficult to translate into a setting with different clients and may not be as relevant to clinicians seeking treatment options for a specific client problem.
In Step 3, the critical appraisal of the evidence involves asking questions regarding how trustworthy the findings are or whether they could be the result of error (see Figure 1). To integrate evidence into practice, clinicians should determine whether the findings are clinically useful by differentiating between statistical significance and clinical significance. Often researchers note that a certain statistical test was significant, with p < .05. However, the p value indicates the likelihood that a finding was the result of chance, not clinical significance. For example, if a study found that a new intervention resulted in increased shoulder ROM in adults who recently had a cerebrovascular accident compared with standard therapy, and this increase was statistically significant, clinicians may be interested in learning more about this new therapy. However, a closer examination of the study may reveal that the new intervention requires expensive equipment and the average gain in ROM was only 3°. In other words, the results are not clinically meaningful and may not justify the expense.
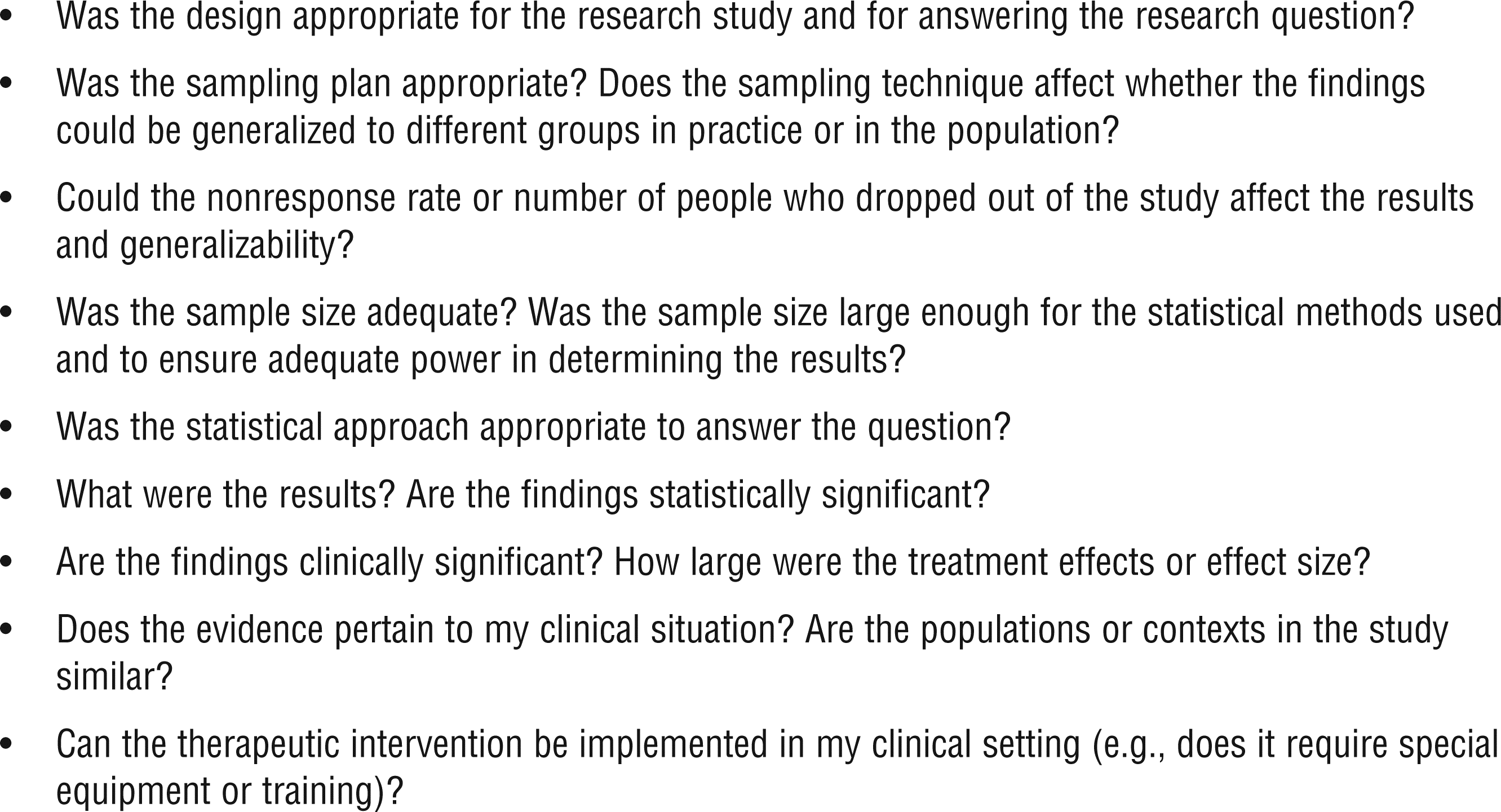
Guide to evaluating research evidence: Guiding questions.
Although some clinicians may find this step of EBP daunting, many resources are available to help them appraise the evidence (see Table 1). Clinicians may form journal clubs, contact nearby occupational therapy programs, or use research groups and online forums to learn more about evaluating research (Craik & Rappolt, 2003).
Resources to Appraise Evidence
Step 4: Integrating the Appraisal With Personal Clinical Expertise and Client's Preferences
One common misperception of EBP is that the quest for answers or treatment decisions ends with the research results. However, best practice requires three critical ingredients: (1) best available external evidence; (2) clinical expertise; and (3) consideration of client's contexts, rights, and preferences (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Occupational therapists, like other health care providers, tend to base clinical decisions on experience, continuing education, and colleagues’ advice (Bennett et al., 2003). Clinical expertise plays an important role for several reasons. First, evidence to support a particular intervention for a particular client in a particular setting may not exist. Second, if evidence exists and the results are conflicting, or if clients’ preferences differ from the recommended intervention, clinical knowledge can help construct a coherent meaning and determine how best to proceed (Tickle-Degnen, 2000b). Finally, research and systematic reviews are not infallible; the process may contain flaws or bias. Clinicians and clients need to feel empowered not only to understand and use research but also to reject or dispute existing findings. This critical step differentiates research use from EBP; the former focuses on applying research findings and the latter is a tailored, client-centered approach based on integrating best evidence with professional judgment and expertise and with client preferences.
Step 5: Evaluating One's Performance or Outcomes of Actions
One of the final steps in the EBP process includes reflection on the process (Straus et al., 2005) or outcomes (Law et al., 2007). How efficiently and effectively did the clinician follow the EBP steps? What effect did the intervention yield? How does the intervention compare with others? If a new intervention is easier to implement but does not adequately improve clients’ functional outcomes, then clinicians may want to return to the standard intervention.
Step 6: Disseminating and Communicating Knowledge
Students, clinicians, and researchers who have performed a SR or developed EBP tools could greatly contribute to the profession's knowledge base by communicating the results to colleagues (Law et al., 2007). After prominent researchers and leaders met in a 2004 International Conference on Evidence-Based Occupational Therapy (Ilott, Taylor, & Bolanos, 2006) sponsored by the American Occupational Therapy Association and the American Occupational Therapy Foundation, the Evidence-Based Occupational Therapy Web portal (www.otevidence.info/) was created on the World Federation of Occupational Therapists’ Web site. This portal provides access to strategies, knowledge, and many resources to promote and facilitate EBP. Although the online resources developed by many countries and organizations are promising, clinicians still find it cumbersome to search through each resource. If the reviews were standardized and placed in a centralized repository with a search feature, clinicians, educators, students, and consumers would benefit.
One challenge for occupational therapy practice and incorporation of EBP principles is the possibility that some clinicians may not understand the goal and steps of EBP. Even when clinicians try to implement EBP, they may become uncertain or discouraged at any of the steps, (e.g., formulating a focused question, searching and evaluating the research literature or presenting their knowledge to others).
Challenges to Moving Evidence Into Practice
One challenge that faces the profession is development of a unified research agenda and strategic plan. For occupational therapy research to advance the profession globally, an ongoing systematic scan of the research is needed at the policy, practice, and theoretical levels to address the critical gaps in the profession's knowledge base. Occupational therapists or organizations that conduct a SR can communicate these gaps in knowledge to researchers, educators, students, and clinicians so that our research efforts are both effective and efficient.
Other challenges to EBP are aligning clinicians’ research questions, researchers’ expertise, and research funders’ priorities. Ideally, research should be relevant to practice, and grantors should be aware of “bottom-up” research needs. For example, an occupational therapist working with a child with autism observes that his sensory defensive behaviors are disrupting the class and interfering with his ability to learn and perform tasks. The clinician searches for literature about interventions to promote adaptive behaviors in the classroom. If the occupational therapist finds several studies but they were not well designed, an opportunity exists for collaboration between researchers and clinicians. If clinicians are engaged in research and observe how research answers their questions and improves their clients’ outcomes, clinicians may be more likely to incorporate research into their clinical reasoning and client discussions. Ideally, funding for research would address these critical knowledge gaps.
Using clinical experts to model or promote how to use evidence for specific practice areas can help bridge the divide between evidence and practice. Scott et al. (2007) described effective knowledge translation strategies that included (1) bringing interactive case-based workshops to clinicians, (2) inviting multidisciplinary participation, and (3) using well-known clinicians (clinical ambassadors) as facilitators. Novel resources need to be developed so that EBP materials and clinical decision-support tools can be accessible at the point of care for efficient use (Grol & Grimshaw, 2003). For example, doctors and other health professionals can subscribe to software (www.uptodate.com/service/index.asp) that provides evidence-based clinical information that can be accessed through personal digital assistants. Investments in such innovative EBP tools and services will improve occupational therapy's effectiveness and efficiency across diverse practice settings.
Implications and Recommendations
To effectively put evidence into practice will require communication, collaboration, funding, and a strategic plan that satisfies all stakeholders. Here we offer some suggestions on and implications of EBP to continue the dialogue regarding translating evidence into practice.
Educators
Educators face challenges and opportunities when teaching students about EBP. “Educators can foster an excitement about research and communicate its applicability, or they can foster indifference to, and even dislike for, the subject” (Fineout-Overholt & Johnston, 2005, p. 39). Occupational therapy faculty should be proponents of EBP by incorporating it into the curriculum across courses (Tickle-Degnen, 2000c) and having the necessary knowledge and skills (Melnyk & Fineout-Overholt, 2004). For example, faculty members need to have resources such as access to databases for searches, knowledge about evidence-based processes, commitment to integrate evidence-based principles throughout the curriculum, and basic computer and search strategy skills.
One strategy to promote the use of research during clinical reasoning is to offer case-based pedagogies and reflective analyses (Craik & Rappolt, 2003; Welch & Dawson, 2007). Faculty could evaluate students’ clinical skills in a simulated scenario such as being able to retrieve and evaluate relevant research for a case study or actual client within a set time period.
Other useful strategies include evidence-based synthesis papers, small-group evidence-based projects, journal clubs, and educational prescriptions (which teach the EBP process). An educational prescription involves identifying the clinical problem; formulating a searchable, answerable question using PICO; looking for the relevant evidence; appraising the evidence and using the best evidence; and presenting how the evidence was found, what was found, its validity and applicability, and how it will alter clinical practice (Melnyk & Fineout-Overholt, 2004).
Clinicians
Clinicians work tirelessly to provide the best services for their clients, despite increasing demands for productivity or challenges regarding reimbursement. Although some clinicians may view EBP as an additional required task, it can be a powerful tool to help clinicians and their clients as treatment questions arise. However, clinicians need to be able to access the literature and have EBP tools. One option is to assertively ask employers for Internet access and subscriptions to databases such as Medline, PsycINFO, and the Cumulative Index to Nursing and Allied Health Literature, citing greater efficiency in finding research to inform best practice. Alternatively, clinicians could join a professional organization to access EBP resources. In-services or department meeting times can be a mechanism for investigating answers within a group whose members have varying levels of research and clinical expertise. Clinicians can brainstorm with peers and managers about how to incorporate evidence into practice and documentation (e.g., modify protocols, include patient-specific reminders in electronic documentation, use opinion leaders, create toolkits; Davis et al., 2003; Grol & Grimshaw, 2003; Pipe, Cisar, Caruso, & Wellik, 2008). If clinicians are unsure of their EBP skills, they can invite an expert in their practice area who is familiar with EBP. Ideally, using a case study approach combined with access to a knowledgeable peer can demonstrate the value of EBP (Glasziou et al., 2001; Institute of Medicine, 2008; Ketelaar, Russell, & Gorter, 2008). Practitioners can also ask occupational therapy faculty to collaborate on research projects or EBP training (Pipe et al., 2008). Finally, clinicians could join special interest sections or form networks to share their resources, such as research summaries justifying interventions or documentation methods that incorporate data collection on interventions and outcomes.
Researchers
Researchers were trained to conduct rigorous research, but some researchers may not consider multiple audiences when they design or disseminate research for multiple audiences (Glasgow & Emmons, 2007; Laupacis & Straus, 2007). When appropriate, researchers should consider studying cost-effectiveness analyses or health care use so that policymakers and reimbursement companies can understand that coverage for occupational therapy can not only improve health outcomes but also save money or resources. In addition, researchers may not be tackling problems that directly benefit clinicians’ care of clients. Sudsawad (2005) reminded researchers to consider whether their research is clinically relevant during the research planning phase. Obtaining clinicians’ input during the research design process will engender clinically relevant and generalizable research.
In addition, researchers who perform SRs need to communicate the knowledge gaps to other researchers and the profession at large so that appropriate types of research are conducted as quickly as possible. Designing the studies needed to inform clinical practice and policy decisions will help the profession become proactive and prepared. Finally, researchers could develop new formats to disseminate evidence for consumers and busy clinicians. For example, Laupacis and Straus (2007) suggested producing SRs in 20-s, 2-min, and 2-hr versions for consumers, clinicians, researchers, and policymakers.
Managers, Administrators, and Policymakers
Managers and administrators can support EBP by allotting time and providing resources to occupational therapists, such as access to computers and literature databases (see Table 2). If employers offer a clinical ladder or promotions, these programs could offer incentives to facilitate EBP, such as providing reimbursement for professional memberships and journal subscriptions, allotting time for research, establishing a mentoring program, and providing reimbursement for books and training about EBP (Pipe et al., 2008).
Resources to Locate Evidence
Note. Free = free with registration; OT = occupational therapy; + = consistently have; ± = sometimes or inconsistently have.
Policymakers and funders of research could communicate the type of data they need from researchers before research implementation. For example, researchers could incorporate research questions about cost analyses or functional outcomes into their studies.
Associations and Organizations
Occupational therapy organizations (e.g., associations, foundations) should be commended for making EBP a priority, but more work is still needed. The implementation of an evidence-based approach involves numerous steps and players, including attention to organizational change strategies. The organization's needs and barriers to and resources needed for implementation of EBP must be assessed. A strategic plan and timeline for implementing the changes and a committee responsible for setting goals, implementing changes, and refining the implementation plan are vital to successful organizational change. An ongoing issue is determining who will fund the SRs. A reproducible, well-done SR is considered to be a research project because of the time and rigor needed, but it is unlikely to be funded by an outside agency as a stand-alone research study. Organizations and researchers who produce SRs have made progress in recent years, adopting requirements for reporting characteristics, such as search strategies, inclusion and exclusion criteria, funding sources, and determination of whether the SR was an update (Moher, Tetzlaff, Tricco, Sampson, & Altman, 2007). To reach a broader audience, organizations could continue to explore nontraditional ways of disseminating evidence and clinical guidelines, such as videos on Web sites, podcasts, and online training. If financially feasible, organizations could increase the availability of evidence-based resources by making SRs free, at least to their members.
Conclusion
Occupational therapy research has made great strides toward EBP that should translate into improved services for clients and society. Some achievements of EBP include (1) numerous online resources for learning and implementing EBP (see Table 2), (2) an increased number of evidence-based occupational therapy practice workshops and conferences globally, (3) more occupational therapists with graduate degrees and research knowledge, and (4) more opportunities to collaborate with other professionals on research projects. Despite these achievements, occupational therapy still faces many challenges to implementing EBP across settings, populations, and countries. To further develop practice and establish occupational therapy as an important contributor in maintaining and improving the health of society and garnering respect as a science-based practice, occupational therapists must focus on key issues in integrating evidence into practice.
To expand EBP of occupational therapy globally and across practice settings, changes need to be made at many levels of the multiple systems that affect practice. Despite these challenges, we have offered a variety of resources, strategies, and suggestions for how each person can facilitate EBP or promote positive changes. Through communication and compromise, occupational therapists can improve their knowledge base, deliver efficient and effective services, and be reimbursed and recognized for their contributions to promoting health and participation through the engagement of occupations.
Footnotes
Acknowledgments
This work was partially supported by Susan L. Murphy's Mentored Research Scientist Award from the National Center of Medical Rehabilitation Research and by Jennifer C. Robinson's National Research Service Award from the National Institute of Nursing Research. During the development and writing of this article, Jennifer C. Robinson was at the University of Michigan School of Nursing and Susan H. Lin taught at Shenandoah University.