
Abstract
Purpose
To develop a reliable and practical questionnaire for glaucoma awareness and evaluate the impact of potential determinants.
Methods
Patients with primary open-angle, pigmentary, and exfoliation glaucoma, as well as healthy controls, were recruited. The instrument included questions about demographic characteristics, as well as 8 questions assessing the participant's familiarity with glaucoma. Rasch analysis was used for the validation of the questionnaire. The effect of demographics as potential determinants of awareness was examined with a multivariate logistic regression analysis. Bonferroni-corrected statistical significance was tested with the Mann-Whitney U test or one-way analysis of variance. Association between demographics and questionnaire scores was examined with Spearman correlation.
Results
As indicated by power analysis, responses from 175 patients (mean age 65.5 years) and 314 controls (mean age 43.3 years) were analyzed. Rasch analysis indicated no multidimensionality and good item-person targeting. Mean ± SD awareness scores for the glaucoma and control groups were 4.43±2.10 and 4.20±2.11, respectively (p=0.207). Sex and residence were not predictors of disease awareness, whereas educational level was only a determinant in the control group (p<0.001). Income was a predictor only for patients (r=0.357, p<0.001), whereas family history was predictive for both groups (p<0.001). Logistic regression analysis revealed that only family history was associated with increased awareness (χ2=4.61, p=0.03, odds ratio 1.98).
Conclusions
This study introduces a practical and valid instrument for the assessment of glaucoma awareness.
Introduction
Glaucoma is a chronic progressive optic neuropathy associated with loss of optic nerve fibers and permanent damage of visual function (1). Left untreated, a substantial proportion of patients will eventually become blind. In fact, glaucoma is a leading cause of visual impairment worldwide (2). Epidemiology studies suggest that the prevalence of glaucoma ranges between 1% and 4%, and increases as age advances (3-5). Besides age, elevated intraocular pressure (IOP) and genetic predisposition are major risk factors for the development of glaucoma (6, 7).
Visual impairment from glaucoma interferes with a variety of visually oriented daily tasks (8, 9). The debilitating impact of the disease on the patients’ quality of life and productivity indicates the need for an efficient awareness program that will educate both caregivers and patients about glaucoma (10-12). International experience on glaucoma awareness suggests that a coordinated effort is necessary, because patients remain unfamiliar with key aspects of their disease even in Western societies (13-15). However, published studies regarding glaucoma awareness present great variability in their methodology. Moreover, the lack of a validated instrument for the evaluation of glaucoma awareness indicates that any comparison of results among different populations or timeframes should be treated with extreme caution.
Within this context, the primary objective of this study was to develop a reliable questionnaire for glaucoma awareness and assess the impact of potential determinants.
METHODS
Setting
The study adhered to the tenets of the Declaration of Helsinki and written informed consent was given by all participants. This was a 2-center study conducted at the Ophthalmology Department of the University Hospital of Larissa, in central Greece, and the Ophthalmology Department of the University Hospital of Alexandroupolis, in northeast Greece, between February and June 2008. The Bioethics Committees of both hospitals approved the protocol. The Glaucoma Outpatient services of the aforementioned hospitals provide integrated care to glaucoma patients from 4 Greek counties in collaboration with the local national health system hospitals.
Participants
The patients were recruited in a consecutive-if-eligible fashion from the outpatient glaucoma services of the aforementioned hospitals during their initial visit. Eligible patients had been diagnosed with primary open angle, pigmentary, or exfoliation glaucoma by their ophthalmologist at least 6 months prior to recruitment and were on topical medications. To be eligible for the study, patients had to present at least one incident of untreated IOP >21 mmHg, typical glaucomatous defects in visual fields, optic discs with alterations typical for glaucoma, and a pathologic peripapillary retinal nerve fibre layer scan with the fast retinal nerve fiber layer mode in optical coherence tomography (Stratus OCT, Carl Zeiss Meditec, Dublin, CA, USA). Patients were excluded if they presented any of the following: history of optic neuropathy other than glaucoma, retinal pathology, corneal opacity, cataract of grade II or above according to the Lens Opacities Classification System II (16), or incisional eye surgery any time in the past. The control group consisted of participants with no ophthalmic disease attending other outpatient services who stated that they did not have glaucoma and did not take any medication for glaucoma.
The Eye Institute of Thrace 8 Glaucoma Awareness (EIT-8G) Instrument
The literature review on glaucoma awareness was negative regarding a validated questionnaire addressing the variable of interest. Thus, an exploratory interview study was designed to create the baseline for a questionnaire development. A panel consisting of 3 glaucoma experts, 2 nurses with experience in glaucoma outpatient care, and a psychologist was recruited for the exploratory study. A number of items covering glaucoma awareness were summarized and written as interview questions. Individual interviews with 10 glaucoma patients who had no previous contact with any of the members of the panel took place. The interviews were analyzed and the findings served as the basis for identifying the variables of interest that would be operationalized in specific questions to be used in our instrument.
The final version of the questionnaire consisted of 2 parts. The first part pertained to the participant's demographic characteristics, with questions regarding age, sex, educational level, residency, approximate annual income, profession, family history of glaucoma, and ophthalmic history. The second part of the instrument (i.e., the EIT-8G) consisted of 8 items that pertained to the participant's familiarity with glaucoma (Tab. I).
EIT-8G SCALE (CORE QUESTIONNAIRE)
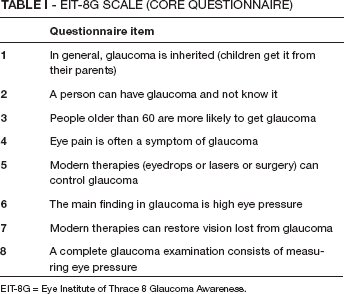
EIT-8G = Eye Institute of Thrace 8 Glaucoma Awareness.
Data collection
Participants responded to the questionnaire in the presence of an independent researcher who had no direct involvement in the provision of care. Responders were not prompted to possible answers. None of the persons approached to participate in the study declined to do so. No questionnaire was excluded from the analysis. Proxy responses were not allowed.
Validation of the EIT-8G
Awareness is a latent variable that can be inferred from a person's report. By means of an item response model, it is possible to estimate the value of the latent variable on an interval scale from the item scores that form an ordinal scale. In brief, the application of item response theory for the assessment of glaucoma awareness begins with the theoretical construction of the variable “glaucoma awareness.” Each patient has a unique glaucoma awareness. Depending on the patient's glaucoma awareness, some questions are easier to answer than others. In fact, each item (i.e., question) requires a certain amount of the latent variable (i.e., glaucoma awareness) in order to be answered correctly. Taking into account the Rasch model assumptions, an estimate of glaucoma awareness is possible on an interval scale. These assumptions are as follows. First, persons recruited for the validation of the model differ in glaucoma awareness. Second, responses to the items depend only on glaucoma awareness. Third, responses are probabilistic and conditional on the person's glaucoma awareness. Thus, if an item is not sensitive enough for the latent variable, it will appear as noisy when evaluating the fit of data to the model. Similarly, if a patient has another problem unrelated to glaucoma that limits his or her ability to respond to the items, that person's response pattern will be identified as outlying relative to the expectations of the model.
Further to adequate internal validity, an instrument should present adequate external validity, as well. In brief, groups who by general consensus have a higher standing on the relevant constructs should score higher; in this case, we compared medical staff and equivalently educated nonmedical staff, in order to test the instrument's sensitivity to knowledge.
Statistical analysis
Rasch analysis was performed with Winsteps software (Linacre, 2007). To examine the independent effects of demographic variables on the likelihood of being unaware of glaucoma, we conducted a multivariate logistic regression analysis. Residency, sex, educational level, and the presence of relatives with glaucoma were included in the model as categorical variables with age and reported annual income as continuous variables. The above variables were subjected to a forward stepwise selection procedure in which variables significantly associated with the outcome at the p<0.2 level were included. Associations between demographic characteristics and questionnaire scores were examined with Spearman correlation coefficient. Statistical significance was tested using one-way analysis of variance (ANOVA) and Tamhane post hoc test or Mann-Whitney U test as appropriate, and its level was set at 0.008 after Bonferroni correction. A power analysis indicated that 170 glaucoma patients would be adequate for a power of 0.8 for most comparisons. These statistical analyses were performed with the SPSS (Statistical Program for the Social Sciences) version 15 software platform (SPSS Inc., Chicago, IL, USA).
Results
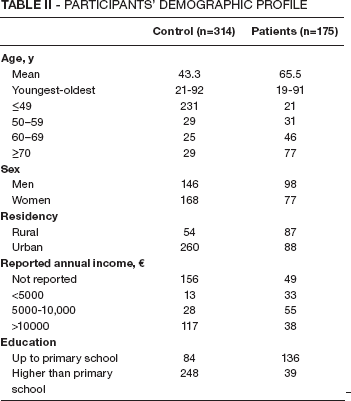
Our study sample consisted of 175 glaucoma patients (98 men, 77 women), with mean age 65.5 years (youngest: 19 years, oldest: 91 years). The control group consisted of 314 healthy volunteers (146 men, 168 women), with mean age 43.3 years (youngest: 21 years, oldest: 92 years). Seventy of the patients (40%) reported that they had at least one parent or sibling who had been diagnosed with glaucoma. Fifty-five (18.3%) of the healthy volunteers declared that they had at least one parent or sibling who had been diagnosed with glaucoma. The detailed demographic characteristics of the 2 groups are presented in Table II.
PARTICIPANTS’ DEMOGRAPHIC PROFILE
Item analysis used patient responses to the 8 items. Mean ± SD item measure was 0.0±0.93 (Tab. III). Regarding fit statistics, none of the items fell outside the 2-logit units tolerance zone (Fig. 1). On the other hand, the mean ± SD person item measure was 0.12±1.65 (Fig. 2). The model demonstrated excellent distributions of the infit and outfit statistics for estimates of glaucoma awareness (Fig. 3).
RASCH ANALYSIS OF THE EIT-8G SCALE: ITEM FIT STATISTICS
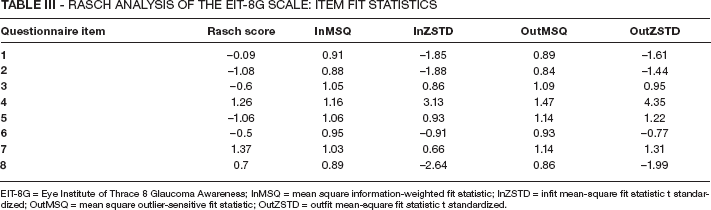
EIT-8G = Eye Institute of Thrace 8 Glaucoma Awareness; InMSQ = mean square information-weighted fit statistic; InZSTD = infit mean-square fit statistic t standardized; OutMSQ = mean square outlier-sensitive fit statistic; OutZSTD = outfit mean-square fit statistic t standardized.
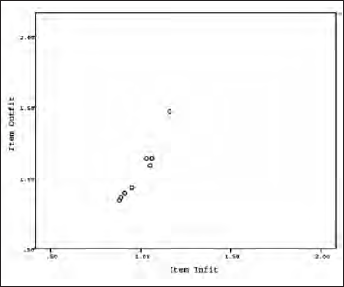
Rasch analysis. Fit statistics for the items.
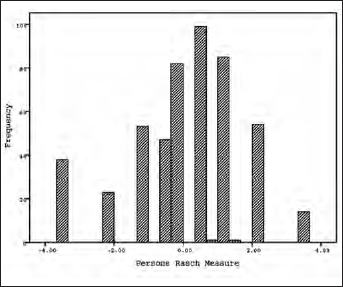
Rasch analysis. Person distribution on the Rasch scale.
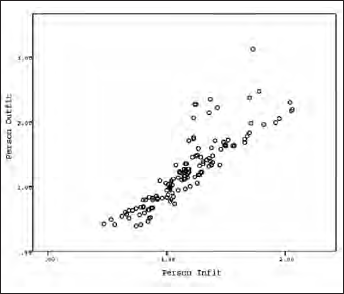
Rasch analysis. Distributions of infit and outfit statistics for estimates of glaucoma awareness.
Regarding the dimensionality of the questionnaire, Rasch analysis indicated no evidence of multidimensionality (the first contrast of the principal components analysis was below 1.5) and no item-person mistargeting (detailed results not shown). However, person reliability was 0.57, possibly due to the limited number of items. On the other hand, the instrument presented adequate freedom for differential item functioning for sex, residency, and presence of relatives with glaucoma.
Regarding the mean awareness scores for the glaucoma and control groups, respectively, the results were 4.43 (SE 0.16, SD 2.10) and 4.20 (SE 0.12, SD 2.11) (p=0.207, Mann-Whitney U test, Tab. IV). Non-significant differences in questionnaire scores were associated with sex (p=0.271, Mann-Whitney U test) and residence (p=0.778, Mann-Whitney U test). Educational level was not a predictor of heightened awareness when all participants were analyzed after Bonferroni correction (p=0.029, one-way ANOVA, Tab. III). Similarly, after a subgroup analysis, educational background was not associated with awareness scores in the patient group (p=0.966, one-way ANOVA, detailed data not shown). On the contrary, awareness was associated with educational level in the control group (p<0.001, one-way ANOVA, detailed data not shown). Specifically, questionnaire scores between participants with up to primary education differed significantly from those with highest education (p<0.001, Tamhane post hoc test). However, there was no significant difference for the comparison between controls with up to primary education and those with up to secondary education (p=0.059, Tamhane post hoc test, data not shown) or for the comparison between controls with up to secondary education and those with highest education (p=0.195, Tamhane post hoc test, data not shown).
IMPACT OF DEMOGRAPHIC VARIABLES ON AWARENESS SCORES
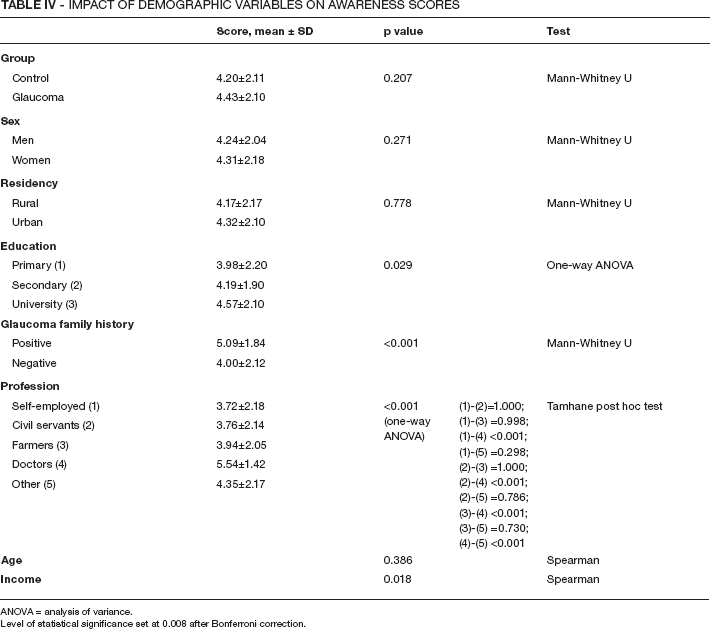
ANOVA = analysis of variance. Level of statistical significance set at 0.008 after Bonferroni correction.
Furthermore, no significant correlation was detected between awareness and income when both groups were considered (Spearman ρ=0.143, p=0.018). However, when each group was examined separately, a significant correlation between income and questionnaire score was detected for the patients (Spearman ρ=0.357, p<0.001), but not the controls (Spearman ρ=0.046, p=0.575). Regarding the participants’ profession, for both groups, medical doctors scored significantly better (p<0.001, Tamhane post hoc test) compared to persons from any other professional group (i.e., civil servants, farmers, self employed), even when scores were adjusted for educational background (i.e., university-level educational background). There was no significant difference between scores achieved by civil servants, farmers, and self-employed participants. On the other hand, family history positive for glaucoma was associated with higher scores in the EIT-8G scale for both groups (p<0.001 in each case, Mann-Whitney U test).
Item analysis of the questionnaire showed that higher income contributed to higher scores in 2 items for the glaucoma group and none for the control group, whereas higher educational background contributed to higher scores in 3 items in controls and none in glaucoma patients (Tab. V).
IMPACT OF DEMOGRAPHIC VARIABLES ON ITEM SCORES
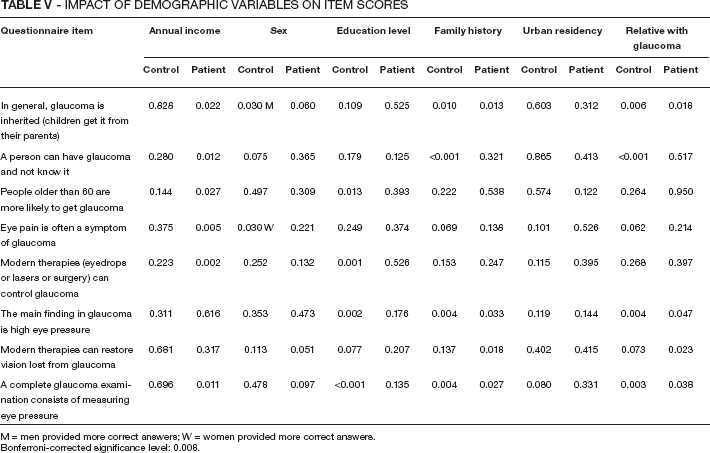
M = men provided more correct answers; W = women provided more correct answers. Bonferroni-corrected significance level: 0.008.
Logistic regression analysis was conducted to assess whether the 5 predictor variables of sex, education, positive family history, age, and reported annual income were significantly associated with a participant being aware of his or her condition. The 5 predictors were subjected to a forward selection procedure in which variables significantly associated with the outcome at the p
Discussion
Glaucoma is a major public health problem due to the disability and the financial burden it causes. Gasch et al (17) suggested that effective education regarding the disease could diminish its personal and societal burden by making individuals undergo screening, so that cases are detected early and treated appropriately. A review of the literature indicates that previous research has attempted to evaluate awareness in homogenous populations (18-21); however, a validated instrument that could construct and quantify the latent variable of glaucoma awareness had yet to be developed.
To our knowledge, this is the first study that investigated glaucoma awareness in a group of known glaucoma patients by means of a validated instrument that allows the construction and quantification of the variable in question. Regarding the EIT-8G instrument, analysis of the 8 items indicated no misfits to the model. Moreover, no serious misfit was observed for persons, as indicated by the mean fit residual value for items. No evidence of differential item functioning was observed for gender, age, education, residence, or family history. On the other hand, the results were supportive of the unidimensionality of the scale with no major loadings on the principal component analysis factors of the residuals. Although a larger number of items would potentially contribute to the unidimensionality of the scale, more questions might have limited the usefulness of the instrument as a screening test for large populations or busy outpatient services. Instrument validity was further supported by known-groups methods. Medical staff scored higher than nonmedical counterparts, suggesting that the EIT-8G scale has the ability to distinguish between groups with established differences in levels of awareness.
The construction of the variable awareness allowed its quantification and evaluation of the impact of potential modifiers. Both groups demonstrated average awareness. Contrary to Danesh-Meyer et al (18), glaucoma patients performed slightly better than controls in the EIT-8G scale. In fact, our results were similar to Gasch et al (17), who reported that the diagnosis for glaucoma was not an independent determinant of glaucoma awareness. However, it should be mentioned that our 2 groups were demographically dissimilar, thus the aforementioned comparison should be treated with caution.
Analysis of the items indicated a series of alerting results. In agreement with previous reports, a significant percentage of the responders believed that glaucoma would present with ocular discomfort, thus its onset or progress could easily be perceived by the patient (18). On the other hand, 43 (24.6%) of the patients and 106 (33.8%) of the controls were under the impression that eyesight lost from glaucoma could be restored.
Regarding the impact of potential modifiers on glaucoma awareness, in agreement with previous surveys, better educated individuals were less likely to be unfamiliar with the disease (17, 22-25). On the other hand, socioeconomic status primarily determined the familiarity of glaucoma patients with their disease (22-25). A possible explanation might be that public screening programs for glaucoma and other ophthalmic diseases have yet to be developed in a nationwide scale in Greece. On the other hand, private insurance funds promote ophthalmologic screening and adopt integrated disease management programs that additionally promote disease awareness. Our results confirmed earlier studies that indicated the higher familiarity of medical staff in comparison to other professional groups (17).
When a logistic regression model was used, the demographic variables that were associated with the probability of being aware of glaucoma indicated that only the presence of a relative with glaucoma was significantly associated with increased familiarity with the disease. This association is in agreement with the majority of previous reports (18, 26-29).
Certain limitations of our study need to be kept in mind. The EIT-8G scale was not designed to explore the whole spectrum of knowledge in glaucoma, but rather to provide a simple and fast instrument for screening purposes in clinical and research settings. For that reason, only items that were considered to be more relevant to glaucoma awareness were used. As a result, certain more complex items used in other surveys that assessed the depth of knowledge (e.g., “fluorescent lights will make glaucoma worse”) were not included in the final version of the scale. Moreover, the scale was developed according to the familiarity norms of the predominantly white Greek population, so that items used for other populations (e.g., “glaucoma is more common in blacks”) were excluded. On the other hand, the instrument solely evaluates the awareness of glaucoma and non-glaucoma populations, and not the medical practice per se, thus, certain items commonly used in other surveys (e.g., “Can you name your medication?” [30, 31] or “Have you ever had an eye exam that included having your pupils dilated?” [30, 31]) were considered as incompatible with the objectives of the scale. Aforementioned considerations indicate that further testing of the fit of data from the EIT-8G to the Rasch measurement model in larger and appropriately targeted samples is recommended to confirm the findings of the current study.
In conclusion, this study introduced a valid instrument for the quantification of glaucoma awareness, enabling comparative studies in different populations and timeframes. In particular, the EIT-8G scale might be useful for the evaluation of educational campaigns in glaucoma and for the evaluation of the overall management of the patients in glaucoma outpatient services. After all, the common methodology in public awareness is crucial in combating vision loss from glaucoma, and restricting the overall burden of the disease.