
Abstract
Purpose
To report the frequency of nonorganic visual loss (NOVL) and associated psychopathology in children.
Methods
A total of 973 children were examined in our ophthalmology practice between 2006 and 2009. Basic ophthalmologic exploration (visual acuity, stereopsis, cycloplegic refraction, ocular motility, pupil dynamics, biomicroscopy, indirect ophthalmoscopy) and specific tests for NOVL diagnosis were performed (confusion with lenses test, mirrors test, Roth test, Bravais test). We also investigated the psychosocial situation and associated psychiatric problems.
Results
Thirty children were diagnosed with NOVL. The mean age of the children was 8.93 years (±2.61); 70% were girls. September was the commonest month of presentation (26.7%) and unilateral (3.3%) or bilateral (80%) visual loss was the most frequent symptom (83.3% in total). In 20% of cases we detected psychosocial anomaly and 40% were seeking to wear glasses.
Conclusions
Malingering in children is very frequent. We can make the diagnosis with simple tests. It is not necessary to perform imaging and electrophysiologic testing, thus avoiding unnecessary examinations as well as absenteeism from work for parents and health care costs.
Introduction
Nonorganic visual loss or functional visual loss (FVL) usually refers to any visual disturbance without any other associated organic pathology. Nonorganic visual loss may be psychogenic or the result of malingering (1, 2).
We must distinguish between malingering in adults and children (3, 4). Adults deliberately feign visual loss for secondary purpose. However, children do not usually have that intentionality, and FVL is usually associated with psychosocial events (family, school) and psychiatric disturbance (anxiety, stress, depression, attention deficit and hyperactivity) (5-7).
Malingering in children or FVL has been reported to be present in between 1% and 5% of children in a general ophthalmology practice (4). Girls predominate, at an age ranging from 9 to 11 years, and most commonly at the beginning of the academic year, while the incidence is lower during holidays (8).
The different types of presentation FVL include monocular or binocular reduced visual acuity, visual field loss, color vision abnormalities, loss of stereo acuity, accommodation paralysis, and accommodation spasms. Some patients have associated symptoms like headache, eye pain, double vision, photopsias, or light sensitivity (9).
Functional visual loss should be suspected when symptoms do not match with the ophthalmic assessment, and are supported by anamnesis about social situation, family stressors, school difficulties, or economic problems (5).
The majority of cases resolve spontaneously, but it is important to inform parents and pediatricians, and specialized psychological or psychiatric treatment is necessary to resolve some cases (2, 5).
MATERIALS AND METHODS
We present a series of 30 cases of malingering in 973 children with visual disturbance seen by Unity of Neuro-ophthalmology and Ocular Motility of San Carlos Hospital, Madrid, Spain, from 2006 until 2009.
A basic ophthalmologic examination was performed on all patients consisting of the following explorations: visual acuity (VA) (Piggasou and Snellen optotypes), slit-lamp and fundus examinations, pupil dynamics and ocular motility, and stereoscopic visual acuity with and without cycloplegic refraction.
If all the previous explorations were normal, more specific examinations were carried out.
The mirror test
The mirror test (Fig. 1) is based on the plane mirrors property to double distances. First, VA is tested 5 meters away from the child and later a mirror is located in front of him or her, reflecting optotypes which are situated at his or her back. If the child can read the same line in both situations, it means that VA doubles the first admitted one (10).

The mirror test.
The confusing lenses test
In the confusing lenses test (Fig. 2), the ophthalmologist places strong plus spherical lenses (+6.00 diopters) in front of both eyes and gradually negative lenses are put in front of the “bad” eye in case of unilateral loss vision until neutralizing it. The examiner retests the vision with each change of lens and obtains the optimum VA of that eye when graduation is zero (10).
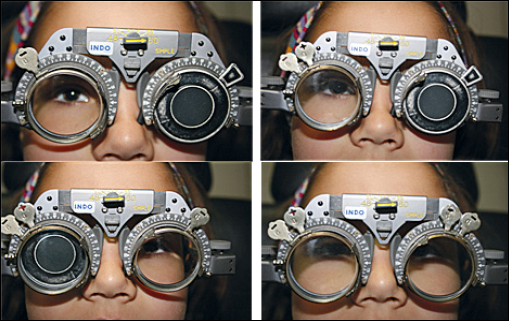
The confusing lenses test.
Roth test or writing test
Older children can do the Roth test or writing test (Fig. 3), which consists of writing his or her name, interrupting him or her during the exercise, and encouraging him or her to continue from the same point. If he or she can do it, that means the VA is 0.1 or higher. Another way to carry out the test is by drawing a thick line, interrupting the child, and encouraging him or her to continue. If the child declares himself or herself unable to do it, that supports malingering (10).
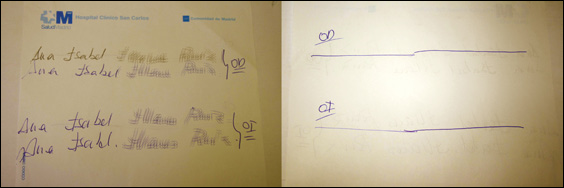
The Roth test.
The Bravais test
The Bravais test (Fig. 4) uses colored lenses and charts. This test is based on the principle that colored glass will filter out complementary colors. We can identify the eye being used by inviting the child to read a chart with alternating red and green letters through red/green glasses. If a red lens is placed in front of the “better” eye, red letters will be neutralized. If the child can read the entire chart we know he or she is using the “bad” eye (2, 10).
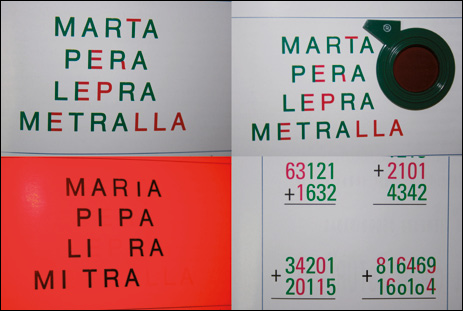
The Bravais test (10).
Analysis of the data was performed using statistical analysis software SPSS 15.0.
Results
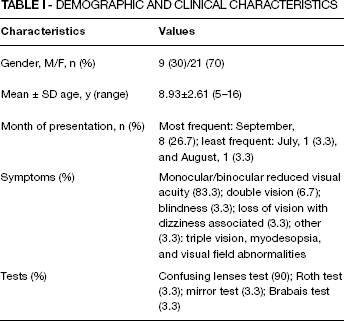
Functional visual loss and malingering were diagnosed in 30 patients (3.08%), 70% girls and 30% boys. Their age range was from 5 to 16 years, with a mean of 8.93 (±2.61) years. The most common month of presentation was September (26.7%) and the least common ones were July (3.3%) and August (3.3%) (Fig. 5 and Tab. I).
DEMOGRAPHIC AND CLINICAL CHARACTERISTICS
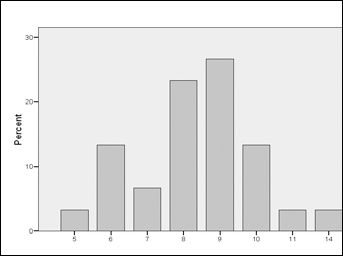
Age distribution of malingering patients.
The most frequent pattern of FVL was monocular (3.3%) or binocular (80%) reduced visual acuity (83.3% in total), followed by double vision (6.7%), blindness (3.3%), loss of vision with associated dizziness (3.3%), and other (3.3%): triple vision, myodesopsia, and visual field abnormalities.
We carried out the confusing lenses test in 90% of cases, the Roth test in 3.3%, and others like the mirror or Bravais test in 6.7%.
The mean VA OD was 0.37±0.2 (0.4 or less in 73.3% of cases) and OS 0.36±0.18 (0.4 or less in 76.7% of cases). These means were improved with confusing lenses test: 0.79±0.2 with OD (0.8 in 70% of cases) and 0.8±0.2 with OS (0.8 in 63.3% of cases) (Tab. II).
RESULTS
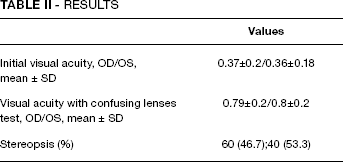
Stereoscopic visual acuity was 60 seconds of arc in 46.7% of the children and 40 seconds of arc in 53.3%. Stereoscopic acuity correlates well with Snellen acuity, and it has shown that 40 seconds of arc of stereoacuity is the equivalent to no less than 6/6 acuity in both eyes (11, 12).
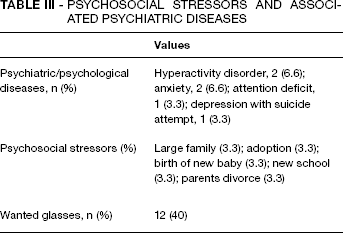
Psychological diseases were diagnosed in 6 cases (20%): hyperactivity disorder (2 cases), attention deficit (1 case), anxiety (2 cases), and depression with suicide attempt (1 case). We detected the following psychosocial stressors in these 6 patients: large family, adoption, birth of new baby, new school, and parents’ divorce. However, the majority of malingering children simply wanted to wear glasses (40%) (Tab. III). (13)
PSYCHOSOCIAL STRESSORS AND ASSOCIATED PSYCHIATRIC DISEASES
It was necessary to talk to their parents alone and explain the good health of their child's eyes. Most cases resolved spontaneously by checking children periodically and only some required psychological treatment.
Discussion
Our study proves high incidence of malingering in children at a general ophthalmology practice and the importance of recognizing FVL and managing basic tests for correct diagnosis. This way we minimize unnecessary and invasive tests and can detect concomitant psychosocial events (2). The suspected diagnosis is fundamental when visual symptoms are not concordant with normal exploration. We must be patient to detect malingerers, spending several sessions if necessary. Legally, it is convenient to perform a differential diagnosis with complementary examinations and consulting other specialists while we confirm diagnosis. We can only diagnose FVL when organic alterations are dismissed (3, 14).
In case of childhood simulated visual symptoms, the prognosis is excellent. The majority of them resolve spontaneously. We should advise parents on good prognosis, inform the pediatrician, and offer specialized psychological or psychiatric treatment in some cases (2, 4, 6).
Regarding management, there has been an important evolution in recent years. The French school used invasive methods like methylene blue intramuscular injection, telling children that blue urine meant total recovery (10). However, the natural history of FVL recommends an expectant attitude, reexamining children to document improvement until complete resolution (2).
In summary, childhood simulated visual symptoms are a relevant pathology at any general ophthalmology practice. We should suspect it and manage the specific diagnostic tests to avoid unnecessary explorations and health expenditure. Multidisciplinary units should be developed for treatment and monitoring of patients due to the high incidence of FVL and associated psychopathology.